Psych · Public and community psychiatry — military and veteran psychiatry
Military and veteran psychiatry
Also known as Veteran mental health · Military psychiatry · Combat-related PTSD · Operational mental health · Moral injury veterans · Military sexual trauma MST · Service-related trauma · Transition stress veterans · Deployment mental health
Exam-exhaustive fellowship reference on military and veteran psychiatry — deployment epidemiology, barriers to care, moral injury as formulation, MST, PCL-5/CAPS-5 assessment, PE/CPT evidence, SSRI/SNRI dosing, prazosin equipoise, suicide and weapons risk, transition pathways, and dual-loyalty ethics. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
This topic is high-yield for FRANZCP MEQs and CASC stations, MRCPsych trauma and public-mental-health items, and ABPN veteran-care blueprints. Examiners test named epidemiology papers (Hoge, Fear, Seal, Fulton), moral injury language, PE/CPT evidence in military samples, sertraline/paroxetine/venlafaxine dosing, and the Raskind prazosin controversy.[1][2][11][19]
Overview and definition
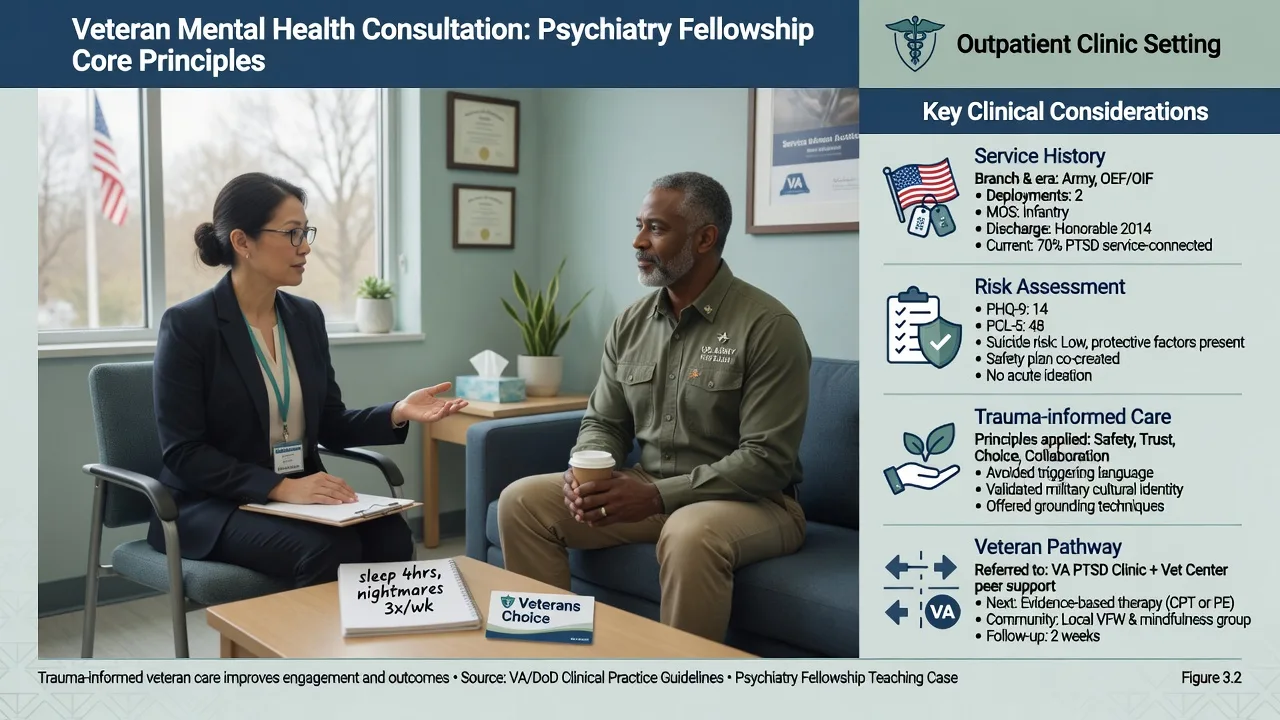
Military and veteran psychiatry is a care context, not a single diagnosis. It covers mental health of active-duty and reserve personnel, veterans after transition, and families affected by service. Clinical tasks include trauma-spectrum disorders, depression, anxiety, substance use, suicide risk, fitness-for-duty interfaces, and navigation of veteran-competent services — without adjudicating compensation claims at the bedside unless that is an instructed dual role.[1][3][6]
Clinical framing. Think across the career arc: pre-deployment selection and training; deployment/operational exposure (combat, peacekeeping, disaster, military sexual trauma); post-deployment reintegration; and transition to civilian life, when identity loss, unemployment, relationship strain, and alcohol escalation commonly unmask or maintain illness. Most service members do not develop PTSD; resilience and recovery are common when supports and treatment access work.[1][2][4]
Nosology. Use DSM-5-TR PTSD (four clusters, duration more than 1 month) or ICD-11 PTSD / complex PTSD when structure fits, plus depressive, anxiety, adjustment, substance-related, and TBI-related diagnoses as indicated. Moral injury (transgression of deeply held moral beliefs by self or others — acts of commission, omission, or betrayal) is a formulation construct, not a DSM/ICD diagnosis; it often co-occurs with PTSD clusters but can present as dominant guilt, shame, and spiritual injury without full PTSD criteria.[5][6]
Classification
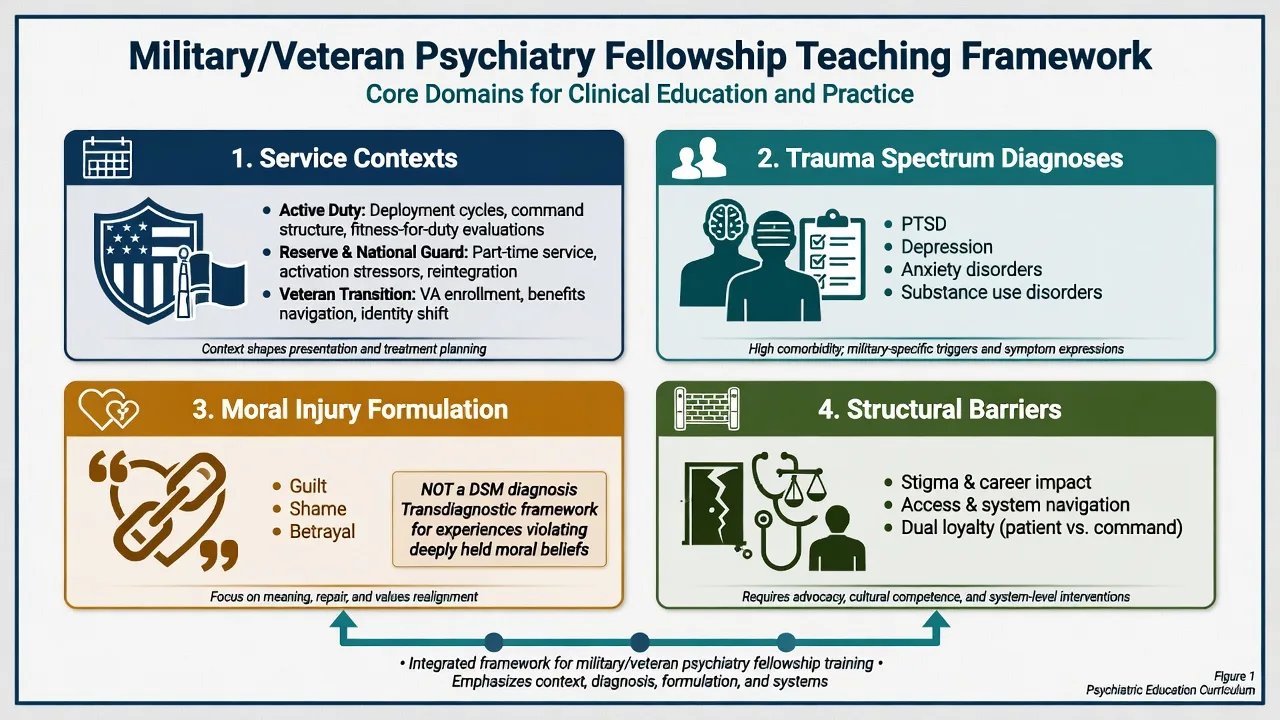
Service context
- Active duty / reserve / veteran
- Rank, role, deployments
- Fitness-for-duty interfaces
- Not a clinical syndrome
PTSD / CPTSD
- Symptom-structure diagnoses
- DSM-5-TR four clusters
- ICD-11 PTSD/CPTSD
- Independent of service label
Moral injury
- Formulation not DSM diagnosis
- Guilt, shame, betrayal
- Self or other transgressions
- Overlaps but not equals PTSD
Structural barriers
- Stigma and career fear
- Access and navigation
- Dual loyalty tensions
- Treat as clinical targets
Epidemiology and risk factors
Headline epidemiology candidates must own
Landmark anchors. Hoge and colleagues (2004) reported substantial mental health symptoms after combat duty in Iraq and Afghanistan and famously quantified barriers to care (stigma, career concerns, access) — the single most examiner-friendly combat psychiatry cite.[1]
Fear and colleagues (2010) examined UK armed forces deployment consequences, highlighting patterns of PTSD symptoms and alcohol misuse and reserve-versus-regular nuances that matter for dual-role personnel.[2]
Seal and colleagues (2007) described mental health diagnoses among more than 100,000 OEF/OIF veterans seen in VA facilities, with a large fraction receiving at least one mental health diagnosis and substantial multi-morbidity — useful for service-planning viva answers, with the caveat that VA users are not all veterans.[3]
Fulton and colleagues (2015) meta-analysed OEF/OIF PTSD prevalence and estimated roughly one in four in included samples, with marked between-study heterogeneity — never quote 23% as "the" global military PTSD rate.[4]
Risk amplifiers. Combat intensity, military sexual trauma, cumulative deployments, TBI/blast exposure, pre-service vulnerability, alcohol and other substances, social isolation after discharge, unemployment, relationship breakdown, and delayed help-seeking.[1][4][6]
Protective factors. Unit cohesion, good leadership, timely access to evidence-based care, peer and family support, meaningful post-service roles, and culturally competent veteran services.[1][2]
Pathophysiology and mechanisms
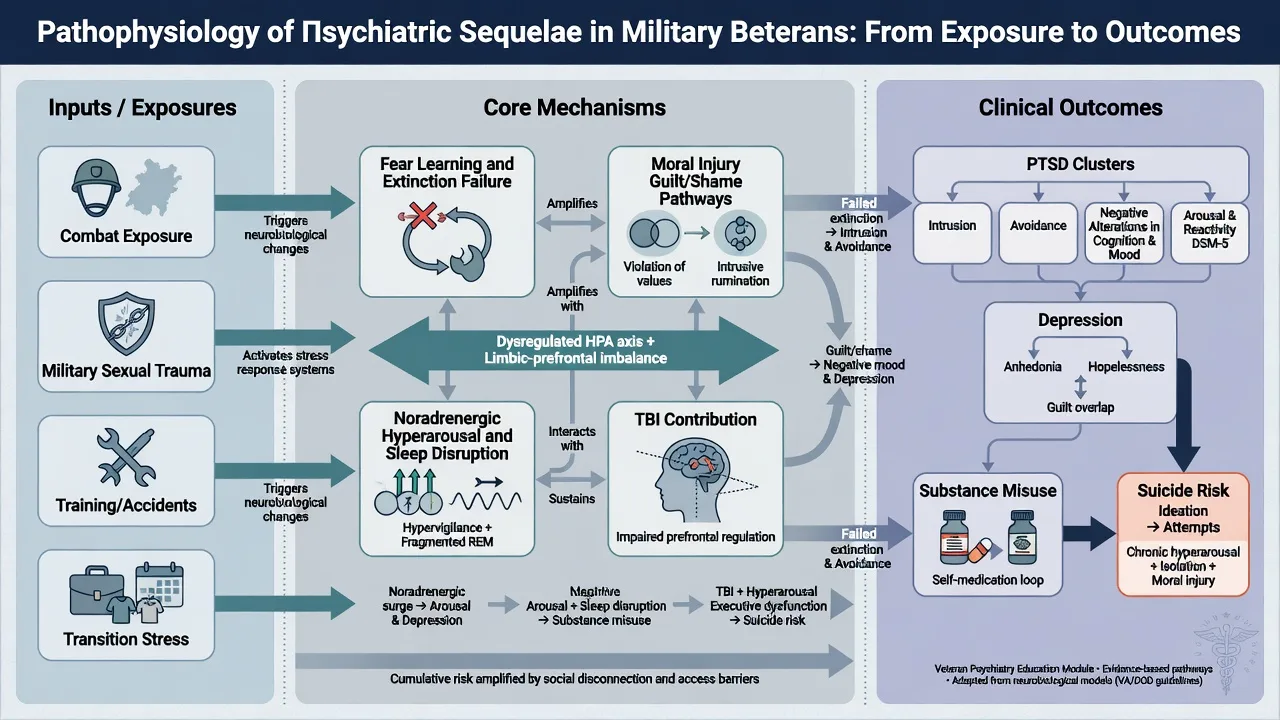
Fear learning and cognition. Combat and other Criterion A events seed conditioned fear and poorly elaborated trauma memories; cognitive models emphasise threat appraisal, memory fragmentation, and maladaptive strategies that maintain intrusion and avoidance. The Yehuda and colleagues disease primer integrates neurobiology with clinical architecture for viva answers.[6]
Moral injury. Litz and colleagues proposed a preliminary model of moral injury and moral repair after potentially morally injurious events (PMIEs) — killing, failing to prevent harm, or betrayal by trusted authorities. Guilt, shame, and loss of trust can drive depression, substance use, and suicide risk even when classic fear-based PTSD clusters are incomplete.[5][20]
Noradrenergic hyperarousal. Heightened noradrenergic tone contributes to hypervigilance, startle, and nightmare physiology — the rationale for alpha-1 antagonism (prazosin) in nightmare-focused treatment, even though later multi-site evidence is mixed.[18][19]
TBI and organic interface. Blast and blunt head injury contribute to irritability, cognitive slowing, headache, and sleep disruption; formulate TBI and PTSD as overlapping rather than mutually exclusive.[6]
Stigma as mechanism. Career threat and warrior-culture norms delay care-seeking, converting treatable early illness into chronic multi-morbidity — name this as a clinical mechanism, not only a policy complaint.[1]
Clinical presentation
Classic combat vignette: recently transitioned infantry veteran with nightmares of firefights, avoidance of crowded shops and news footage, hypervigilance at night, explosive anger at home, heavy evening drinking, and passive death wishes after relationship strain. Quote the patient ("I still scan every rooftop"; "I was supposed to bring them all home").[1][6]
Moral injury vignette. Persistent self-condemnation after an incident that violated personal ethics, or corrosive betrayal by leadership, with shame-driven isolation and suicidal ideation — may or may not meet full PTSD criteria.[5]
Military sexual trauma (MST). Nightmares, mistrust of command and medical systems, mixed PTSD and depression, sexual dysfunction, and avoidance of same-gender or hierarchical clinical settings; enquire privately without forcing graphic detail in the first minutes.[6][10]
MSE focus. Affect may be restricted, irritable, or tearful; thought content often includes threat scanning, guilt, foreshortened future, and service-identity loss; perception may include trauma flashbacks distinguished from primary psychosis; insight into the trauma link is often present; suicide and weapons access must be assessed every contact when risk is plausible.[20]
Differential diagnosis
| Discriminator | Favours trauma/PTSD-spectrum | Favours alternative |
|---|---|---|
| Intrusions linked to specific events, avoidance, hyperarousal more than 1 month | PTSD / CPTSD | Non-specific distress without trauma linkage |
| Dominant guilt/shame after PMIE without full PTSD clusters | Moral injury formulation + depression | Fear-based PTSD alone |
| Pseudo-hallucinatory flashbacks vs novel psychotic percepts with thought disorder | Trauma-related | Primary psychosis / substance-induced |
| Cognitive change after blast/blunt trauma | TBI work-up + PTSD comorbidity | "All psychological" assumption |
| Anger and mistrust only in intimate relationships | Trauma-driven interpersonal pattern | Primary personality disorder alone |
Also discriminate major depression, adjustment disorder after transition, substance-induced states, compensation-context symptom presentation (assess carefully without default disbelief), and organic causes including endocrine and sleep disorders.[3][6]
Clinical and bedside assessment
Service history structure. Branch, rank, military occupational role, number and nature of deployments, combat and non-combat potentially traumatic events, training accidents, disaster/humanitarian missions, disciplinary or administrative actions, discharge type, and current veteran-service engagement. Ask about military sexual trauma in private language that normalises enquiry.[1][7]
Trauma-informed stance. Safety, trustworthiness, choice, collaboration, and cultural humility toward military identity. Obtain enough detail to establish exposure and symptom linkage without forcing a graphic first-session retelling. Offer control over pacing and who is in the room.[6]
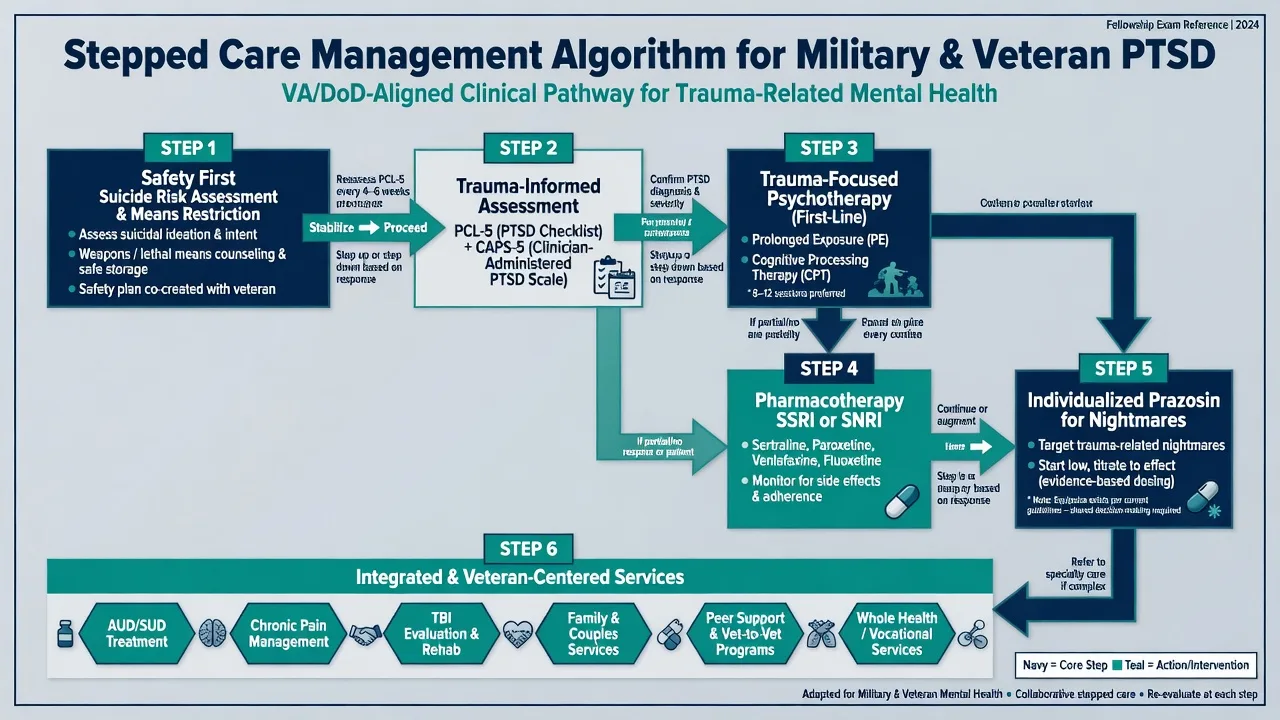
Risk. Suicide (ideation, intent, plan, means — especially firearms), self-harm, violence, intimate partner violence, child protection, and self-neglect. Collaborative safety planning with means restriction. Capacity is decision-specific. Involuntary care uses local Mental Health Act principles — least restrictive; do not invent section numbers for the wrong jurisdiction.[20]
Dual loyalty. When treating serving personnel, clarify confidentiality limits related to fitness-for-duty and safety without abandoning the therapeutic alliance. When writing for compensation systems, separate treating-clinician and independent-examiner roles.[1]
Measures. PCL-5 supports severity monitoring and treatment response tracking; CAPS-5 is a gold-standard diagnostic interview with psychometric evaluation including military veteran samples. Interpret scores alongside clinical interview, not as standalone diagnoses.[7][8]
Investigations
There is no military-specific diagnostic biomarker. Investigate to exclude mimics and prepare for medication: TSH, FBC, U&E, LFT, metabolic panel as indicated; ECG when cardiac risk; pregnancy test when relevant; urine drug screen when substance contribution is plausible; neuroimaging only with neurological red flags (including possible TBI). Document sleep, pain, and substance quantity as formulation data.[6]
Management — acute / resuscitation
Immediate priorities. Physical safety, medical needs, and collaborative safety planning. Manage acute suicidality and agitation through usual pathways while minimising retraumatising coercion where safe alternatives exist. Avoid mandatory single-session critical-incident debriefing as universal prophylaxis for all exposed personnel.[6][14]
Management — definitive and stepwise
Psychological therapies
Prolonged exposure (PE) and cognitive processing therapy (CPT) are first-line trauma-focused options with strong adult PTSD evidence and specific military/veteran trials. Monson and colleagues demonstrated CPT benefit for veterans with military-related PTSD. Schnurr and colleagues showed PE efficacy in a women veterans / women trauma RCT context highly cited in military care teaching. Foa and colleagues established PE efficacy in academic and community clinics; Powers meta-analysis supports PE effect sizes across samples.[9][10][12][13]
Military psychotherapy synthesis. Steenkamp, Litz, Hoge and Marmar (2015) reviewed RCTs of psychotherapy for military-related PTSD: CPT and PE are the most studied trauma-focused therapies, yet many patients retain substantial residual symptoms — temper over-claiming of cure rates in viva answers.[11]
Broader adult PTSD psychotherapy systematic reviews (including Cochrane) support trauma-focused psychological therapies as first-line when available and acceptable.[14]
Pharmacotherapy — agent, dose, monitoring
Medication does not replace trauma-focused psychological treatment when that treatment is available and acceptable. When chosen (preference, limited therapy access, severe comorbid depression/anxiety, partial response), SSRIs and SNRIs have RCT support for PTSD symptoms.[15][16][17]
| Agent | Typical adult start | Common range | Monitoring notes |
|---|---|---|---|
| Sertraline | 25–50 mg orally daily | 50–200 mg daily | Sexual dysfunction, GI effects; early review for activation/suicidality |
| Paroxetine | Per fixed-dose trial protocols; often 20 mg oral daily class start | Individualise (trial used fixed doses) | Anticholinergic effects, discontinuation syndrome; pregnancy counselling |
| Venlafaxine XR | Low oral daily start, titrate | Toward evidence-based antidepressant ranges for PTSD | BP monitoring; discontinuation symptoms; suicide risk early in treatment |
| Prazosin (nightmares) | Often 1 mg orally at night, slow titration | Individualise; BP-guided | Dizziness, falls, orthostatic hypotension; equipoise counselling |
Prazosin equipoise (exam classic). Raskind and colleagues (2013) found benefit for combat-related nightmares in active-duty soldiers; the large multi-site 2018 NEJM trial in military veterans did not show superiority over placebo for primary PTSD outcomes. Exam stance: discuss mixed evidence; consider a carefully monitored individual trial when nightmares dominate, blood pressure allows, and the patient is informed; do not present prazosin as mandatory or universally effective.[18][19]
Avoid reflexive long-term benzodiazepines for core trauma symptoms (dependence risk; interference with extinction learning). Address alcohol and other substance use as co-primary targets, not afterthoughts.[6][14]
Integrated and service-level care
Integrate pain, sleep, TBI rehabilitation, family-inclusive practice, peer/veteran supports, and vocational rehabilitation. Continuity across military-to-civilian transition is a major quality lever — fragmented handover is a common system failure. Name local veteran-competent services as a class (e.g. DVA-linked or VA-type pathways) without inventing funding rules or statute numbers.[3][11]
ANZ: Veteran mental health and DVA-linked pathways are high-yield; apply RANZCP trauma principles and local Mental Health Act least-restrictive standards — do not invent entitlement sections. UK: Fear cohort data and NHS/armed forces pathways; NICE PTSD principles with military cultural competence. US/Canada: VA/DoD-class systems, MST screening expectations, and ABPN veteran-care items; APA trauma-informed principles apply. Global: Peacekeeping and conscript systems differ; same clinical principles of trauma-focused care, risk assessment, and stigma reduction apply.[2][3][11][14]
Subtypes and clinical scenarios
- Active-duty combat-exposed: dual loyalty, fitness-for-duty, unit return-to-duty planning.[1]
- Reservists: dual civilian-military stress; UK cohort relevance for reserves.[2]
- Women and MST survivors: private enquiry, preference for clinician gender, system trust repair.[10]
- Transition window: identity loss, alcohol escalation, unemployment, high suicide vigilance.[3][20]
- Older veterans of earlier conflicts: chronic PTSD, substance patterns, medical comorbidity.
- High-ops tempo / special roles: cumulative load, secrecy constraints, peer stigma.
- Peacekeeping/disaster deployments: moral injury and helplessness themes without classic firefight trauma.[5]
- Medico-legal/compensation interface: dual-role ethics; longitudinal consistency without default disbelief.
Complications and pitfalls
Stereotyping ("all veterans have PTSD"); missing MST; ignoring moral injury when guilt dominates; under-assessing firearms and suicide; presenting prazosin as proven for all combat nightmares; long-term benzodiazepines for core trauma; dual-loyalty failures; inventing compensation statutes; equating alcohol "self-medication" with an adequate treatment plan; failing to plan transition continuity.[1][5][19][20]
Prognosis and disposition
Many improve with evidence-based trauma-focused care and social recovery, but military psychotherapy syntheses caution that residual symptoms are common — plan measurement-based follow-up rather than single-session optimism.[11][14]
Step-up for active suicidal intent, psychosis, severe withdrawal, unsafe weapon access, or failed outpatient engagement. Step-down when risk is managed, symptoms improve on PCL-5 and function, and social supports are stable. Disposition spans primary care collaborative care, specialist trauma psychology, veteran services, and inpatient care when required.[8][11][20]
Special populations
Women and gender-diverse service members; MST survivors; Indigenous and culturally diverse veterans; reservists and remote veterans; older veterans with cognitive comorbidity; partners and children (secondary trauma, IPV risk); personnel with amputation, chronic pain, or disability; LGBTQIA+ service members navigating stigma within hierarchical systems.[2][6][10]
Evidence and guidelines
Anchor answers to named papers: Hoge 2004; Fear 2010; Seal 2007; Fulton 2015; Litz moral injury; Yehuda primer; CAPS-5/PCL-5; Monson CPT; Schnurr PE; Steenkamp 2015 military psychotherapy review; Foa/Powers PE evidence; Bisson Cochrane; Brady/Marshall/Davidson pharmacotherapy; Raskind 2013 vs 2018 prazosin; Pompili suicide review. Know that RANZCP, NICE, APA, and VA/DoD-class frameworks inform practice — cite principles, not invented page numbers.[1][2][5][11][14][19]
Exam pearls
VETERAN care checklist
References
- [1]Hoge CW, Castro CA, Messer SC, McGurk D, et al. Combat duty in Iraq and Afghanistan, mental health problems, and barriers to care N Engl J Med, 2004.PMID 15229303
- [2]Fear NT, Jones M, Murphy D, Hull L, et al. What are the consequences of deployment to Iraq and Afghanistan on the mental health of the UK armed forces? A cohort study Lancet, 2010.PMID 20471076
- [3]Seal KH, Bertenthal D, Miner CR, Sen S, Marmar C Bringing the war back home: mental health disorders among 103,788 US veterans returning from Iraq and Afghanistan seen at Department of Veterans Affairs facilities Arch Intern Med, 2007.PMID 17353495
- [4]Fulton JJ, Calhoun PS, Wagner HR, Schry AR, et al. The prevalence of posttraumatic stress disorder in Operation Enduring Freedom/Operation Iraqi Freedom (OEF/OIF) Veterans: a meta-analysis J Anxiety Disord, 2015.PMID 25768399
- [5]Litz BT, Stein N, Delaney E, Lebowitz L, et al. Moral injury and moral repair in war veterans: a preliminary model and intervention strategy Clin Psychol Rev, 2009.PMID 19683376
- [6]Yehuda R, Hoge CW, McFarlane AC, Vermetten E, et al. Post-traumatic stress disorder Nat Rev Dis Primers, 2015.PMID 27189040
- [7]Weathers FW, Bovin MJ, Lee DJ, Sloan DM, Schnurr PP, et al. The Clinician-Administered PTSD Scale for DSM-5 (CAPS-5): Development and initial psychometric evaluation in military veterans Psychol Assess, 2018.PMID 28493729
- [8]Blevins CA, Weathers FW, Davis MT, Witte TK, Domino JL The Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): Development and Initial Psychometric Evaluation J Trauma Stress, 2015.PMID 26606250
- [9]Monson CM, Schnurr PP, Resick PA, Friedman MJ, et al. Cognitive processing therapy for veterans with military-related posttraumatic stress disorder J Consult Clin Psychol, 2006.PMID 17032094
- [10]Schnurr PP, Friedman MJ, Engel CC, Foa EB, Shea MT, et al. Cognitive behavioral therapy for posttraumatic stress disorder in women: a randomized controlled trial JAMA, 2007.PMID 17327524
- [11]Steenkamp MM, Litz BT, Hoge CW, Marmar CR Psychotherapy for Military-Related PTSD: A Review of Randomized Clinical Trials JAMA, 2015.PMID 26241600
- [12]Foa EB, Hembree EA, Cahill SP, Rauch SA, et al. Randomized trial of prolonged exposure for posttraumatic stress disorder with and without cognitive restructuring: outcome at academic and community clinics J Consult Clin Psychol, 2005.PMID 16287395
- [13]Powers MB, Halpern JM, Ferenschak MP, Gillihan SJ, Foa EB A meta-analytic review of prolonged exposure for posttraumatic stress disorder Clin Psychol Rev, 2010.PMID 20546985
- [14]Bisson JI, Roberts NP, Andrew M, Cooper R, Lewis C Psychological therapies for chronic post-traumatic stress disorder (PTSD) in adults Cochrane Database Syst Rev, 2013.PMID 24338345
- [15]Brady K, Pearlstein T, Asnis GM, Baker D, et al. Efficacy and safety of sertraline treatment of posttraumatic stress disorder: a randomized controlled trial JAMA, 2000.PMID 10770145
- [16]Marshall RD, Beebe KL, Oldham M, Zaninelli R Efficacy and safety of paroxetine treatment for chronic PTSD: a fixed-dose, placebo-controlled study Am J Psychiatry, 2001.PMID 11729013
- [17]Davidson J, Baldwin D, Stein DJ, Kuper E, et al. Treatment of posttraumatic stress disorder with venlafaxine extended release: a 6-month randomized controlled trial Arch Gen Psychiatry, 2006.PMID 17015818
- [18]Raskind MA, Peterson K, Williams T, Hoff DJ, et al. A trial of prazosin for combat trauma PTSD with nightmares in active-duty soldiers returned from Iraq and Afghanistan Am J Psychiatry, 2013.PMID 23846759
- [19]Raskind MA, Peskind ER, Chow B, Harris C, et al. Trial of Prazosin for Post-Traumatic Stress Disorder in Military Veterans N Engl J Med, 2018.PMID 29414272
- [20]Pompili M, Sher L, Serafini G, Forte A, et al. Posttraumatic stress disorder and suicide risk among veterans: a literature review J Nerv Ment Dis, 2013.PMID 23995037