Psych · Psychotherapy
Mentalisation-based treatment
Also known as Mentalization-based treatment · MBT · Mentalization based therapy · Mentalisation based therapy · MBT-A · Partial hospitalisation mentalization · Reflective function therapy
Exam-exhaustive fellowship reference on mentalisation-based treatment (MBT): definition of mentalising, pre-mentalising modes, attachment-arousal model, not-knowing stance, individual-plus-group structure, landmark Bateman/Fonagy trials, MBT-A and ASPD extensions, comparators (DBT, SCM/GPM, schema, TFP), and stepped care. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Fellowship exams test whether you can define mentalising, name the three pre-mentalising modes, link attachment arousal to clinical crises, outline MBT structure and stance, cite Bateman/Fonagy evidence (including SCM comparison), and choose MBT vs DBT vs structured generalist care without fidelity myths.[4][7][14]
Definition and classification
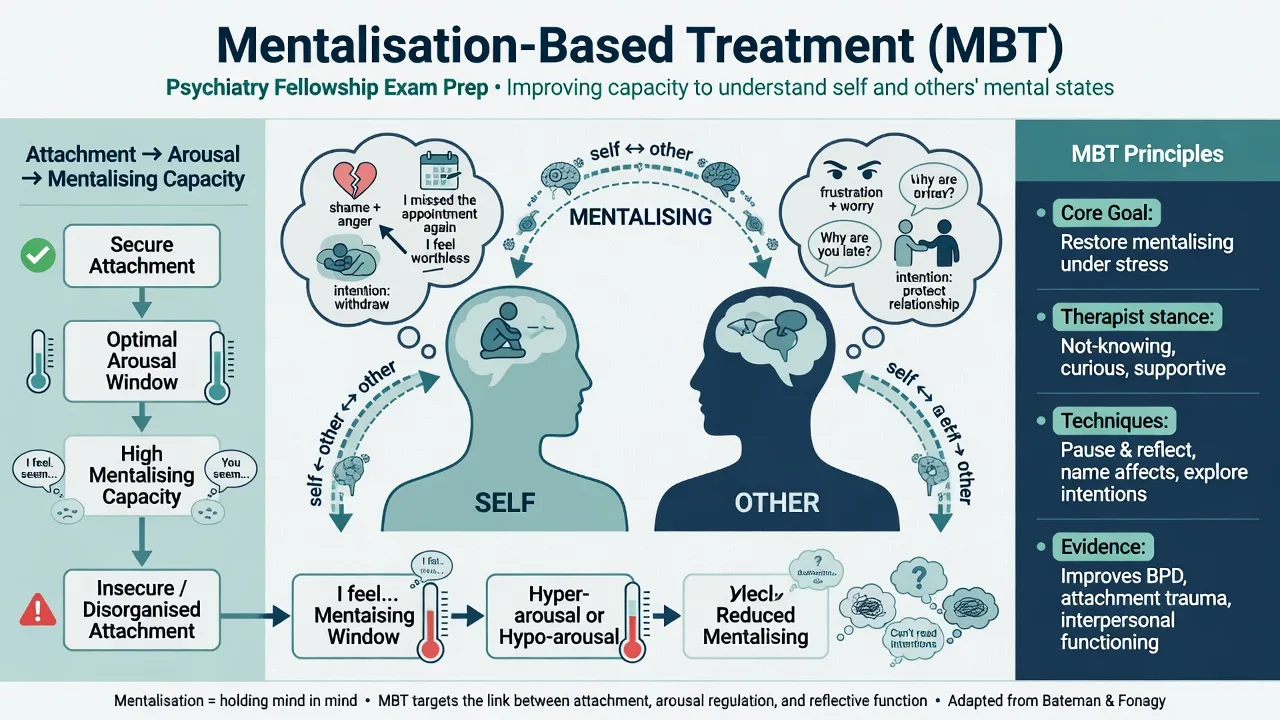
Mentalising (mentalization) is the imaginative activity of interpreting human behaviour as underpinned by mental states. It can be implicit (automatic) or explicit (reflective), about self or other, and more cognitive or affective. It is related to reflective function in developmental theory and is context-sensitive: robust in calm states, fragile under threat, shame, or abandonment cues.[5][6][7]
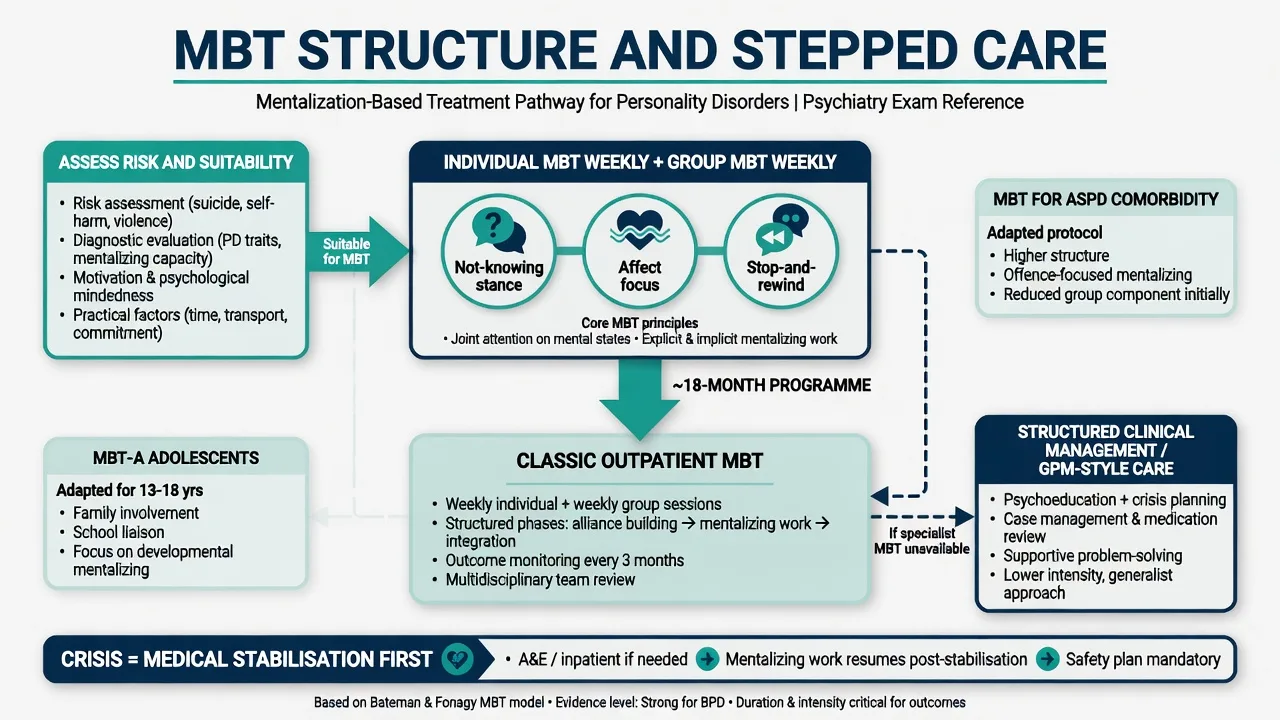
MBT is not “any psychodynamic chat.” It is a time-structured programme with explicit goals to restore and stabilise mentalising in high-arousal interpersonal contexts, using a not-knowing stance, affect focus, and dual individual + group formats in standard adult models.[4][6]
| Format / variant | Core idea | Exam anchor |
|---|---|---|
| Partial hospitalisation / day MBT | Intensive multimodal day programme | Bateman 1999/2001/2008 lineage |
| Outpatient adult MBT | Weekly individual + weekly group (classic ~18 months) | Bateman 2009 vs SCM |
| MBT-A | Adolescent adaptation, often with family work | Rossouw and Fonagy 2012 |
| MBT for ASPD ± BPD | Mentalising violence, other minds, obligation | Bateman 2016; forensic extensions |
| MBT-FACTS | Family/carer mentalising intervention | Bateman and Fonagy 2019 |
Pre-mentalising modes (classification of collapse)
When mentalising fails, people often shift into pre-mentalising modes that organise BPD crises and therapy stuckness.[5][7]
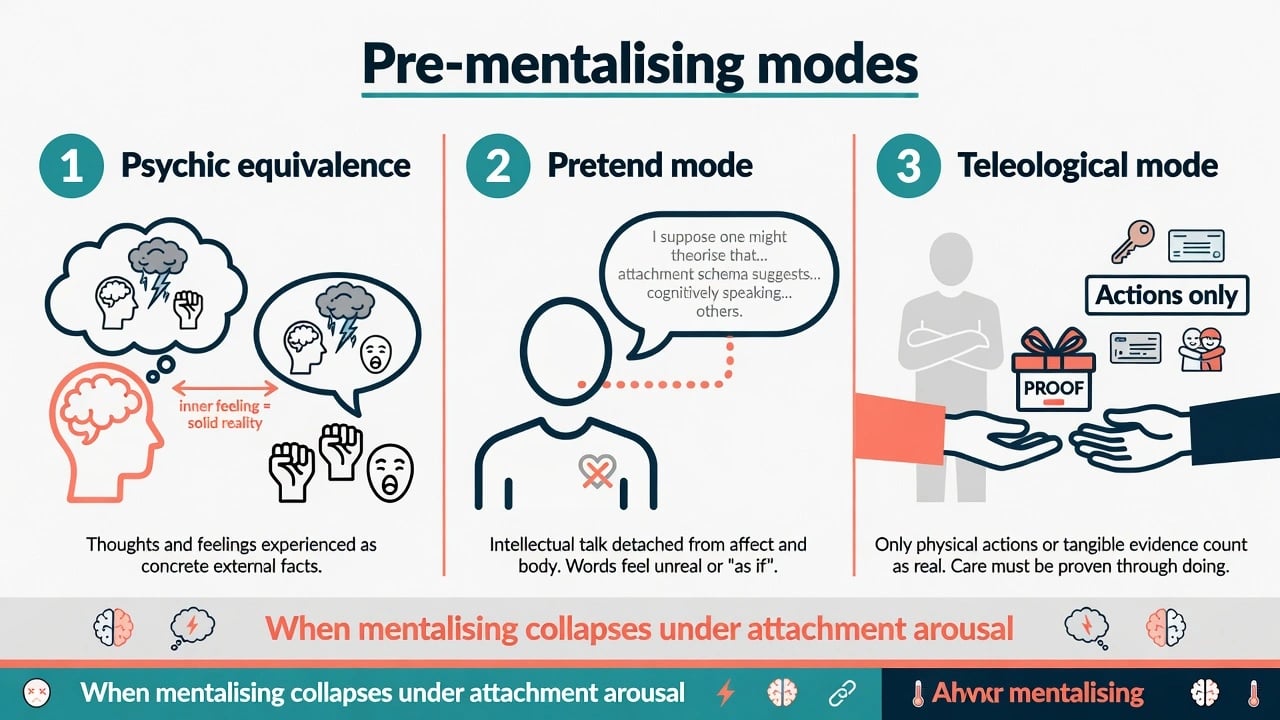
- Psychic equivalence — inner experience is treated as external fact (“I feel abandoned, therefore you abandoned me”; absolute certainty of rejection or contamination by emotion).
- Pretend mode — mental talk is decoupled from real affect and reality (clever, empty, intellectualised discourse that changes nothing).
- Teleological mode — only observable actions count as evidence of mental states (“If you cared, you would text me / keep me in hospital / prescribe X”).
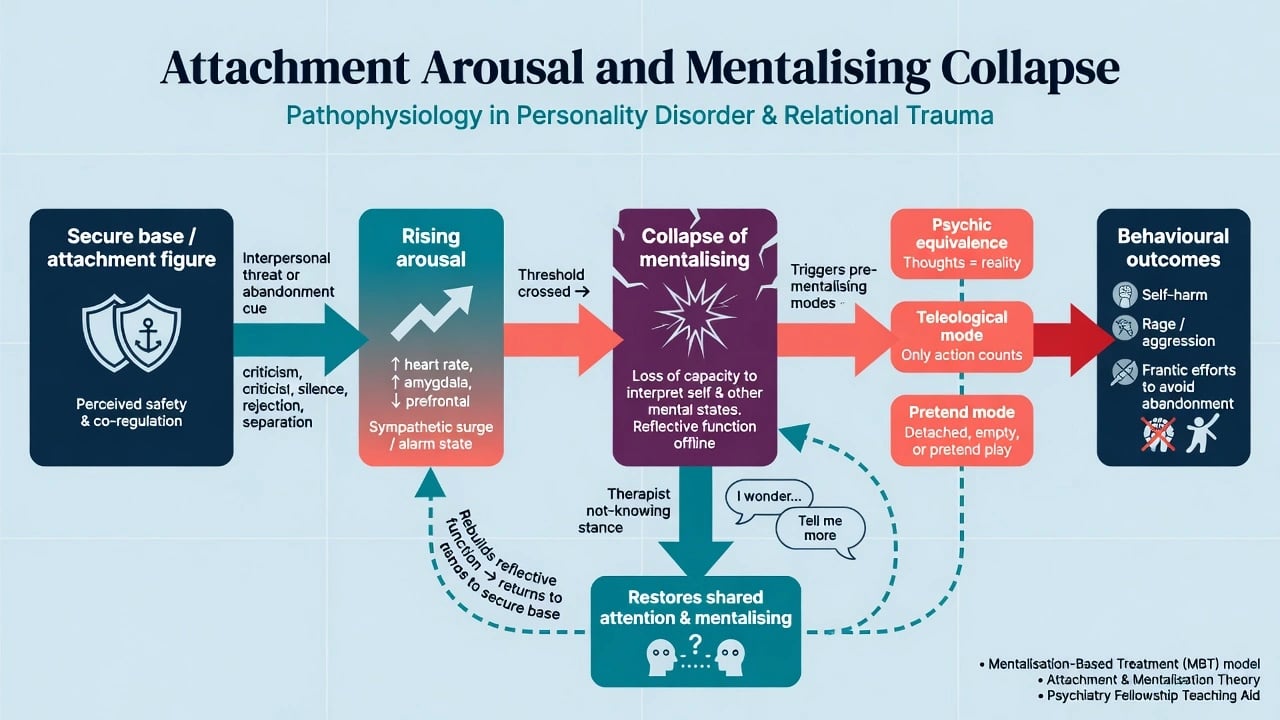
Mechanism: attachment, arousal, mentalising collapse
Developmental MBT theory holds that secure attachment scaffolds the capacity to represent mind; adversity, trauma, and disorganised attachment undermine robust mentalising, especially in intimate or threatening relationships.[7]
Under attachment hyperactivation (fear of abandonment, rejection sensitivity) or extreme arousal, mentalising capacity drops. Behaviour then becomes organised by pre-mentalising modes, increasing risk of self-harm, rage, frantic contact, or abrupt cut-off. Therapy aims to lower arousal enough to restore mentalising and to practice it where it usually fails — close relationships, including the therapeutic relationship.[5][6][7]
Common-factors reading: mentalising is also framed as a mechanism through which good BPD treatment works (alliance, structure, epistemic trust), not only a brand-specific trick.[17]
Clinical presentation and bedside assessment
Typical referral profile: BPD or severe personality pathology with affective storms lasting hours, identity instability, chaotic relationships, recurrent self-harm or suicidality, and repeated mentalising failures after perceived rejection. MSE and history often show rapid shifts from idealisation to devaluation, mind-reading accusations, and teleological tests of care.[6][7]
Assess suitability for MBT (typical): interpersonal dysregulation with mentalising failures; ability (with support) to attend individual and group; willingness to explore mind rather than only suppress symptoms; and service capacity for a structured dual-format programme.[4][6]
Always assess and document: current suicide/self-harm risk; violence risk (especially ASPD comorbidity); substance use; trauma/dissociation load; psychosis/mania that needs medical priority; neurodivergence (adapt language — do not equate autism with BPD); cultural models of self and mind; practical barriers to dual attendance.[6][9]
Investigations do not diagnose mentalising failure. Track outcomes with self-harm frequency, hospital days, interpersonal crises, and symptom scales; research settings may use reflective-function or mentalising measures.[4][11]
Standard MBT structure and techniques
Structure
Classic outpatient adult MBT combines weekly individual sessions with weekly group therapy, often over about 18 months in research protocols (local duration varies). Earlier evidence came from psychoanalytically oriented partial hospitalisation programmes that became the MBT lineage.[1][4][6]
Group provides multiple minds, live interpersonal arousal, and practice of other-mentalising. Individual work personalises formulation, repairs ruptures, and tracks crises without replacing emergency care.[4][6]
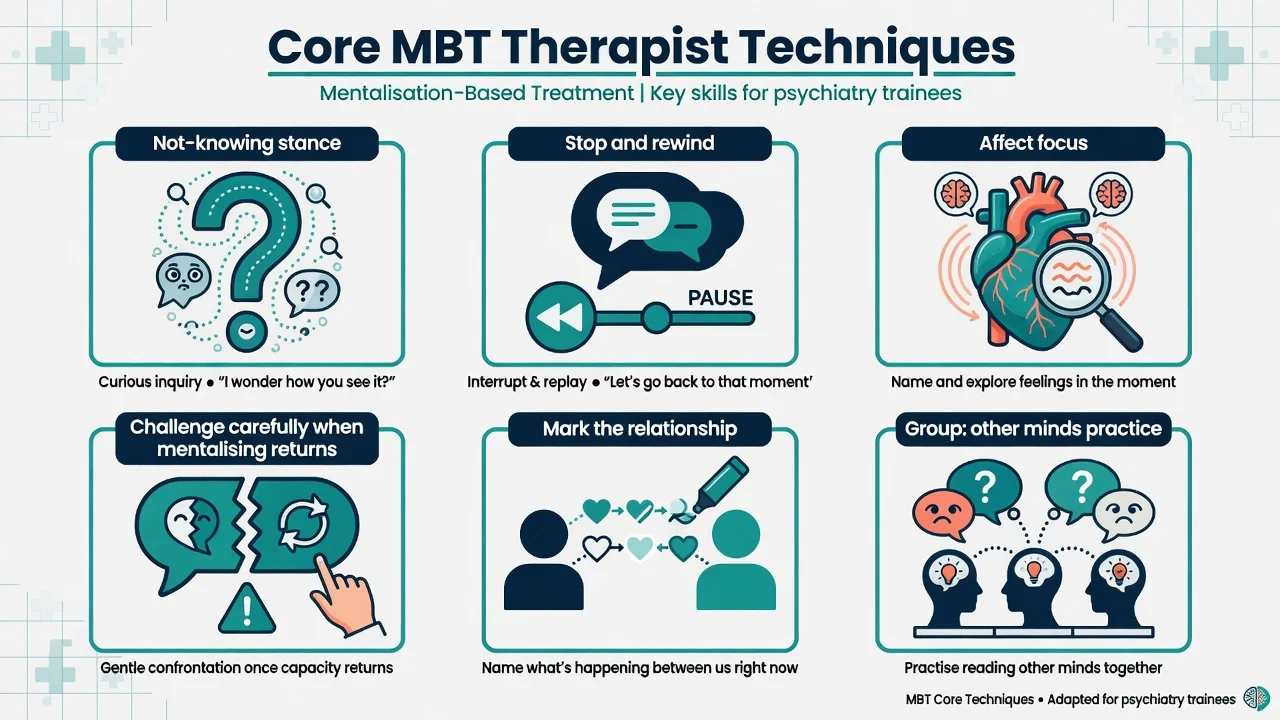
Therapist stance and techniques
- Not-knowing / inquisitive curiosity — share uncertainty; avoid premature certainty about the patient’s mind.
- Stop and rewind — pause interaction when mentalising is lost; reconstruct what just happened in mental-state terms.
- Affect focus — prioritise feeling states over intellectual content when pretend mode dominates.
- Challenge — only when some mentalising has returned; avoid challenges that spike arousal further.
- Mark the relationship — carefully mentalise what is happening between patient and therapist without heavy classical interpretation early.
- Team mentalising — staff meetings that model curiosity about the patient and about countertransference, reducing splitting and pejorative culture.[5][6][17]
Acute care and definitive management
Acute / resuscitation of the mentalising frame
Medical stabilisation and standard risk assessment outrank therapy vocabulary after overdose, serious self-injury, or imminent suicide risk. Once safe, help the person mentalise the crisis sequence without blame: vulnerability factors, interpersonal trigger, collapse mode, behaviour, and aftermath. Avoid iatrogenic non-mentalising (punitive discharge language, staff certainty that “this is manipulative”).[4][6][12]
Definitive and stepped pathway
| Presentation | Prefer |
|---|---|
| BPD with recurrent self-harm and mentalising failures; dual format acceptable | Comprehensive outpatient MBT if available |
| Same, specialist MBT unavailable | Structured clinical management / GPM-style: scheduled sessions, crisis plan, psychoeducation, treat comorbidities, clear goals |
| Adolescent self-harm with interpersonal crises | MBT-A pathway (or other evidence-based youth programmes per local service) |
| BPD + ASPD with aggression/offending context | Adapted MBT where available; structured risk management always |
| Family trapped in non-mentalising cycles | Consider family mentalising intervention (MBT-FACTS principles) as adjunct |
| Preference/match for skills-heavy Stage 1 focus | DBT or skills-informed structured care (not a pejorative “instead of”) |
Medication: no drug cures BPD or replaces mentalising work. Treat comorbid depression, anxiety, ADHD, substance use, sleep, and medical sequelae thoughtfully; avoid polypharmacy as pseudo-therapy.[11][12]
Comparators and differentials
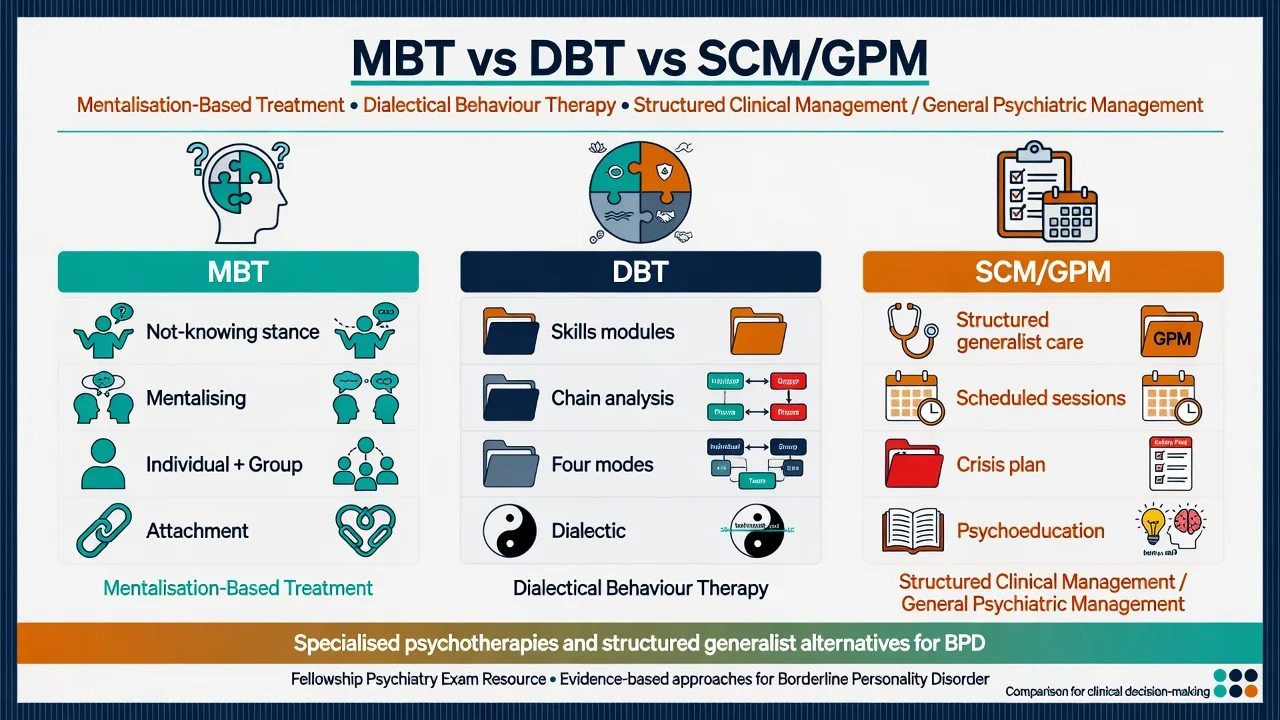
- Primary aim: restore mentalising under attachment arousal
- Not-knowing stance; pre-mentalising modes
- Classic individual + group dual format
- Primary aim: emotion regulation and behavioural control
- Four modes; skills modules; chain analysis
- Dialectic of acceptance and change
- Structured generalist psychiatric care
- Scheduled sessions, crisis plans, psychoeducation
- Key active comparator in Bateman 2009 / McMain teaching
Also distinguish schema therapy and transference-focused psychotherapy (TFP) as specialised alternatives with different focal mechanisms (early maladaptive schemas / object relations), supported by comparative trial literature outside the MBT brand.[16]
Barnicot and Crawford compared DBT versus MBT in routine care settings — know that both specialised approaches can help, and choice may depend on availability, fit, and clinical match rather than brand loyalty.[14]
Landmark evidence
Bateman and Fonagy programme trials
- 1999: partial hospitalisation programme superior to standard psychiatric care for BPD on multiple clinical outcomes in a randomised trial — foundational specialised-programme evidence.[1]
- 2001: 18-month follow-up maintained and extended benefits after the partial hospitalisation programme.[2]
- 2008: 8-year follow-up showed lasting advantages versus treatment-as-usual for many key outcomes after the original MBT partial hospitalisation pathway.[3]
- 2009: outpatient MBT versus structured clinical management (SCM) — MBT superior on several primary outcomes including self-harm trajectories in the trial analysis; this is the core specialised-versus-structured-generalist teaching paper for MBT.[4]
Extensions and meta-analyses
- Mechanisms and model papers: Fonagy and Bateman on change mechanisms; Fonagy and Luyten developmental mentalisation model of BPD.[5][7]
- MBT-A (2012): RCT of mentalization-based treatment for adolescent self-harm — reductions in self-harm and depression versus treatment-as-usual in that trial context.[8]
- BPD + ASPD (2016): MBT versus SCM for comorbid borderline and antisocial personality disorder — specialised mentalising focus for a high-risk dual diagnosis group.[9]
- Families (2019): MBT-FACTS randomised trial for families of people with BPD.[10]
- Meta-analyses (2017–2022): specialised psychotherapies for BPD (including MBT among others) show overall efficacy versus control conditions, with heterogeneity and comparator-quality caveats.[11][12][13]
- Forensic/probation ASPD: large multicentre trial programmes continue to test mentalisation-based approaches in offending populations — know the existence of this research frontier without overclaiming local availability.[18]
Pitfalls, special populations, prognosis
Special populations. Adolescents: MBT-A evidence for self-harm; involve family mentalising where possible.[8] ASPD ± BPD: focus on other minds, violence sequences, and obligation without collusion.[9][18] Cultural care: curiosity about mind must respect kinship, spirituality, and collective selfhood — avoid imposing individualist mind-reading scripts.[7] Neurodivergence: distinguish lifelong social-communication differences from attachment-triggered mentalising collapse; adapt pace and language.[6] Perinatal: safety, bonding, sleep, and joint perinatal planning first; mentalise infant and self carefully.[6]
Prognosis and disposition. Specialised psychotherapies improve borderline-relevant outcomes and reduce self-harm relative to poorly structured care in aggregate evidence; individual response varies. Plan for step-down, crisis planning, residual skills/mentalising practice, and honest discussion of waitlists. Engagement, alliance, substance use, and therapist adherence influence outcome.[3][11][12][13]
Regional practice notes
ANZ (FRANZCP). Public services often lack full dual-format MBT. Examiners expect stepped-care reasoning: offer MBT when available and indicated; otherwise structured generalist care (SCM/GPM-style), clear crisis plans, treat comorbidities, and avoid therapeutic nihilism. Align with RANZCP themes that personality disorder is valid and treatable with structured psychological therapy. Do not invent mental health act section numbers.[4][11][15]
UK (MRCPsych). NICE-aligned teaching emphasises structured psychological treatments for BPD and self-harm pathways; MBT is a named specialised option in many services. CASC stations test engagement, not-knowing curiosity, and plain-language explanation of mentalising without jargon piles.[4][12]
US (ABPN). APA-aligned evidence supports specialised psychotherapies for BPD (MBT among several). Know outpatient vs partial hospital formats and generalist structured alternatives.[4][11]
Exam pearls
Pre-mentalising triad
Mentalising ≠ mind-reading as fact. High arousal collapses mentalising — restore safety first. Not-knowing stance is the therapist technology. Classic dual format: individual + group. Quote Bateman 2009 MBT vs SCM alongside McMain DBT vs GPM when discussing specialised versus structured generalist care. MBT-A has RCT evidence for adolescent self-harm. BPD+ASPD is examinable with 2016 data. MBT is not superior-by-brand to every alternative for every patient — match mechanism, access, and preference.[4][8][9][14][15]
References
See frontmatter PMIDs (title/year verified). Landmark anchors: Bateman and Fonagy 1999/2001/2008/2009; Fonagy and Bateman 2006; Fonagy and Luyten 2009; Rossouw and Fonagy 2012; Bateman et al. 2016; Bateman and Fonagy 2019 MBT-FACTS; Barnicot and Crawford 2019; Cristea 2017; Storebø Cochrane 2020; Stoffers-Winterling 2022; McMain 2009; Giesen-Bloo 2006; Bateman common-factors 2018; Fonagy MOAM 2025.[1][4][11]
References
- [1]Bateman A, Fonagy P Effectiveness of partial hospitalization in the treatment of borderline personality disorder: a randomized controlled trial Am J Psychiatry, 1999.PMID 10518167
- [2]Bateman A, Fonagy P Treatment of borderline personality disorder with psychoanalytically oriented partial hospitalization: an 18-month follow-up Am J Psychiatry, 2001.PMID 11136631
- [3]Bateman A, Fonagy P 8-year follow-up of patients treated for borderline personality disorder: mentalization-based treatment versus treatment as usual Am J Psychiatry, 2008.PMID 18347003
- [4]Bateman A, Fonagy P Randomized controlled trial of outpatient mentalization-based treatment versus structured clinical management for borderline personality disorder Am J Psychiatry, 2009.PMID 19833787
- [5]Fonagy P, Bateman AW Mechanisms of change in mentalization-based treatment of BPD J Clin Psychol, 2006.PMID 16470710
- [6]Bateman A, Fonagy P Mentalization based treatment for borderline personality disorder World Psychiatry, 2010.PMID 20148147
- [7]Fonagy P, Luyten P A developmental, mentalization-based approach to the understanding and treatment of borderline personality disorder Dev Psychopathol, 2009.PMID 19825272
- [8]Rossouw TI, Fonagy P Mentalization-based treatment for self-harm in adolescents: a randomized controlled trial J Am Acad Child Adolesc Psychiatry, 2012.PMID 23200287
- [9]Bateman A, O'Connell J, Lorenzini N, et al. A randomised controlled trial of mentalization-based treatment versus structured clinical management for patients with comorbid borderline personality disorder and antisocial personality disorder BMC Psychiatry, 2016.PMID 27577562
- [10]Bateman A, Fonagy P A randomized controlled trial of a mentalization-based intervention (MBT-FACTS) for families of people with borderline personality disorder Personal Disord, 2019.PMID 29999394
- [11]Cristea IA, Gentili C, Cotet CD, et al. Efficacy of Psychotherapies for Borderline Personality Disorder: A Systematic Review and Meta-analysis JAMA Psychiatry, 2017.PMID 28249086
- [12]Storebø OJ, Stoffers-Winterling JM, Völlm BA, et al. Psychological therapies for people with borderline personality disorder Cochrane Database Syst Rev, 2020.PMID 32368793
- [13]Stoffers-Winterling JM, Storebø OJ, Kongerslev MT, et al. Psychotherapies for borderline personality disorder: a focused systematic review and meta-analysis Br J Psychiatry, 2022.PMID 35088687
- [14]Barnicot K, Crawford M Dialectical behaviour therapy v. mentalisation-based therapy for borderline personality disorder Psychol Med, 2019.PMID 30303061
- [15]McMain SF, Links PS, Gnam WH, et al. A randomized trial of dialectical behavior therapy versus general psychiatric management for borderline personality disorder Am J Psychiatry, 2009.PMID 19755574
- [16]Giesen-Bloo J, van Dyck R, Spinhoven P, et al. Outpatient psychotherapy for borderline personality disorder: randomized trial of schema-focused therapy vs transference-focused psychotherapy Arch Gen Psychiatry, 2006.PMID 16754838
- [17]Bateman A, Campbell C, Luyten P, et al. A mentalization-based approach to common factors in the treatment of borderline personality disorder Curr Opin Psychol, 2018.PMID 28985628
- [18]Fonagy P, Simes E, Yirmiya K, et al. Mentalisation-based treatment for antisocial personality disorder in males convicted of an offence on community probation in England and Wales (Mentalization for Offending Adult Males, MOAM): a multicentre, assessor-blinded, randomised controlled trial with economic evaluation Lancet Psychiatry, 2025.PMID 39978982