Psych · public-community
Community mental health models of care
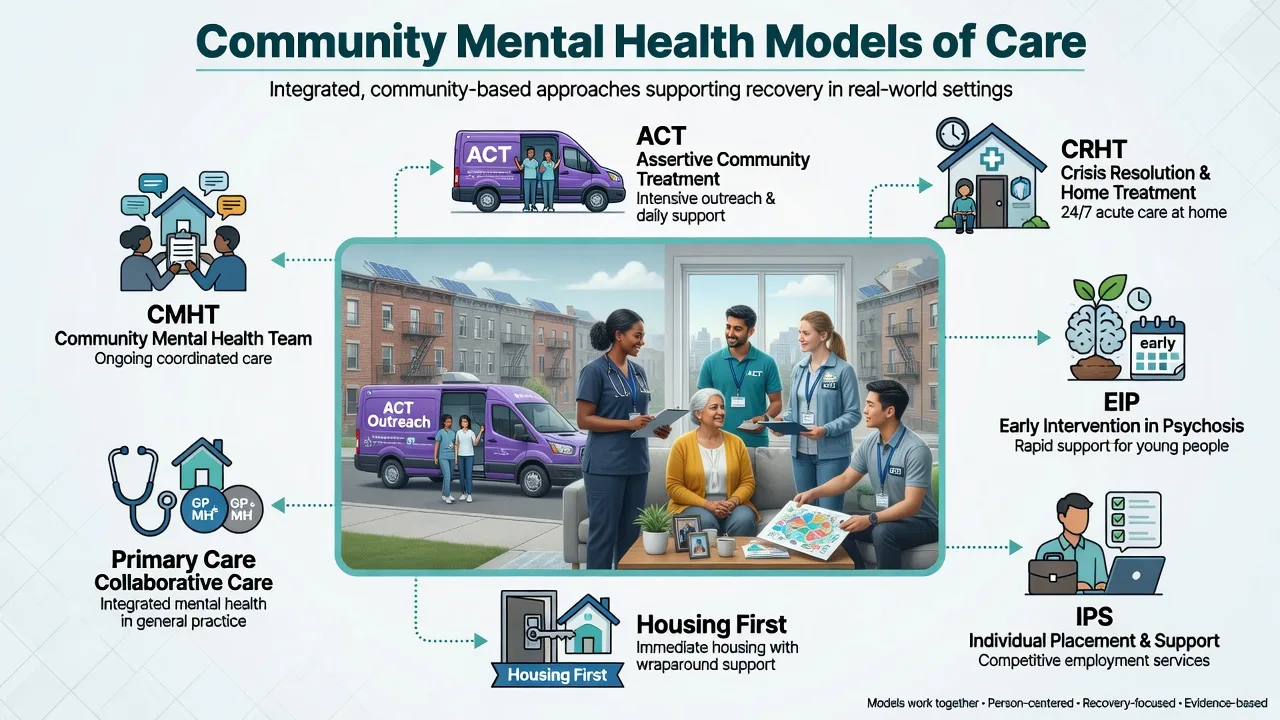
Also known as Assertive community treatment ACT · Community mental health team CMHT · Intensive case management ICM · Crisis resolution home treatment CRHT · Early intervention in psychosis EIP · Flexible ACT FACT · Collaborative care primary care psychiatry · Housing First · Individual placement and support IPS · Deinstitutionalisation balance of care
Exam-exhaustive fellowship topic on community mental health service models: CMHT, case management, ICM, ACT/PACT, FACT, crisis resolution/home treatment, early intervention in psychosis, collaborative care, Housing First, IPS, step-up/step-down disposition, fidelity, and regional architecture. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Definition and classification
From asylum to balanced community care
Deinstitutionalisation shifted long-stay asylum care toward community living, but examiners expect the balance-of-care concept: acute inpatient, secure, and rehabilitation beds remain essential alongside ambulatory and outreach services. Community mental health care means organised, multi-professional support delivered primarily outside hospital, with hospital as one node in a network rather than the default locus of care.[15]
Global reviews stress that community systems must still address the treatment gap, workforce, primary care integration, and rights — not only close beds.[15]
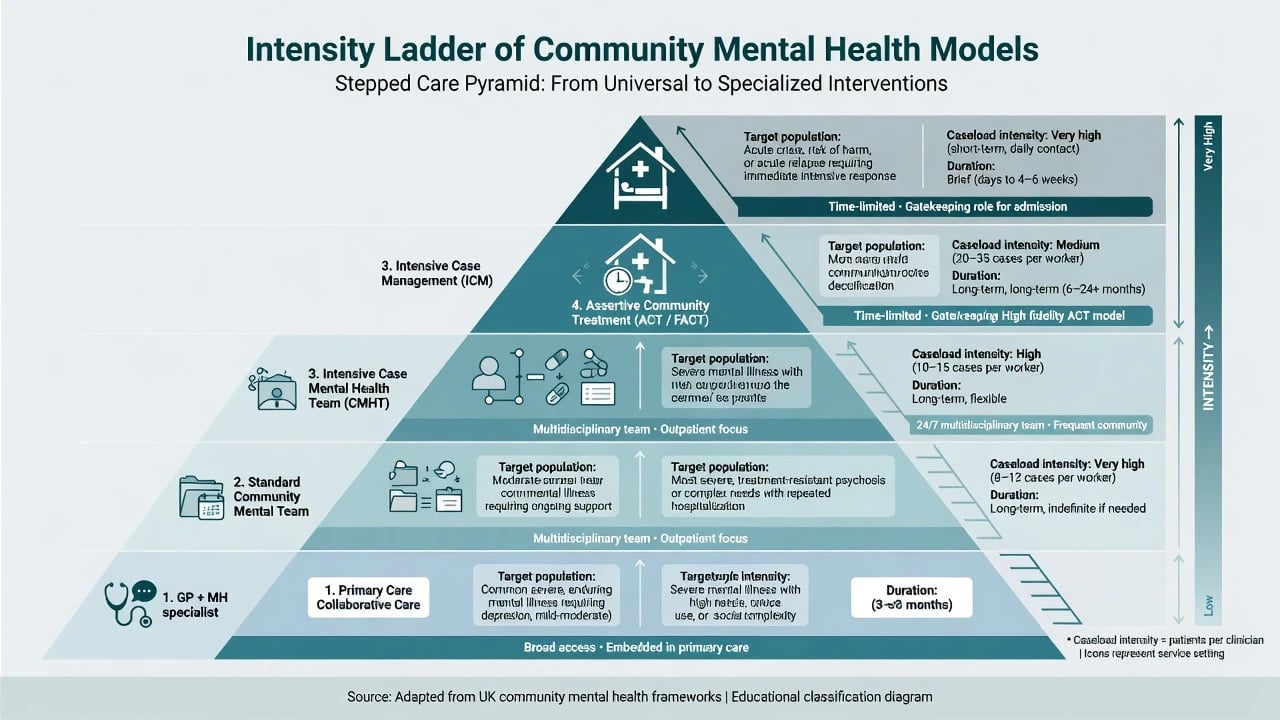
Taxonomy by intensity and purpose
| Model | Typical target | Intensity / structure | Duration |
|---|---|---|---|
| Collaborative care | Depression/anxiety in primary care | Care manager + primary clinician + specialist backup | Episode-based, stepped |
| Standard CMHT | Secondary-care SMI and complex common disorders | MDT, clinic + home visits, individual care coordination | Ongoing, variable |
| Clinical case management / ICM | Higher-need SMI | Higher contact frequency, lower caseload than standard | Ongoing |
| ACT / PACT | High hospital use, disengaged, homeless, dual diagnosis SMI | Team shared caseload, in vivo, assertive, often 24/7 | Often time-unlimited for high need |
| FACT | Mixed caseloads within one service | Flexible step-up to ACT-level within team | Flexible |
| CRHT / home treatment | Acute crisis alternative to admission | Intensive daily (or more) home visits, short term | Days–weeks |
| EIP / EIS | First-episode psychosis (age bands vary) | Phase-specific, family, vocational, low caseload | Typically 2–3 years |
| Rehab / recovery teams | Complex long-term disability | Skills, housing pathways, slow-stream | Months–years |
| Mobile crisis / CAT | Emergency community assessment | Rapid assessment, de-escalation, disposition | Hours–days |
Case management is a function (brokerage of services vs clinical care delivery). ACT is a team model with specified organisational features, not merely "a nurse who visits". Confusing the two is a classic exam fail.[3]
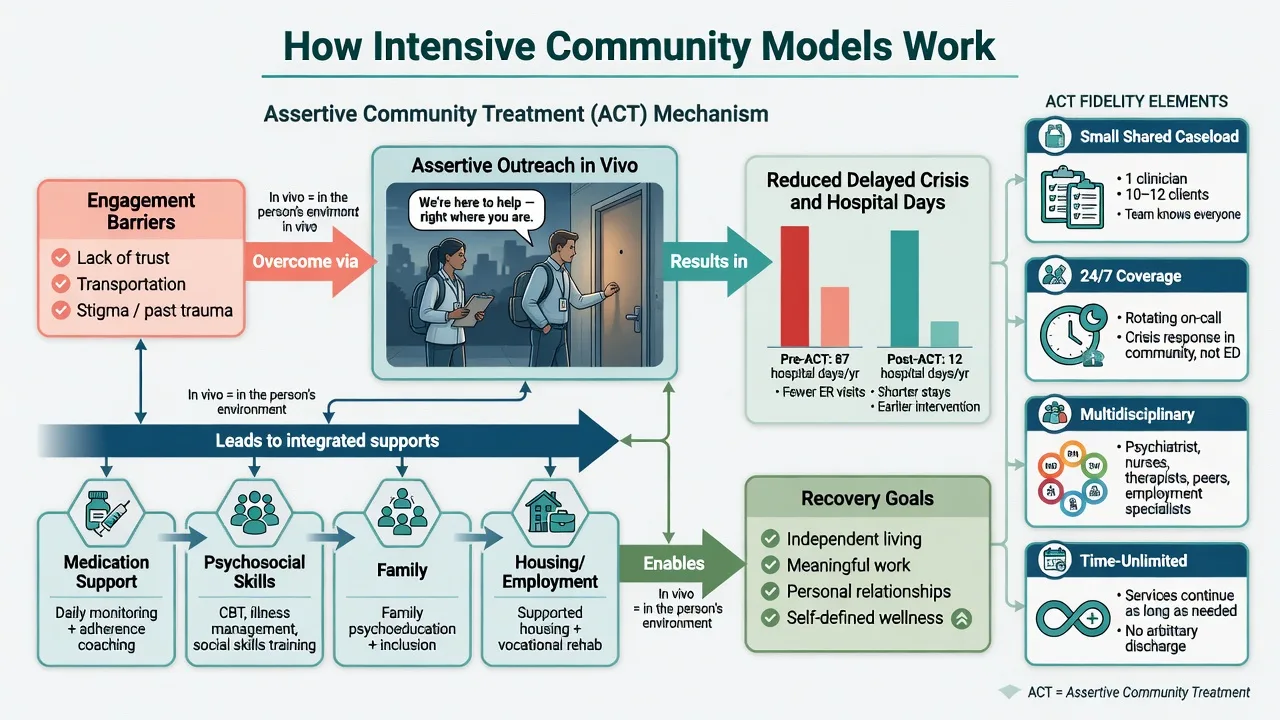
ACT fidelity — conceptual domains
High-fidelity ACT characteristically includes: small caseloads; shared team caseload (not purely individual); most contacts in vivo (home, street, workplace); assertive engagement of hard-to-reach people; multidisciplinary mix (psychiatry, nursing, social work, substance, vocational as available); time-unlimited care for those who need it; and rapid after-hours response in full models. Branding a poorly staffed, office-based service as ACT without these features is ACT-in-name-only.[1][2][3]
Epidemiology and service need
Severe mental illness (especially schizophrenia-spectrum and bipolar) drives high rates of relapse, hospital use, homelessness risk, and physical health inequality. A minority of service users account for a large share of bed-days — the population for whom ICM/ACT was designed.[3][4][5]
Crisis demand clusters around acute relapse, suicidality, family breakdown, substance intoxication, and failed engagement with standard outpatient care — the CRHT niche when home treatment is safe enough.[6][7]
First-episode psychosis incidence is low population-wide but high stakes: delayed treatment (long DUP) and the critical period after onset motivate specialist EIP investment.[8][9][10]
Common mental disorders dominate primary care volume; collaborative care targets the large treatment-gap population that never reaches specialist SMI teams.[11][12]
Mechanisms of benefit (service-level "pathophysiology")
Intensive community models work through engagement, continuity, rapid response, in vivo skill practice, medication support, family work, and social resource mobilisation (housing, benefits, employment) — reducing delayed presentation and revolving-door admissions rather than via a single drug pathway.[1][3][16]
Why fidelity matters: if caseloads rise, contacts become clinic-based, and the team fragments into individual caseworkers without shared responsibility, the mechanism collapses. Cochrane-level synthesises support ACT for service contact and reduced hospitalisation versus standard community care for severe mental disorders.[2]
ICM dose-response with hospital culture: meta-regression shows intensive case management reduces hospital days more where baseline bed use is high; in systems that already use few beds, the marginal reduction is smaller. This is a high-yield viva pearl from Burns and colleagues.[5][4]
Early intervention mechanisms include earlier access, reduced DUP, phase-specific psychosocial interventions, family psychoeducation, and vocational support during the critical period after onset.[9][10]
Collaborative care mechanisms include measurement-based care, proactive follow-up by a care manager, treatment-to-target algorithms, and stepped specialist supervision embedded in primary care — not a one-off psychiatry letter.[11][12]
Clinical presentation and exam stems
Typical stems: revolving-door schizophrenia with multiple admissions yearly; homeless dual-diagnosis patient DNA-ing clinic; first-episode psychosis referral from ED or GP; family requesting admission for mania when home treatment might be feasible; GP depression not improving on antidepressant alone with diabetes comorbidity; long-stay inpatient ready for community rehab; rural area with sparse MDT; post-discharge discontinuity after acute admission.[3][6][8][11][18]
Service cues of under-matched care: rising DNA rates, repeated ED crisis presentations, carer burnout, untreated metabolic disease, hostel eviction, police welfare checks, and notes full of "non-compliant" without assertive engagement plan.[3][15][16]
Differential — model discriminators
| Compare | Discriminator |
|---|---|
| CMHT vs ICM | Contact frequency, caseload size, intensity for complex SMI |
| ICM vs ACT | Shared team caseload, in vivo percentage, after-hours, fidelity package |
| ACT vs FACT | All clients on ACT-level vs flexible step-up within one team |
| CRHT vs inpatient | Safety at home, medical stability, overnight risk, containment needs |
| CRHT vs chronic ACT | Time-limited crisis vs ongoing high-need support |
| EIP vs generic youth CMHT | Phase-specific psychosis package, DUP focus, fixed early-period tenure |
| Collaborative care vs secondary CMHT | Primary care population with care manager vs specialist SMI caseload |
| Housing First vs staircase housing | Immediate housing without sobriety prerequisite vs treatment-first continuum |
| IPS vs prevocational training | Competitive job first, zero exclusion, integrated employment specialist |
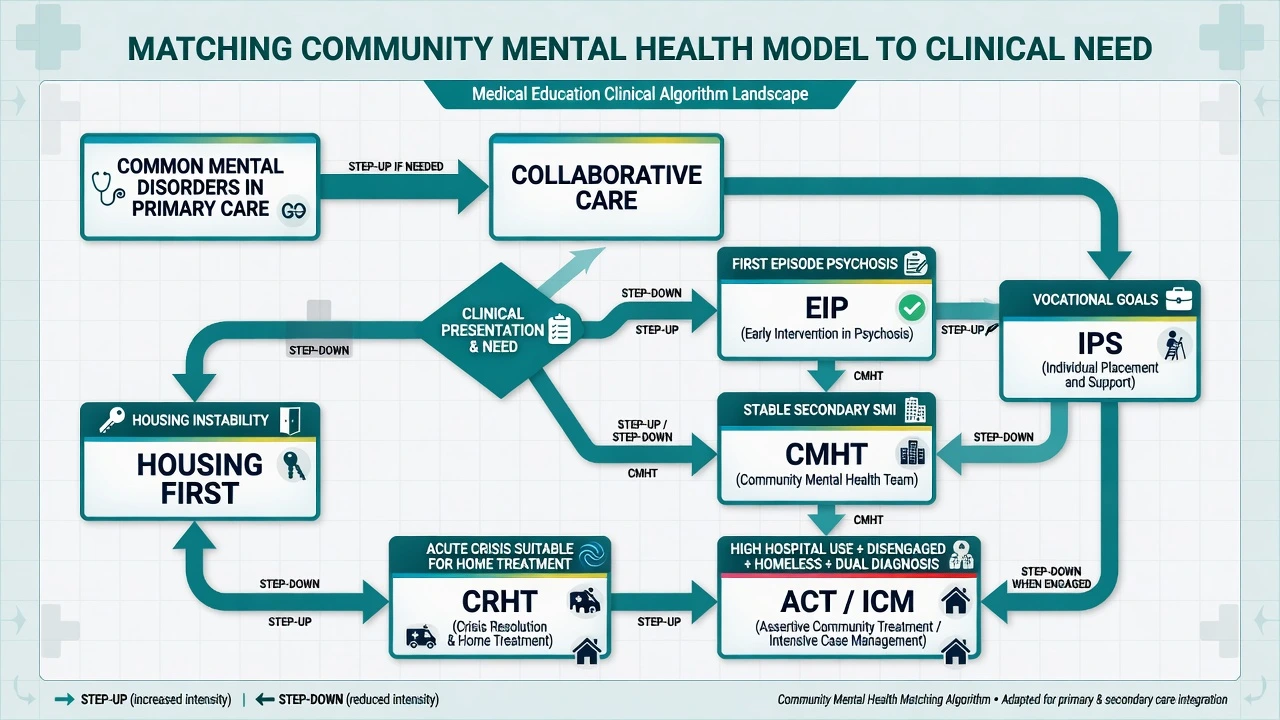
Assessment — matching model to need
Map: diagnosis and severity; suicide/violence/vulnerability risk; engagement history and DNA pattern; hospital days and crisis use; housing and homelessness; dual diagnosis; carer capacity; cultural and language access; geography/rurality; legal status under local mental health law (do not invent sections); physical health multimorbidity; vocational goals.[3][15][16]
CRHT suitability (principles): able to be seen frequently at home; relative medical stability; some engagement or reachable location; overnight risk manageable with plan; substance intoxication not requiring medical detox unit; safeguarding issues addressed; if home is unsafe or containment is required, admit.[6]
Step-down readiness from ACT/ICM: sustained engagement, reduced crisis use, housing stability, workable medication plan, crisis plan known to the person and network, goals shifting toward recovery roles — then transfer to standard CMHT with warm handover.[4][17]
"Investigations" and service metrics
There is no laboratory test for model choice. Investigate with service data: bed-days, 28-day readmissions, time to first face-to-face contact, DNA rates, crisis presentations, employment rates, housing stability, physical health screening completion, and process fidelity (caseload size, contact frequency, multidisciplinary composition).[4][5][15]
Community SMI care still requires metabolic monitoring, side-effect review, and ECG when indicated for specific psychotropics — model choice does not cancel physical health duty (see psychopharmacology topics).[15][16]
Acute / crisis management
Crisis pathway principles: rapid assessment (including medical exclusion), risk formulation, least restrictive safe option, gatekeeping of inpatient beds, intensive home treatment when suitable, or voluntary/involuntary admission under local law when required. CRHT is an acute service, not a moral alternative to all hospitalisation.[6][7]
Mobile crisis / crisis assessment teams provide community assessment, de-escalation, and disposition linkage. Critical time intervention after discharge is an evidence-informed bridge to prevent discontinuity for high-risk transitions.[18]
Definitive management — model by model
Standard CMHT
Multidisciplinary secondary care: assessment, care coordination, medication, psychological therapies access, family work, physical health screening, and liaison with primary care. Suitable for many people with SMI who engage and do not need ultra-high intensity. Risk: caseload inflation and clinic-only drift.[3][15]
Intensive case management and ACT
Stein and Test's foundational program showed that comprehensive community treatment reduced need for hospitalisation versus hospital-based care pathways — the conceptual root of modern ACT.[1] Cochrane synthesis supports ACT for keeping people in contact with services and reducing hospitalisation for severe mental disorders.[2] Intensive case management (broader evidence base including ACT-like packages) reduces hospitalisation and improves outcomes, with larger bed-day reductions where baseline use is high.[4][5]
Implement evidence-based practices within teams: illness management, family psychoeducation, integrated dual-disorder treatment, supported employment, and ACT where indicated.[16]
FACT (flexible ACT)
FACT organises a shared team that delivers standard community care for most clients and scales to ACT-level intensity for a subset, aiming for efficiency without losing step-up capacity. Real-world implementation studies report clinical and social outcome tracking during FACT roll-out; examiners should know the concept even where local branding differs.[17]
Crisis resolution / home treatment
Johnson and colleagues' RCT of a crisis resolution team demonstrated reduced hospital admissions for people in mental health crisis versus standard care pathways.[6] Ecological analyses in England associated CRHT implementation with greater reductions in admission rates, with stronger effects where teams were more fully established — implementation quality matters.[7]
Early intervention in psychosis
EPPIC provided a comprehensive early detection and phase-specific management framework that shaped global EIP design.[9] The LEO randomised trial showed specialised early psychosis care improved clinical and social outcomes versus standard care.[8] McGorry and colleagues summarise early intervention as better access plus systematic delivery of existing treatments and incremental improvements across the critical period.[10]
Collaborative care (primary care)
IMPACT showed collaborative care for late-life depression in primary care was more effective than usual care across diverse primary care settings.[11] Cochrane review supports collaborative care for depression and anxiety outcomes versus usual care.[12] Core ingredients: population identification, measurement-based follow-up, care manager, treatment-to-target, and specialist supervision.
Housing First and IPS
Housing First provides immediate access to permanent housing with support, without requiring sobriety or treatment compliance as a precondition; Tsemberis and colleagues showed participants obtained and maintained independent housing without worsening psychiatric or substance outcomes relative to continuum models in key trials.[13]
Individual Placement and Support (IPS) is the evidence-based supported employment model: competitive jobs first, zero exclusion, rapid job search, integration with mental health care, benefits counselling, and time-unlimited support. Generalisability reviews support IPS effectiveness beyond original US settings.[14]
Subtypes and scenarios
High-yield scenarios: urban high bed-use SMI to ACT/ICM; mixed caseload redesign to FACT; first-episode age-band pathway to EIP; primary care depression with multimorbidity to collaborative care; homeless dual diagnosis to Housing First plus assertive outreach; home crisis with family support to CRHT; complex disability to rehab/recovery teams; forensic step-down to specialised outreach; rural sparse workforce to hub-and-spoke and telepsychiatry interfaces; post-discharge high-risk to critical time intervention.[4][6][8][11][13][17][18]
Complications and pitfalls
Pitfalls include ACT branding without fidelity; CRHT used as a cover for bed closures without skill or staffing; failure to step down stable intensive clients; multi-team fragmentation without a named coordinator; moralising non-engagement; ignoring metabolic and cardiac monitoring; equating community care with zero beds; and inventing legal section numbers when describing community treatment orders or crisis detention.[2][5][7][15]
Prognosis and disposition
Outcomes that improve most consistently with intensive models are service contact and reduced hospital days (context-dependent); symptom effect sizes are more variable; social recovery improves when employment and housing interventions are embedded, not merely discussed.[2][4][5][14]
Disposition algorithm: step up on rising risk, disengagement, or relapse; step down on sustained stability and goal achievement; always provide a written crisis plan and warm handover. Continuity of trusted relationships often matters as much as the brand name of the team.[15][18]
Special populations
Special populations include youth EIP and transition cliffs to adult CMHT; older adults with multimorbidity and home-based care needs; perinatal community and mother-baby interfaces; intellectual disability dual diagnosis pathways; Indigenous and culturally diverse access barriers; rural/remote workforce limits; forensic and prison-discharge transitions; and dual diagnosis integrated within assertive models rather than sequential exclusion.[9][15][16]
Evidence and guidelines (exam anchors)
| Anchor | Take-home |
|---|---|
| Stein and Test (1980) | Foundational comprehensive community program reduced hospitalisation need |
| Mueser et al. (1998) | Taxonomy of community care / case management models |
| Marshall ACT Cochrane | ACT improves contact and reduces hospitalisation for SMI |
| Dieterich ICM Cochrane (2017) | ICM evidence package for severe mental illness |
| Burns et al. (2007) | ICM reduces bed-days most when baseline hospital use is high |
| Johnson CRT RCT (2005) | Crisis resolution teams can reduce admissions |
| Glover et al. (2006) | CRHT implementation associated with admission rate falls |
| Craig LEO (2004); McGorry EPPIC (1996, 2008) | Specialised early psychosis care works |
| Unützer IMPACT (2002); Archer Cochrane (2012) | Collaborative care for depression/anxiety |
| Tsemberis Housing First (2004); Bond/Drake IPS | Housing and employment evidence-based models |
| Thornicroft et al. (2016) | Global community care principles and development agenda |
| Mueser EBPs (2003); Nugter FACT; Dixon CTI | Implementation, flexible ACT, transition continuity |
ANZ: public mental health services are organised around community teams, acute inpatient units, and increasingly specialised early psychosis and assertive outreach functions; legal frameworks for compulsory community treatment are state/territory- or NZ-specific — principles only in a general exam answer. UK: national history of CMHTs, CRHT roll-out, and EIP programmes is heavily examined; NICE psychosis guidance emphasises community-based psychosocial care and rehabilitation access at principle level. USA: ACT/PACT with fidelity monitoring and Medicaid funding structures; collaborative care and Housing First have strong US trial roots. MD-DNB / global: resource-limited settings may prioritise primary care integration, task-sharing, and balanced care rather than full ACT fidelity packages — state principles of stepped intensity and continuity.[6][8][11][15]
Exam pearls
ACT fidelity cues — SHARED
Exam pearls: name the intensity ladder in any service-planning stem; ACT is a team package, not a single visiting worker; ICM hospital-day benefit is largest where baseline bed use is high; CRHT is time-limited crisis care; EIP = early access + phase-specific package (name LEO/EPPIC); Housing First does not require sobriety first; IPS is competitive employment first with team integration; fidelity beats branding; step-down frees scarce intensive capacity; balanced care still needs beds; do not invent MHA section numbers.[4][5][6][8][13][14][15]
Worked micro-formulation (exam style)
Person: 34-year-old with schizophrenia, four admissions in 18 months, hostel eviction risk, methamphetamine use, DNA rate high, metabolic syndrome, parents exhausted. Need map: high hospital use + disengagement + dual diagnosis + housing instability. Model match: high-fidelity ACT or ICM-level assertive outreach with integrated dual-diagnosis approach; Housing First pathway rather than "housing after compliance"; IPS if vocational goals emerge; physical health monitoring within team; family psychoeducation. Crisis plan: CRHT for future home-manageable relapse; low threshold for admission if overnight risk or medical instability. Step-down criteria: 12 months reduced crisis use, housing stable, engagement sustained — then standard CMHT with warm handover. Avoid: labelling only "non-compliant"; ACT branding without home visits; sequential exclusion from housing until "clean".[1][4][13][16]
References
- [1]Stein LI, Test MA Alternative to mental hospital treatment. I. Conceptual model, treatment program, and clinical evaluation Arch Gen Psychiatry, 1980.PMID 7362425
- [2]Marshall M, Lockwood A Assertive community treatment for people with severe mental disorders Cochrane Database Syst Rev, 2000.PMID 10796415
- [3]Mueser KT, Bond GR, Drake RE, Resnick SG Models of community care for severe mental illness: a review of research on case management Schizophr Bull, 1998.PMID 9502546
- [4]Dieterich M, Irving CB, Bergman H, et al. Intensive case management for severe mental illness Cochrane Database Syst Rev, 2017.PMID 28067944
- [5]Burns T, Catty J, Dash M, et al. Use of intensive case management to reduce time in hospital in people with severe mental illness: systematic review and meta-regression BMJ, 2007.PMID 17631513
- [6]Johnson S, Nolan F, Pilling S, et al. Randomised controlled trial of acute mental health care by a crisis resolution team: the north Islington crisis study BMJ, 2005.PMID 16103032
- [7]Glover G, Arts G, Babu KS Crisis resolution/home treatment teams and psychiatric admission rates in England Br J Psychiatry, 2006.PMID 17077435
- [8]Craig TK, Garety P, Power P, et al. The Lambeth Early Onset (LEO) Team: randomised controlled trial of the effectiveness of specialised care for early psychosis BMJ, 2004.PMID 15485934
- [9]McGorry PD, Edwards J, Mihalopoulos C, et al. EPPIC: an evolving system of early detection and optimal management Schizophr Bull, 1996.PMID 8782288
- [10]McGorry PD, Killackey E, Yung A Early intervention in psychosis: concepts, evidence and future directions World Psychiatry, 2008.PMID 18836582
- [11]Unützer J, Katon W, Callahan CM, et al. Collaborative care management of late-life depression in the primary care setting: a randomized controlled trial JAMA, 2002.PMID 12472325
- [12]Archer J, Bower P, Gilbody S, et al. Collaborative care for depression and anxiety problems Cochrane Database Syst Rev, 2012.PMID 23076925
- [13]Tsemberis S, Gulcur L, Nakae M Housing First, consumer choice, and harm reduction for homeless individuals with a dual diagnosis Am J Public Health, 2004.PMID 15054020
- [14]Bond GR, Drake RE, Becker DR Generalizability of the Individual Placement and Support (IPS) model of supported employment outside the US World Psychiatry, 2012.PMID 22295007
- [15]Thornicroft G, Deb T, Henderson C Community mental health care worldwide: current status and further developments World Psychiatry, 2016.PMID 27717265
- [16]Mueser KT, Torrey WC, Lynde D, et al. Implementing evidence-based practices for people with severe mental illness Psychiatr Serv, 2003.PMID 12841590
- [17]Nugter MA, Engelsbel F, Bähler M, et al. Outcomes of FLEXIBLE Assertive Community Treatment (FACT) implementation: a prospective real life study Community Ment Health J, 2016.PMID 25648552
- [18]Dixon L, Goldberg R, Iannone V, et al. Use of a critical time intervention to promote continuity of care after psychiatric inpatient hospitalization Psychiatr Serv, 2009.PMID 19339319