Psych · Public and community psychiatry — collaborative care and primary care
Collaborative care and primary care psychiatry
Also known as Collaborative Care Model · CoCM · IMPACT model · TEAMcare · Primary care mental health · Integrated behavioural health · Measurement-based care primary care · Psychiatric consultation primary care · Stepped care depression · AIMS Center collaborative care
Exam-exhaustive fellowship reference on collaborative care and primary care psychiatry: Wagner Chronic Care Model roots, five CoCM principles, IMPACT/TEAMcare/CADET/Cochrane evidence, PHQ-9/GAD-7 measurement-based care, caseload review, tele-collaborative care, multimorbidity, fidelity and regional guidelines. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Collaborative care is the most rigorously tested organisational intervention for depression and anxiety in primary care. Fellowship examiners expect you to define the model (and distinguish it from co-location), name landmark trials (IMPACT, TEAMcare, CADET), quote systematic evidence (Gilbody, Archer Cochrane, Thota), describe the care manager–PCP–psychiatric consultant triad, operationalise measurement-based care, and know when to step up to specialty or crisis pathways.[1][2][4][11]

Overview and definition
Primary care psychiatry is the clinical and systems domain in which most common mental disorders (CMD) — depression, anxiety, mixed presentations, distress with long-term conditions — first present and are largely treated. Traditional referral psychiatry cannot absorb that volume; collaborative care redesigns the primary care platform rather than relying on sequential specialty queues.[14]
Collaborative Care Model (CoCM) (AIMS Center lineage from Unützer, Katon and colleagues) is a multicomponent chronic-disease-style programme: proactive identification, a shared caseload registry, a care manager who provides structured support and measurement, evidence-based pharmacological and brief psychological treatments delivered with the PCP, and systematic psychiatric caseload review for non-improvers.[1][14]
| Model | Structure | What examiners expect |
|---|---|---|
| Usual primary care | Episodic GP visits; ad hoc referral | High undetected non-response |
| Co-location | MH clinician on site; often referral-in | Useful access, not automatically CoCM |
| Consultation-liaison | Specialist advice on referred cases | Reactive; limited population reach |
| Shared care | Joint plan PCP + specialist | Variable fidelity; may lack registry |
| Collaborative care (CoCM) | Team + registry + measurement + caseload review + treatment-to-target | Preferred organisational model for CMD |
Classification — five principles and the Chronic Care Model
Wagner Chronic Care Model (CCM) supplies the systems DNA: productive interactions between an informed, activated patient and a prepared, proactive practice team, supported by self-management support, delivery system design, decision support, clinical information systems, community resources, and health care organisation priorities.[7] Collaborative depression care is CCM applied to mental disorders.[14]
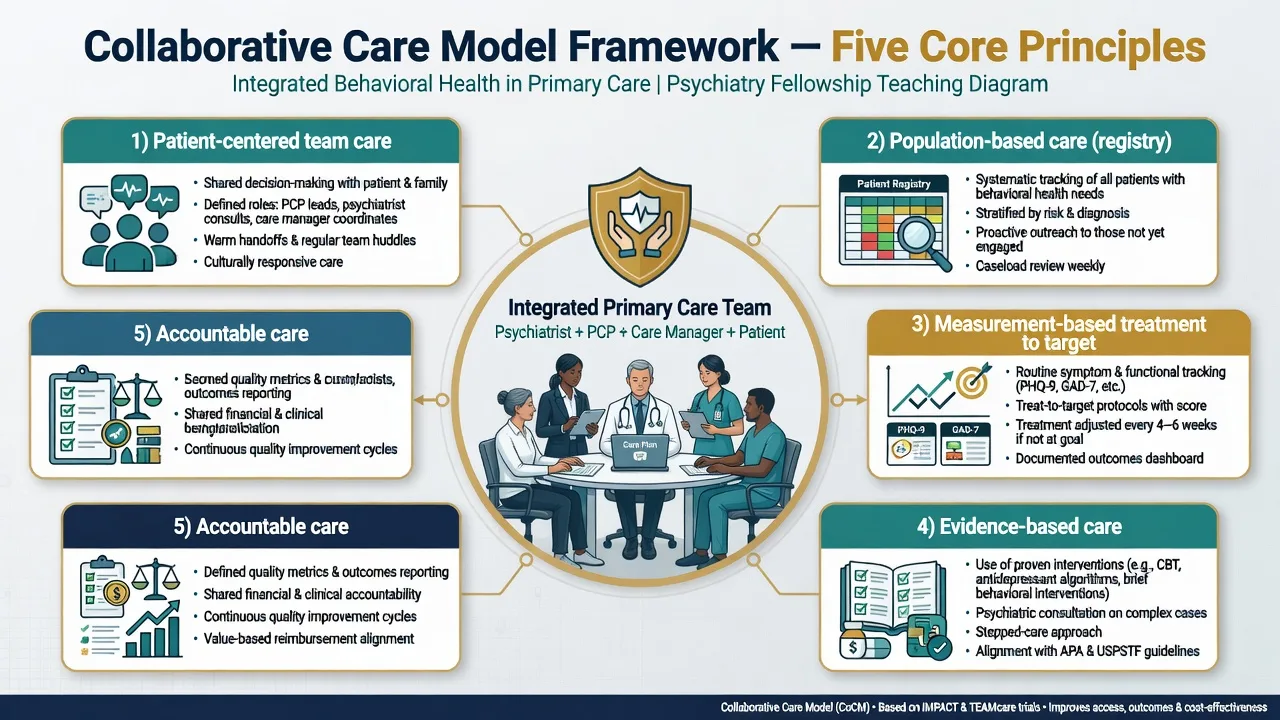
Five core CoCM principles (exam list — memorise): patient-centered team care; population-based registry care; measurement-based treatment to target; evidence-based care; accountable care for the whole caseload.[1][14]
- Patient-centered team care — PCP, behavioural health care manager, psychiatric consultant working from one plan.[1]
- Population-based care — whole enrolled caseload tracked on a registry; non-attenders are still on the radar.[14]
- Measurement-based treatment to target — serial validated scales drive intensification when not improving.[1]
- Evidence-based care — guideline antidepressants, brief structured psychotherapy, self-management.[14]
- Accountable care — the team owns outcomes for the caseload, not only for those who happen to rebook.[1][14]
Roles. PCP, behavioural health care manager, and psychiatric consultant form the CoCM triad.[1][14]
| Role | Core functions |
|---|---|
| Primary care provider | Diagnosis partnership, prescribe, medical differential, ongoing relationship |
| Care manager (nurse, social worker, psychologist, or trained BHCM) | Engagement, psychoeducation, brief behavioural interventions, serial measures, outreach, registry hygiene |
| Psychiatric consultant | Regular caseload review of non-responders; brief direct consult/assessment when needed; education of team — not full intake of every mild case |
Epidemiology and risk
Primary care mental health headlines
Most depression and anxiety is managed outside specialty psychiatry. Usual primary care often fails to achieve guideline-level intensity, follow-up, and adjustment — the problem Katon collaborative management trials and IMPACT were designed to fix.[1][13] Depression co-occurring with diabetes or cardiovascular disease worsens self-management and outcomes; multicondition collaborative care targets both domains.[3][12]
Pathophysiology and systems mechanisms
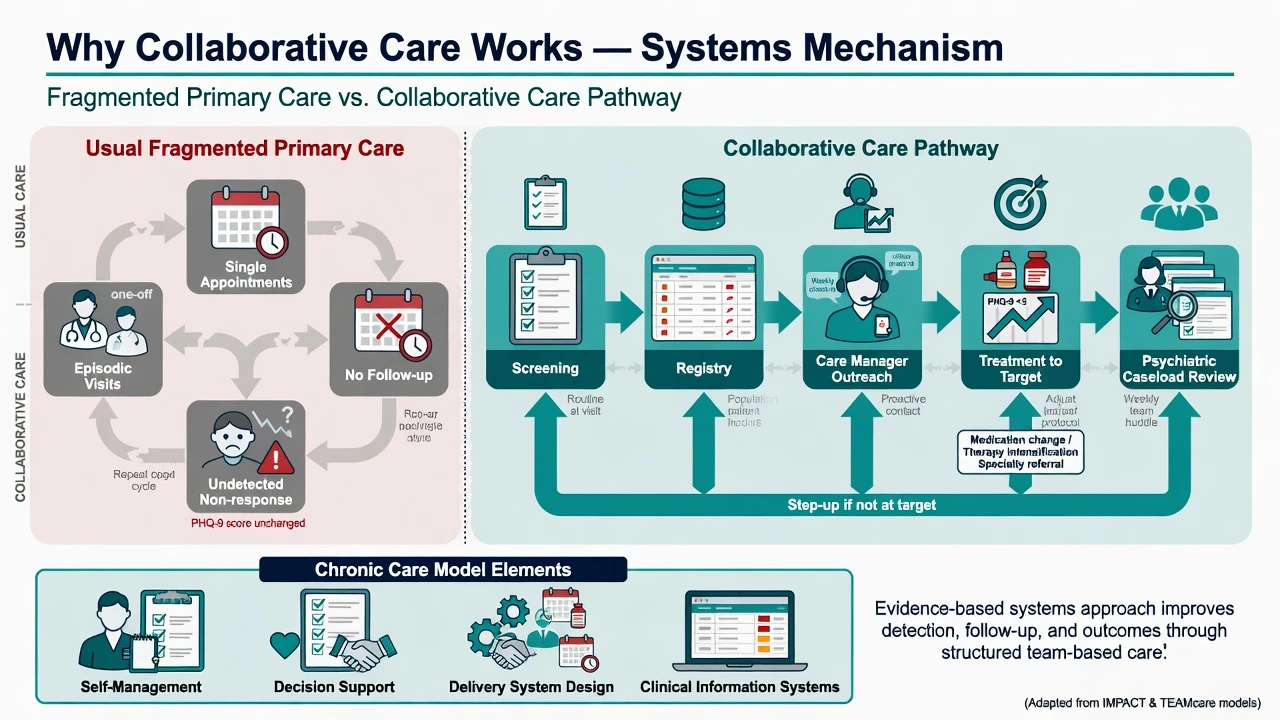
The "pathophysiology" examiners want is organisational: recognition, initiation, intensity, follow-up, and adjustment failures in usual primary care.[6][14]
- Recognition failure — somatic presentations, short appointments, no routine screening.[6]
- Initiation failure — diagnosis without treatment start.[14]
- Intensity failure — subtherapeutic antidepressant dose/duration; no structured psychotherapy access.[13]
- Follow-up failure — no proactive contact; non-attenders disappear.[6]
- Adjustment failure — therapeutic inertia when symptoms persist.[14]
CCM components (self-management support, decision support, redesigned delivery, clinical information systems) reverse these failure modes. Measurement-based care applies the same logic as titrating hypertension: you do not declare "blood pressure treated" after one prescription without re-check.[7][8]
Depression–chronic disease bidirectionality. Depressive symptoms impair adherence to diet, exercise, medication, and follow-up for diabetes and coronary disease; medical burden and inflammation pathways worsen mood. TEAMcare nurses treated depression and cardiometabolic targets in one package and improved both.[3]
Clinical presentation in primary care
Typical CoCM populations: major depression and dysthymia in adult and late-life primary care (IMPACT age ≥60), anxiety disorders, mixed anxiety–depression, and depression with long-term physical conditions.[1][2][12] Patients often present with fatigue, pain, sleep disturbance, or poor control of diabetes/BP rather than a psychiatric narrative. Late-life depression may be under-recognised as "normal ageing."[1]
Caseload review surfaces a signature exam vignette: the patient who "is on an SSRI" but still has PHQ-9 of 16 at week 8 with no dose change, no therapy, and no specialist review — organisational failure, not patient failure.[6][14]
Differential: who belongs in CoCM vs specialty now
| Keep / enrol in CoCM pathway (after assessment) | Escalate / do not park in routine CoCM alone |
|---|---|
| Mild–moderate depression/anxiety with risk manageable in primary care | Active suicidal intent/plan, recent attempt, inability to contract for safety |
| Stable chronic depression needing structured follow-up | Acute psychosis, mania, severe mixed states |
| Depression with LTC needing multicondition support | Severe anorexia, catatonia, NMS/serotonin emergency |
| Ambivalent but engageable patients | High-risk forensic/violence scenarios needing specialist risk services |
| Complex trauma needing intensive specialty psychotherapy when unavailable in CoCM |
Always complete a differential for organic, bipolar, substance-induced, grief, and dementia before locking a "primary care depression" label. PHQ-9 is a severity and screening tool, not a full diagnostic interview.[8]
Assessment and measurement-based care
Structure. History (mood, anxiety, sleep, substance, medical, past treatment response), focused MSE, suicide/homicide/vulnerability risk, functional impact, collateral when needed, and shared decision-making about goals.[14]
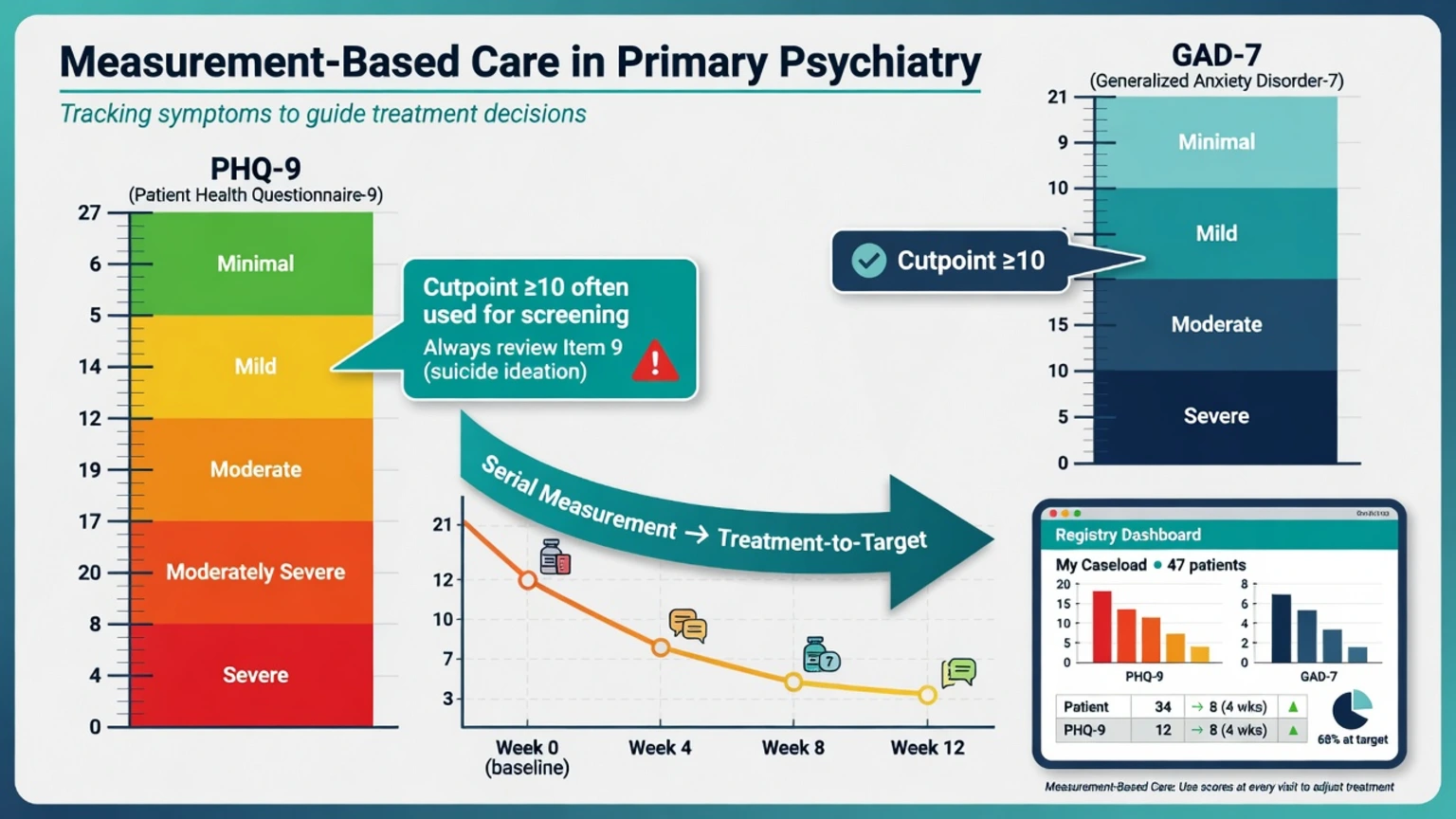
PHQ-9. Nine DSM-aligned items scored 0–3 (total 0–27). Common severity bands: 0–4 minimal, 5–9 mild, 10–14 moderate, 15–19 moderately severe, 20–27 severe. A total of 10 or greater is a widely used screening threshold with good sensitivity/specificity for major depression in validation samples — still confirm clinically.[8] Item 9 (thoughts of being better off dead or of hurting yourself) must always be reviewed; positive answers trigger structured risk assessment, not silent charting.[8]
GAD-7. Seven items, total 0–21; score of 10 or greater is a common screen cut-point for generalised anxiety with validated operating characteristics; elevated scores also flag other anxiety disorders clinically.[9]
Registry and caseload review. Every enrolled patient appears on a list with last measure, treatment, and weeks since change. The psychiatric consultant systematically reviews non-improvers (and high-risk flags) with the care manager on a regular cadence — the high-leverage specialist activity of CoCM.[1][14]
Investigations
Before antidepressants in primary care: targeted history for bipolarity, medical review, pregnancy status when relevant, baseline FBC/U&E/LFT/TSH as clinically indicated, ECG when cardiac risk or QT-prolonging combinations, and metabolic baseline if atypical antipsychotics ever enter the plan. Serial PHQ-9/GAD-7 is the response "investigation."[8][14] Escalate imaging/EEG/autoimmune work-ups when organic red flags appear — CoCM does not replace medical reasoning.
Acute / emergency management
[1] [2]In primary care: means restriction counselling, crisis contacts, same-day mental health crisis team or ED, document risk formulation, and communicate with care manager so the registry does not falsely list the patient as "stable follow-up."[8]
Definitive management — algorithm and stepped care
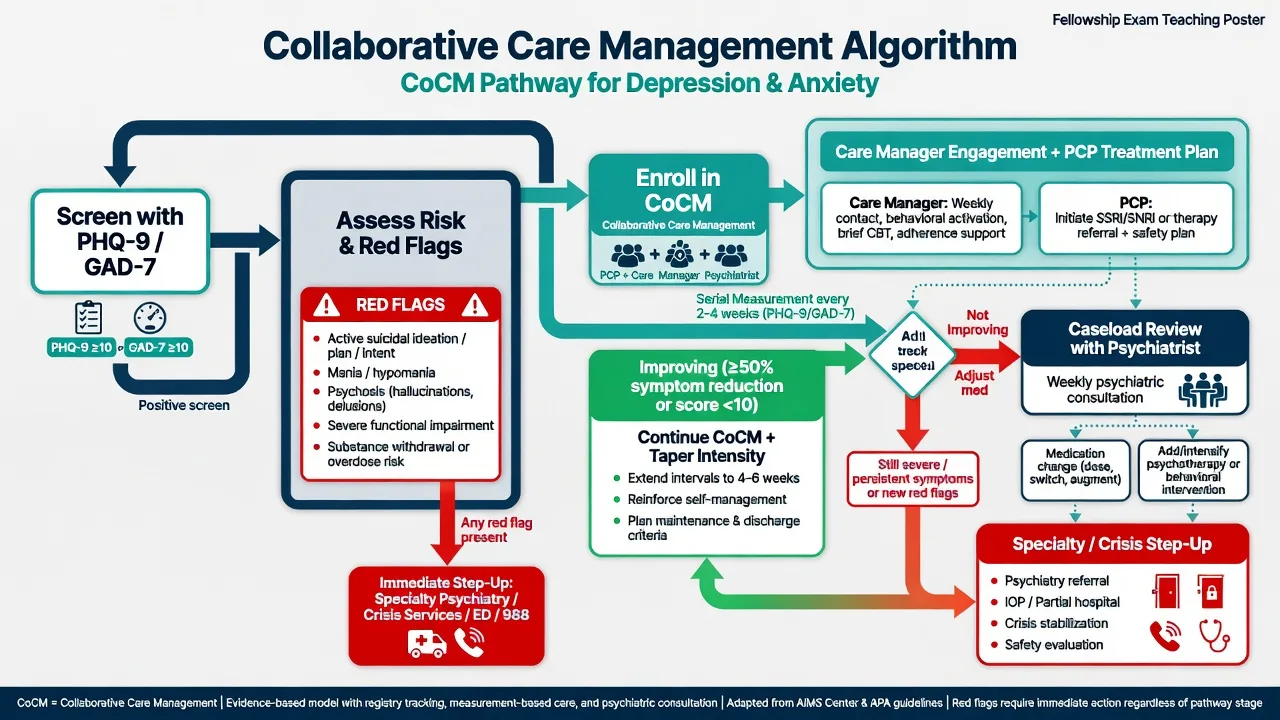
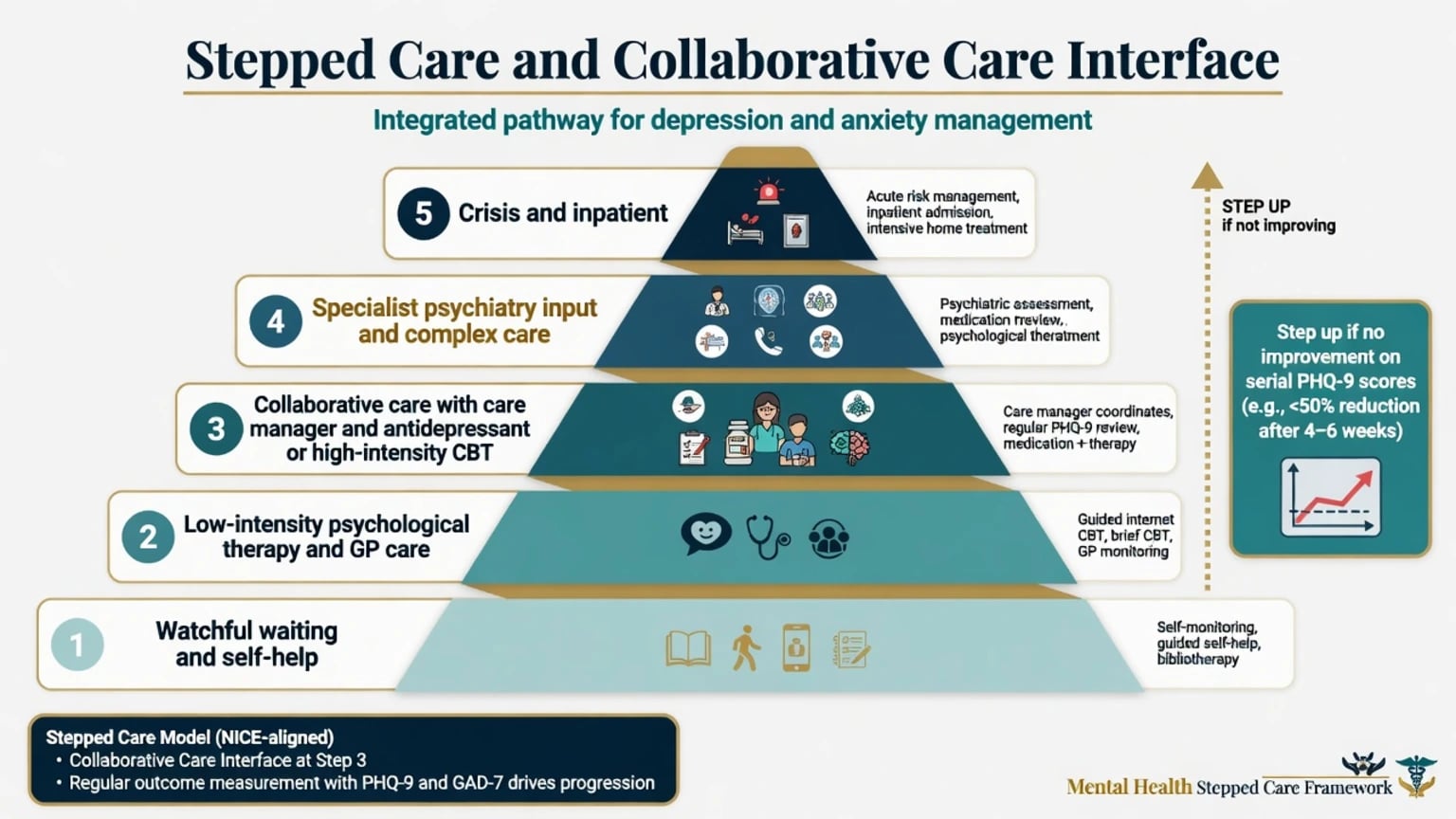
Operational sequence. Identify, risk-triage, enrol, treat, measure, adjust, and step up — the CoCM treatment-to-target loop.[1][2][5][14]
- Identify — opportunistic or systematic screening; clinical diagnosis.[1]
- Risk triage — emergency vs CoCM-eligible.[2]
- Enrol — shared plan, registry entry, care manager assignment.[14]
- Treat — evidence-based antidepressant and/or structured brief psychological therapy (e.g. behavioural activation, problem-solving, CBT elements) with self-management support.[5]
- Measure — PHQ-9/GAD-7 at regular intervals (commonly every 2–4 weeks in active phase).[8]
- Adjust — if not improving, change dose/agent/modality after caseload review.[1]
- Step up — specialty psychiatry, intensive psychological therapy, or crisis care when indicated.[2][14]
Pharmacotherapy principles in primary care CoCM (link to dedicated antidepressant topics for full monographs): start an evidence-based first-line agent at a therapeutic dose with clear review date; titrate using side-effect and scale data; do not declare failure before adequate dose and duration unless intolerability or risk forces change. Care managers support adherence and side-effect troubleshooting between PCP visits.[13][16]
Psychological elements. Brief structured therapies and behavioural activation are commonly embedded; fidelity and training of care managers matter more than branding. Meta-regression work suggests key active ingredients include mental health professional input and case management intensity components — interpret as support for structured multi-element packages, not a single magic module.[6]
Psychiatric consultant workflow. Scheduled caseload conferences; recommendations documented to PCP; direct assessment when diagnosis is unclear, risk is high, or treatment resistance emerges. This multiplies specialist reach compared with full traditional intakes for every mild case.[1][14]
Subtypes and scenarios
| Scenario | Landmark / model | Exam takeaway |
|---|---|---|
| Late-life depression | IMPACT (Unützer 2002) | Depression care manager + PCP + psychiatrist; better outcomes than usual care |
| Depression + diabetes/CAD | TEAMcare (Katon 2010) | Multicondition nurses improve depression and medical targets |
| UK primary care depression | CADET (Richards 2013) | Collaborative care effective and preferred by patients to 12 months |
| Depression + diabetes/CVD multimorbidity (UK) | Coventry 2015 | Integrated collaborative care reduced depression, aided self-management |
| Rural PTSD | Fortney telemedicine CoCM | Off-site team + telehealth improves engagement and PTSD outcomes |
| Anxiety disorders | Archer Cochrane | Collaborative care benefits anxiety as well as depression |
Youth, perinatal, Indigenous, and LMIC settings. Principles transfer (team, measurement, stepped intensity, cultural safety) but programme design must match local workforce, funding, and cultural protocols. Task-sharing frameworks (e.g. mhGAP-style primary care packages) are related public-health cousins — do not claim identical CoCM RCT fidelity without local evidence.[14]
Complications and pitfalls
- Fidelity decay — drop registry, drop measures, drop caseload review; outcomes collapse toward usual care.[6][14]
- Screening without capacity — identifies illness then strands patients.
- Ignoring item 9.
- Therapeutic inertia at high PHQ-9.
- Overloading care managers so outreach becomes impossible.
- Mislabeling liaison letters or co-location as CoCM in essays.
- Using CoCM as rationing to block needed specialty care for complex SMI.
Prognosis and disposition
Cumulative meta-analysis showed collaborative care superior to usual care for depression outcomes by the early 2000s, with benefits extending beyond short-term windows.[4] Cochrane review concluded collaborative care improves depression and anxiety outcomes versus usual care.[2] Community Guide (Thota) recommended collaborative care for depressive disorders based on robust evidence for symptoms, adherence, response, and remission-related outcomes.[11] IMPACT demonstrated large clinical gains in late-life depression; longer-term analyses found favourable total cost trajectories versus usual care over multi-year horizons in that programme context.[1][15]
Disposition. Stay in primary care CoCM when improving and risk is managed; intensify within CoCM when not at target; step to specialty for complexity, treatment resistance, or diagnostic uncertainty; use crisis pathways for acute risk. Recovery metrics include symptom scales, function, chronic disease control, and patient preference — not only prescription counts.[3][5][14]
Special populations
Older adults. IMPACT is the canonical late-life CoCM RCT: depression care managers, structured algorithms, psychiatric supervision, better depression and functional outcomes than usual care.[1]
Multimorbidity. TEAMcare and Coventry-type programmes show collaborative models can address depression alongside diabetes and cardiovascular disease targets.[3][12]
Rural / telehealth. Telemedicine-based collaborative care extends psychiatric expertise and evidence-based psychotherapy engagement for populations distant from specialty hubs (e.g. PTSD in rural veterans).[10]
Cultural safety. CoCM implementation in ANZ and globally must embed interpreter access, Indigenous governance partnerships, and non-stigmatising primary care pathways — measurement tools need language-validated versions where used; principles transfer from dissemination literature even when local RCT packages differ.[14]
Evidence and guidelines
| Landmark | Design / message |
|---|---|
| Katon 1995 collaborative management | Early RCT: multifaceted collaborative intervention improved depression care vs usual primary care |
| IMPACT 2002 | Late-life depression CoCM RCT — foundational |
| Gilbody 2006 cumulative MA | Sufficient evidence of benefit by ~2000; longer-term gains |
| Bower 2006 meta-regression | Unpacks components of a complex intervention |
| Archer Cochrane 2012 | Depression and anxiety outcomes improved vs usual care |
| Thota Community Guide 2012 | Strong recommendation for depressive disorders |
| TEAMcare 2010 | Multicondition depression + chronic disease |
| CADET 2013 | UK cluster RCT effectiveness and patient preference |
| Coventry 2015 | Multimorbidity collaborative care |
| Fortney 2015 | Telemedicine CoCM for PTSD |
Regional frames. Collaborative care evidence is global; local implementation language differs by board and health system.[2][14]
ANZ (RANZCP-facing). Position collaborative care as high-value primary care mental health architecture: GPs, practice nurses/allied health care managers, and psychiatrist consultancy; align with stepped models and local primary health network programmes. Mood disorder guidelines emphasise measurement, adequate trials, and timely specialist input for complexity — CoCM operationalises that in primary care.[14]
UK (NICE / MRCPsych). Stepped care is core language; CADET supports collaborative care effectiveness in NHS primary care. Essays should link CoCM elements to stepped intensity and IAPT/community interfaces without inventing service codes.[5]
US (APA / ABPN). Strong CoCM evidence base (IMPACT lineage, Community Guide); psychiatric consultant role and billing/implementation science often appear in systems questions. TEAMcare is the multimorbidity classic.[1][3][11]
India / MD-DNB / NEET-SS. Primary care and district mental health programme task-sharing are the local cousins; apply CoCM principles (team, measures, supervision) without claiming identical US trial infrastructure.[14]
Exam pearls
[1] [14]- IMPACT = late-life depression collaborative care RCT (Unützer 2002).[1]
- TEAMcare = depression + diabetes/CAD multicondition collaborative care (Katon 2010).[3]
- CADET = UK collaborative care depression cluster RCT (Richards 2013).[5]
- Co-location without registry and treatment-to-target is not CoCM.[14]
- PHQ-9 cut-point 10 is a common screen threshold; always action item 9.[8]
- Caseload review is how one psychiatrist multiplies impact across hundreds of primary care patients.[1]
- Cochrane supports depression and anxiety benefit — cite honestly as organisational evidence, not a new molecule.[2]
- Never invent jurisdiction-specific MBS/CPT item numbers unless the stem supplies them.[14]
Related topics
Measurement-based care and rating scales; major depressive disorder; generalised anxiety; suicide risk assessment; epidemiology and public mental health; dual diagnosis integrated care; stigma and rights-based care; consultation-liaison models — cross-link after mastering CoCM principles and landmark trials above.[1][14]
References
- [1]Unützer J, Katon W, Callahan CM, et al. Collaborative care management of late-life depression in the primary care setting: a randomized controlled trial JAMA, 2002.PMID 12472325
- [2]Archer J, Bower P, Gilbody S, et al. Collaborative care for depression and anxiety problems Cochrane Database Syst Rev, 2012.PMID 23076925
- [3]Katon WJ, Lin EH, Von Korff M, et al. Collaborative care for patients with depression and chronic illnesses N Engl J Med, 2010.PMID 21190455
- [4]Gilbody S, Bower P, Fletcher J, et al. Collaborative care for depression: a cumulative meta-analysis and review of longer-term outcomes Arch Intern Med, 2006.PMID 17130383
- [5]Richards DA, Hill JJ, Gask L, et al. Clinical effectiveness of collaborative care for depression in UK primary care (CADET): cluster randomised controlled trial BMJ, 2013.PMID 23959152
- [6]Bower P, Gilbody S, Richards D, et al. Collaborative care for depression in primary care. Making sense of a complex intervention: systematic review and meta-regression Br J Psychiatry, 2006.PMID 17139031
- [7]Wagner EH, Austin BT, Davis C, et al. Improving chronic illness care: translating evidence into action Health Aff (Millwood), 2001.PMID 11816692
- [8]Kroenke K, Spitzer RL, Williams JB The PHQ-9: validity of a brief depression severity measure J Gen Intern Med, 2001.PMID 11556941
- [9]Spitzer RL, Kroenke K, Williams JB, Löwe B A brief measure for assessing generalized anxiety disorder: the GAD-7 Arch Intern Med, 2006.PMID 16717171
- [10]Fortney JC, Pyne JM, Kimbrell TA, et al. Telemedicine-based collaborative care for posttraumatic stress disorder: a randomized clinical trial JAMA Psychiatry, 2015.PMID 25409287
- [11]Thota AB, Sipe TA, Byard GJ, et al. Collaborative care to improve the management of depressive disorders: a community guide systematic review and meta-analysis Am J Prev Med, 2012.PMID 22516495
- [12]Coventry P, Lovell K, Dickens C, et al. Integrated primary care for patients with mental and physical multimorbidity: cluster randomised controlled trial of collaborative care for patients with depression comorbid with diabetes or cardiovascular disease BMJ, 2015.PMID 25687344
- [13]Katon W, Von Korff M, Lin E, et al. Collaborative management to achieve treatment guidelines. Impact on depression in primary care JAMA, 1995.PMID 7897786
- [14]Katon W, Unützer J, Wells K, Jones L Collaborative depression care: history, evolution and ways to enhance dissemination and sustainability Gen Hosp Psychiatry, 2010.PMID 20851265
- [15]Unützer J, Katon WJ, Fan MY, et al. Long-term cost effects of collaborative care for late-life depression Am J Manag Care, 2008.PMID 18269305
- [16]Katon W, Von Korff M, Lin E, et al. Collaborative management to achieve depression treatment guidelines J Clin Psychiatry, 1997.PMID 9054905