Psych · public-community
Health economics and mental health service planning
Also known as Mental health economics · Cost-effectiveness psychiatry · ICER QALY mental health · ACE-Mental Health priority setting · Service planning mental health · Budget impact mental health · DALY burden mental disorders · Health technology assessment psychiatry
Exam-exhaustive fellowship topic on health economics for mental health and service planning: burden (DALY/YLD), cost-of-illness, CEA/CUA/CBA, ICER and QALY logic, ACE-MH priority setting, efficiency-equity-feasibility, workforce and financing, budget impact, and regional HTA deltas. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
3 MCQs with explanations
Target exams
Red flags

Definition and classification
What health economics is (and is not)
Health economics studies how societies allocate scarce resources to produce health and related social value. In psychiatry the core maxim is opportunity cost: every bed-day, clinic session, ACT slot, or formulary listing displaces an alternative use of the same money, staff time, or capital.[3][11]
It is not synonymous with cost-cutting, nor with equating high disease cost with automatic priority for every proposed programme. Large cost-of-illness estimates support advocacy and context; economic evaluation compares incremental costs and effects of alternatives.[13][9]
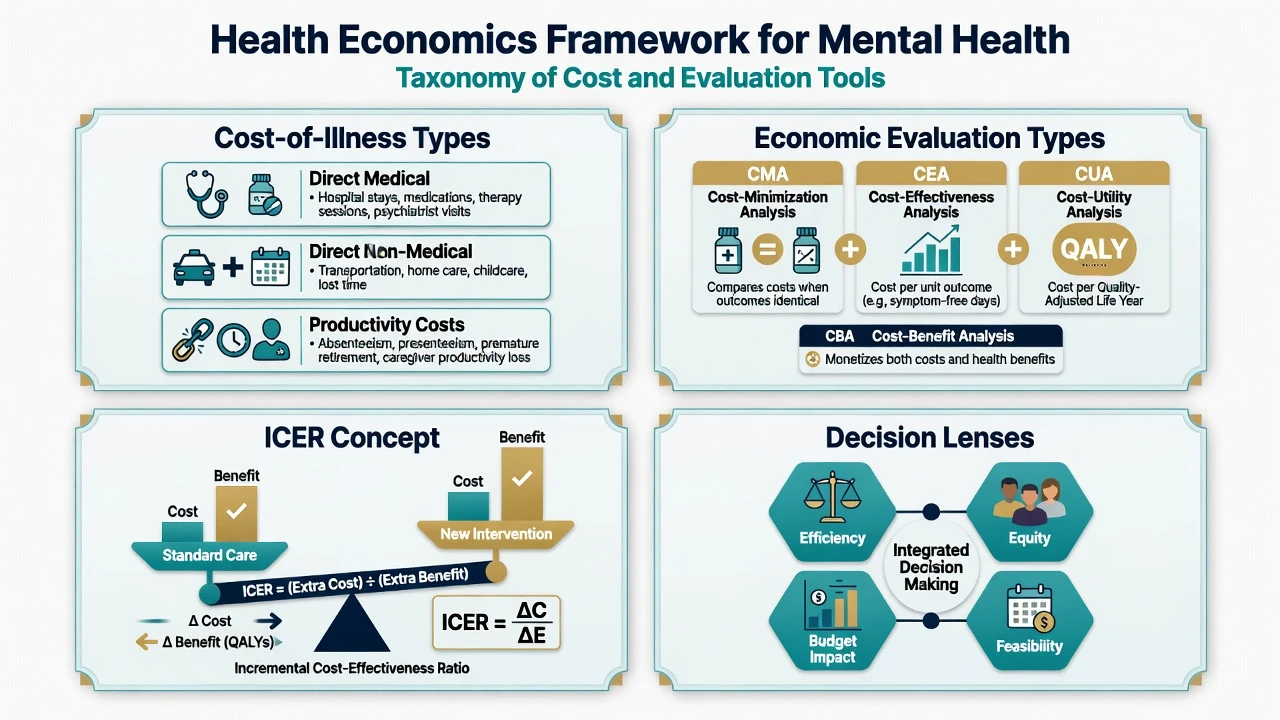
Types of economic analysis
| Type | Outcome | Typical use in MH |
|---|---|---|
| Cost-minimisation (CMA) | Outcomes assumed equal | Compare two equally effective pathways; rare and often unsafe to assume |
| Cost-effectiveness (CEA) | Natural units (e.g. symptom-free days, relapse averted) | Single-condition decisions |
| Cost-utility (CUA) | QALY (or sometimes DALY averted) | Compare across dissimilar programmes |
| Cost-benefit (CBA) | Money-valued benefits | Social investment cases; harder valuation of health |
| Cost-consequence | Multi-outcome dashboard | Transparent trade-offs without single index |
| Budget-impact analysis | Affordability over 1–5 years for a payer | Complements CE when a high-value item is still unaffordable now |
Standard taxonomy for economic evaluation types used in health-technology assessment and mental health priority setting.[9][11]
ICER (incremental cost-effectiveness ratio) = (C_new − C_comparator) / (E_new − E_comparator). Interventions that cost less and work better dominate. Decision-makers may apply a willingness-to-pay threshold as a rule of thumb; thresholds are jurisdiction-specific and change — do not recite another country's historic figure as universal law.[9][11]
Perspectives and cost categories
- Health-system perspective: formal care costs (inpatient, community, medicines, diagnostics).
- Societal perspective: adds productivity losses, informal care, criminal justice, education externalities where relevant.
- Direct medical / direct non-medical / productivity (indirect) costs should be defined explicitly; depression burden studies show productivity and comorbidity costs can dwarf drug spend alone.[13]
Service planning defined
Mental health service planning translates epidemiology and evidence into capacity: how many primary-care collaborative-care slots, CMHT posts, intensive outreach places, crisis beds, and rehabilitation pathways a catchment needs — and which packages deliver best value under equity constraints.[10][14]
Epidemiology and economic burden
Global Burden of Disease analyses show mental and substance use disorders contribute a large share of years lived with disability, especially in working-age adults — a structural reason mental health is both a clinical and economic priority.[1]
No health without mental health links mental disorders to excess physical disease, injury, and social adversity; under-investment is therefore a whole-health-system problem, not a niche specialty budget line.[2]
Cost-of-illness work on major depression documents substantial workplace and societal costs alongside treatment costs, explaining why payers and employers care about effective detection and care pathways.[13]
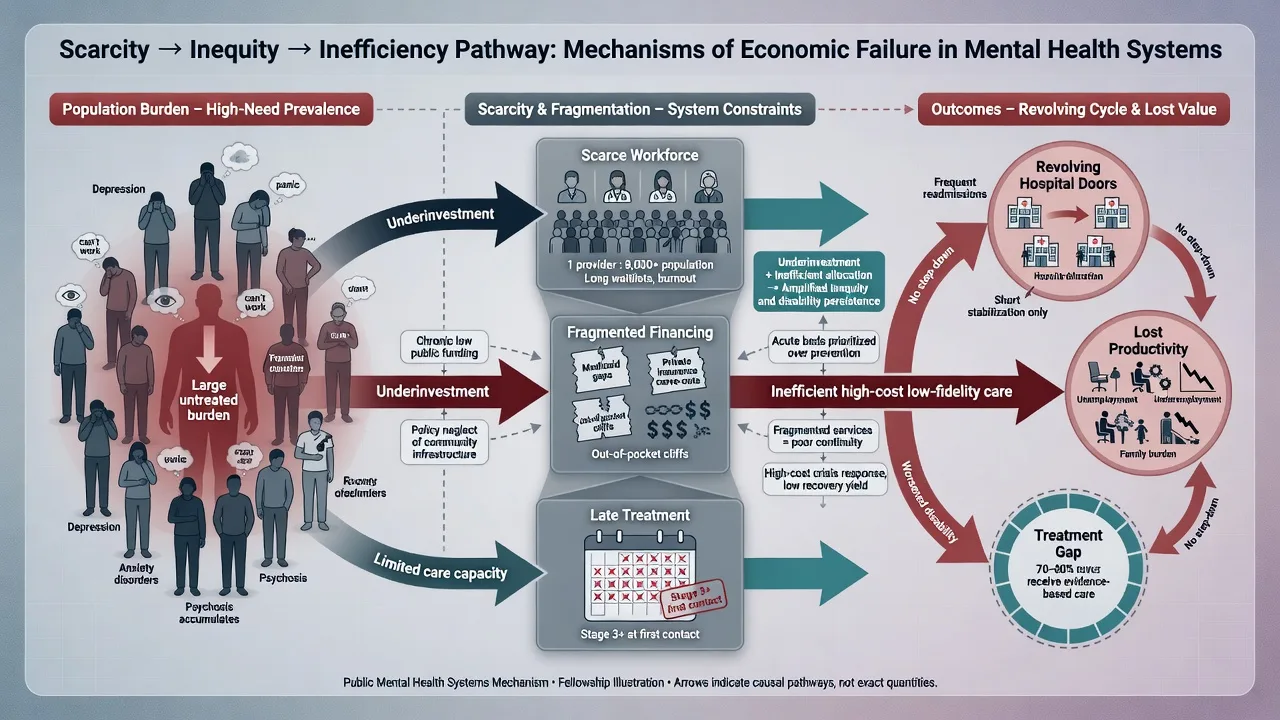
Yet financing and workforce remain mismatched to need. Saxena and colleagues frame the triple problem of scarcity (too few resources), inequity (resources concentrated away from those with greatest need, including LMICs and marginalised groups), and inefficiency (resources spent on low-value or poorly organised care).[3]
Mechanisms of value and waste (system-level "pathophysiology")
Economic harm in mental health systems is produced by mechanisms candidates should name — scarcity meeting avoidable disability and high-cost fragmented care.[3][1]
- Late or no treatment of high-prevalence disorders → long disability tails and productivity loss despite relatively low unit cost of effective care at scale.[5][7]
- Revolving-door high-cost care without assertive engagement, dual-diagnosis capacity, or housing support — high spend, poor outcomes.[14]
- Low-fidelity expensive models (branded ACT/EIP without caseload or skill mix) waste incremental investment.[14]
- Fragmented financing (siloed budgets for hospital, primary care, social care, disability) blocks packages that look cost-effective in models but cannot be purchased as a bundle.[3][4]
- Workforce shortage as a binding constraint: money without trained people does not convert to coverage.[12]
Conversely, optimal evidence-based packages can improve population cost-effectiveness relative to fragmented "current" treatment patterns, as modelled for schizophrenia and for depression across world regions.[7][8]
Clinical and managerial "presentation"
Examiners present economics as service redesign, formulary, or commissioning stems that force explicit trade-offs under scarcity.[3][10]
- Expand intensive community care vs open more acute beds.[14]
- Fund stepped psychological therapy for common mental disorders in primary care.[7]
- Introduce a high-price medicine with modest incremental benefit.[9]
- Scale primary mental health care packages in a low-resource region.[5][4]
- Defend disinvestment from low-value care to free capacity for high-value packages.[10][3]
Clinical signals that are economic signals: high DNA rates, long waits, 100% bed occupancy with corridor care, high readmission, carer collapse, and unemployed recovery-phase patients all imply mismatched intensity, access, or social support — not only "need more money".[14][3]
Differential: tools and decisions candidates confuse
| Confusion | Discriminator |
|---|---|
| Cost-of-illness vs CE evaluation | Magnitude of burden ≠ ICER of a programme |
| CEA vs CUA | Natural units vs QALY/DALY for cross-programme comparison |
| Cost-effective vs affordable | ICER favourable but budget impact may still block this year |
| Technical vs allocative efficiency | Doing a task cheaply vs choosing the right mix of programmes |
| Health-system vs societal perspective | Whether productivity/carer costs are in or out |
| Average vs incremental analysis | Always define the comparator carefully |
These discriminators prevent classic exam errors that confuse burden advocacy with incremental value and affordability.[9][11][13]
Assessment for planning (the "work-up")
Catchment needs assessment
Estimate prevalence and severity (surveys and administrative data), unmet need, current utilisation (contacts, bed-days, crisis presentations), wait times, and equity gaps (rural, Indigenous, CALD, dual diagnosis, forensic interface).[10][14]
Appraising an economic paper (exam checklist)
Fellowship appraisal of mental health economic studies follows the same method discipline as ACE-style priority work: clear question, comparator, perspective, horizon, outcomes, uncertainty, and implementation filters.[9][11]
- Research question and comparator clear?
- Perspective and cost inventory stated?
- Time horizon long enough for mental health disability?
- Outcome measure (QALY instrument? DALY modelling? clinical scale only?)
- Discounting, uncertainty, sensitivity analyses?
- Generalisability to local prices, wages, and care pathways?
- Equity and implementation discussed, or pure league-table fetish?
Investigations and metrics (no lab test)
Useful planning metrics: cost per QALY or DALY averted (modelled), bed occupancy and average length of stay, cost per weighted community contact, 28-day readmission, time-to-first-contact, employment and housing stability rates, workforce FTE per 100,000, and fidelity process measures for intensive models.[10][14][12]
Acute resource decisions
In surge or crisis, protect safe containment capacity. Community ideology that closes beds without alternative intensive home treatment, crisis staffing, and admission pathways is neither ethical nor efficient when high-risk patients bounce through emergency departments.[14]
Opportunity cost cuts both ways: overtime ward staffing and delayed elective medical care are also costs of under-planned mental health capacity.[3][14]
Definitive management: priority setting and planning cycle
ACE-Mental Health logic (high-yield ANZ)
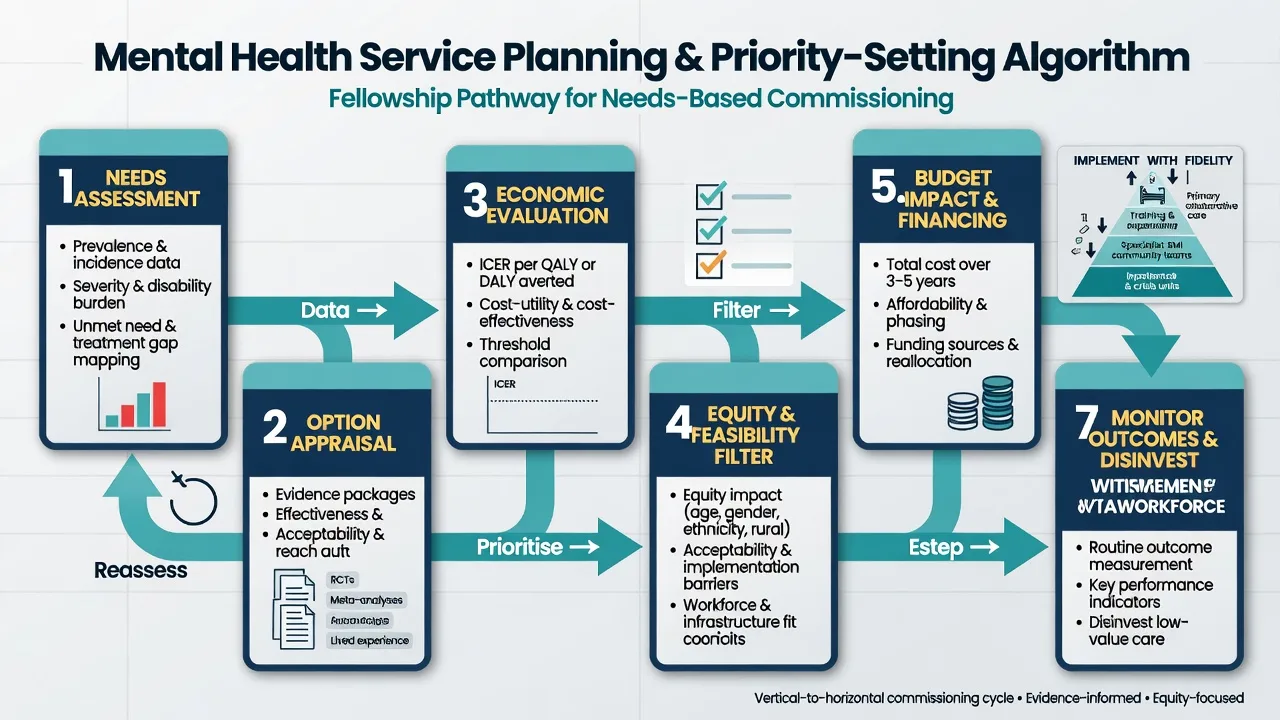
The Australian Assessing Cost-Effectiveness — Mental Health (ACE-MH) programme provides a fellowship-friendly method story: define interventions, model costs and health gains with consistent methods, produce comparative cost-effectiveness information, then apply second-stage filters (equity, feasibility, strength of evidence, acceptability) rather than pure rank dictatorship.[9][10][11]
Examples within that tradition include modelling family interventions and vocational packages for schizophrenia-related conditions as part of broader priority setting — the exam point is the method, not memorising every modelled ICER.[10]
Population CE of better coverage
Multi-region modelling suggests scaled depression interventions can be cost-effective in many settings when organised efficiently.[7] Modelling of current versus optimal schizophrenia treatment illustrates inefficiency of partial, late, or poorly coordinated care relative to evidence-based packages.[8]
Global scale-up and financing
Effective treatment and prevention options exist for LMICs, but barriers include governance, stigma, low political priority, and weak community platforms — not only absence of drugs.[4][5] The 2018 Lancet Commission reframes mental health within sustainable development, rights, and whole-of-society action, with financing and implementation as central tasks.[6]
Workforce strategies (training, task-sharing, retention, skill-mix) are economic interventions because labour is the main production function of mental health care.[12]
Balanced community architecture
Efficient systems use stepped intensity: primary collaborative care for common disorders, secondary teams for SMI, intensive outreach for high-need disengaged people, crisis alternatives where safe, and retained acute beds — with continuity and fidelity, not brand names alone.[14]
Subtypes and exam scenarios
- Formulary / HTA stem: new agent, modest benefit, high price → demand incremental analysis vs standard care, adverse-effect costs, and budget impact.
- Common mental disorder scale-up: collaborative care / stepped psychological therapy as population CE play.[7]
- SMI intensive packages: ACT/ICM expansion justified by high bed use and disengagement — still require fidelity and step-down to protect scarce slots.[14]
- Early intervention investment: long disability horizon may favour earlier packages in business cases (link early-psychosis topics).
- LMIC primary care scale-up: packages exist; fix financing, supervision, and medicines supply.[5][4]
- Disinvestment: low-fidelity day programmes, duplicate assessment teams, or care without outcome monitoring.
Complications and pitfalls
- Treating cost-of-illness headlines as automatic funding entitlement.[13]
- Short horizons that ignore chronic disability.
- Importing foreign CE thresholds without local prices or values.
- Equity blindness (average CE that abandons remote or Indigenous populations).
- Ignoring carer and productivity costs — or double-counting them.
- "Efficiency" that shifts risk to emergency departments and police.
- Workforce plans that assume infinite psychiatrists without training pipelines.[12]
Prognosis and disposition of programmes
Sustainable programmes need recurrent funding, supervision, fidelity review, and outcome dashboards. Disposition decisions for services mirror clinical step-up/step-down: expand when unmet high-need demand and CE/equity support it; step down or disinvest when value is low or capacity is captured by lower-need users.[10][11]
Special populations
- Youth: longer lifetime horizon for benefits of early effective care.
- Older adults: multimorbidity costs and informal care dominate.
- SMI: high direct costs plus housing/employment externalities.
- Rural/Indigenous: access costs and equity weights matter as much as average ICER.
- LMIC and high OOP settings: financial protection is part of the intervention.[4][6]
Evidence and guidelines (named anchors)
| Anchor | Pearl |
|---|---|
| Whiteford GBD 2013 | Mental/substance disorders large YLD contribution |
| Prince 2007 | No health without mental health |
| Saxena 2007 | Scarcity, inequity, inefficiency |
| Saraceno / Patel 2007 | Barriers and effective packages in LMIC |
| Patel Commission 2018 | MH in SDG/rights frame; implementation and financing |
| Chisholm 2004 | Depression intervention CE across regions |
| Andrews 2003 | Current vs optimal schizophrenia treatment CE |
| ACE-MH (Haby/Vos/Carter) | Methods for priority setting with second-stage filters |
| Kakuma 2011 | Workforce as binding constraint |
| Greenberg 2015 | Depression economic burden including workplace |
| Thornicroft 2016 | Community balanced care principles worldwide |
Exam pearls
- Opportunity cost is the first sentence of any viva answer.
- QALY/DALY allow comparison across dissimilar programmes; symptom scores alone do not.
- Burden argues importance; CE + equity + feasibility argue priority (ACE logic).[10][11]
- Budget impact ≠ ICER. Both needed for real decisions.
- Scarcity–inequity–inefficiency triad is examiner gold.[3]
- Do not invent local bed prices, MBS item numbers, or a single universal cost-per-QALY threshold as statute.
- Service planning loop: need → evidence packages → economic appraisal → equity/feasibility → finance and workforce → implement with fidelity → evaluate/disinvest.[10][12][14]
References
- [1]Whiteford HA, Degenhardt L, Rehm J, et al. Global burden of disease attributable to mental and substance use disorders: findings from the Global Burden of Disease Study 2010 Lancet, 2013.PMID 23993280
- [2]Prince M, Patel V, Saxena S, et al. No health without mental health Lancet, 2007.PMID 17804063
- [3]Saxena S, Thornicroft G, Knapp M, Whiteford H Resources for mental health: scarcity, inequity, and inefficiency Lancet, 2007.PMID 17804062
- [4]Saraceno B, van Ommeren M, Batniji R, et al. Barriers to improvement of mental health services in low-income and middle-income countries Lancet, 2007.PMID 17804061
- [5]Patel V, Araya R, Chatterjee S, et al. Treatment and prevention of mental disorders in low-income and middle-income countries Lancet, 2007.PMID 17804058
- [6]Patel V, Saxena S, Lund C, et al. The Lancet Commission on global mental health and sustainable development Lancet, 2018.PMID 30314863
- [7]Chisholm D, Sanderson K, Ayuso-Mateos JL, Saxena S Reducing the global burden of depression: population-level analysis of intervention cost-effectiveness in 14 world regions Br J Psychiatry, 2004.PMID 15123502
- [8]Andrews G, Sanderson K, Corry J, et al. Cost-effectiveness of current and optimal treatment for schizophrenia Br J Psychiatry, 2003.PMID 14594918
- [9]Haby MM, Carter R, Mihalopoulos C, et al. Assessing Cost-Effectiveness--Mental Health: introduction to the study and methods Aust N Z J Psychiatry, 2004.PMID 15298579
- [10]Vos T, Haby MM, Magnus A, et al. Assessing cost-effectiveness in mental health: helping policy-makers prioritize and plan health services Aust N Z J Psychiatry, 2005.PMID 16050924
- [11]Carter R, Vos T, Moodie M, et al. Priority setting in health: origins, description and application of the Australian Assessing Cost-Effectiveness initiative Expert Rev Pharmacoecon Outcomes Res, 2008.PMID 20528370
- [12]Kakuma R, Minas H, van Ginneken N, et al. Human resources for mental health care: current situation and strategies for action Lancet, 2011.PMID 22008420
- [13]Greenberg PE, Fournier AA, Sisitsky T, et al. The economic burden of adults with major depressive disorder in the United States (2005 and 2010) J Clin Psychiatry, 2015.PMID 25742202
- [14]Thornicroft G, Deb T, Henderson C Community mental health care worldwide: current status and further developments World Psychiatry, 2016.PMID 27717265