Psych · psychotherapy
Interpersonal psychotherapy (IPT)
Also known as IPT · Interpersonal therapy · Klerman Weissman IPT · IPT-A · IPT-M · IPSRT · Interpersonal counselling · IPC
Exam-exhaustive fellowship reference on interpersonal psychotherapy — medical model, sick role, four problem areas, phase structure, communication analysis, adaptations (IPT-A, perinatal, IPT-M, IPSRT, PTSD), landmark trials and meta-analyses, combined care with antidepressants, and CASC/MEQ technique. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Fellowship examiners expect you to select a focus, sketch an interpersonal inventory, run communication analysis, explain the sick role, cite TDCRP / Cuijpers / perinatal / IPT-A / IPSRT / PTSD landmarks, and integrate antidepressants without false dichotomies.[2][4][10]
Definition and scope
IPT was developed by Klerman, Weissman and colleagues in the 1970s as a structured psychological treatment for depression that could be manualised and tested alongside medication.[1][7] It is not classical psychoanalysis: free association and reconstruction of childhood conflict are not the method. It is not CBT: automatic thoughts and behavioural experiments are not the primary change tools, though some patients receive both modalities over a care pathway.
Two organising principles
- Medical model of depression — symptoms are named as illness; blame is externalised from character to treatable syndrome.
- Interpersonal formulation — recent life events and relationship patterns (loss, conflict, role change, isolation) are linked to onset and maintenance of the episode.[7]
The sick role (exam favourite)
In the initial phase the therapist may grant a temporary sick role: the patient is relieved of some social expectations while being mobilised to seek help, adhere to treatment, and work toward recovery — not chronic invalidism or permanent exemption from all roles.[7]
What IPT is and is not
| IPT is | IPT is not |
|---|---|
| Time-limited with explicit ending | Open-ended supportive chat |
| Present- and future-focused | Primary free-association analysis of childhood |
| Focused on one primary interpersonal problem area | Scattershot multi-problem counselling |
| Affective work on recent interpersonal episodes | Pure cognitive restructuring manuals |
| Compatible with antidepressants | An anti-medication ideology |
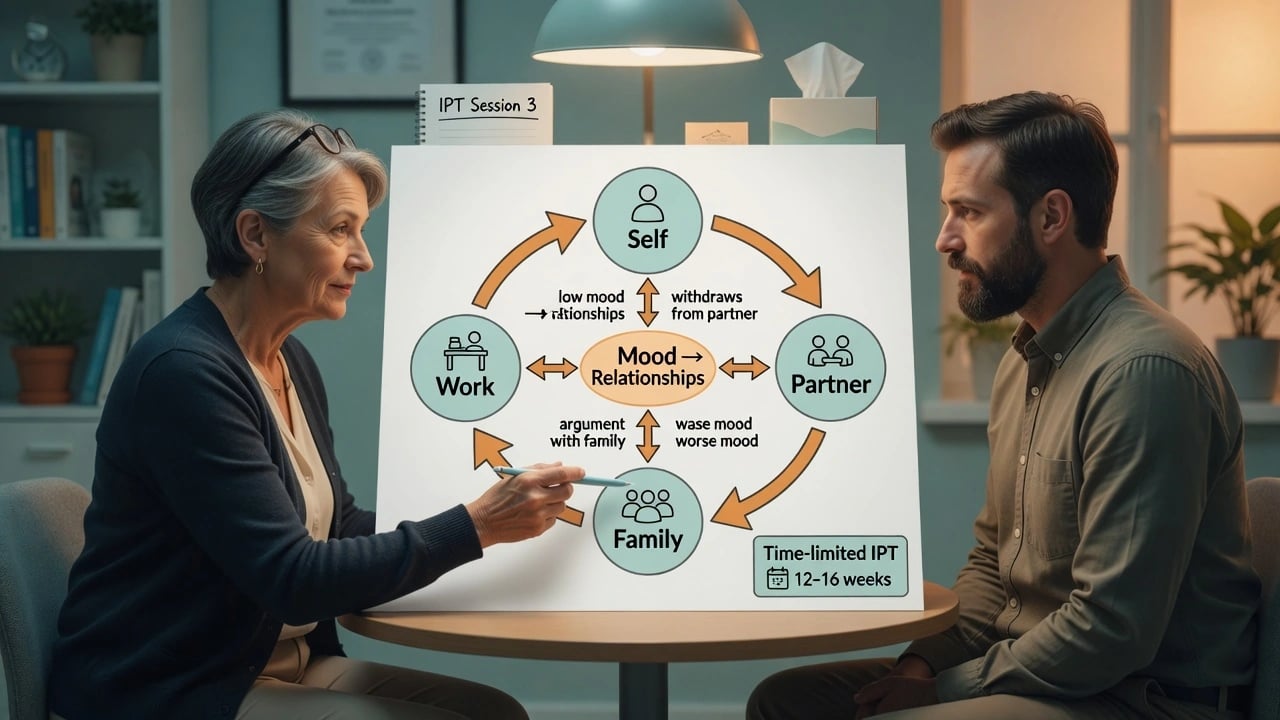
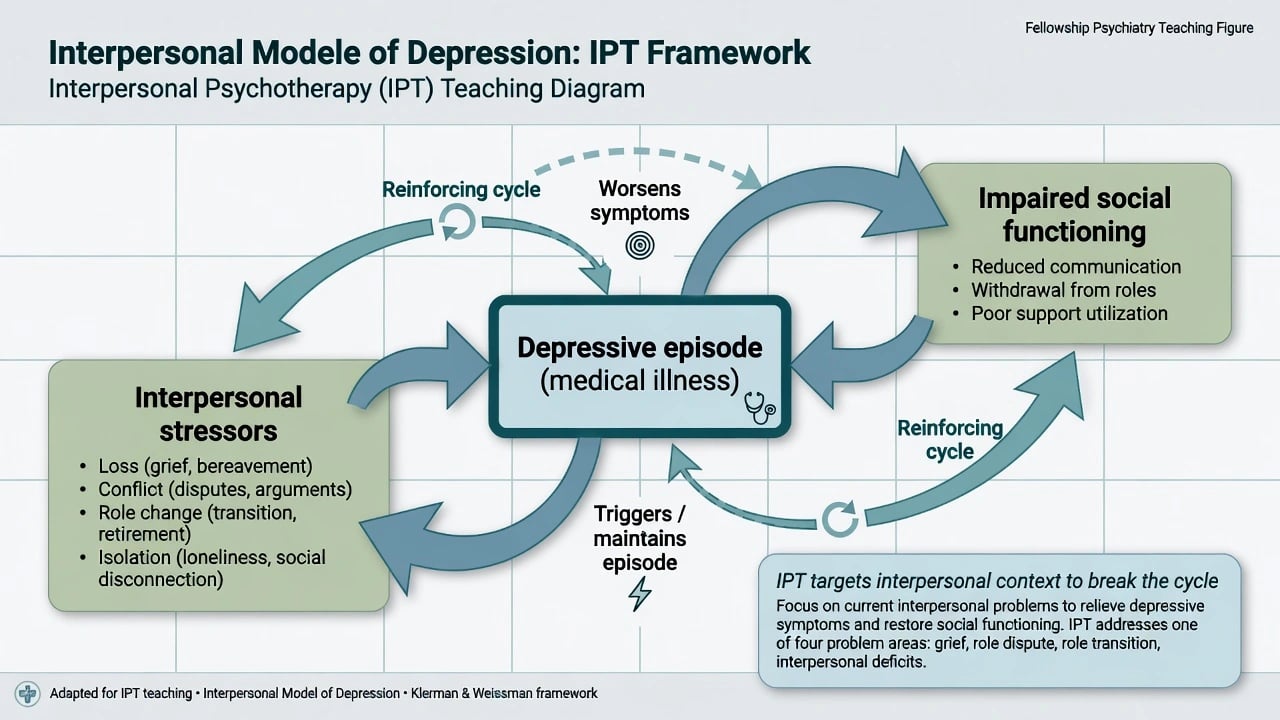
Interpersonal model (mechanisms)
Depression both arises from and worsens interpersonal functioning. Loss, chronic conflict, forced role change, and sparse support increase episode risk; once depressed, withdrawal, irritability, and role failure reduce support further — a reinforcing cycle. IPT interrupts the cycle by clarifying the interpersonal problem, improving communication and social support, and mobilising the sick role while symptoms are treated as medical illness.[7][4]
For bipolar disorder, IPSRT adds the social zeitgeber idea: irregular sleep–wake, meal, and activity rhythms destabilise circadian systems and increase episode risk; therapy stabilises routines and works interpersonal triggers.[14][12]
Four problem areas (classification)
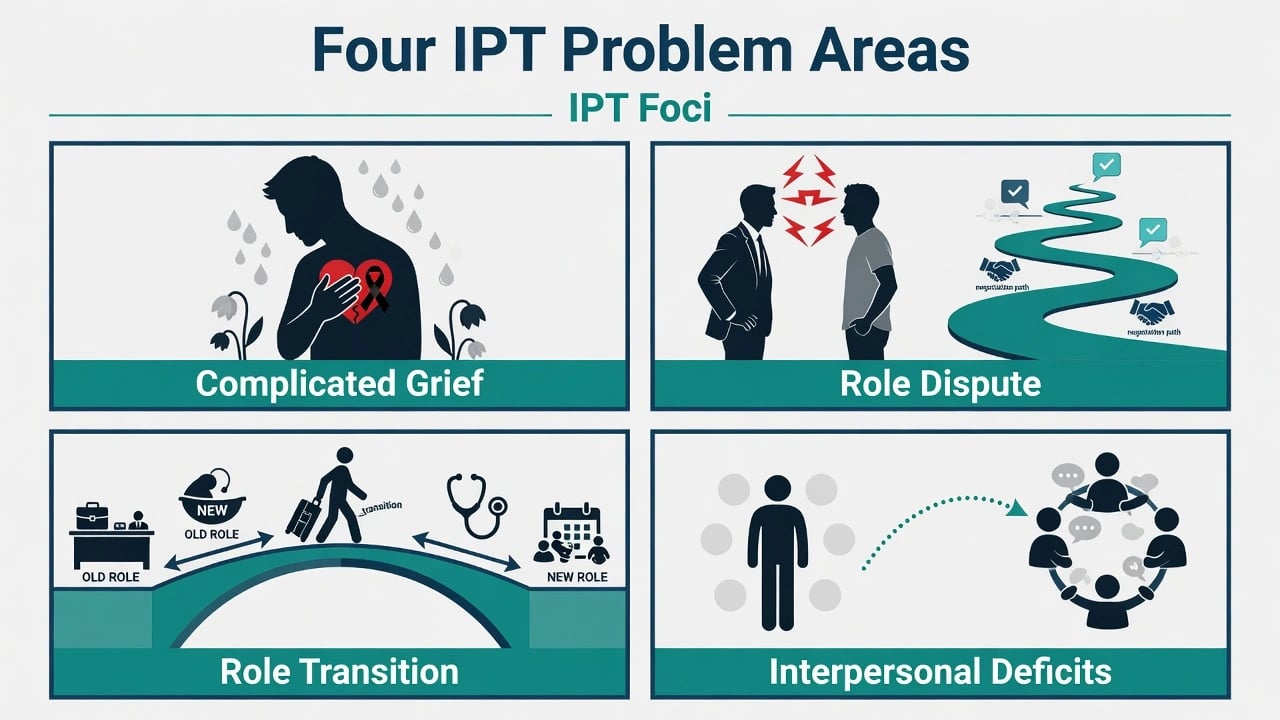
1. Complicated grief
Abnormal, delayed, or inhibited mourning after death (or sometimes other major losses framed as grief). Middle-phase work facilitates mourning, reviews the relationship realistically (ambivalence included), and rebuilds social connection. Distinguish from prolonged grief disorder pathways that may need specialised grief-focused packages when criteria are met — still map the interpersonal loss carefully.[7]
2. Interpersonal role disputes
Nonreciprocal expectations in a key relationship (partner, parent, boss). Stages often taught: renegotiation possible → impasse → dissolution. Techniques include clarifying wants, communication analysis, and decision about whether to repair or exit safely. Always screen for intimate partner violence before homework that escalates confrontation.[7]
3. Role transitions
Difficulty adapting to a new role: parenthood, job loss, migration, retirement, medical illness role, divorce, coming out, leaving home. Work: mourn the old role, identify gains and losses, build skills and supports for the new role.[7][10]
4. Interpersonal deficits (sensitivity)
Sparse or unsatisfying relationships; loneliness; limited social skills or chronic isolation. Often the default when no clear recent event — harder focus; build a small network carefully, use therapy relationship carefully as practice without converting IPT into open-ended personality reconstruction.[7]
Course and session structure
Typical acute IPT for depression is about 12–16 weekly sessions (adaptations vary). State the time limit from the start so termination is part of the treatment, not a surprise.[7][4]
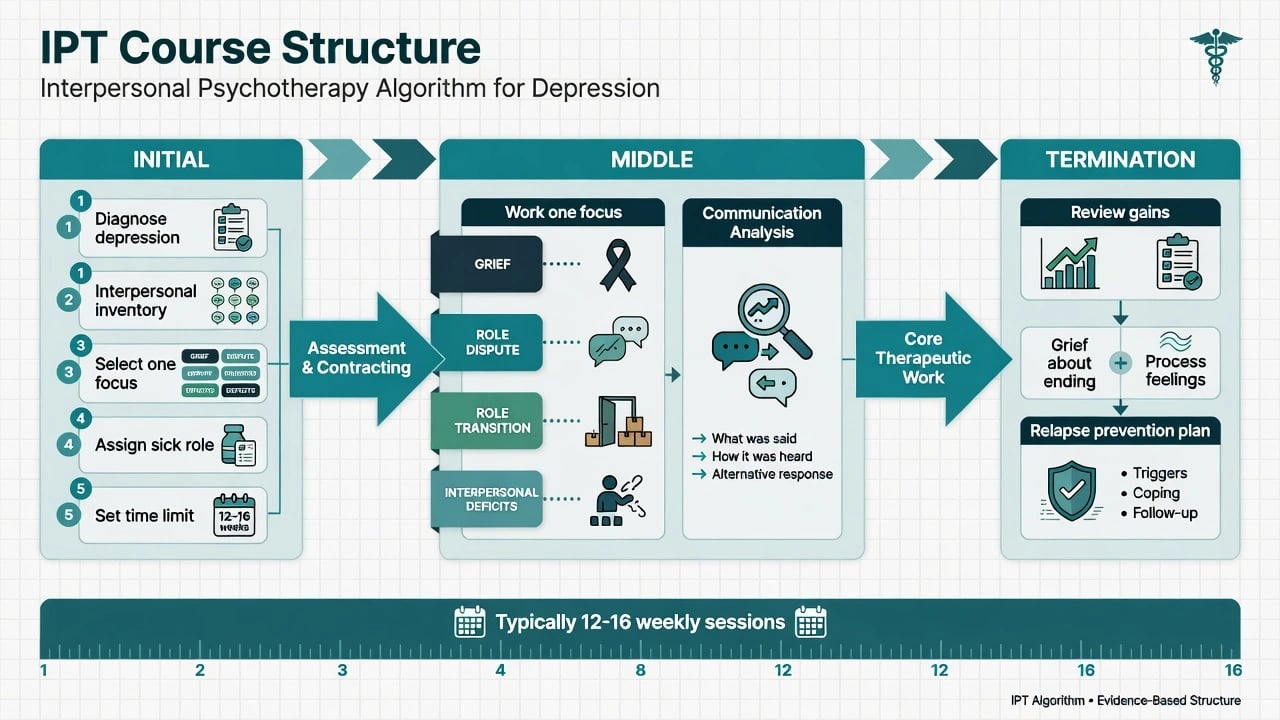
Initial phase (roughly sessions 1–3)
- Confirm depressive (or other) diagnosis and severity; complete risk assessment.
- Explain the medical model and grant temporary sick role.
- Complete interpersonal inventory (map key relationships, recent events, patterns of expectation and communication).
- Select one primary problem area temporally linked to the episode.
- Set goals and review whether medication is indicated (severity, preference, prior response, access).[7][2]
Middle phase
Stay on the focus. Core technique: communication analysis — reconstruct a recent interpersonal episode in detail (what was said, felt, intended; how it was heard; options for clearer needs and affect expression). Use role play when helpful. Affect is welcomed; the goal is interpersonal change that supports symptom remission.[7]
Termination phase
Treat ending as a role transition and sometimes a small loss. Review gains, name interpersonal early-warning signs, plan boosters or maintenance if recurrent, and process feelings about ending rather than avoiding them.[7][3]
Evidence base (high-yield landmarks)
Adult depression
Meta-analysis shows IPT efficaciously treats depression, with meaningful effects versus control conditions and a place among first-line psychological treatments.[4][6] A broader comprehensive meta-analysis supports IPT for depression and selected other mental health problems, with signals for prevention of new episodes and relapse in some contexts.[5]
NIMH TDCRP (Elkin 1989)
Four arms for outpatient depression: IPT, CBT, imipramine + clinical management, and placebo + clinical management. Overall message for exams: brief structured psychotherapies and medication are effective treatments in this research tradition; historical debates about severity interactions exist, but do not claim “IPT failed.” Use as comparative efficacy context, not a single slogan.[2]
Maintenance (Frank 1990)
In recurrent depression, after acute/continuation response, a three-year maintenance trial informed the field on pharmacotherapy maintenance and maintenance IPT (IPT-M) strategies — long-horizon relapse prevention matters after remission.[3]
Adolescents (IPT-A)
IPT adapted for depressed adolescents shows efficacy versus control and effectiveness in school-based clinics versus treatment as usual — developmentally relevant role transitions and parent involvement are built into the model.[8][9]
Perinatal
Postpartum IPT reduced depressive symptoms and improved social adjustment versus wait-list in a landmark RCT.[10] Antenatal IPT outperformed a parenting education control for depressed pregnant women in a controlled trial — important when patients prefer non-pharmacological options or when combined care is planned.[11]
Bipolar — IPSRT
Interpersonal and social rhythm therapy, as adjunctive psychosocial treatment, has two-year outcome data supporting attention to routine stability and interpersonal triggers alongside pharmacotherapy.[12][14]
PTSD
A randomised trial of IPT for PTSD found meaningful improvement and positioned IPT as a non-exposure alternative relative to prolonged exposure for some patients — know this as an adaptation, not the default first-line trauma protocol in every guideline.[13]
Differential and modality choice
- IPT vs CBT: both first-line for many depressive presentations; choose by formulation (interpersonal trigger/focus vs cognitive-behavioural maintaining cycles), patient preference, comorbidity (OCD/panic often favour CBT/ERP), and local access/supervision.[4][2]
- IPT vs psychodynamic: IPT is shorter, medical-model, focus-limited, present-oriented; dynamic work may suit longer exploratory goals when indicated and available.
- IPT vs supportive: supportive psychotherapy is a broader ego-strengthening continuum; IPT has manualised foci and termination structure.[7]
- IPT vs IPSRT: IPSRT is the bipolar-adapted package with social rhythm metrics — do not call standard depression IPT “IPSRT.”[14]
Assessment bedside checklist
- Diagnosis and differential (bipolar screen, psychosis, substance, medical, grief vs MDD).
- Risk (suicide, violence, self-neglect, safeguarding, IPV).
- Interpersonal inventory + timeline of episode onset.
- Primary focus selection with patient buy-in.
- Baseline measures (e.g. PHQ-9) and serial monitoring.
- Medication decision and shared care plan.
- Cultural formulation of roles, grief rituals, and family structure.[7][2]
Management — combined care and systems
When IPT is appropriate
Outpatient (or step-down) patients with depressive disorders (and selected adaptations) who can engage weekly, accept a time limit, and identify interpersonal material. Prefer combination with antidepressant when moderate–severe depression, prior partial response, melancholic features, or patient preference for dual modality.[2][4][1]
When IPT is not the priority today
Active high suicide risk needing containment, mania/mixed states requiring medical priority, delirium/organic syndromes, severe substance intoxication, or situations where exposure-based trauma work is indicated and accepted and IPT-PTSD is not the local pathway.[13]
Regional guidance (exam language)
NICE-style stepped care commonly lists IPT among evidence-based psychological therapies for depression; APA guidance likewise recognises IPT for MDD; FRANZCP training expects psychological therapy competence and formulation-based modality choice rather than brand loyalty. Always match local service pathways, waiting times, and supervised competence.[4][5]
Disposition ladder
Primary care / IPC brief forms → outpatient IPT with supervision → CMHT shared care for complexity/risk → brief admission for safety only, with psychotherapy resumed when stable. Group IPT and culturally adapted implementations exist; fidelity still requires focus and structure.[5][7]
Adaptations map
| Adaptation | Population | Exam pearl |
|---|---|---|
| IPT-A | Depressed adolescents | Efficacy + school-based effectiveness; parents/school roles matter.[8][9] |
| Perinatal IPT | Pregnancy / postpartum | Strong psychological option; O’Hara, Spinelli landmarks.[10][11] |
| IPT-M | Recurrent depression after recovery | Maintenance dosing of sessions; Frank lineage.[3] |
| IPSRT | Bipolar I (adjunct) | Social rhythms + interpersonal foci + meds.[12][14] |
| IPT for PTSD | PTSD (selected) | Non-exposure alternative in Markowitz RCT.[13] |
| IPC | Primary care / milder | Briefer interpersonal counselling derivative.[7] |
Complications and safety traps
- IPV: communication homework can increase danger — safety plan first.
- Sick role misuse: temporary support must not become permanent avoidance of recovery tasks.
- Therapist drift: losing the focus, skipping inventory, or infinite extensions without review.
- Boundary expansion: dispute work is not covert couple therapy without consent and frame.
- Premature deep trauma processing outside the chosen model when stabilisation is needed. [7] [1]
Exam traps (rapid fire)
- Inventing a fifth classic problem area called “trauma” — trauma-related presentations may map to grief/transition/dispute, or use the PTSD adaptation deliberately.[13]
- Claiming IPT is only for mild depression — meta-analysis and comparative trials support broader use with meds when needed.[2][4]
- Claiming IPT forbids discussion of the past (past informs inventory; work stays present).[1]
- Equating IPT with CBT or with open psychodynamic therapy.[1][7]
- Forgetting termination as active phase.[7]
- Misreading TDCRP as negative for IPT overall.[2]
CASC / viva technique snippets
Plain-language opener: “Your low mood is a real illness, not a weakness. In IPT we look at how recent stresses in relationships — loss, conflict, big life changes, or isolation — are tied to this episode, and we work for a set number of weeks on that focus so symptoms ease and relationships work better.”[7]
Focus pitch (role transition postpartum): “Becoming a parent changed almost every role you hold. We will name what you have lost and gained, build supports, and practise asking for help without self-attack.”[10]
Combined care line: “Tablets and IPT often work together. Starting therapy is not a reason to stop medication without a planned medical review.”[2][1]
Bottom line for fellowship candidates
Deliver IPT as time-limited medical-model interpersonal work with inventory, one focus, communication analysis, and planned ending. Know the evidence ladder from depression meta-analyses through perinatal, adolescent, maintenance, IPSRT, and PTSD adaptations. Combine with pharmacotherapy when severity or preference demands it. Never sacrifice risk, capacity, or safety for modality purity.[4][5][7]
References
- [1]Klerman GL, DiMascio A, Weissman M, Prusoff B, Paykel ES Treatment of depression by drugs and psychotherapy Am J Psychiatry, 1974.PMID 4587807
- [2]Elkin I, Shea MT, Watkins JT, et al. National Institute of Mental Health Treatment of Depression Collaborative Research Program. General effectiveness of treatments Arch Gen Psychiatry, 1989.PMID 2684085
- [3]Frank E, Kupfer DJ, Perel JM, et al. Three-year outcomes for maintenance therapies in recurrent depression Arch Gen Psychiatry, 1990.PMID 2244793
- [4]Cuijpers P, Geraedts AS, van Oppen P, et al. Interpersonal psychotherapy for depression: a meta-analysis Am J Psychiatry, 2011.PMID 21362740
- [5]Cuijpers P, Donker T, Weissman MM, Ravitz P, Cristea IA Interpersonal Psychotherapy for Mental Health Problems: A Comprehensive Meta-Analysis Am J Psychiatry, 2016.PMID 27032627
- [6]de Mello MF, de Jesus Mari J, Bacaltchuk J, Verdeli H, Neugebauer R A systematic review of research findings on the efficacy of interpersonal therapy for depressive disorders Eur Arch Psychiatry Clin Neurosci, 2005.PMID 15812600
- [7]Markowitz JC, Weissman MM Interpersonal psychotherapy: principles and applications World Psychiatry, 2004.PMID 16633477
- [8]Mufson L, Weissman MM, Moreau D, Garfinkel R Efficacy of interpersonal psychotherapy for depressed adolescents Arch Gen Psychiatry, 1999.PMID 10359475
- [9]Mufson L, Dorta KP, Wickramaratne P, et al. A randomized effectiveness trial of interpersonal psychotherapy for depressed adolescents Arch Gen Psychiatry, 2004.PMID 15184237
- [10]O'Hara MW, Stuart S, Gorman LL, Wenzel A Efficacy of interpersonal psychotherapy for postpartum depression Arch Gen Psychiatry, 2000.PMID 11074869
- [11]Spinelli MG, Endicott J Controlled clinical trial of interpersonal psychotherapy versus parenting education program for depressed pregnant women Am J Psychiatry, 2003.PMID 12611838
- [12]Frank E, Kupfer DJ, Thase ME, et al. Two-year outcomes for interpersonal and social rhythm therapy in individuals with bipolar I disorder Arch Gen Psychiatry, 2005.PMID 16143731
- [13]Markowitz JC, Petkova E, Neria Y, et al. Is Exposure Necessary? A Randomized Clinical Trial of Interpersonal Psychotherapy for PTSD Am J Psychiatry, 2015.PMID 25677355
- [14]Frank E, Swartz HA, Kupfer DJ Interpersonal and social rhythm therapy: managing the chaos of bipolar disorder Biol Psychiatry, 2000.PMID 11018230