Psych · psychotherapy
Group psychotherapy
Also known as Group therapy · Group treatment · Process group · Interpersonal group psychotherapy · Cognitive behavioural group therapy · CBGT · DBT skills group · Therapeutic community groups · Multiperson psychotherapy
Exam-exhaustive fellowship reference on group psychotherapy — definition and formats, Yalom therapeutic factors, cohesion, selection and frame, leadership, disorder-specific evidence (depression, anxiety/SAD, PTSD, schizophrenia, BPD multiperson programmes), format equivalence vs individual therapy, crises and confidentiality limits, and CASC/MEQ technique. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Fellowship examiners expect you to select candidates, set a frame (size, closed/open, confidentiality limits), name therapeutic factors, lead process without scapegoating, cite disorder-specific group evidence, and know when group is contraindicated or when individual risk care must come first.[10][4][8]

Definition and scope
Group psychotherapy is a planned clinical intervention with assessment, goals, session structure, outcome monitoring, and clinical accountability. It differs from peer support and from non-therapy multiperson meetings that lack a treatment contract.[3][10]
| Format | Primary aim | Clinical leadership |
|---|---|---|
| Group psychotherapy | Symptom change and/or interpersonal change via group process or protocol | Trained therapist(s); clinical notes; risk responsibility |
| Psychoeducation group | Knowledge, illness model, self-management | Educator-clinician; less process depth |
| Peer support / mutual aid | Lived-experience support, hope | Peer facilitators; not equivalent to therapy |
| Ward community meeting | Milieu communication, practical issues | Variable; not automatically therapy |
Pseudo-group care — unstructured chat labelled “group therapy” without goals, selection, or leadership competence — fails both fidelity and safety standards.[3][10]
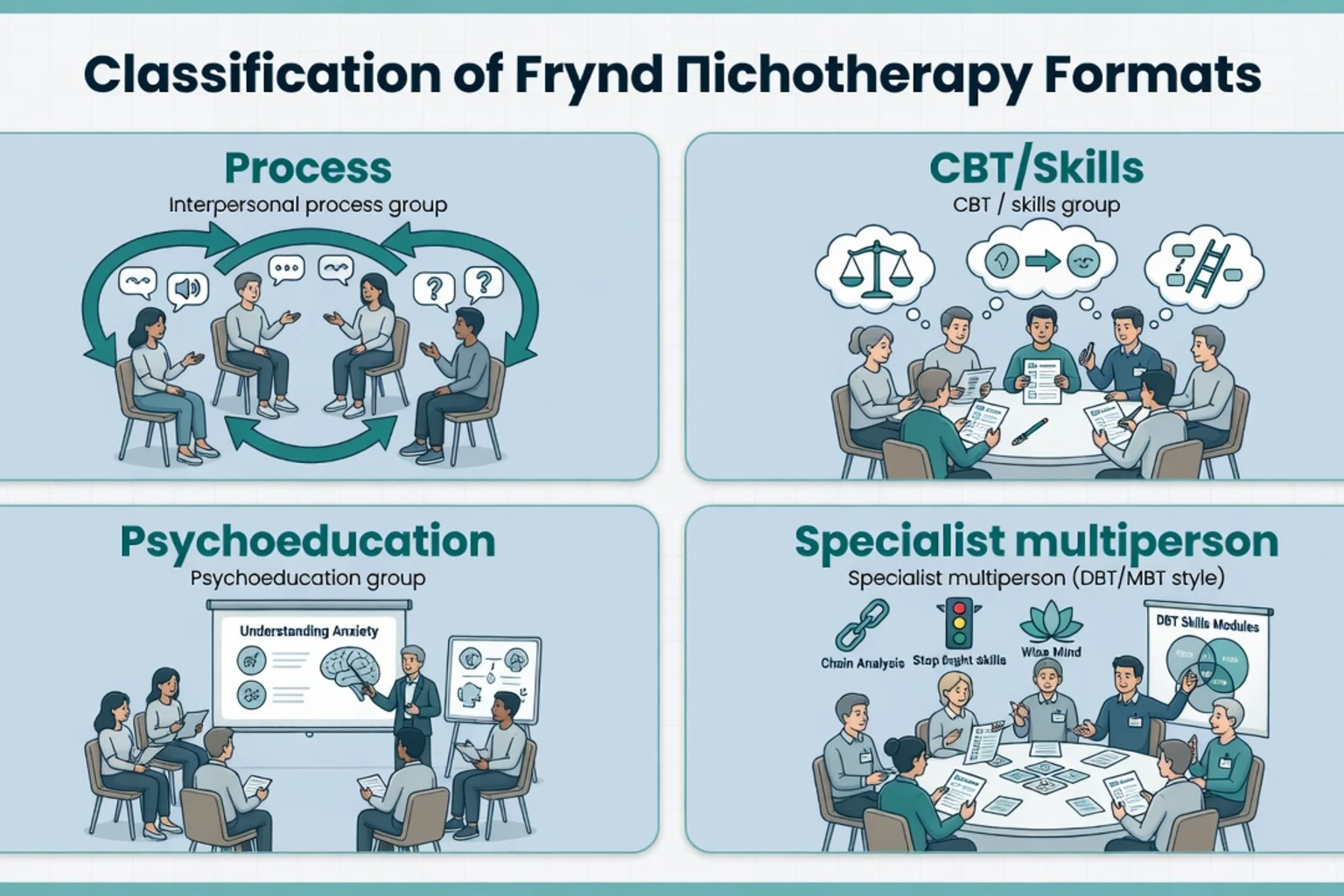
Major model families
- Interpersonal / process groups (Yalom lineage) — here-and-now interaction, feedback, social microcosm.[10]
- CBT groups / CBGT — structured agenda, cognitive and behavioural methods, homework, exposure where indicated (classically social anxiety).[5][4]
- Skills groups — modular skill acquisition (prototype: DBT skills within comprehensive DBT).[14][15]
- Psychodynamic / group-analytic — free-floating discussion, transferences to members and conductor, matrix concepts.[10]
- Specialist multiperson programmes — MBT partial hospitalisation and multiperson mentalising work; multi-family psychoeducation in psychosis pathways.[12][13][7]
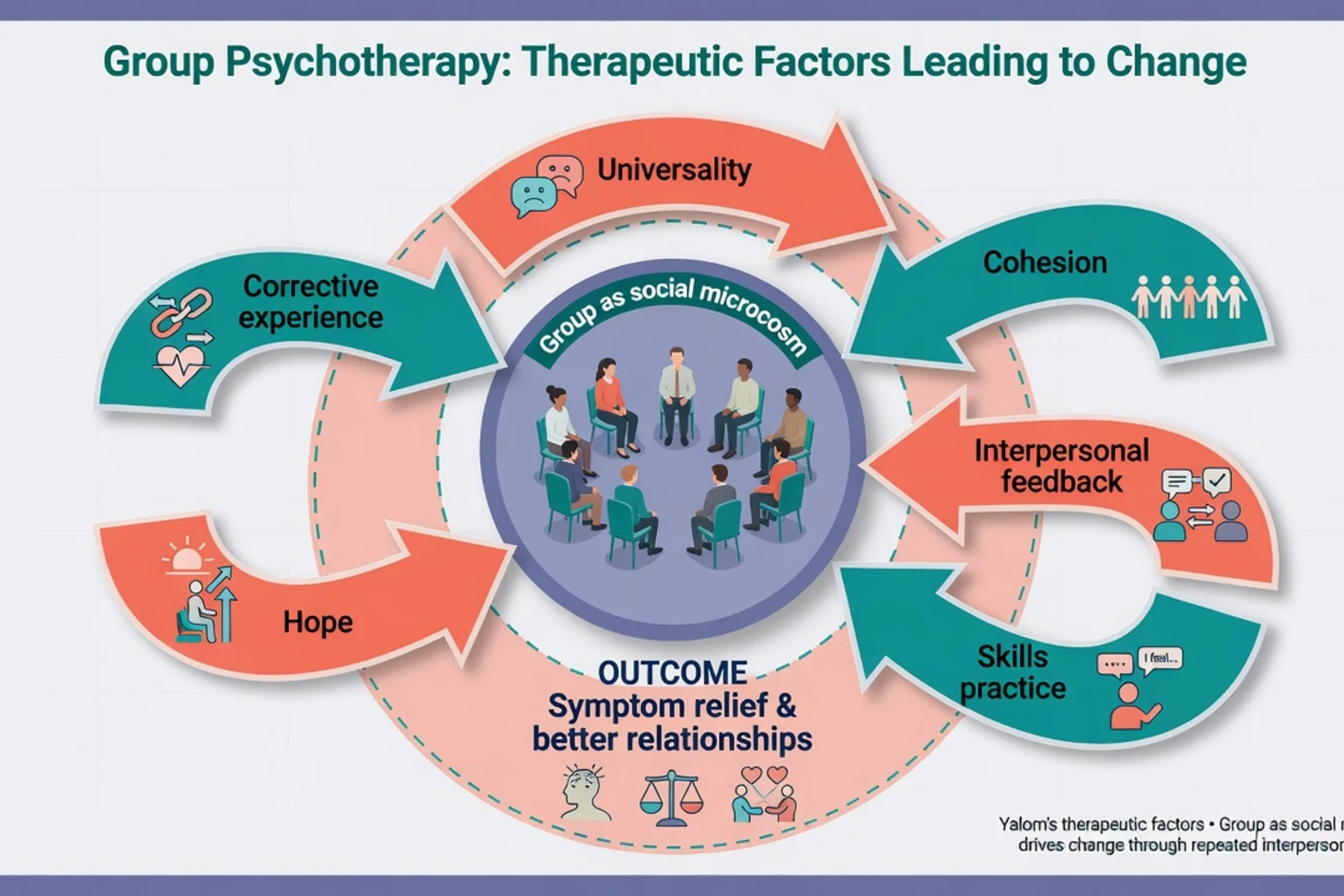
Therapeutic factors and mechanisms
Classic reviews catalogue therapeutic factors members and therapists report as helpful: universality, instillation of hope, imparting information, altruism, corrective recapitulation of the primary family group, development of socialising techniques, imitative behaviour, interpersonal learning, group cohesiveness, catharsis, and existential factors.[10]
Cohesion — members’ sense of belonging, commitment, and mutual engagement — shows a reliable positive association with outcome across dozens of studies in contemporary meta-analysis.[1] Alliance to the leader and cohesion to the group can both predict change in short-term groups; leadership that builds early engagement matters.[17]
Mechanism language by model
- Process groups: habitual interpersonal patterns reappear in the room (social microcosm); feedback and new relational experiences produce interpersonal learning.
- CBT groups: shared psychoeducation, cognitive restructuring, behavioural experiments, graded exposure, and homework accountability; peer modelling amplifies practice.
- DBT skills groups: acquisition, strengthening, and generalisation of mindfulness, distress tolerance, emotion regulation, and interpersonal effectiveness — skills group is necessary but not sufficient for comprehensive DBT.[14][15]
- MBT multiperson settings: multiple minds scaffold mentalising under interpersonal arousal; day-hospital packages combine individual and group elements.[12][13]
Epidemiology, access, and systems role
Groups expand access and cost-efficiency in public mental health. Community group psychological therapies for depression show benefit versus usual care in systematic review, supporting stepped-care deployment.[8] Network meta-analysis of CBT delivery formats for adult depression positions group CBT among effective formats alongside individual, telephone, and guided self-help options — format choice is not a pure efficacy hierarchy when protocols are sound.[16]
Child and adolescent group treatments also show overall positive effects versus wait-list/placebo controls in classic meta-analysis — developmental adaptations (parents, school roles, shorter attention spans) still apply.[11]
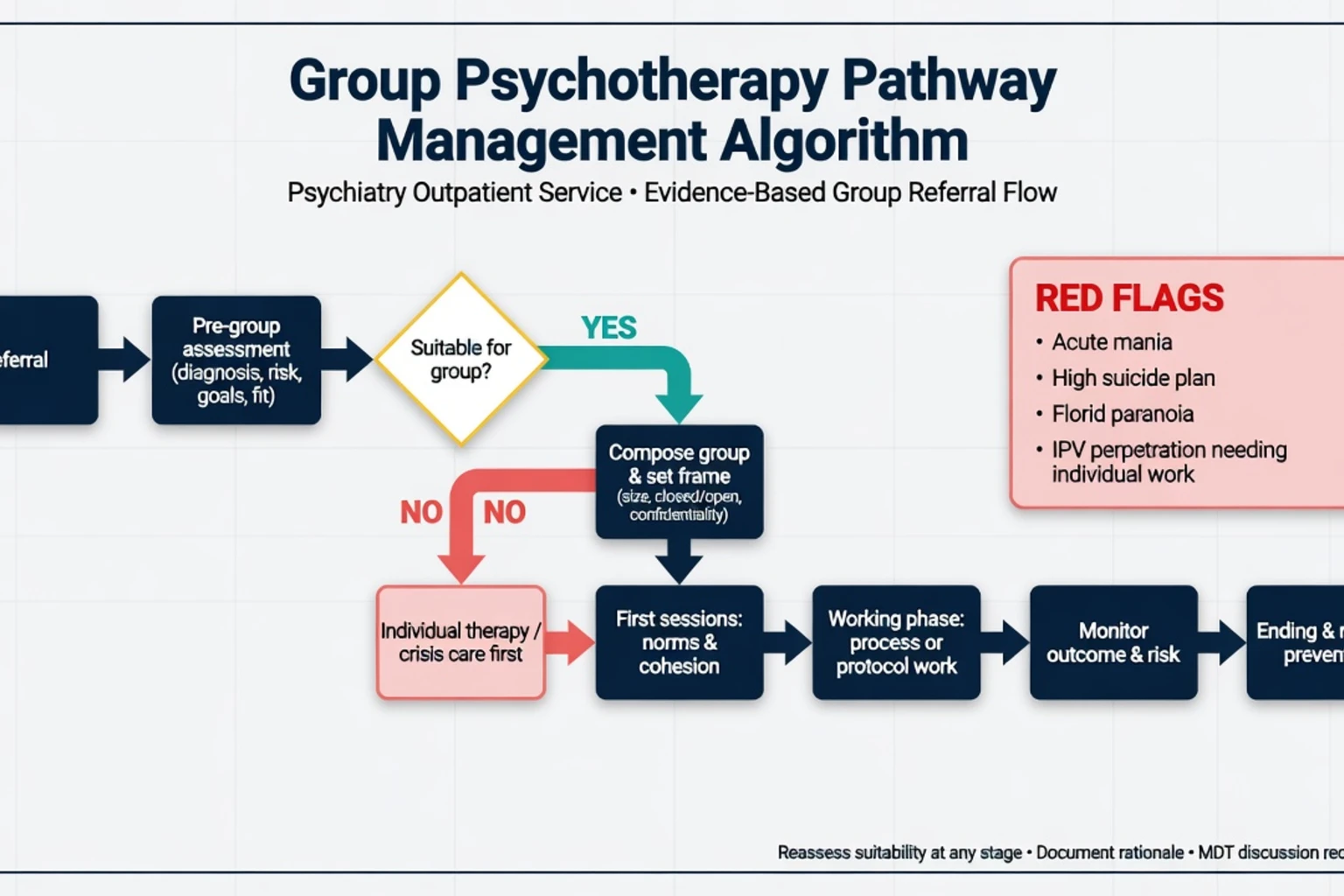
Assessment and selection (pre-group work)
Pre-group individual assessment is not optional bureaucracy; it is clinical risk and composition work that protects cohesion and safety.[3][1]
Assess
- Diagnosis, severity, comorbidity (substance, personality, neurodevelopmental).
- Risk: suicide, self-harm, violence, safeguarding, intimate partner violence (victim or perpetrator dynamics).
- Goals: symptoms, interpersonal change, skills, relapse prevention.
- Interpersonal style: monopolising, silent/withdrawn, hostile, paranoid, highly shame-prone.
- Prior group experience, literacy/language needs, transport/childcare attendance barriers.
- Capacity to honour limited confidentiality and give/receive feedback.
Composition principles
- Prefer homogeneous enough membership for shared goals (e.g. social anxiety CBGT) while avoiding a single isolated “different” member who becomes a scapegoat.[5]
- For process groups, balance verbal activity and severity when possible.[10]
- Trauma-focused groups need careful screening, grounding capacity, and leader competence — poorly run trauma groups risk iatrogenic harm.[6]
Common relative contraindications / deferrals
- Acute mania or mixed state needing medical priority.
- Florid persecutory psychosis without engagement capacity for process work.
- High immediate suicide plan requiring containment (group is not a safety plan).
- Active perpetrator of IPV needing individual risk and legal pathways first.
- Severe intoxication each session; profound cognitive impairment precluding protocol.
- Unwillingness to accept limited confidentiality norms.
Defer elective process work when acute risk or inability to use multiperson norms dominates; reassess after stabilisation.[3]
Stable psychotic-spectrum patients may still benefit from structured group psychosocial treatments supported by meta-analysis — format and content matter more than a blanket ban on “any group.”[7]
Frame, structure, and leadership
Practical frame (exam-ready defaults)
- Size: often about 6–10 for process/therapy groups; skills groups may be larger; very large “groups” become classes.
- Closed vs open/rolling: closed groups protect cohesion and termination work; open groups improve access but challenge cohesion.
- Duration: time-limited CBT packages (e.g. 8–16 sessions) vs longer process/dynamic groups.
- Co-therapy: two leaders improve observation of process, modelling, and cover for leave — clarify roles.
- Confidentiality: members must understand limits — duty of care, mandatory reporting, and that other members are not bound by professional codes.
Frame choices should serve cohesion, attendance, and model fidelity rather than administrative convenience alone.[1][3]
Phase structure
| Phase | Leadership tasks |
|---|---|
| Beginning | Norms, hope, engagement, early cohesion, manage anxiety and drop-out risk |
| Working | Process: here-and-now feedback, block scapegoating; Protocol: agenda fidelity, exposure/skills practice |
| Ending | Consolidate gains, process loss of group, relapse-prevention plans, individual step-down |
Leadership is active: protect the frame, invite silent members, limit monopolisers, name subgrouping, and keep risk monitoring live even in “process time.” Recent research syntheses emphasise both outcome efficacy and process quality (cohesion, alliance, composition) as examination-worthy domains.[3][1][17]
Disorder-specific evidence (high-yield)
Format equivalence
A large meta-analytic perspective comparing individual and group formats finds no consistent superiority of individual therapy when treatments, patients, and doses are appropriately compared — group is not a second-class default when content is equivalent and selection is sound.[2]
Depression
Community group psychological therapies reduce depressive symptoms versus usual care; group CBT shows efficacy and acceptable dropout profiles in systematic review/meta-analysis.[8][9] Cuijpers network meta-analysis supports group CBT as an effective delivery format for adult depression among several viable formats.[16]
Anxiety and social anxiety
Group psychotherapy for anxiety disorders shows overall efficacy in systematic review/meta-analysis.[4] For social anxiety disorder, group treatments (including CBGT traditions) have RCT meta-analytic support — exposure and cognitive restructuring transfer naturally to a multiperson laboratory.[5]
PTSD
Group psychotherapy reduces PTSD symptoms versus no-treatment controls; comparative efficacy versus alternative active treatments is more mixed — selection, model (especially exposure-based group CBT), and safety structure matter.[6]
Schizophrenia / psychotic-spectrum
Group treatments targeting positive/negative symptoms and related domains show meta-analytic signals for several commonly used group psychosocial approaches — use as adjunct to antipsychotic care and recovery-oriented systems, not as monotherapy for acute psychosis.[7]
Borderline personality pathways
Landmark DBT packages include skills training groups as a core mode alongside individual therapy, phone coaching, and team consultation — Linehan’s foundational RCT and later component work inform this architecture.[14][15] MBT partial hospitalisation and multiperson mentalising programmes demonstrate substantial and durable gains versus treatment as usual in classic trials and long-term follow-up.[12][13]
Combined care, medication, and stepped care
Group therapy is compatible with antidepressants, mood stabilisers, and antipsychotics. For moderate–severe depression, combine optimised pharmacotherapy with group CBT when indicated rather than forcing an either/or ideology.[16][8] In personality disorder pathways, multiperson programmes sit within structured packages, not as casual add-ons to polypharmacy.
Stepped care sketch (exam language): brief psychoeducation → structured group CBT/skills → specialist process or multiperson programmes (MBT/DBT-aligned) → individual therapy for those who cannot use group or need additional work. NICE-style depression pathways and APA-aligned practice commonly accept evidence-based group formats; RANZCP training expects psychological therapy competence including group settings. Match local supervised competence, waiting lists, and cultural access needs.[3][16]
Complications, crises, and ethics
High-yield hazards that require active leadership and documentation include scapegoating, subgrouping, confidentiality breaches, symptom contagion, boundary failures, and iatrogenic trauma activation in poorly prepared trauma groups.[10][3][6]
- Scapegoating — leader must block and reframe; do not collude.
- Subgrouping and secrets — name out-of-session alliances that split the group.
- Confidentiality breaches including social media — restate rules; consider removal if repeated.
- Symptom contagion (self-harm methods) — set norms early; redirect to skills and individual risk review.
- Boundary failures — dual relationships, favouritism, post-session socialising with selected members.
- Iatrogenic trauma activation in poorly prepared trauma groups.
Process failures and safety breaches are clinical events, not merely “group dynamics entertainment.”[10][3][6]
Special populations
- Adolescents: group efficacy supported meta-analytically; involve carers/schools as model requires; bullying risk needs active management.[11]
- Older adults: late-life depression groups and role-transition themes; hearing/mobility and cognitive load adaptations.[8]
- Perinatal: prefer evidence-based protocols with childcare logistics; risk and infant safety always primary.[3]
- Cultural and language-matched groups: improve engagement and universality; avoid assuming Western process norms fit every community.[3]
- Intellectual disability: simplified psychoeducation and skills groups with carers; process groups rarely appropriate without adaptation.[3]
Exam traps (rapid fire)
- Claiming group is always inferior to individual therapy.[2]
- Confusing peer support with group psychotherapy.[3]
- Promising absolute confidentiality.[3]
- Equating DBT skills group alone with full DBT.[15]
- Putting acute high-risk or manic patients into unstructured process groups.
- Forgetting cohesion as a process variable linked to outcome.[1]
- Running exposure-based trauma groups without selection and competence.[6]
CASC / viva technique snippets
Plain-language opener: “Group therapy is a planned treatment where you work with others who share similar difficulties. You practise skills and notice how you relate to people — not just talk to me alone. What you hear is private in spirit, but I cannot guarantee what others say outside, and I still have the same safety duties as in any clinic.”[3][10]
Social anxiety CBGT pitch: “The group becomes a safe practice space for the social fears we map — graded experiments with others who understand the anxiety, not a forced performance.”[5]
When to decline group today: “Your risk is too high for a multiperson process setting right now. We will stabilise safety first, then reconsider a structured group when it is safe and useful.”[3]
Bottom line for fellowship candidates
Offer group psychotherapy as structured, selected, framed multiperson treatment with a named model (process, CBT/skills, psychoeducation, or specialist package). Know the evidence map for depression, anxiety/SAD, PTSD, schizophrenia-adjunct groups, and BPD multiperson programmes. Protect safety and confidentiality limits. Use groups to expand access without diluting clinical standards — and never use the circle as a warehouse for patients who need individual containment first.[2][3][8][4][12]
References
- [1]Burlingame GM, McClendon DT, Yang C Cohesion in group therapy: A meta-analysis Psychotherapy (Chic), 2018.PMID 30335452
- [2]Burlingame GM, Seebeck JD, Janis RA, et al. Outcome differences between individual and group formats when identical and nonidentical treatments, patients, and doses are compared: A 25-year meta-analytic perspective Psychotherapy (Chic), 2016.PMID 27918191
- [3]Rosendahl J, Alldredge CT, Burlingame GM, Strauss B Recent Developments in Group Psychotherapy Research Am J Psychother, 2021.PMID 33745284
- [4]Barkowski S, Schwartze D, Strauss B, et al. Efficacy of group psychotherapy for anxiety disorders: A systematic review and meta-analysis Psychother Res, 2020.PMID 32093586
- [5]Barkowski S, Schwartze D, Strauss B, et al. Efficacy of group psychotherapy for social anxiety disorder: A meta-analysis of randomized-controlled trials J Anxiety Disord, 2016.PMID 26953823
- [6]Schwartze D, Barkowski S, Strauss B, et al. Efficacy of group psychotherapy for posttraumatic stress disorder: Systematic review and meta-analysis of randomized controlled trials Psychother Res, 2019.PMID 29179647
- [7]Burlingame GM, Svien H, Hoppe L, Hunt I, Rosendahl J Group therapy for schizophrenia: A meta-analysis Psychotherapy (Chic), 2020.PMID 32478561
- [8]Huntley AL, Araya R, Salisbury C Group psychological therapies for depression in the community: systematic review and meta-analysis Br J Psychiatry, 2012.PMID 22383765
- [9]Okumura Y, Ichikura K Efficacy and acceptability of group cognitive behavioral therapy for depression: a systematic review and meta-analysis J Affect Disord, 2014.PMID 24856569
- [10]Bloch S, Crouch E, Reibstein J Therapeutic factors in group psychotherapy. A review Arch Gen Psychiatry, 1981.PMID 7235852
- [11]Hoag MJ, Burlingame GM Evaluating the effectiveness of child and adolescent group treatment: a meta-analytic review J Clin Child Psychol, 1997.PMID 9292381
- [12]Bateman A, Fonagy P Effectiveness of partial hospitalization in the treatment of borderline personality disorder: a randomized controlled trial Am J Psychiatry, 1999.PMID 10518167
- [13]Bateman A, Fonagy P 8-year follow-up of patients treated for borderline personality disorder: mentalization-based treatment versus treatment as usual Am J Psychiatry, 2008.PMID 18347003
- [14]Linehan MM, Armstrong HE, Suarez A, Allmon D, Heard HL Cognitive-behavioral treatment of chronically parasuicidal borderline patients Arch Gen Psychiatry, 1991.PMID 1845222
- [15]Linehan MM, Korslund KE, Harned MS, et al. Dialectical behavior therapy for high suicide risk in individuals with borderline personality disorder: a randomized clinical trial and component analysis JAMA Psychiatry, 2015.PMID 25806661
- [16]Cuijpers P, Noma H, Karyotaki E, Cipriani A, Furukawa TA Effectiveness and Acceptability of Cognitive Behavior Therapy Delivery Formats in Adults With Depression: A Network Meta-analysis JAMA Psychiatry, 2019.PMID 30994877
- [17]Joyce AS, Piper WE, Ogrodniczuk JS Therapeutic alliance and cohesion variables as predictors of outcome in short-term group psychotherapy Int J Group Psychother, 2007.PMID 17661544