Psych · psychotherapy
Psychoeducation and family psychoeducation
Also known as Family psychoeducation · FPE · Patient psychoeducation · Multifamily groups · MFG · Illness education · Behavioural family therapy · Relapse prevention education
Exam-exhaustive fellowship reference on psychoeducation and family psychoeducation — definitions, expressed emotion and relapse, session structure, FPE/MFG/BFT/bipolar group PE, Cochrane and trial evidence, NICE/RANZCP/APA principles, engagement without blame, confidentiality and safety, special populations, and CASC technique. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview and definition
Psychoeducation is a foundational psychosocial intervention across psychiatry: a planned process that improves knowledge of illness and treatment, builds self-management and carer skills, and links people to services, while remaining emotionally supportive rather than purely didactic.[17] Bäuml and colleagues frame PE as a basic psychotherapeutic intervention for schizophrenia and families — structured, interactive, and integrated with medication and other care, not a substitute for them.[17]
Family psychoeducation evolved from EE research and landmark programmes (Anderson/Hogarty, Falloon behavioural family therapy, McFarlane multifamily groups). It is now a recognised evidence-based practice for schizophrenia and bipolar disorder with multi-session dose, skill practice, and relapse focus.[7][10][11][16]

Classification of models (viva map)
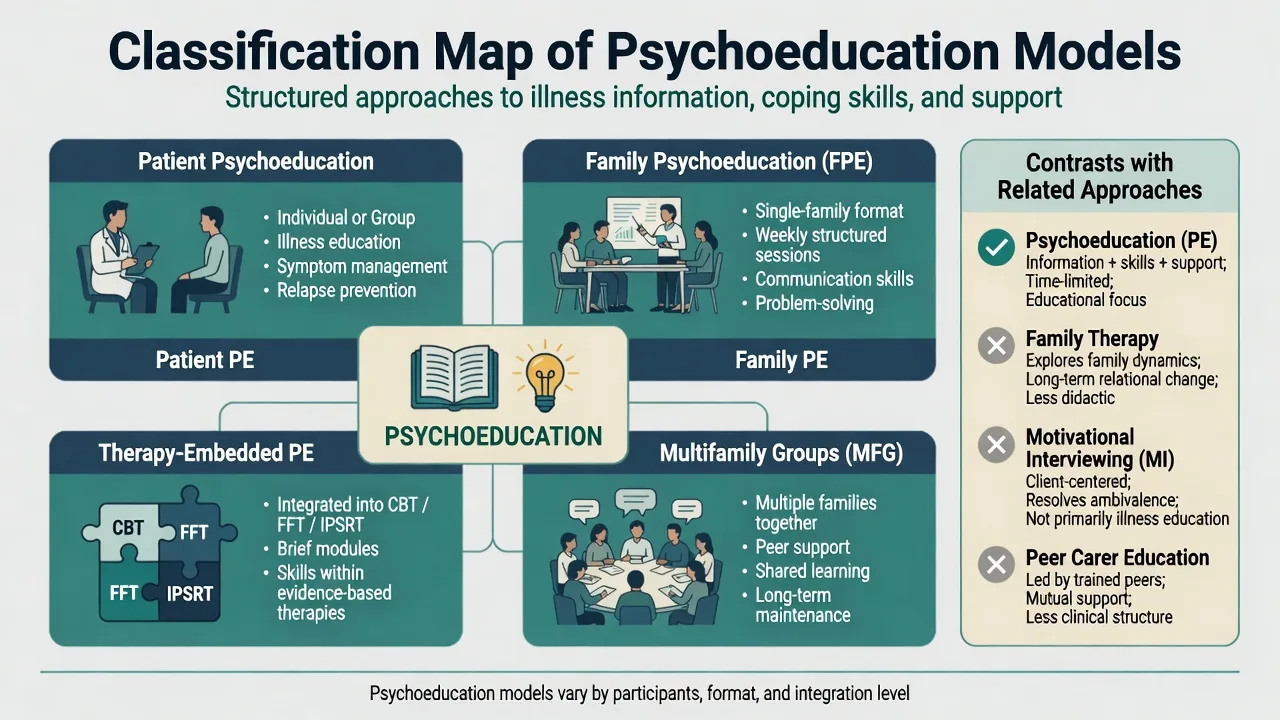
Examiner distinctions that lose marks if blurred — map format by who attends and the evidence package named in viva.[10][11][17]
| Model | Who | Core focus | Exam anchor |
|---|---|---|---|
| Patient PE (individual/group) | Service user ± optional carer | Illness model, meds, early signs, lifestyle | Xia Cochrane PE for schizophrenia[5] |
| Brief PE | Same, fewer sessions (often ≤10) | Condensed content | Zhao brief PE Cochrane — potential benefit, evidence still limited/heterogeneous[6] |
| Family PE / FPE (single-family) | Patient + relatives | Education + skills + support over months | Hogarty/Anderson lineage; Falloon BFT[7][16] |
| Multifamily groups (MFG) | Several families together | Peer modelling + problem-solving | McFarlane MFG trials/reviews[9][10] |
| Bipolar group PE | Patients in remission (often groups) | Awareness, adherence, early signs, lifestyle | Colom Barcelona model[13] |
| Family-focused therapy (FFT) | Patient + family | PE + communication + problem-solving in bipolar | Miklowitz FFT RCTs[15] |
| Family therapy (systemic/structural) | Family system | Relational patterns as primary target | Different evidence base; complementary, not synonym of FPE[10] |
| Peer carer education (e.g. NAMI-type) | Relatives, peer-led | Support and information | Valuable; not identical to clinician-led FPE dose/evidence[11] |
Epidemiology and implementation
High EE environments are associated with roughly doubled relapse risk in schizophrenia across meta-analysis — a robust psychosocial predictor, not proof that families cause schizophrenia.[1][2] Caregiver burden, depression, and social isolation are common among relatives of people with severe mental illness; FPE addresses both patient outcomes and carer strain.[11][18]
Despite decades of positive trials and guideline endorsement, implementation of FPE remains low relative to the evidence — a standard viva point on system quality and recovery-oriented services.[10][11][12]
Mechanisms: EE, stress-vulnerability, and caregiving appraisals
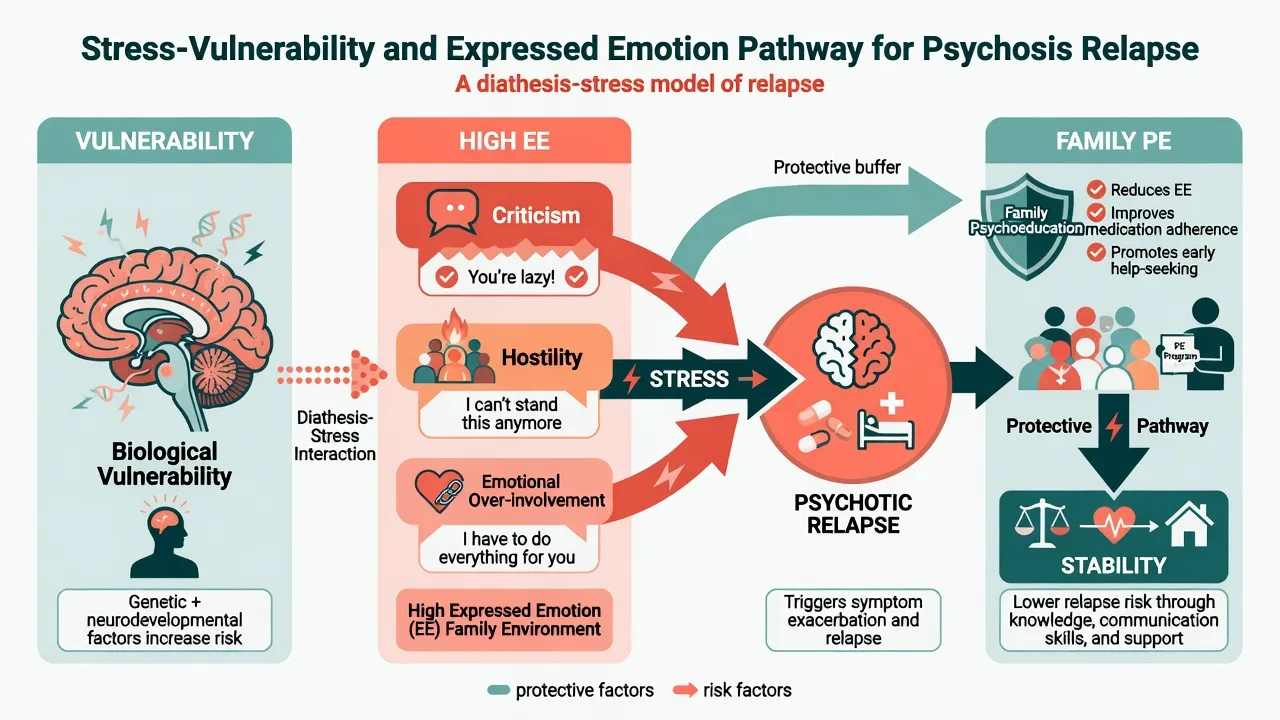
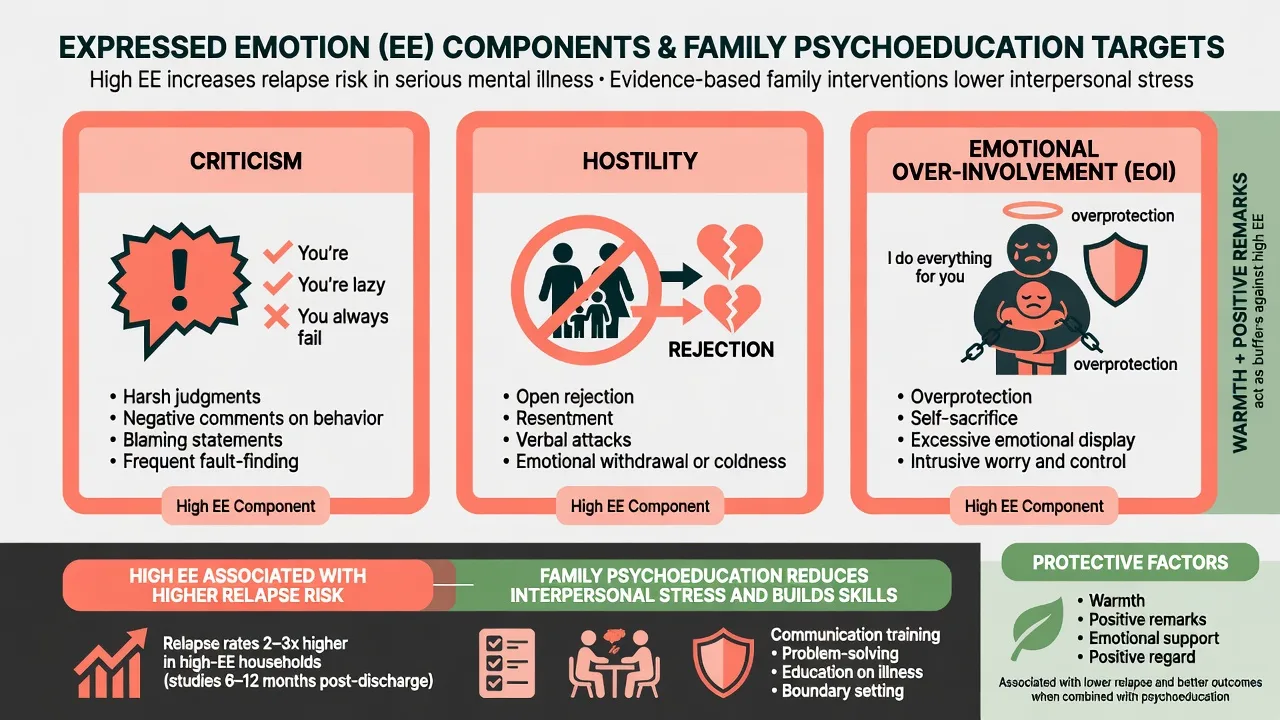
Expressed emotion (EE) components: criticism, hostility, and emotional over-involvement (EOI). Classic Camberwell Family Interview research linked high EE after discharge to relapse risk; warmth and positive remarks are protective correlates.[1][2]
Proposed active ingredients of PE/FPE include: a shared non-blaming illness model, better medication adherence, earlier help-seeking for prodromes, reduced critical or hostile interactions, improved problem-solving, social support, and reduced carer isolation.[3][10][17] The Kuipers cognitive model of caregiving links relatives' appraisals of illness to burden and EE pathways — a useful formulation bridge in viva.[18]
Clinical presentation and assessment
Family/system assessment for PE: who lives with the person; contact hours; genogram (three generations when feasible); explanatory models of each member; language and literacy needs; cultural decision-makers; children in the home (COPMI); carer sleep, mood, substances, and suicide risk; living-situation stress.[18]
EE proxies in ordinary clinic (when formal CFI is unavailable): frequency of critical comments, global hostility, EOI behaviours (self-sacrifice, overprotection, dramatic distress about the patient), versus warmth and collaborative problem-solving.[1]
Confidentiality contract before joint sessions: what individual-session content may be shared, exceptions for risk, and how secrets will be handled. Obtain consent for family meetings when capacity allows — FPE implementation reviews emphasise structured engagement without breaching individual privacy or safety duties.[11]
Differential and related interventions
- High EE household vs cultural closeness: high contact and strong family involvement are not automatically EOI; EOI implies intrusive overprotection, self-sacrifice, and excessive emotional display out of proportion and impairing autonomy.[1]
- Family conflict secondary to untreated psychosis vs primary relational disorder — treat the illness and still offer FPE.
- Shared delusional disorder vs family explanatory model — assess for induced psychosis carefully.
- Carer major depression needing individual treatment vs "only carer burden."
- PE vs CBTp: PE is foundational knowledge/skills; CBTp targets residual psychotic symptoms with cognitive-behavioural methods after engagement.
Acute / crisis psychoeducation
In acute settings prioritise medical and risk stabilisation first. Then deliver brief crisis PE: plain-language working diagnosis, medication purpose and common side effects, sleep and substance advice, early warning signs card, crisis contacts, leave/discharge safety roles for carers, and a plan for multi-session FPE after the acute phase.[5][17] Do not hold emergency treatment for a full FPE programme.
Definitive management — content, dose, formats
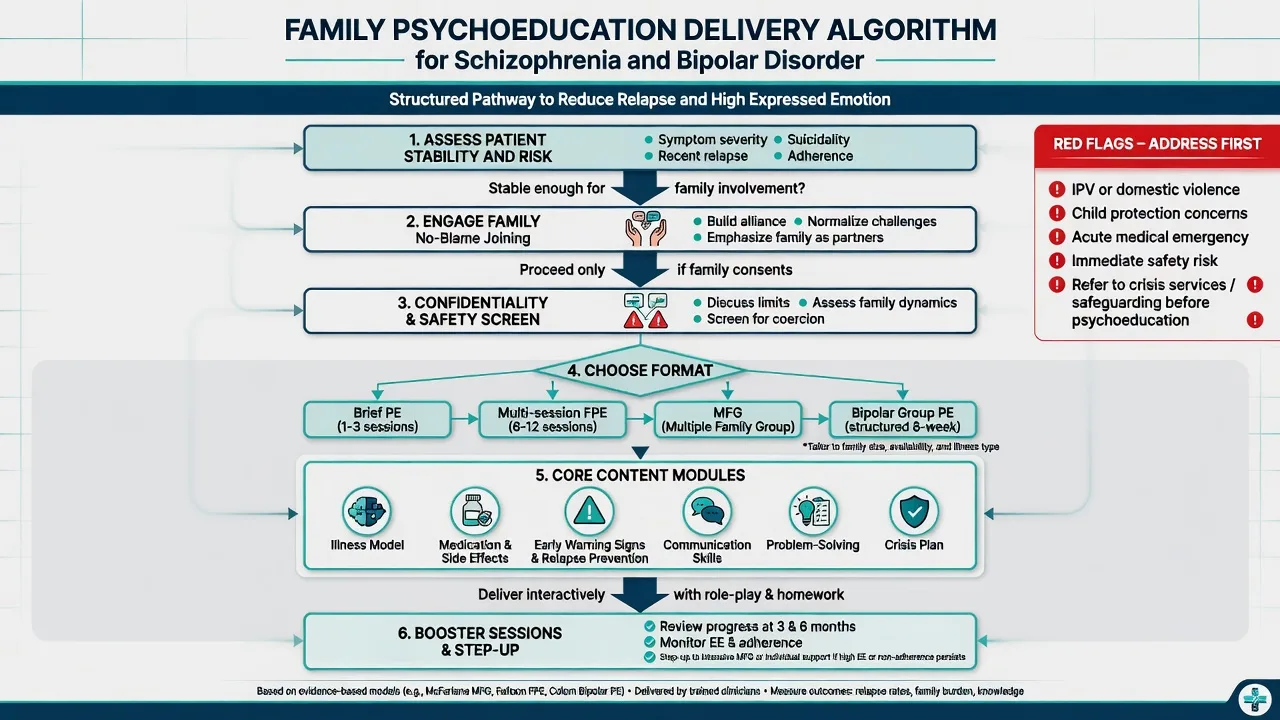
Core content modules (any high-quality PE)
- Diagnosis, course, and stress-vulnerability model (non-blaming).
- Medications: benefits, side effects, monitoring concepts (e.g. metabolic care with antipsychotics; lithium level principles in bipolar).
- Early warning signs and personalised relapse signature.
- Communication skills and reducing critical/hostile exchanges.
- Structured problem-solving.
- Crisis and help-seeking plan; rights, services, and stigma.[10][17]
Session structure
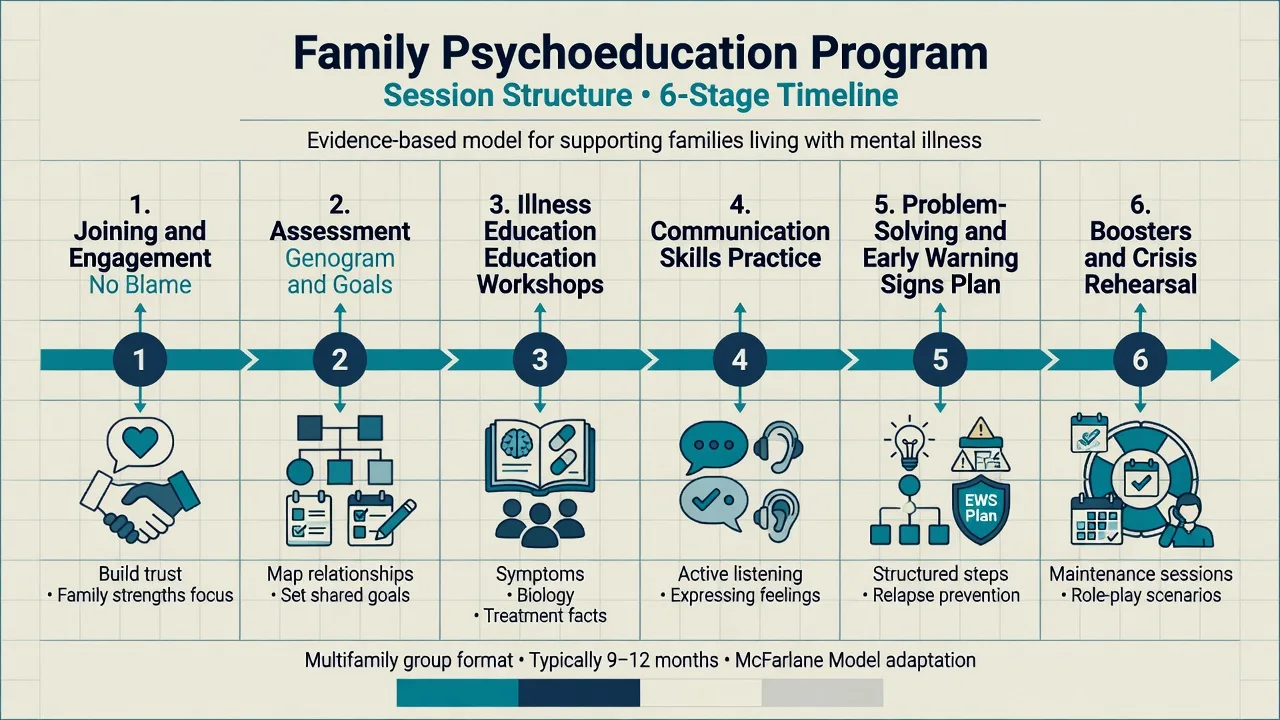
Typical FPE arc: joining (alliance, no blame) → assessment and goals → education workshops → communication training → problem-solving and early-warning plan → booster/crisis rehearsal sessions over months.[10][16]
Psychosis / schizophrenia
NICE-aligned family intervention principles (exam phrasing): offer structured family intervention including the service user when possible, commonly at least about 10 sessions over 3–12 months, covering psychoeducation, communication, and problem-solving (single-family or multifamily formats).[3][4][12]
Landmark packages for psychosis FPE (name these in viva) include Hogarty/Anderson FPE, Falloon BFT, and McFarlane MFG.[7][9][16]
- Hogarty/Anderson family psychoeducation with social skills training and maintenance medication reduced relapse versus control conditions in aftercare trials.[7][8]
- Falloon behavioural family therapy (BFT): assessment, education, communication skills, problem-solving — improved clinical and social outcomes over two years in classic trials.[16]
- McFarlane multifamily groups: psychoeducational multi-family format; multi-family groups can outperform single-family treatment for extending remission in higher-risk patients in key trials.[9][10]
Cochrane and synthesis evidence: Pharoah et al. found family intervention may reduce relapse events and hospitalisations.[3] Rodolico et al. network meta-analysis supports several family intervention formats versus treatment as usual for relapse prevention.[4] Xia et al. found psychoeducation added to standard care appears to reduce relapse and readmission and encourage medication compliance, with shorter hospital stay in synthesised data.[5] Brief PE may help but needs more high-quality trials.[6]
Bipolar disorder
- Colom group psychoeducation (structured multi-session group in remitted bipolar I/II on pharmacotherapy) reduced recurrences versus control — important pearl: benefits extend beyond "non-compliant" patients.[13]
- Perry et al. teaching early warning signs of manic relapse improved time to manic episode and functioning.[14]
- Miklowitz family-focused therapy (FFT) combines psychoeducation, communication enhancement, and problem-solving with pharmacotherapy and improves outcomes versus less intensive comparison conditions in key RCTs.[15]
Other common PE applications
Depression and anxiety stepped care; OCD family accommodation reduction; dual-diagnosis education; perinatal couple PE; brief dementia carer education (related but distinct pathways). Always match dose and manualisation to the evidence for that diagnosis — psychosis and bipolar packages above are the highest-yield exam anchors.[10][13][17]
Regional guidance deltas
Pitfalls and professionalism
- Blaming families / schizophrenogenic mother language — obsolete and harmful.[10]
- Didactic monologue without checking understanding or emotional impact.
- Overloading an acutely psychotic person with dense education before stabilisation.
- Therapist triangulation or taking sides.
- Ignoring carer mental health and suicide risk.
- Pathologising culture as EOI.
- Confidentiality breaches in joint sessions.
- Claiming PE alone is sufficient for acute mania, catatonia, or high suicide risk.
Prognosis and disposition
Expect reduced relapse/readmission risk and better adherence metrics when structured PE/FPE is delivered with pharmacotherapy, though effect sizes and formats vary across reviews.[3][4][5] Disposition checklist: personalised early warning signs card, crisis contacts, medication plan, carer support linkage, booster PE or step-up to full family intervention/CBTp if high EE proxies, non-adherence driven by family beliefs, or carer collapse.
Special populations
- First-episode psychosis: high family distress and high yield for early FPE/MFG engagement.[9][12]
- Youth: developmental language, school liaison, sibling inclusion.
- Older adults: cognitive load, sensory needs, adult-child carers.
- Perinatal: partner PE, sleep protection, bonding support under risk protocols.
- Intellectual disability: simplified language, visual aids, carer co-learning, longer sessions.
- Indigenous and culturally diverse families: define who is "family," involve elders appropriately, use interpreters, avoid imposing nuclear-family templates.
- COPMI: age-appropriate PE and child protection assessment.
Exam pearls
- EE triad = criticism, hostility, EOI — not "emotionally expressive family."[1]
- High EE predicts relapse; it does not mean families caused schizophrenia.[1][2]
- Name packages: Hogarty/Anderson FPE, Falloon BFT, McFarlane MFG, Colom bipolar PE, Miklowitz FFT, Perry early signs.[7][9][13][14][15][16]
- Cochrane anchors: Pharoah family intervention; Xia PE; Zhao brief PE.[3][5][6]
- NICE-style dose: multi-session family intervention over months, not one meeting.
- CASC: join each member, neutral stance, plain language, check understanding, shared problem (illness and stress), not "fix the parent."
- Always state safety overrides joint PE and confidentiality limits.
Self-test hooks (fellowship)
- Define PE and FPE and give three format differences (patient group vs single-family FPE vs MFG).[17]
- List EE components and one meta-analytic claim about relapse.[1]
- Outline a 6-module PE content list and NICE-style dose for psychosis family intervention.[3][17]
- Contrast Colom PE vs Miklowitz FFT for bipolar.[13][15]
- Name two situations where joint PE is deferred.[11]
- Quote one Cochrane finding for PE and one for family intervention without overclaiming cure rates.[3][5]
References
- [1]Butzlaff RL, Hooley JM Expressed emotion and psychiatric relapse: a meta-analysis Arch Gen Psychiatry, 1998.PMID 9633674
- [2]Brown GW, Birley JL, Wing JK Influence of family life on the course of schizophrenic disorders: a replication Br J Psychiatry, 1972.PMID 5073778
- [3]Pharoah F, Mari J, Rathbone J, et al. Family intervention for schizophrenia Cochrane Database Syst Rev, 2010.PMID 21154340
- [4]Rodolico A, Bighelli I, Avanzato C, et al. Family interventions for relapse prevention in schizophrenia: a systematic review and network meta-analysis Lancet Psychiatry, 2022.PMID 35093198
- [5]Xia J, Merinder LB, Belgamwar MR Psychoeducation for schizophrenia Schizophr Bull, 2011.PMID 21147896
- [6]Zhao S, Sampson S, Xia J, et al. Psychoeducation (brief) for people with serious mental illness Cochrane Database Syst Rev, 2015.PMID 25854522
- [7]Hogarty GE, Anderson CM, Reiss DJ, et al. Family psychoeducation, social skills training, and maintenance chemotherapy in the aftercare treatment of schizophrenia. II. Two-year effects of a controlled study on relapse and adjustment Arch Gen Psychiatry, 1991.PMID 1672589
- [8]Hogarty GE, Anderson CM, Reiss DJ, et al. Family psychoeducation, social skills training, and maintenance chemotherapy in the aftercare treatment of schizophrenia. I. One-year effects of a controlled study on relapse and adjustment Arch Gen Psychiatry, 1986.PMID 2872870
- [9]McFarlane WR, Lukens E, Link B, et al. Multiple-family groups and psychoeducation in the treatment of schizophrenia Arch Gen Psychiatry, 1995.PMID 7632121
- [10]McFarlane WR, Dixon L, Lukens E, et al. Family psychoeducation and schizophrenia: a review of the literature J Marital Fam Ther, 2003.PMID 12728780
- [11]Lucksted A, McFarlane W, Downing D, et al. Recent developments in family psychoeducation as an evidence-based practice Psychiatr Serv, 2012.PMID 22283383
- [12]McFarlane WR Family Interventions for Schizophrenia and the Psychoses: A Review Fam Process, 2016.PMID 27411376
- [13]Colom F, Vieta E, Martinez-Aran A, et al. A randomized trial on the efficacy of group psychoeducation in the prophylaxis of recurrences in bipolar patients whose disease is in remission Arch Gen Psychiatry, 2003.PMID 12695318
- [14]Perry A, Tarrier N, Morriss R, et al. Randomised controlled trial of efficacy of teaching patients with bipolar disorder to identify early symptoms of relapse and obtain treatment BMJ, 1999.PMID 9888904
- [15]Miklowitz DJ, George EL, Richards JA, et al. A randomized study of family-focused psychoeducation and pharmacotherapy in the outpatient management of bipolar disorder Arch Gen Psychiatry, 2003.PMID 12963672
- [16]Falloon IR, Boyd JL, McGill CW, et al. Family management in the prevention of morbidity of schizophrenia. Clinical outcome of a two-year longitudinal study Arch Gen Psychiatry, 1985.PMID 2864032
- [17]Bäuml J, Froböse T, Kraemer S, et al. Psychoeducation: a basic psychotherapeutic intervention for patients with schizophrenia and their families Schizophr Bull, 2006.PMID 16920788
- [18]Kuipers E, Onwumere J, Bebbington P Cognitive model of caregiving in psychosis Br J Psychiatry, 2010.PMID 20357299