Psych · psychotherapy
Supportive psychotherapy techniques
Also known as Supportive psychotherapy · Brief supportive psychotherapy · BSP · Supportive therapy · Ego-supportive psychotherapy · Supportive-expressive therapy · Common factors psychotherapy
Exam-exhaustive fellowship reference on supportive psychotherapy techniques — definition, expressive–supportive continuum, technique toolkit, brief supportive psychotherapy (BSP), alliance and rupture–repair, indications, Winston/Pinsker/Hellerstein/Misch/Markowitz evidence, boundaries, combined medication-visit practice, and CASC/MEQ skills. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview and definition
Supportive psychotherapy is not residual "being nice" while waiting for a real therapy. Fellowship candidates must define it as a technique-bearing psychotherapy with frame, goals, formulation (even if brief), and review points.[1][2][7]
Historically under-theorised relative to psychoanalysis and later CBT, modern supportive work was codified by Winston, Pinsker, Hellerstein, Rosenthal and colleagues, with Misch articulating basic strategies and Markowitz refining brief supportive psychotherapy (BSP) as both an active clinical intervention and a credible research control.[1][2][5][7]
Training priorities are shifting: Dotson and Markowitz argue residency programmes should plant the tree right-side up — teach supportive technique first as the psychotherapy of everyday psychiatric practice, not as a leftover after specialised models.[6]

Definition and classification (examiner dimension 1)
| Construct | Exam definition |
|---|---|
| Supportive psychotherapy | Ego-strengthening, reality-oriented psychotherapy building adaptive defences, self-esteem, coping, and alliance rather than systematic uncovering |
| Expressive–supportive continuum | Technique spectrum from interpretation/clarification to advice/praise/environmental help; same patient may move along it |
| BSP | Manualised, time-limited, affect-focused common-factors treatment (often ~12–16 sessions in research frames) |
| Supportive-expressive (SE) | Hybrid that can flex toward focal conflict work while retaining support |
| Not a diagnosis | Modality/technique set for treatment planning |
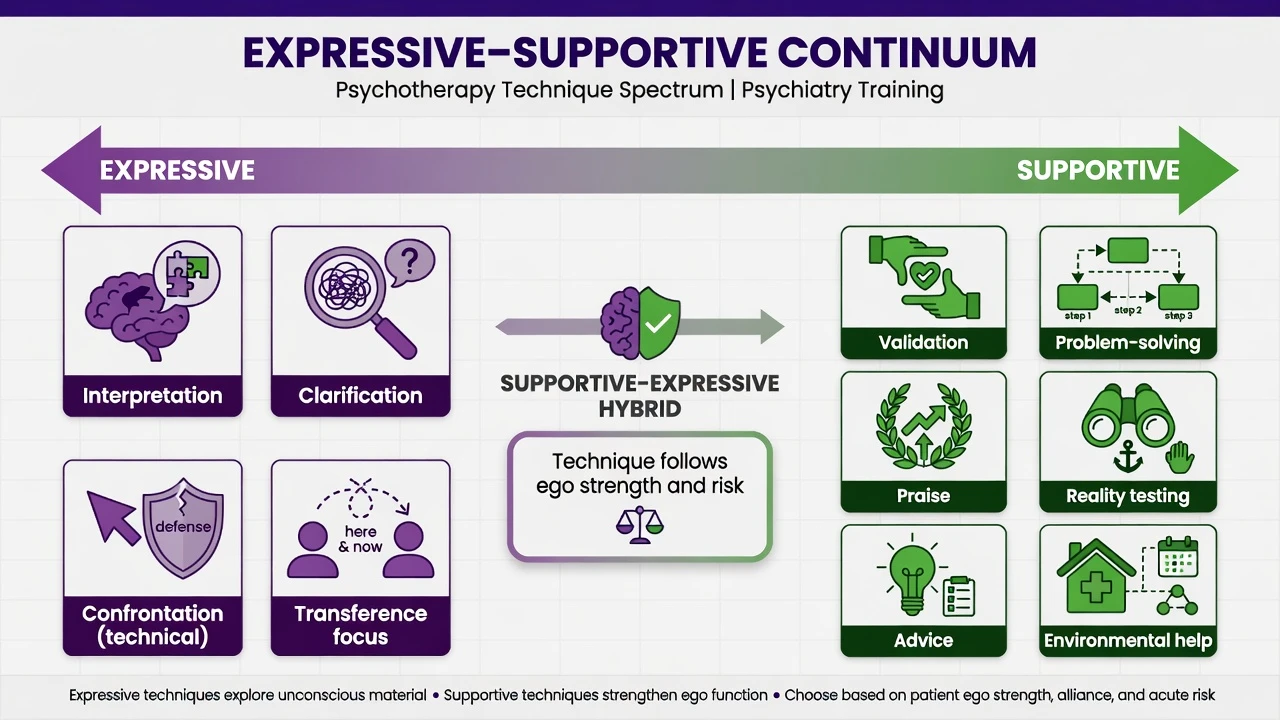
- Strengthen adaptive defences
- Validation and praise
- Advice and problem-solving
- Reality testing and structure
- Containment over uncovering
- Clarification and timed interpretation
- Defence and conflict focus
- Selective transference work
- Tolerance of affect and silence
- Needs adequate ego strength
- Shift within a session
- Support first if overwhelmed
- Deepen when stable
- Review goals regularly
- Supervise complex work
Epidemiology and service context (dimension 2)
In routine general adult psychiatry, supportive techniques dominate medication clinics, community follow-up, and inpatient contacts. Specialised CBT/IPT/psychodynamic packages are often waitlisted; examiners still expect you to deliver structured support rather than pure script-writing.[2][5][6]
Risk interfaces: intense idealising or dependent transferences can pull toward boundary erosion; hostile ruptures can trigger therapist withdrawal; fragile ego states can be harmed by premature uncovering.[14][15][16]
Mechanisms (dimension 3)
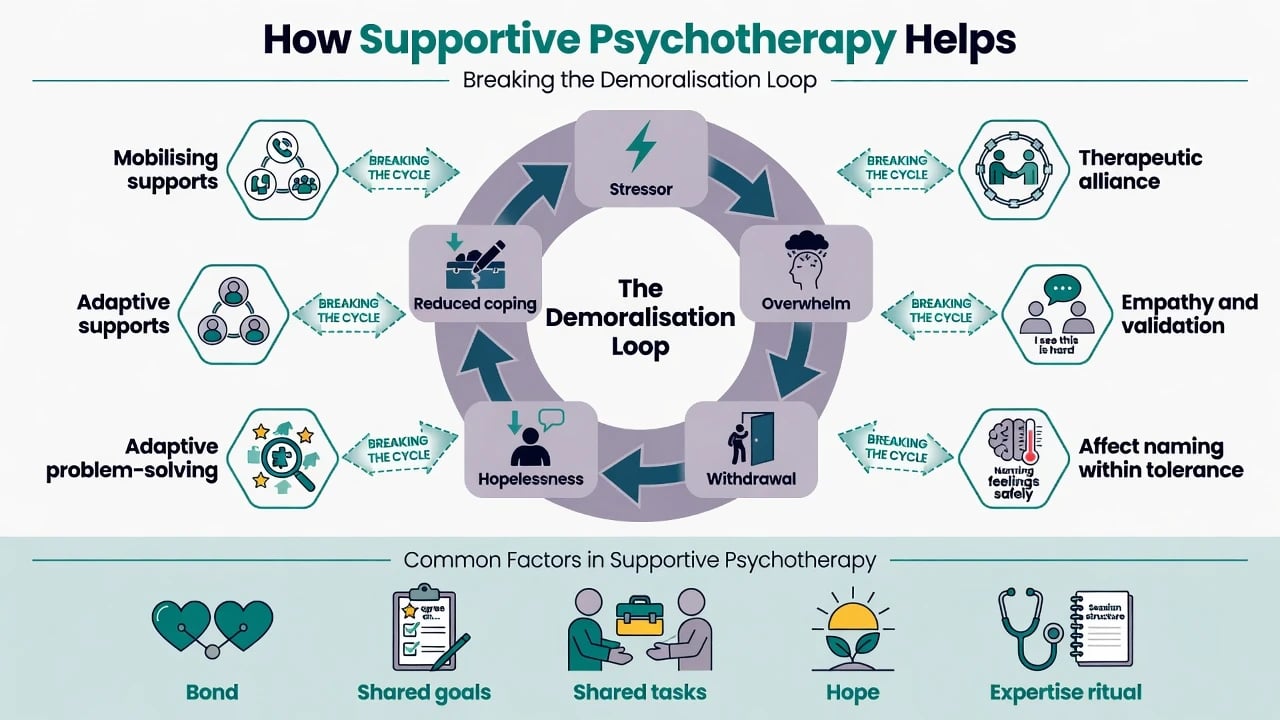
Supportive change mechanisms include reducing demoralisation, bolstering self-esteem, modelling problem-solving, strengthening adaptive defences (for example anticipation, humour, sublimation rather than splitting or projective identification), improving reality testing, containing affect within a tolerable window, and mobilising external supports.[1][2][7]
BSP deliberately maximises common factors: feeling understood, emotional arousal within tolerance, alliance through ritual and expertise, realistic hope, and success experiences.[5]
Alliance (bond + agreed goals + agreed tasks) is a pantheoretical predictor of outcome across modalities — meta-analyses by Martin, Horvath, and Flückiger show a moderate, robust alliance–outcome association.[9][10][11] Rupture recognition and repair is itself a change process; unrepaired rupture predicts poorer outcome.[12][13]
Clinical process presentation (dimension 4)
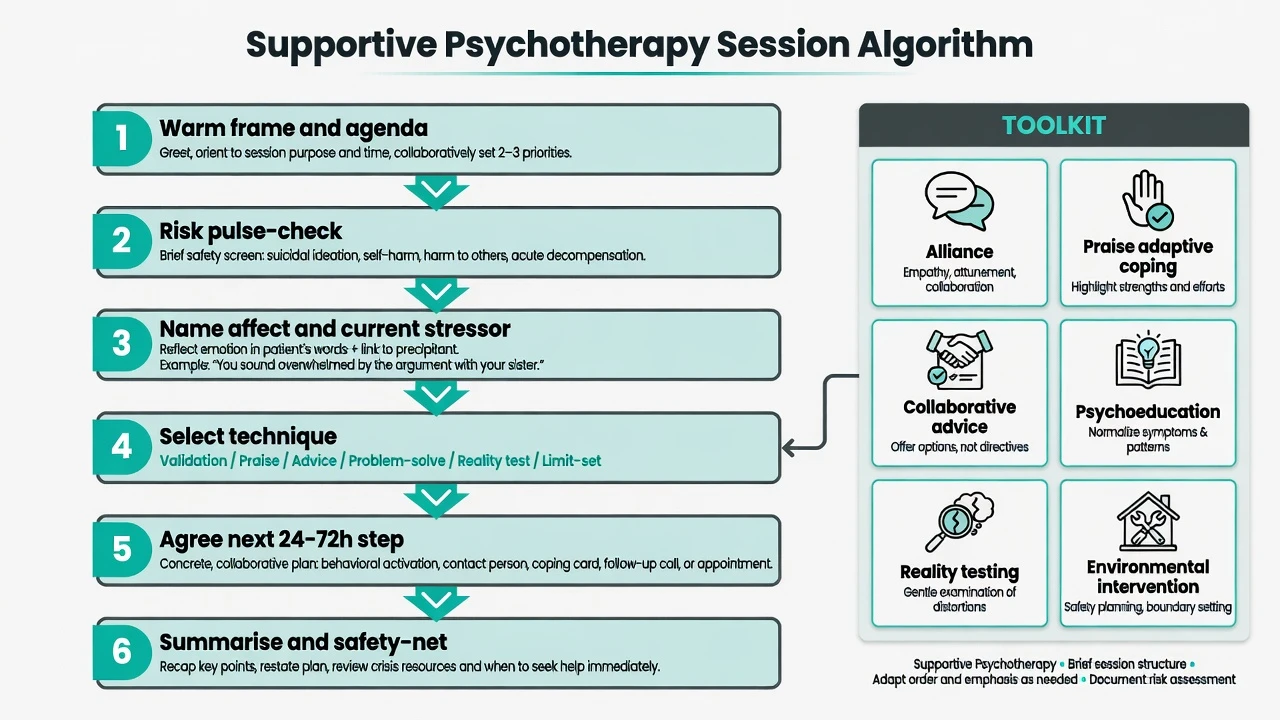
Good supportive notes show: warm frame, collaborative agenda, risk pulse-check, named affect linked to a current stressor, selected technique (validation, praise, advice, problem-solve, reality test, limit-set), concrete next-step plan, summary, and safety-net.[5][7]
Process phenomena still appear — idealisation, dependency, hostility, eroticised gratitude — but the default technical move is supportive management (frame, limits, validation of affect without acting out the induced role), not systematic deep transference interpretation every session.[15][16]
Countertransference remains data and risk: Gabbard's contemporary model treats the therapist's total emotional response as informative when recognised and supervised, dangerous when enacted.[15][16]
Differential and modality discrimination (dimension 5)
| Lookalike | Discriminator |
|---|---|
| Unstructured chat | No goals, no technique selection, no review |
| Case management | Resource coordination without psychotherapeutic process skill |
| Collusion | Avoids necessary limits, risk talk, or destructive-pattern feedback |
| Expressive psychodynamic | Timed interpretation of defence/conflict/transference as main work |
| CBT | Structured cognitive/behavioural curriculum and homework emphasis |
| IPT | Four interpersonal problem areas and role transitions/disputes/grief/deficits |
| MI | Explicit focus on ambivalence and change talk about a target behaviour |
Assessment and contracting (dimension 6)
Assess ego strength (frustration tolerance, impulse control, reality testing), alliance capacity, motivation and goals, substance use, organic contributors, cultural explanatory model, prior therapy (including boundary trauma), and full risk (suicide, violence, vulnerability, neglect).[1][7][14]
Contract: frequency, likely duration or review points, contact rules, cancellation, crisis plan, how medication will be co-managed, confidentiality limits, and what success looks like in functional terms (sleep, role return, adherence, affect tolerance).[5][14]
Outcome monitoring: disorder scales (for example PHQ-9/GAD-7 where appropriate) plus functional goals and alliance quality — not scale fetish alone.[9][11]
Investigations (dimension 7)
No laboratory test selects supportive therapy. Medical review revises the plan when delirium, endocrine disease, substance intoxication/withdrawal, medication toxicity, or neurological disease is possible. Baseline metabolic panel/ECG when combining with psychotropics is about medication safety, not about proving therapy indication.[5][8]
Acute priorities (dimension 8)
Crisis supportive moves: name affect briefly, simplify to the next 24 hours, safety plan, mobilise supports, increase contact intensity temporarily, document, and supervise. Do not use deep conflict interpretation as crisis management.[7][12]
Definitive technique toolkit (dimension 9)
Core techniques (Winston–Pinsker–Hellerstein–Misch–Markowitz lineage)
- Alliance building — explicit warmth, shared goals, shared tasks.[9][10][11]
- Empathic validation — name the understandable part of the reaction without agreeing to distortions that harm.
- Affect ventilation within tolerance — allow expression; stop short of flooding.
- Praise of adaptive coping — specific, credible praise of effort and skill, not empty flattery.[7]
- Selective advice — collaborative options, not authoritarian monologue; check fit with patient values.[1][7]
- Problem-solving — define problem, generate options, choose one small step, review barriers.
- Psychoeducation — symptoms, illness course, medication rationale, sleep/stress links — in plain language.
- Reality testing — gentle examination of distortions when ego can use it; firmer structure when reality testing fails.
- Adaptive defence strengthening — reinforce anticipation, humour, sublimation, altruism over primitive defences when possible.[1][7]
- Limit-setting — clear, non-humiliating boundaries on time, contact, aggression, substance use in session.[14]
- Environmental intervention — mobilise family, housing, benefits, occupational supports via appropriate pathways.
- Demoralisation repair — restore hope with realistic, achievable next steps and success experiences.[5]
Session structure
Warm greeting → collaborative agenda → risk pulse-check → focus current stressor/function → technique selection → agree next 24–72 hour step → summarise and safety-net.[5][7]
BSP specifically
BSP is time-limited, affect-focused, common-factors maximising, and less homework-heavy than CBT. Markowitz synthesises decades of trials using BSP as active control and clinical intervention — it is not placebo.[5] In depressed HIV-positive patients, IPT and medication packages showed advantages over BSP alone for depressive symptoms in key trials, yet BSP still produced clinically meaningful change and matched some comparators in nuanced analyses — know the hierarchy without dismissing support.[5][8]
Combined pharmacotherapy visits
The 15–20 minute medication review is a supportive psychotherapy session if you use the toolkit. Dotson and Markowitz argue this is where most psychiatrists actually practise therapy and where training investment belongs.[6]
Clinical scenarios (dimension 10)
| Scenario | Supportive emphasis |
|---|---|
| Outpatient depression/anxiety | BSP-style course; combine with antidepressant when indicated |
| Psychosis / SMI | Reality testing, adherence alliance, ego support — not insight-at-all-costs |
| Personality pathology | Firm frame, validation without collusion; step to DBT/MBT/TFP/GPM when indicated |
| C-L / medical illness | Demoralisation, illness coping, adherence, family communication |
| Inpatient short contacts | Containment, discharge-linked micro-goals |
| Medication clinic | Micro-session supportive technique every review |
Interpersonal change can occur even in brief supportive work when adaptive interpersonal behaviour is actively fostered.[3][4] Comparative RCT work found supportive and dynamic therapies can both help, with alliance quality mattering across models.[3]
Complications and pitfalls (dimension 11)
- Drift into chat without goals or homework/next-step review.[7]
- Collusion that never addresses risk or self-defeating patterns.[7][14]
- Over-advice creating dependency and undercutting autonomy.
- Premature uncovering that floods a fragile patient.[1]
- Boundary crossings under idealisation (special patient, after-hours dual roles).[14]
- Therapist withdrawal after hostility without rupture–repair attempt.[12][13]
- Cultural imposition of therapist lifestyle as "advice".
Prognosis and disposition (dimension 12)
Hellerstein and colleagues showed supportive and dynamic therapies can both improve outcomes with important alliance signals.[3] Rosenthal demonstrated interpersonal change in brief supportive work.[4] Markowitz BSP synthesis positions supportive therapy as active treatment with a multi-decade trial footprint.[5]
Step up when: non-response after adequate supportive dose/fidelity; need for trauma-focused work; specialised personality model indicated; escalating risk; strong preference and access for CBT/IPT with matching problem focus.[5][8]
Step down / maintain: spaced supportive contacts for chronic illness stabilisation, adherence, and early relapse detection.[2][6]
Special populations (dimension 13)
- Youth: caregiver involvement, school function goals, developmental language.
- Older adults: medical comorbidity, grief/role loss, cognitive pacing, polypharmacy interface.
- Pregnancy/lactation: psychological support often preferred early for mild–moderate illness; medication co-decision if severe — local perinatal pathways apply.
- Intellectual disability: concrete goals, carer scaffolding, behavioural emphasis.
- Cultural diversity / Indigenous care: co-define valued supports; cultural humility in advice; avoid Eurocentric "lifestyle fixes".
- Forensic interfaces: supportive engagement within a clear legal frame; therapy is not a substitute for risk management.
Evidence and guidelines (dimension 14)
Core supportive literature: Winston/Pinsker/McCullough review; Hellerstein "model of choice"; Hellerstein RCT supportive vs dynamic; Rosenthal interpersonal change; Misch basic strategies; Markowitz HIV depression work and 2022 BSP synthesis; Dotson/Markowitz training priority.[1][2][3][4][5][6][7][8]
Alliance and process: Martin 2000; Horvath 2011; Flückiger 2018; Safran rupture–repair 2011; Eubanks meta 2018.[9][10][11][12][13]
Boundaries/CT: Gutheil and Gabbard; Gabbard countertransference models.[14][15][16]
Exam pearls (dimension 15)
- Supportive therapy is skilled technique, not lesser therapy.[2][5][6]
- Continuum language scores viva marks.
- Alliance = bond + goals + tasks; alliance predicts outcome across models.[9][10][11]
- Praise adaptive behaviour specifically; advice is collaborative and selective.[7]
- Collusion ≠ support; limits protect the work.[14]
- BSP is active treatment and active control — never call it placebo.[5]
- Support first in acute psychosis/mania/delirium/overwhelming risk.[1][7]
- Medication visit = supportive psychotherapy opportunity.[6]
- Rupture without repair attempt is a CASC fail pattern.[12][13]
- Countertransference: use as data; do not act it out.[15][16]
One-page technique card
| Phase | Do this |
|---|---|
| Open | Warm frame, agenda, risk pulse-check |
| Focus | Name affect + current stressor in patient language |
| Technique | Pick 1–2 tools: validate, praise adaptive, advise options, problem-solve one step, reality-test gently, limit-set if needed |
| Close | Next 24–72 h plan, crisis contacts, follow-up |
References
- [1]Winston A, Pinsker H, McCullough L A review of supportive psychotherapy Hosp Community Psychiatry, 1986.PMID 3781499
- [2]Hellerstein DJ, Pinsker H, Rosenthal RN, et al. Supportive therapy as the treatment model of choice J Psychother Pract Res, 1994.PMID 22700197
- [3]Hellerstein DJ, Rosenthal RN, Pinsker H, et al. A randomized prospective study comparing supportive and dynamic therapies. Outcome and alliance J Psychother Pract Res, 1998.PMID 9752637
- [4]Rosenthal RN, Muran JC, Pinsker H, et al. Interpersonal change in brief supportive psychotherapy J Psychother Pract Res, 1999.PMID 9888107
- [5]Markowitz JC Supportive Evidence: Brief Supportive Psychotherapy as Active Control and Clinical Intervention Am J Psychother, 2022.PMID 35232221
- [6]Dotson S, Markowitz JC Planting the Tree Right-Side Up: Supportive Psychotherapy as a Priority in Residency Training Acad Psychiatry, 2025.PMID 40921918
- [7]Misch DA Basic strategies of dynamic supportive therapy J Psychother Pract Res, 2000.PMID 11069130
- [8]Markowitz JC, Kocsis JH, Fishman B, et al. Treatment of depressive symptoms in human immunodeficiency virus-positive patients Arch Gen Psychiatry, 1998.PMID 9596048
- [9]Martin DJ, Garske JP, Davis MK Relation of the therapeutic alliance with outcome and other variables: a meta-analytic review J Consult Clin Psychol, 2000.PMID 10883561
- [10]Horvath AO, Del Re AC, Flückiger C, Symonds D Alliance in individual psychotherapy Psychotherapy (Chic), 2011.PMID 21401269
- [11]Flückiger C, Del Re AC, Wampold BE, Horvath AO The alliance in adult psychotherapy: A meta-analytic synthesis Psychotherapy (Chic), 2018.PMID 29792475
- [12]Safran JD, Muran JC, Eubanks-Carter C Repairing alliance ruptures Psychotherapy (Chic), 2011.PMID 21401278
- [13]Eubanks CF, Muran JC, Safran JD Alliance rupture repair: A meta-analysis Psychotherapy (Chic), 2018.PMID 30335462
- [14]Gutheil TG, Gabbard GO The concept of boundaries in clinical practice: theoretical and risk-management dimensions Am J Psychiatry, 1993.PMID 8422069
- [15]Gabbard GO A contemporary psychoanalytic model of countertransference J Clin Psychol, 2001.PMID 11449380
- [16]Gabbard GO The role of countertransference in contemporary psychiatric treatment World Psychiatry, 2020.PMID 32394567