Psych · Psychotherapy
Trauma-focused CBT and EMDR
Also known as Trauma-focused CBT · TF-CBT · Prolonged exposure · Cognitive processing therapy · CT-PTSD · EMDR · Eye movement desensitization and reprocessing · Trauma-focused psychotherapy
Exam-exhaustive fellowship reference on trauma-focused psychological therapies — PE, CPT, CT-PTSD/TF-CBT, child TF-CBT, and EMDR — with Ehlers–Clark and exposure mechanisms, readiness, session architecture, meta-analytic and guideline evidence, complex presentations, pharmacotherapy interface, and CASC/MEQ pearls. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
2 MCQs with explanations
Target exams
Red flags
Fellowship examiners (FRANZCP MEQ/CASC, MRCPsych Paper B/CASC, ABPN, MD/DNB viva) test named protocols, mechanisms (Ehlers–Clark; exposure/emotional processing; EMDR dual attention), readiness and safety, guideline deltas, and the ability to explain a plan in plain language without collapsing into unstructured “talking about the trauma.”[1][10][17]
Definition and classification
Trauma-focused psychological therapy means a structured, protocol-guided treatment that includes active processing of trauma memories and/or trauma-related meanings (appraisals, stuck points), usually with between-session practice. Supportive counselling, case management, and pure present-centred support may help engagement or quality of life but are not interchangeable with trauma-focused packages for PTSD symptom change in major syntheses.[8][9][10]
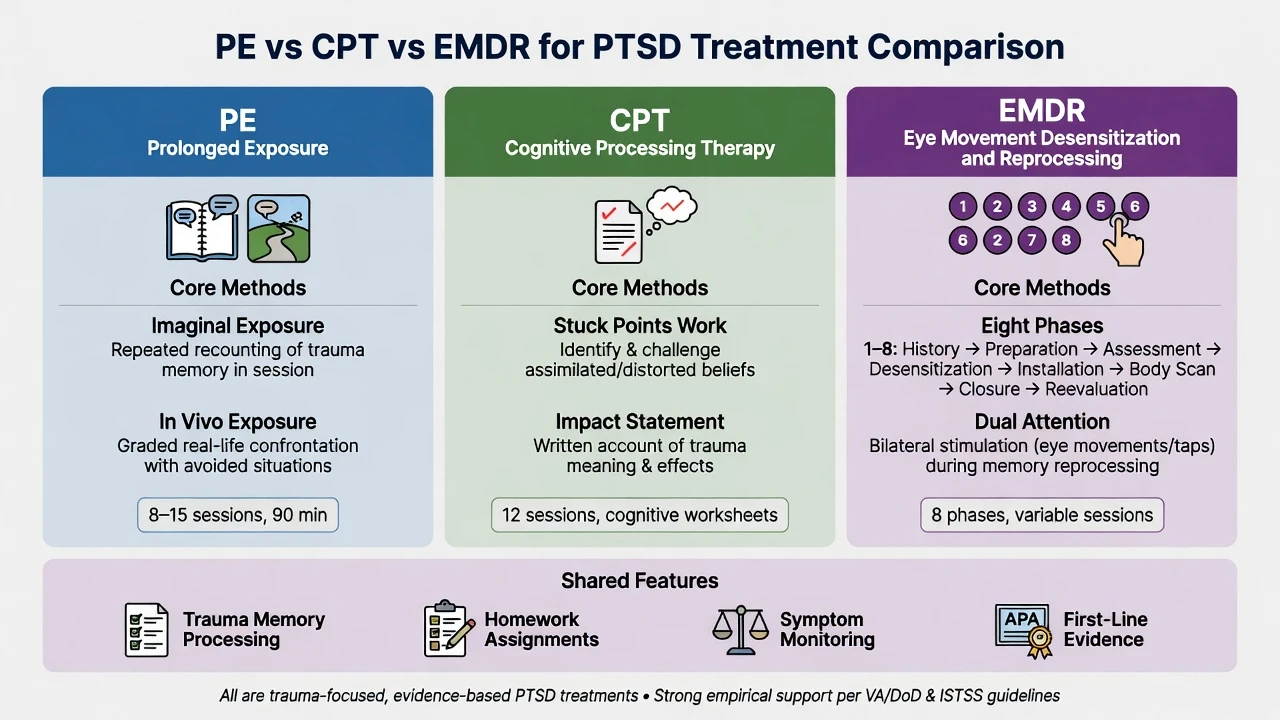
| Package | Core technology | Exam skeleton |
|---|---|---|
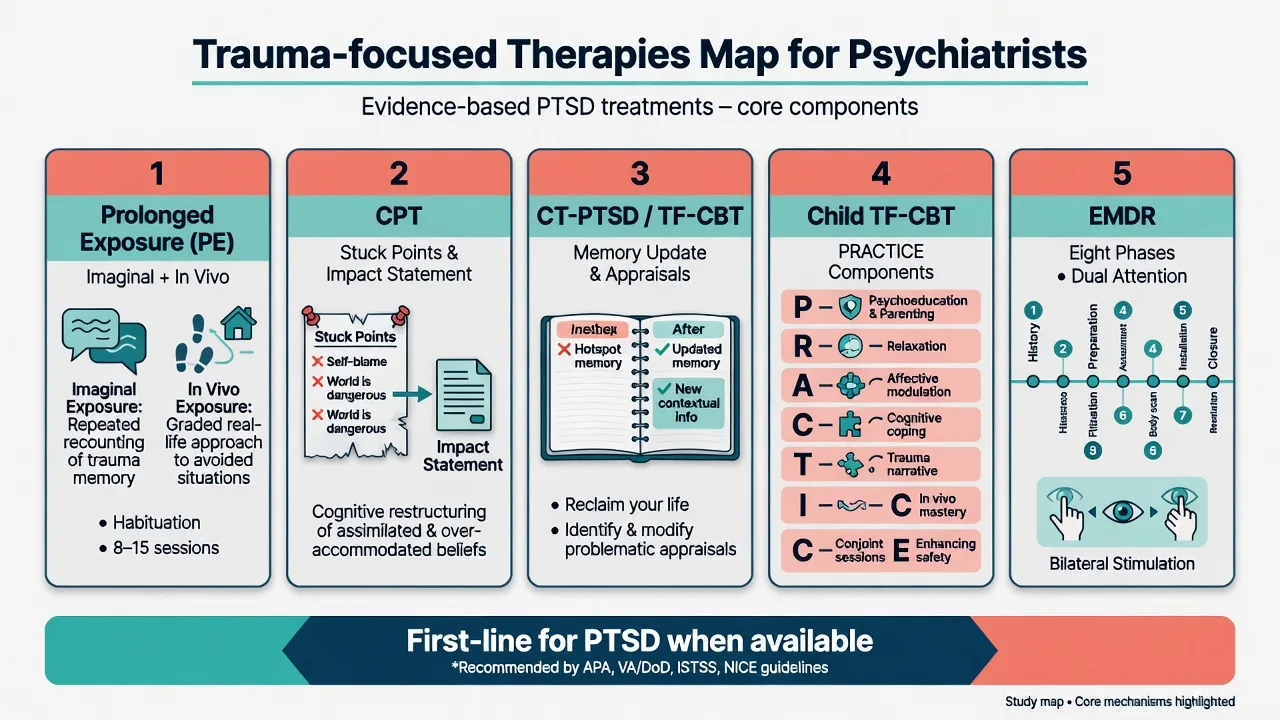
| Prolonged exposure (PE) | Imaginal exposure to trauma narrative; in vivo exposure to avoided safe cues; processing | Foa lineage; strong meta-analytic support |
| Cognitive processing therapy (CPT) | Impact statement; stuck points; Socratic cognitive work; optional written account | Resick lineage; CPT-C dismantling |
| CT-PTSD / TF-CBT (adult) | Update memory; change appraisals; drop maintaining strategies; reclaim life | Ehlers–Clark cognitive model |
| Child TF-CBT | PRACTICE components + caregiver when safe | Cohen/Mannarino/Deblinger |
| EMDR | Eight phases; dual-attention bilateral stimulation while processing targets | Shapiro; AIP model |
Non-trauma-focused approaches (present-centred therapy, pure supportive therapy, skills-only without memory work) are important comparators and adjuncts, not default “first-line PTSD cures” when trauma-focused care is feasible.[8][10]
Epidemiology and system risk (therapy lens)
PTSD risk after trauma is conditional (many exposed never meet criteria); interpersonal and combat trauma drive high service need. From a therapy systems view, the examinable risks are: waitlists for trained clinicians; incomplete “trauma-informed” branding without protocol; high dropout in exposure packages; and therapist drift (avoiding trauma processing). Comorbid depression, substance use, personality pathology, and ongoing threat increase complexity and sequencing decisions.[8][9][17]
Mechanisms (pathophysiology of maintenance and change)
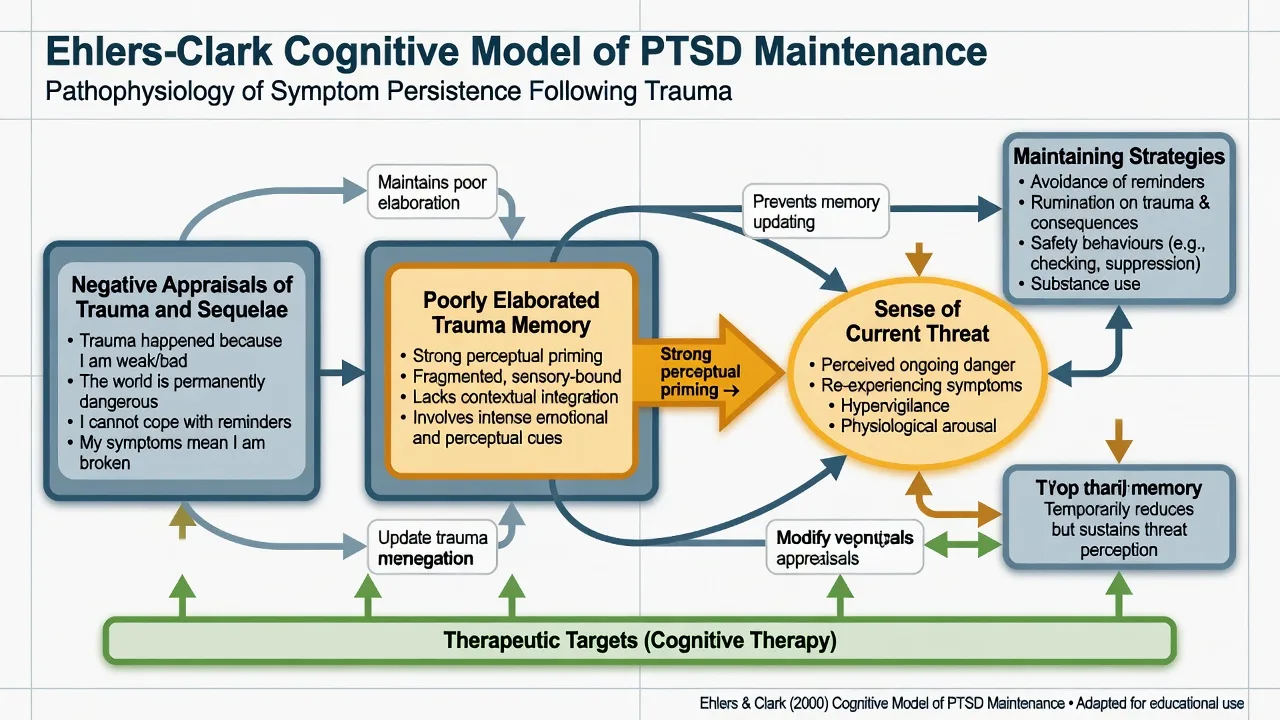
Ehlers–Clark cognitive model
Persistent PTSD reflects processing that produces a sense of serious current threat. Two engines: (1) excessively negative appraisals of the trauma and/or its sequelae; (2) autobiographical memory disturbance — poorly elaborated, strongly perceptually primed memories that reappear as if “happening now.” Strategies meant to control threat (avoidance, thought suppression, rumination, safety behaviours, substances) block updating and maintain symptoms. CT-PTSD targets memory updating, appraisal change, and strategy drop while rebuilding valued activity (“reclaiming life”).[1][2]
Exposure / emotional processing (PE)
PE activates the trauma-related fear structure through imaginal and in vivo exposure so corrective information can be encoded (the feared catastrophe does not occur; anxiety peaks and falls; contexts can be safe). Modern teaching also uses inhibitory learning language: expectancy violation, varied contexts, removal of safety behaviours. Meta-analysis supports large PE effects for PTSD.[3][4]
CPT: stuck points
CPT focuses on stuck points — unhelpful beliefs that maintain PTSD. Classic exam contrast: assimilation (e.g. self-blame that preserves a just-world belief: “It was my fault”) versus over-accommodation (global conclusions: “No one can be trusted; the world is entirely dangerous”). Written impact statements and structured cognitive worksheets operationalise change; full CPT includes a written trauma account, while CPT-C omits it with evidence of efficacy in dismantling work.[6][7]
EMDR: AIP and dual attention
EMDR conceptualises symptoms as inadequately processed traumatic memory networks (Adaptive Information Processing). Standard work uses dual attention: holding a target memory representation while receiving bilateral stimulation (usually guided eye movements; alternatives include taps/tones). Shapiro’s clinical framework organises care into eight phases. Laboratory and treatment dismantling signals suggest eye movements can reduce vividness/emotionality of aversive memories (working-memory taxation account is examinable), though mechanism debates continue and fidelity matters.[11][12][13]
Clinical presentation of “good protocol care”
Examiners recognise protocol signals in notes.[2][3][6][11]
- PE: hierarchy of avoided situations; imaginal exposure with recording and homework listening; SUDS tracking; post-exposure processing of meaning.[3][4]
- CPT: impact statement; ABC sheets; stuck-point log; challenging questions / patterns of problematic thinking modules.[6]
- CT-PTSD: hot-spot updating, discrimination training (then vs now), behavioural experiments, site visits when safe, reclaiming-life activity schedule.[2]
- EMDR: target assessment (image, negative cognition, positive cognition, VoC, emotion, SUDs, body sensation), desensitisation sets, installation, body scan, closure, re-evaluation next session.[11]
Therapy-interfering patterns: severe dissociation mid-set, no homework, substance use immediately before sessions, ongoing unsafe relationships, or clinician collusion with avoidance — address with formulation review, safety planning, and fidelity rather than silent collusion with avoidance.[3][10][16]
Differential: choosing a package
| Question | Discriminator |
|---|---|
| TF-CBT family vs EMDR | Both first-line in major syntheses; choose by preference, access, competence, formulation — not ideology |
| Trauma-focused vs present-centred | Trauma focus generally superior for PTSD symptoms vs waitlist/usual care; active non-TF controls still often lose on PTSD outcomes |
| Psychotherapy vs medication alone | SSRIs (e.g. sertraline) and related agents have RCT evidence; trauma-focused therapy is preferred first-line when available |
| Single-incident vs complex childhood abuse | Standard PE/CPT/EMDR still often effective; STAIR, DBT-PTSD, intensified PE are tools for complexity — not automatic exclusion from TF care |
| Wrong protocol | Grief-focused therapy, pure ERP for OCD, panic interoceptive work — use when those maintaining processes dominate |
Assessment and readiness
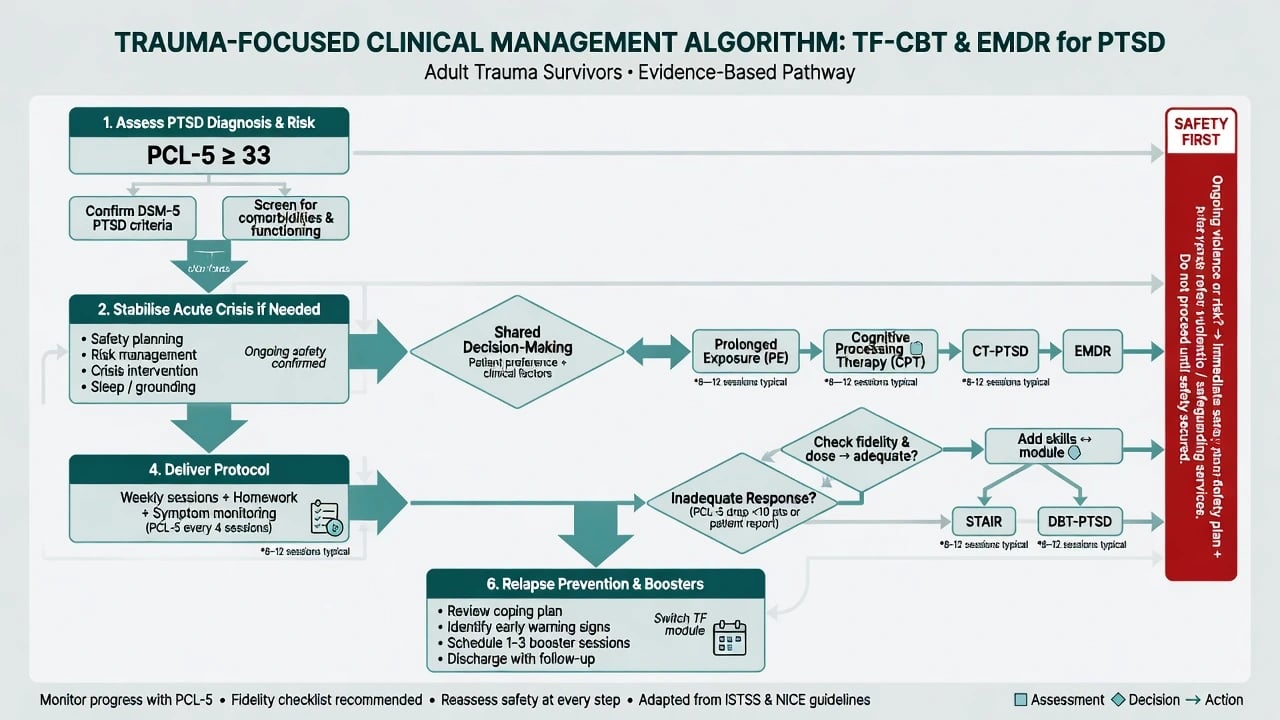
Assessment checklist: (1) trauma and diagnosis — Criterion A clarity; DSM-5-TR four-cluster PTSD vs ICD-11 PTSD/complex PTSD as relevant; differential (depression, BPD, grief, psychosis, substance-induced); (2) measures — PCL-5 for serial monitoring; CAPS-5 when structured gold-standard diagnosis is needed; (3) risk — suicide, self-harm, violence, dependents, safeguarding; (4) ongoing safety — if the perpetrator is still present, physical safety planning precedes in vivo tasks that increase contact risk; (5) readiness for trauma focus — can attend; can tolerate moderate affect with a plan; life-threatening behaviours relatively controlled; substance pattern compatible with learning; dissociation manageable with preparation; alliance workable; (6) shared decision — explain PE/CPT/CT-PTSD/EMDR options; prior therapy; cultural preferences; literacy/language.[10][17]
Acute / emergency interface
Trauma-focused sessions are elective structured care. Override with acute management when risk or medical instability dominates: active high suicide risk needing containment or medical treatment after overdose/self-injury; severe intoxication/withdrawal, mania, delirium, or acute psychosis; medical instability or seizure risk requiring adaptation (especially EMDR stimulation choices); immediate interpersonal violence without a safe base. After stabilisation, return to a trauma-focused plan rather than abandoning evidence-based care forever. Temporary intensification of skills, grounding, and crisis plans is appropriate mid-course distress — distress rise during exposure is expected, not automatic protocol failure.[3][10][17]
Definitive management
Guideline and synthesis position
Cochrane and subsequent systematic reviews/meta-analyses support individual trauma-focused CBT and EMDR as effective psychological treatments for chronic PTSD in adults; broader AHRQ-style and updated meta-analyses reinforce large effects for trauma-focused packages versus control conditions. Lewis and colleagues’ 2020 synthesis strengthens confidence in recommending CBT-T and EMDR as first-line psychological therapies. ISTSS guideline processes organise prevention and treatment recommendations by evidence strength.[8][9][10][17]
NICE (PTSD pathway teaching): offer trauma-focused CBT or EMDR for adults with PTSD (details and session bands per current local guideline version). APA PTSD guideline tradition: strong recommendations for trauma-focused psychotherapies including PE, CPT, CT, and EMDR family interventions. RANZCP: expects psychological therapy competence in training; trauma-focused options should be available or referred. Always check the current local pathway for exact session numbers and digital options.[8][10][17]
Prolonged exposure (practical map)
Psychoeducation → breathing retraining if used → in vivo hierarchy of safe avoided cues → imaginal exposure to the trauma narrative with processing → homework (listen to imaginal recording; complete in vivo tasks). Foa’s multi-site work showed PE effective in academic and community clinics; PE with or without formal cognitive restructuring both improved PTSD; Schnurr demonstrated PE benefit in women veterans versus present-centred therapy.[3][4][5]
CPT (practical map)
Orientation → impact statement → identification of stuck points → cognitive work (ABC, challenging questions, patterns of problematic thinking) → written trauma account in full CPT (optional in CPT-C) → final impact statement. Efficacy extends to military-related PTSD in veteran samples.[6][7]
CT-PTSD / adult TF-CBT (practical map)
Shared formulation from the Ehlers–Clark model; reclaiming-life activities early; trauma memory work with updating (including “then vs now” discrimination); behavioural experiments testing appraisals; dropping rumination/safety behaviours; site visits when indicated and safe.[1][2]
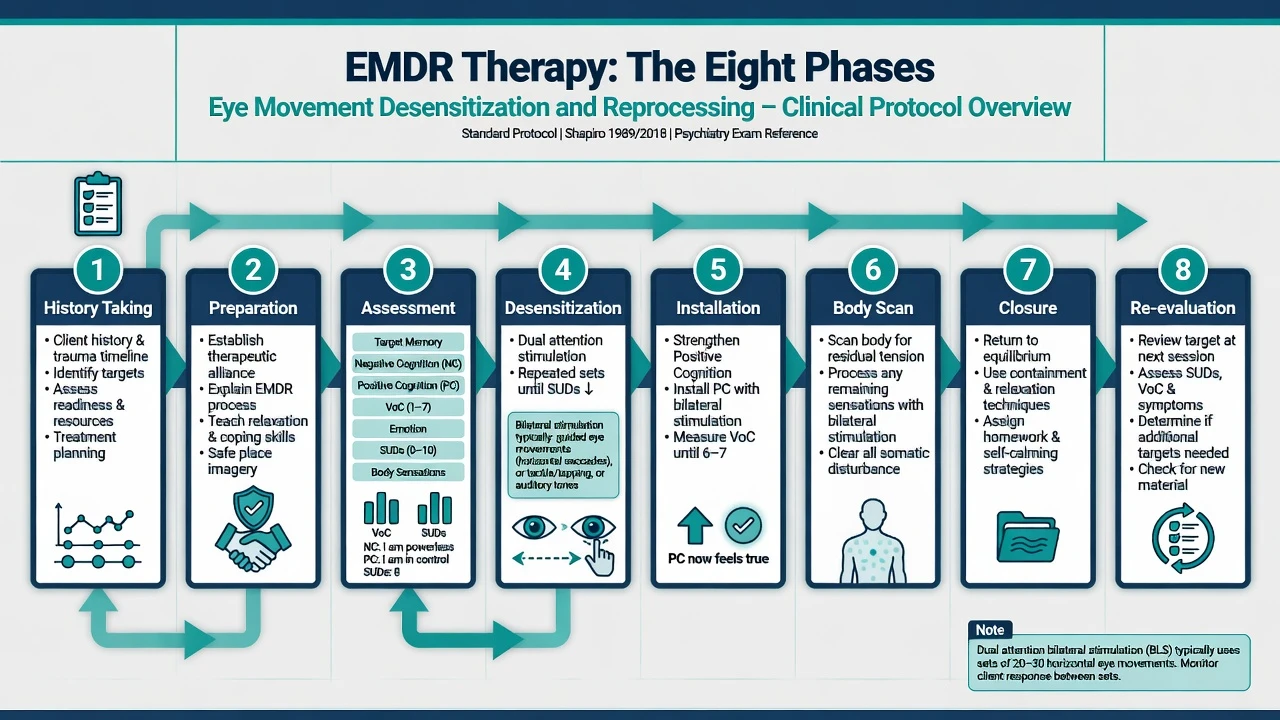
EMDR eight phases (viva list)
Standard EMDR phases: (1) history and treatment planning; (2) preparation (alliance, psychoeducation, resources/grounding); (3) assessment of target (image, NC, PC, VoC, emotion, SUDs, body); (4) desensitisation (dual-attention sets until SUDs fall); (5) installation of positive cognition; (6) body scan; (7) closure; (8) re-evaluation next session. Target sequencing often past → present triggers → future templates. Do not reduce EMDR to “wiggling fingers without phases.”[11][12]
Child and adolescent TF-CBT
TF-CBT (Cohen, Mannarino, Deblinger) is components-based care for trauma-related symptoms, typically involving a non-offending caregiver when safe. Multisite RCT evidence in sexual-abuse-related PTSD symptoms showed superiority to child-centred therapy. PRACTICE mnemonic (exam aid): Psychoeducation/parenting, Relaxation, Affective expression/modulation, Cognitive coping, Trauma narrative, In vivo mastery, Conjoint sessions, Enhancing safety.[14]
Complex presentations: skills, sequencing, and the de Jongh critique
STAIR (skills training in affective and interpersonal regulation) followed by exposure is a classic phase-based package for childhood-abuse-related PTSD.[15] A critical literature argues against mandatory lengthy stabilisation phases for all “complex” patients when trauma-focused therapy is indicated and feasible — delay can be iatrogenic if it becomes permanent avoidance of processing.[16] Intensified PE, concurrent skills, and specialised packages (e.g. DBT-PTSD vs CPT in complex childhood-abuse presentations — cross-link complex PTSD topic) are tools for matching intensity, not excuses to never process trauma.
Pharmacotherapy interface
Evidence-based medications for PTSD include SSRIs such as sertraline (RCT efficacy) and paroxetine, with venlafaxine also supported in major trials (see PTSD hub for dosing/monitoring). Medication is appropriate when psychotherapy is unavailable, declined, partially effective, or when comorbid depression/anxiety needs parallel treatment — not a reason to omit offering trauma-focused therapy. Avoid default long-term benzodiazepines for PTSD core treatment.[18][10]
Example exam-safe SSRI line (confirm local formulary and product information): sertraline oral, often start 25–50 mg daily, titrate toward evidence-based PTSD ranges (commonly up to 150–200 mg daily as tolerated) with monitoring for activation, suicidality risk early in treatment (especially youth), sexual side effects, hyponatraemia in older adults, and serotonin toxicity risk with combinations.[18]
Stepped care and incomplete response
Guided self-help trauma programmes where commissioned → individual TF therapy → high-intensity or specialist complex trauma pathways. If one TF modality fails after adequate dose and fidelity, switch to another TF package (e.g. PE → EMDR or CPT) rather than indefinite non-specific counselling.[9][10]
Subtypes and scenarios
- Single-incident civilian trauma — standard PE/CPT/CT-PTSD/EMDR often sufficient.[2][3]
- Military/veteran — PE and CPT evidence base including Schnurr and Monson trials.[5][7]
- Sexual assault / IPV — CPT and PE classic samples; safety planning mandatory.[6]
- Childhood abuse in adults — TF therapies still core; STAIR/DBT-PTSD/intensified PE for complexity.[15][16]
- Comorbid SUD — integrated or carefully sequenced care; infinite wait for abstinence can perpetuate PTSD-driven use.
- BPD traits — Stage 1 behavioural control (e.g. DBT) then trauma focus, or specialist DBT-PTSD pathways.
- Early post-trauma — watchful waiting vs early intervention per guideline; avoid harmful single-session forced debriefing culture (cross-link ASD/PTSD hub).
Complications and pitfalls
| Pitfall | Correction |
|---|---|
| Endless stabilisation | Time-limited skills then trauma focus when feasible; de Jongh critique |
| Unsafe in vivo tasks | Safety first |
| Pseudo-EMDR / pseudo-PE | Protocol fidelity, supervision |
| Benzo-first chronic care | Prefer TF therapy ± evidence-based antidepressant |
| Mid-course distress = “failed” | Expected activation; process and support |
| No measures | Serial PCL-5 or equivalent |
| Cultural dismissal | Adapt language, family roles, shame narratives; use interpreters |
Prognosis and disposition
Trauma-focused therapies produce large average symptom reductions versus control conditions in meta-analyses; many patients achieve clinically meaningful gains, though residual symptoms and comorbidity are common. Poorer response associates with ongoing trauma, severe comorbidity, low engagement, and non-adherent delivery. Preferred disposition is outpatient specialist TF therapy with crisis plan; step up only for safety/severity. Plan relapse prevention, early-warning signs, and boosters.[4][8][9][10]
Special populations
- Children/adolescents: TF-CBT with caregiver when safe is first-line teaching; developmental adaptation of narrative and exposure.[14]
- Older adults: slower pacing, sensory/cognitive adaptations, medical comorbidity review.
- Pregnancy: prioritise psychotherapy; medication risk–benefit if needed (cross-link perinatal psychopharmacology).
- ID/autism: simplified language, longer sessions, visual supports, adapted EMDR only with training.
- Indigenous and culturally diverse clients: cultural safety, community supports, avoid imposing metaphors; trauma meanings may be collective.
- Refugees/asylum: ongoing threat, legal uncertainty, torture-informed care, interpreters.
Evidence map (high-yield names)
- Model: Ehlers and Clark 2000; CT-PTSD development Ehlers 2005.[1][2]
- PE: Foa 2005 multi-site; Powers 2010 meta; Schnurr 2007 women veterans.[3][4][5]
- CPT: Resick 2008 dismantling; Monson 2006 military-related PTSD.[6][7]
- Syntheses/guidelines: Bisson Cochrane 2013; Cusack 2016; Lewis 2020; ISTSS 2019 process paper.[8][9][10][17]
- EMDR: Shapiro framework; Lee and Cuijpers 2013 eye-movement contribution; Cuijpers 2020 broader EMDR meta (read critically for outcomes beyond PTSD).[11][12][13]
- Child TF-CBT: Cohen 2004 multisite RCT.[14]
- Complex: Cloitre STAIR 2002; de Jongh 2016 critical analysis of phase-based mandates.[15][16]
- Pharma adjunct: Brady sertraline 2000.[18]
Exam pearls
- List EMDR’s eight phases under pressure.[11]
- Draw Ehlers–Clark in 30 seconds: appraisals + memory + strategies → current threat.[1]
- CPT: assimilation vs over-accommodation stuck points.[6]
- Complex ≠ automatic years of skills-only; cite the de Jongh teaching counterpoint.[16]
- Child TF-CBT = PRACTICE + caregiver when safe.[14]
- After failed TF trial with fidelity, switch TF modality, do not abandon trauma focus.[9][10]
- Monitor with PCL-5; expect temporary distress during processing.[3]
- Safety of environment beats heroic in vivo homework into danger.[17]
References
- [1]Ehlers A, Clark DM A cognitive model of posttraumatic stress disorder Behav Res Ther, 2000.PMID 10761279
- [2]Ehlers A, Clark DM, Hackmann A, et al. Cognitive therapy for post-traumatic stress disorder: development and evaluation Behav Res Ther, 2005.PMID 15701354
- [3]Foa EB, Hembree EA, Cahill SP, Rauch SA, et al. Randomized trial of prolonged exposure for posttraumatic stress disorder with and without cognitive restructuring: outcome at academic and community clinics J Consult Clin Psychol, 2005.PMID 16287395
- [4]Powers MB, Halpern JM, Ferenschak MP, Gillihan SJ, Foa EB A meta-analytic review of prolonged exposure for posttraumatic stress disorder Clin Psychol Rev, 2010.PMID 20546985
- [5]Schnurr PP, Friedman MJ, Engel CC, Foa EB, Shea MT, et al. Cognitive behavioral therapy for posttraumatic stress disorder in women: a randomized controlled trial JAMA, 2007.PMID 17327524
- [6]Resick PA, Galovski TE, Uhlmansiek MO, Scher CD, et al. A randomized clinical trial to dismantle components of cognitive processing therapy for posttraumatic stress disorder in female victims of interpersonal violence J Consult Clin Psychol, 2008.PMID 18377121
- [7]Monson CM, Schnurr PP, Resick PA, Friedman MJ, et al. Cognitive processing therapy for veterans with military-related posttraumatic stress disorder J Consult Clin Psychol, 2006.PMID 17032094
- [8]Bisson JI, Roberts NP, Andrew M, Cooper R, Lewis C Psychological therapies for chronic post-traumatic stress disorder (PTSD) in adults Cochrane Database Syst Rev, 2013.PMID 24338345
- [9]Cusack K, Jonas DE, Forneris CA, Wines C, et al. Psychological treatments for adults with posttraumatic stress disorder: A systematic review and meta-analysis Clin Psychol Rev, 2016.PMID 26574151
- [10]Lewis C, Roberts NP, Andrew M, Starling E, Bisson JI Psychological therapies for post-traumatic stress disorder in adults: systematic review and meta-analysis Eur J Psychotraumatol, 2020.PMID 32284821
- [11]Shapiro F The role of eye movement desensitization and reprocessing (EMDR) therapy in medicine: addressing the psychological and physical symptoms stemming from adverse life experiences Perm J, 2014.PMID 24626074
- [12]Lee CW, Cuijpers P A meta-analysis of the contribution of eye movements in processing emotional memories J Behav Ther Exp Psychiatry, 2013.PMID 23266601
- [13]Cuijpers P, Veen SCV, Sijbrandij M, Yoder W, Cristea IA Eye movement desensitization and reprocessing for mental health problems: a systematic review and meta-analysis Cogn Behav Ther, 2020.PMID 32043428
- [14]Cohen JA, Deblinger E, Mannarino AP, Steer RA A multisite, randomized controlled trial for children with sexual abuse-related PTSD symptoms J Am Acad Child Adolesc Psychiatry, 2004.PMID 15187799
- [15]Cloitre M, Koenen KC, Cohen LR, Han H Skills training in affective and interpersonal regulation followed by exposure: a phase-based treatment for PTSD related to childhood abuse J Consult Clin Psychol, 2002.PMID 12362957
- [16]De Jongh A, Resick PA, Zoellner LA, van Minnen A, et al. CRITICAL ANALYSIS OF THE CURRENT TREATMENT GUIDELINES FOR COMPLEX PTSD IN ADULTS Depress Anxiety, 2016.PMID 26840244
- [17]Bisson JI, Berliner L, Cloitre M, Forbes D, et al. The International Society for Traumatic Stress Studies New Guidelines for the Prevention and Treatment of Posttraumatic Stress Disorder: Methodology and Development Process J Trauma Stress, 2019.PMID 31283056
- [18]Brady K, Pearlstein T, Asnis GM, Baker D, et al. Efficacy and safety of sertraline treatment of posttraumatic stress disorder: a randomized controlled trial JAMA, 2000.PMID 10770145