Psych · Public and community psychiatry — disaster and mass casualty psychiatry
Disaster and mass casualty psychiatry
Also known as Disaster mental health · Mass casualty behavioural health · Psychological first aid PFA · Critical incident stress debriefing CISD · MHPSS emergency psychiatry · Bushfire flood terrorism mental health · Hobfoll five essential elements · Disaster psychiatry surge
Exam-exhaustive fellowship reference on disaster and mass casualty psychiatry — exposure gradients, normal distress versus disorder, Hobfoll five elements, Psychological First Aid versus mandatory debriefing, stepped triage and treatment of ASD/PTSD/depression/grief, first-responder and child care, and regional MHPSS architecture. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
This topic is high-yield for FRANZCP MEQs on service planning and trauma, MRCPsych public-health and CASC crisis stems, and ABPN disaster/systems blueprints. Examiners test whether candidates can name epidemiology anchors, distinguish normal distress from disorder, reject universal debriefing, and operationalise stepped care under resource pressure.[5][8][12]
Overview and definition
Disaster psychiatry addresses the mental health consequences of events that overwhelm local capacity — natural hazards, technological failures, intentional mass violence, and large-scale epidemics — and the systems needed to prepare, respond, and recover.[5][18] Mass casualty incident (MCI) behavioural health work sits inside emergency medical systems: life-saving triage first, then psychological stabilisation, case finding, and stepped specialist care.
Clinical framing. Think in four phases — preparedness, impact/response, early recovery, and long-term reconstruction — and match psychiatric tasks to each: stockpile plans and training before impact; PFA, crisis assessment, and medication continuity during response; skills-based care and grief support in recovery; specialist trauma treatment and community reconstruction later.[8][18]
Nosology. Use DSM-5-TR acute stress disorder and PTSD (four symptom clusters), ICD-11 PTSD / complex PTSD when structure fits, plus major depression, prolonged grief, adjustment, substance-related disorders, and exacerbation of pre-existing serious mental illness (SMI). Disaster exposure is a context, not a diagnosis.[4][5]
Classification
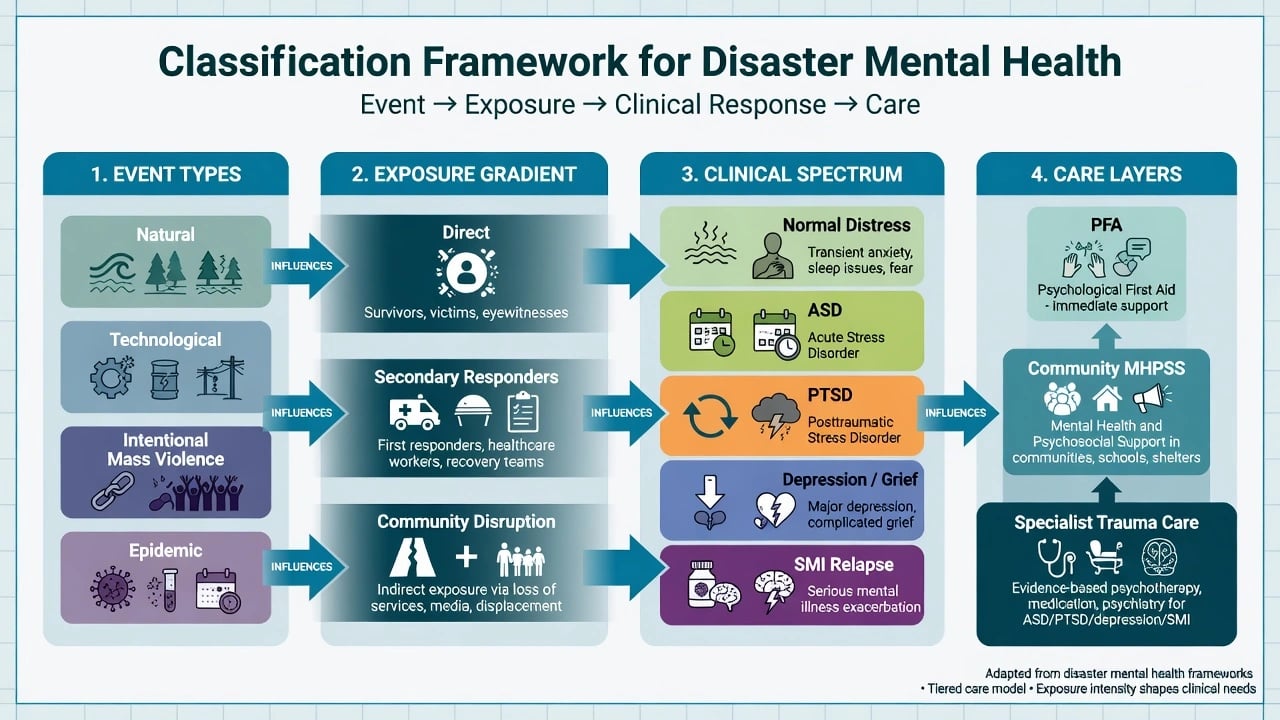
Event types
- Natural hazard (fire, flood, quake)
- Technological / industrial
- Intentional mass violence
- Epidemic / pandemic surge
Exposure gradient
- Direct threat, injury, bereavement
- Secondary: responders, family
- Community disruption / media
- Dose-response with severity
Clinical spectrum
- Normal adaptive distress
- ASD then PTSD if persistent
- Depression, grief, substance surge
- SMI relapse / script loss
Care layers
- PFA / practical supports
- Community MHPSS
- Primary care stepped care
- Specialist TF-CBT / EMDR / meds
Epidemiology and risk factors
Headline epidemiology candidates must own
Landmark anchors. Norris and colleagues synthesised decades of disaster mental health research across tens of thousands of victims, emphasising that outcomes and risk factors vary by disaster type, sample, and severity — never quote one false-precision percentage as "the" disaster PTSD rate.[1][2]
Neria, Nandi and Galea systematically reviewed PTSD following disasters and highlighted higher rates among the most severely exposed, consistent with a dose-response concept examiners expect by name.[4]
Galea and colleagues documented elevated PTSD and depression among Manhattan residents weeks after the September 11 attacks, with concentration near the epicentre — a classic intentional-mass-violence epidemiology stem.[3]
Goldmann and Galea summarised presentation, burden, correlates, and treatment of mental disorders after disasters for public-health audiences.[5] Beaglehole and colleagues meta-analysed natural disasters and found increased psychological distress and psychiatric disorder with substantial between-study heterogeneity.[7]
Resilience and trajectories. Bonanno and colleagues argued that published reports often overestimate uniform catastrophe; many survivors show resilience or recovery trajectories, while chronic and delayed paths still demand services for the minority who need them.[6]
ANZ high-yield. Longitudinal work after the Victorian Black Saturday bushfires shows that several years later the majority are without clinical-level distress, yet high-impact communities retain elevated PTSD, depression, and severe distress — resilience and residual need coexist.[16]
Risk factors. Meta-analytic work on PTSD risk after trauma identifies factors such as prior trauma, prior psychopathology, trauma severity, and low social support among stronger and more consistent predictors; demographic effects (including sex) can vary by sample.[15] Secondary stressors — displacement, job loss, insurance battles, ongoing media — maintain mid-term morbidity beyond the index event.[5][6]
Suicide. Systematic review of natural disasters and suicidal behaviour shows complex, time-varying associations rather than a single predictable immediate mass suicide surge; still assess suicide risk routinely in clinical contacts.[17]
Pathophysiology and mechanisms
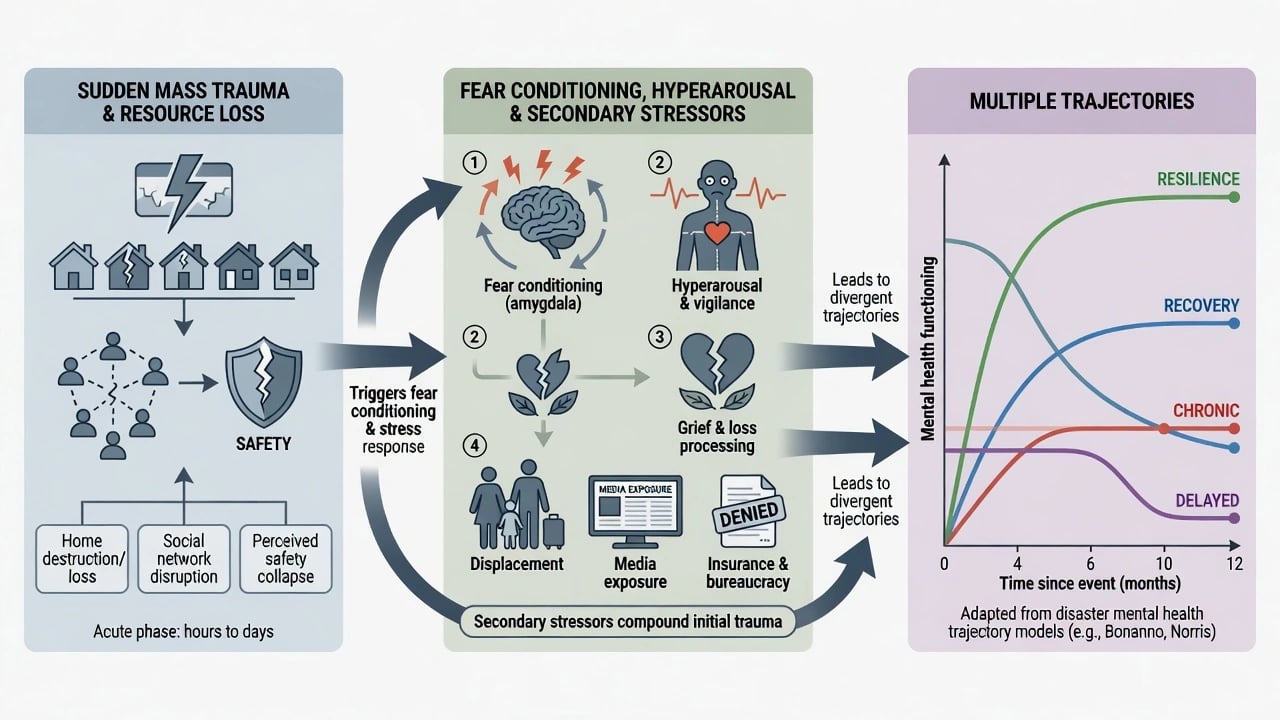
Fear conditioning and safety learning. Sudden uncontrollable threat seeds conditioned fear, hyperarousal, and disrupted sleep; ongoing threat cues (sirens, smoke smell, news loops) maintain activation.[5][18]
Conservation of resources. Hobfoll-aligned models emphasise loss of home, social networks, work, and agency; resource-loss spirals predict worse outcomes and justify practical assistance as clinical intervention, not optional social work add-on.[9]
Collective trauma and grief. Mass bereavement, survivor guilt, and moral injury (especially among responders and clinicians) overlap with PTSD and depression; community rituals and accurate information support adaptive grief.[6][8]
Clinical presentation
Classic adult vignette: adult evacuated from a bushfire or flood zone, presenting with insomnia, startle, intrusive images of flames or water, irritability, alcohol use to sleep, and worry about missing relatives — or a first responder after body recovery with numbing and delayed tearfulness.[16][18]
MSE focus. Affect may be tearful, restricted, or irritable; thought content includes threat expectancy, guilt, and foreshortened future; perception may include trauma-linked flashbacks that must be distinguished from primary psychotic hallucinations; cognition shows concentration failure; risk assessment is mandatory.[5]
Community signals. Sleep complaints, somatic presentations to primary care, interpersonal conflict, school refusal in children, and delayed help-seeking until secondary stressors accumulate.[1][5]
Differential diagnosis
| Discriminator | Favours trauma-related disorder | Favours alternative |
|---|---|---|
| Intrusions linked to disaster cues, avoidance, hyperarousal lasting beyond acute window | ASD / PTSD | Transient adaptive distress resolving with safety |
| Preoccupation with deceased, yearning, identity disruption | Prolonged grief pathway | PTSD without grief structure |
| Cognitive change after blast/collapse head injury | TBI work-up | "All psychological" assumption |
| Tremor, autonomic surge with last drink days ago | Withdrawal | Pure trauma hyperarousal |
| Pre-existing psychosis; meds lost in evacuation | SMI relapse + continuity failure | New-onset primary psychosis only |
Also consider medical mimics, substance-induced states, and compensation-context assessment without default disbelief.[8]
Clinical and bedside assessment
Triage first. Medical stability, safety of the environment, acute suicidality/violence, dependent children, and shelter for tonight precede a full trauma narrative.[8][18]
Exposure map. Where were you; what did you see/do; injuries; deaths of loved ones; missing persons; property loss; role (survivor vs responder). Link exposure severity to expected risk without pathologising everyone.[1][4]
Risk. Suicide, self-harm, IPV escalation in crowded shelters, child protection, and vulnerable older adults left alone. Collaborative safety planning with means restriction and clear follow-up.[17]
Measures. PCL-5 and PHQ-9 can monitor severity when language and setting allow; interpret cut-offs cautiously in acute field conditions. Prefer brief functional questions over lengthy batteries during surge.[8]
Language and culture. Professional interpreters; never children. Trauma-informed pacing: enough history to plan care without forced graphic retelling for forms.[11]
Investigations
No disaster-specific diagnostic biomarker. Investigate medical injury, infection, metabolic derangement, pregnancy, and substance contribution as indicated; ECG and basic labs before starting or restarting psychotropics when cardiac or metabolic risk is present. For planners, track surge volume, equity of access, and referral completion — service metrics are part of the "work-up" of a disaster system.[5][8]
Management — acute / resuscitation
Command integration. Psychiatry works within incident command / emergency medical systems. Do not enter active hazard zones outside safety protocols. Support medical triage, family notification processes, and staff welfare.[8][18]
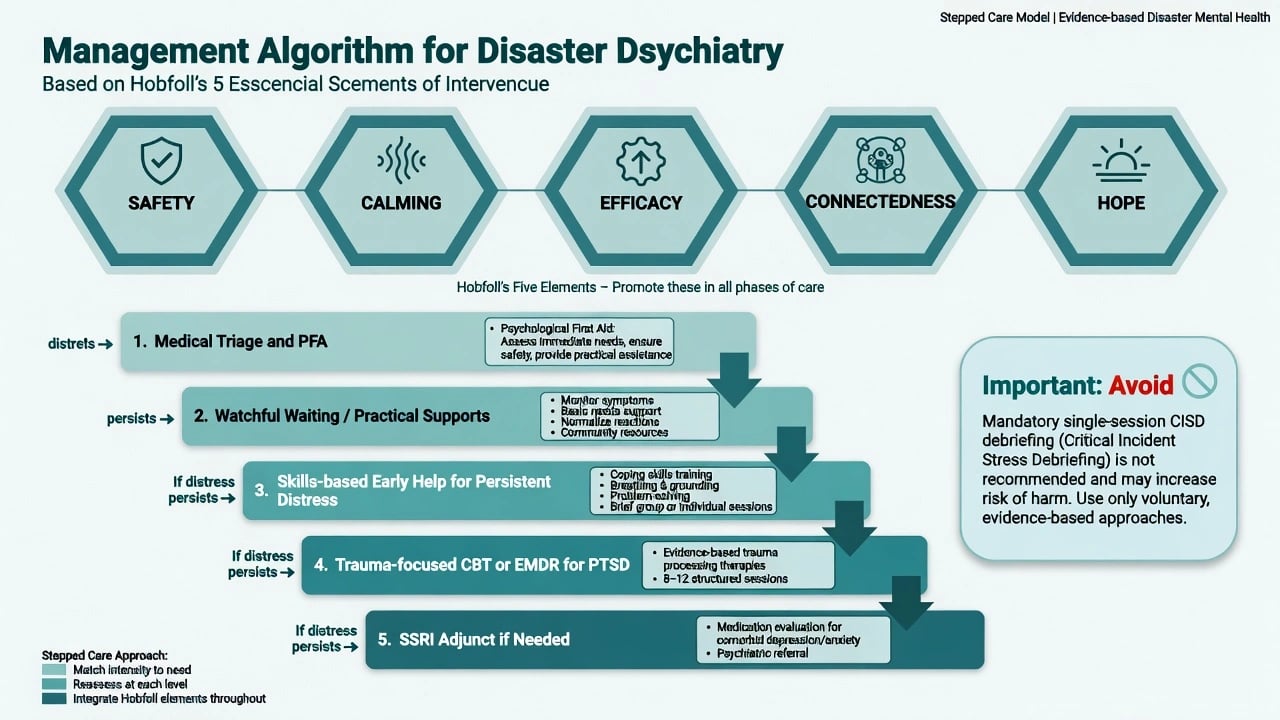
Hobfoll five essential elements. Promote: (1) a sense of safety, (2) calming, (3) self- and community efficacy, (4) connectedness, and (5) hope — the empirical principles that should guide immediate and mid-term mass trauma intervention.[9]
Psychological First Aid. PFA operationalises early support: contact and engagement, safety and comfort, stabilisation, information gathering, practical assistance, connection with social supports, information on coping, and linkage with collaborative services. Implementation frameworks exist for high-risk organisations; evidence quality for outcomes is still developing — expert consensus and guideline adoption outpaced trial depth, a point Shultz and Forbes emphasise.[11][12]
Medication continuity. Replace lost scripts for antipsychotics, mood stabilisers, and antidepressants early. Avoid chaotic polypharmacy and default long-term benzodiazepines for "nerves."[8][14]
Management — definitive and stepwise
Stepped care ladder
- Medical triage + PFA + practical needs (shelter, food, information, reunification).[9][11]
- Watchful waiting with monitoring for most recovering people.[6][10]
- Skills-based early help (coping, sleep, problem-solving) if distress persists.[8]
- Trauma-focused CBT or EMDR for chronic PTSD — Cochrane evidence supports individual trauma-focused psychological therapies over waitlist/usual care for clinician-rated PTSD symptoms.[13]
- SSRI adjunct when preferred, therapy access limited, or comorbid depression/anxiety prominent.
Pharmacotherapy — agent, dose, monitoring
Medication does not replace trauma-focused psychological treatment when that treatment is available and acceptable. Sertraline has RCT support for PTSD symptoms in general adult populations and is a common adjunct after disasters when medication is indicated.[14]
| Agent | Typical adult start | Common range | Monitoring notes |
|---|---|---|---|
| Sertraline | 25–50 mg orally daily | 50–200 mg daily | GI effects, sexual dysfunction; early review for activation/suicidality; check interactions and pregnancy status |
| Other SSRI/SNRI | Per PTSD/depression protocols | Individualise | Same cautions; restore pre-disaster effective regimens when known |
Avoid reflexive long-term benzodiazepines for core trauma symptoms (dependence; interference with extinction learning). Titrate carefully amid substance-use risk and disrupted sleep architecture.[13][14]
System-level care
Outreach to shelters, schools, workplaces, and primary care; culturally adapted public messaging; restore routines; protect staff with rotation, peer support, and supervision. North and Pfefferbaum outline a systematic framework for case identification, triage, and integration of mental health into emergency medical response.[8]
ANZ: Black Saturday and subsequent bushfire mental-health programmes are high-yield; name Bryant longitudinal anchors; align with local disaster recovery frameworks and telepsychiatry for rural/remote. UK/Europe: NICE PTSD principles (trauma-focused therapies; caution regarding routine debriefing) plus multi-agency resilience planning. US/Canada: APA disaster psychiatry principles, SAMHSA/crisis counselling models, hospital incident command interfaces. Global: WHO/IASC mental health and psychosocial support (MHPSS) pyramid — basic services and security first, then community and family supports, focused non-specialised supports, and specialised services at the tip.[8][13][16]
Subtypes and clinical scenarios
- Bushfire / wildfire communities: long tail of secondary stressors; ANZ evidence base.[16]
- Flood / cyclone displacement: housing loss as primary clinical lever.[7]
- Intentional mass violence / terrorism: high media exposure; epicentre dose-response (Galea-type stems).[3]
- Hospital internal MCI: staff moral injury and dual-role strain.[18]
- Epidemic/pandemic surge: isolation, grief, health-worker burnout layered on trauma models.[5]
- First responders: delayed presentation, occupational culture barriers, cumulative exposure.[8]
- Children/schools: developmental presentations; caregiver mental health drives child outcomes.[6]
Complications and pitfalls
Mandatory CISD for all exposed; pathologising normal grief or ignoring true disorder in high-exposure groups; therapy-only plans that ignore housing and information needs; child interpreters; lost SMI medication continuity; long-term benzodiazepine defaults; freelancing outside command safety; inventing emergency statute numbers; equity failures for Indigenous, disability, rural, and undocumented populations.[6][10][12]
Prognosis and disposition
Expect heterogeneous trajectories: resilience, recovery, chronic impairment, and delayed onset.[6] Higher chronic risk with severe exposure, bereavement, ongoing displacement, prior illness, and low support.[4][15] Long-term follow-up for high-impact communities remains justified years later.[16]
Step-up for high suicide risk, psychosis, severe self-neglect, unsafe shelter, or failed community engagement. Step-down when risk is managed, function improves, and practical supports stabilise. Disposition maps field/shelter → primary care → specialist trauma/crisis → inpatient when needed.[8]
Special populations
Children and adolescents; older adults with medical comorbidity and isolation; perinatal patients needing care continuity; people with SMI and intellectual disability requiring supported decision-making and script replacement; first responders and health workers; Indigenous and culturally diverse communities; rural/remote populations (telepsychiatry interface); refugees co-exposed to disaster on top of prior trauma.[5][6][16]
Evidence and guidelines
Anchor answers to named papers: Norris 2002 I–II; Galea 2002; Neria 2008; Goldmann/Galea 2014; Beaglehole 2018; Bonanno 2010; Hobfoll 2007; Rose Cochrane debriefing; Forbes PFA framework; Shultz/Forbes evidence critique; North/Pfefferbaum JAMA 2013; Bisson Cochrane TF therapies; Brady sertraline; Brewin risk factors; Bryant Black Saturday; Kõlves suicide review; Norwood/Ursano principles. Cite RANZCP, NICE, APA, and WHO/IASC principles — not invented page numbers.[1][9][10][13][16]
Exam pearls
SCECH + STEP disaster care
References
- [1]Norris FH, Friedman MJ, Watson PJ, et al. 60,000 disaster victims speak: Part I. An empirical review of the empirical literature, 1981-2001 Psychiatry, 2002.PMID 12405079
- [2]Norris FH, Friedman MJ, Watson PJ 60,000 disaster victims speak: Part II. Summary and implications of the disaster mental health research Psychiatry, 2002.PMID 12405080
- [3]Galea S, Ahern J, Resnick H, et al. Psychological sequelae of the September 11 terrorist attacks in New York City N Engl J Med, 2002.PMID 11919308
- [4]Neria Y, Nandi A, Galea S Post-traumatic stress disorder following disasters: a systematic review Psychol Med, 2008.PMID 17803838
- [5]Goldmann E, Galea S Mental health consequences of disasters Annu Rev Public Health, 2014.PMID 24159920
- [6]Bonanno GA, Brewin CR, Kaniasty K, La Greca AM Weighing the costs of disaster: consequences, risks, and resilience in individuals, families, and communities Psychol Sci Public Interest, 2010.PMID 26168411
- [7]Beaglehole B, Mulder RT, Frampton CM, et al. Psychological distress and psychiatric disorder after natural disasters: systematic review and meta-analysis Br J Psychiatry, 2018.PMID 30301477
- [8]North CS, Pfefferbaum B Mental health response to community disasters: a systematic review JAMA, 2013.PMID 23925621
- [9]Hobfoll SE, Watson P, Bell CC, et al. Five essential elements of immediate and mid-term mass trauma intervention: empirical evidence Psychiatry, 2007.PMID 18181708
- [10]Rose S, Bisson J, Churchill R, Wessely S Psychological debriefing for preventing post traumatic stress disorder (PTSD) Cochrane Database Syst Rev, 2002.PMID 12076399
- [11]Forbes D, Lewis V, Varker T, et al. Psychological first aid following trauma: implementation and evaluation framework for high-risk organizations Psychiatry, 2011.PMID 21916629
- [12]Shultz JM, Forbes D Psychological First Aid: Rapid proliferation and the search for evidence Disaster Health, 2014.PMID 28228996
- [13]Bisson JI, Roberts NP, Andrew M, Cooper R, Lewis C Psychological therapies for chronic post-traumatic stress disorder (PTSD) in adults Cochrane Database Syst Rev, 2013.PMID 24338345
- [14]Brady K, Pearlstein T, Asnis GM, Baker D, et al. Efficacy and safety of sertraline treatment of posttraumatic stress disorder: a randomized controlled trial JAMA, 2000.PMID 10770145
- [15]Brewin CR, Andrews B, Valentine JD Meta-analysis of risk factors for posttraumatic stress disorder in trauma-exposed adults J Consult Clin Psychol, 2000.PMID 11068961
- [16]Bryant RA, Waters E, Gibbs L, et al. Psychological outcomes following the Victorian Black Saturday bushfires Aust N Z J Psychiatry, 2014.PMID 24852323
- [17]Kõlves K, Kõlves KE, De Leo D Natural disasters and suicidal behaviours: a systematic literature review J Affect Disord, 2013.PMID 22917940
- [18]Norwood AE, Ursano RJ, Fullerton CS Disaster psychiatry: principles and practice Psychiatr Q, 2000.PMID 10934746