Psych · public-community
Quality improvement and patient safety in psychiatry
Also known as Clinical governance mental health · Patient safety psychiatry · QI PDSA psychiatry · Human factors mental health · Just culture psychiatry · Safewards quality improvement · Serious incident review mental health · Donabedian structure process outcome
Exam-exhaustive fellowship topic on quality improvement and patient safety in psychiatry: Donabedian measures, Model for Improvement/PDSA, systems thinking and Swiss-cheese human factors, just culture, psychiatry-specific harm domains, Safewards and suicide-prevention service design, measurement (outcome/process/balancing), RCA pitfalls, and regional governance frames (ACSQHC/NICE/APA). FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Definition and classification
Fellowship answers start with precise language. Quality of care is the degree to which health services increase the likelihood of desired outcomes and are consistent with current professional knowledge. A useful domain set (safe, effective, patient-centred, timely, efficient, equitable) orients design; safety is necessary but not sufficient for quality — ineffective, inequitable, or delayed care can still be "safe" in a narrow sense.[1][4]
Patient safety focuses on reducing preventable harm from care itself — the core of modern safety science after landmark error literature reframed harm as a systems problem.[2][3] Core terms used in incident review:
| Term | Working definition | Psychiatry example |
|---|---|---|
| Adverse event | Unintended injury or complication from care | Postural injury after restraint; lithium toxicity from failed level monitoring |
| Preventable adverse event | AE judged avoidable with better systems | Missed high-risk observation after expressed suicidal plan |
| Near miss | Hazard that did not reach the patient (or reached without harm) | Wrong depot drawn, caught at double-check |
| Hazard / latent condition | System condition that makes error more likely | Ligature-rich bathroom design; chronic understaffing |
| Never event (local lists) | Serious, largely preventable event defined by jurisdiction | Do not invent a universal list in exams |
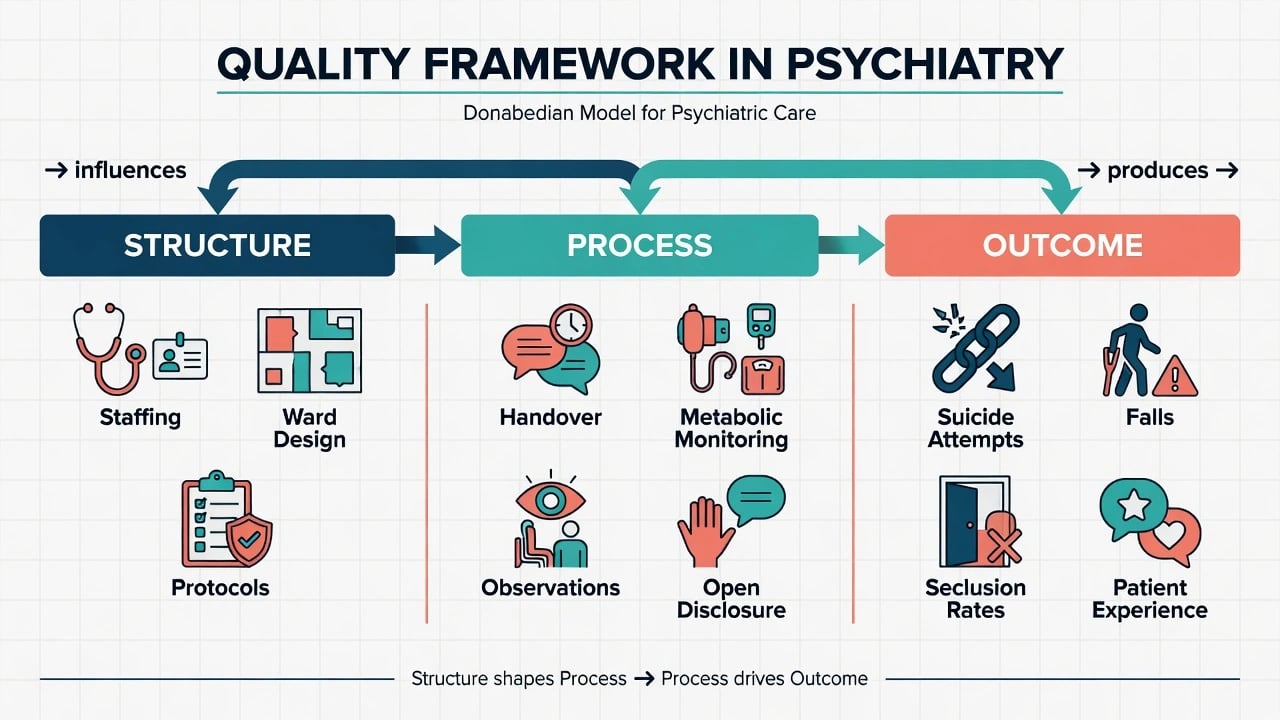
Donabedian's classic triad remains examiner gold:[1]
- Structure — people, skills, buildings, equipment, policies (e.g. ligature-reduced environment, clozapine registry access, observation policy).
- Process — what is done (timely post-discharge contact, metabolic monitoring, medication reconciliation, open disclosure).
- Outcome — what happens (completed suicide, seclusion hours, assault rates, readmission, patient-reported experience).
Distinguish quality assurance/audit (compare practice to standard), quality improvement (iterative redesign toward a measured aim), research (generate generalisable knowledge under ethics frameworks), and clinical governance (the organisational system that assures quality and accountability). Labeling a single retrospective audit "QI" without cycles of change is a common exam trap.[12]
Epidemiology and risk landscape
Healthcare harm is common enough that safety is core professional work, not optional bureaucracy. Landmark hospital studies established that adverse events affect a substantial minority of admissions and that many are preventable; the exact percentages vary by method, but the direction of travel for examiners is clear: systems produce predictable harm if left unexamined.[3][5]
Inpatient mental health has a distinctive profile. Systematic review of patient safety in inpatient mental health settings highlights self-harm and suicide, violence and aggression, absconding, medication-related problems, accidents/falls, and coercive practices among dominant themes — not merely "medical" complications imported from general wards.[11] Medication error literature specific to inpatient psychiatry documents that psychotropic complexity, PRN culture, and information gaps create a real safety surface.[13]
Suicide after contact with services is a population-level quality signal. National clinical survey work established that a large share of suicides occur in people with recent mental health service contact, making follow-up design, risk formulation, and access after discharge organisational safety issues, not only bedside assessment skill.[10] Observational data from England and Wales linked greater implementation of National Confidential Inquiry service recommendations to lower suicide rates — a high-yield pearl that service design changes can move hard outcomes.[9]
Environmental risk for inpatient hanging clusters around available ligature points and materials; national analysis of ligature points and types informs environmental QI priorities (bathroom/bedroom fixtures, doors, rails) rather than vague "be more careful" exhortations.[14]
Mechanisms: human factors and systems thinking
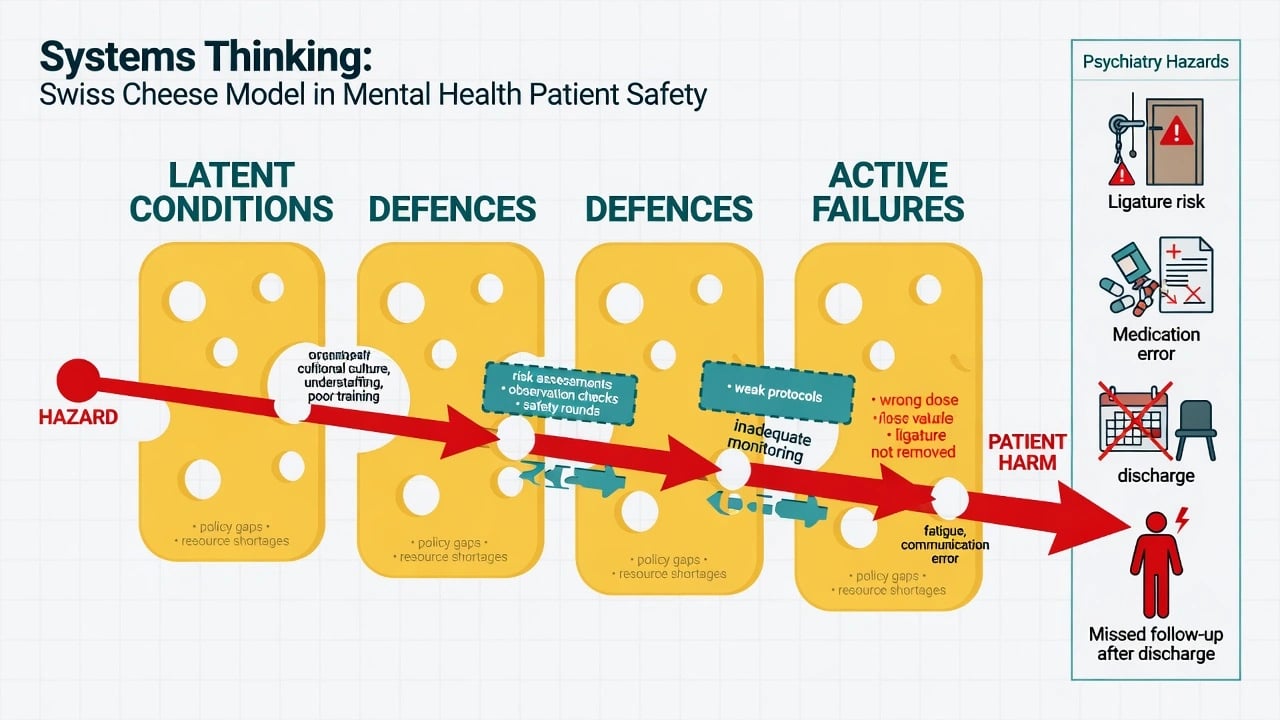
Leape's classic argument reframed medical error as a systems problem requiring industrial-grade safety science, not moral failing alone.[3] Reason's models distinguish the person approach (blame, train, write a policy) from the system approach (accept fallibility; design defences). The Swiss-cheese model depicts successive defensive layers; harm occurs when holes (latent conditions and active failures) transiently align.[2]
In psychiatry the same architecture applies to mental-health-specific hazards (self-harm, violence, absconding, medication error, restrictive practice).[2][11] Latent conditions include production pressure, poorly designed observation policies, ligature-rich environments, fragmented electronic records, weak weekend medical cover, and cultures that punish reporting. Active failures include missed risk reassessment after bad news, wrong dose, incomplete leave decision, and failed double-check on high-alert meds. Defences include standardised handovers, independent double-checks for high-risk drugs, environmental design, safety huddles, and second-check of leave and discharge plans.[2][3][14]
Just culture separates human error (console, redesign), at-risk behaviour (coach, remove incentives for shortcuts), and reckless conduct (strong accountability). Blame culture drives under-reporting; under-reporting starves learning systems. Psychological safety for speaking up is therefore a clinical safety mechanism, not a soft HR slogan.[2][3]
Clinical "presentations" of safety failure
Examiners present safety as cases, not theory — reflecting the inpatient mental health safety profile in systematic review and suicide-after-contact epidemiology:[10][11]
- Completed suicide days after discharge with no follow-up plan or crisis contacts.
- Restraint-related injury or near asphyxia after prolonged prone hold.
- Absconding from an unlocked leave status mismatched to risk.
- Clozapine continued without timely bloods; lithium toxicity after failed monitoring across shared care.
- Polypharmacy PRN escalation without review of total daily antipsychotic load.
- Fall with fracture in an older inpatient on multiple sedating agents.
- Ward culture of high seclusion hours with no reduction strategy or data transparency.
Also recognise organisational presentations: falling incident reporting after a punitive investigation; rising "informal" containment not coded as seclusion; staff second-victim distress after a death. These are culture and measurement failures as much as individual events.[2][3]
Differential framing for governance
- Unintended slip/lapse
- System contribution likely
- Console + redesign
- Reporting must feel safe
- Workaround normalised
- Incentives favour speed
- Coach + fix incentives
- Do not only retrain
- Conscious unjustified risk
- Rare but real
- Strong accountability
- Still learn system enablers
Also differentiate: illness trajectory vs iatrogenic harm; research vs QI ethics pathways; serious incident requiring formal review vs common-cause variation needing local PDSA; true outcome improvement vs documentation compliance only — QI begins when you test changes, not when you only re-measure the same gap.[4][12]
Assessment at the sharp end (bedside and board)
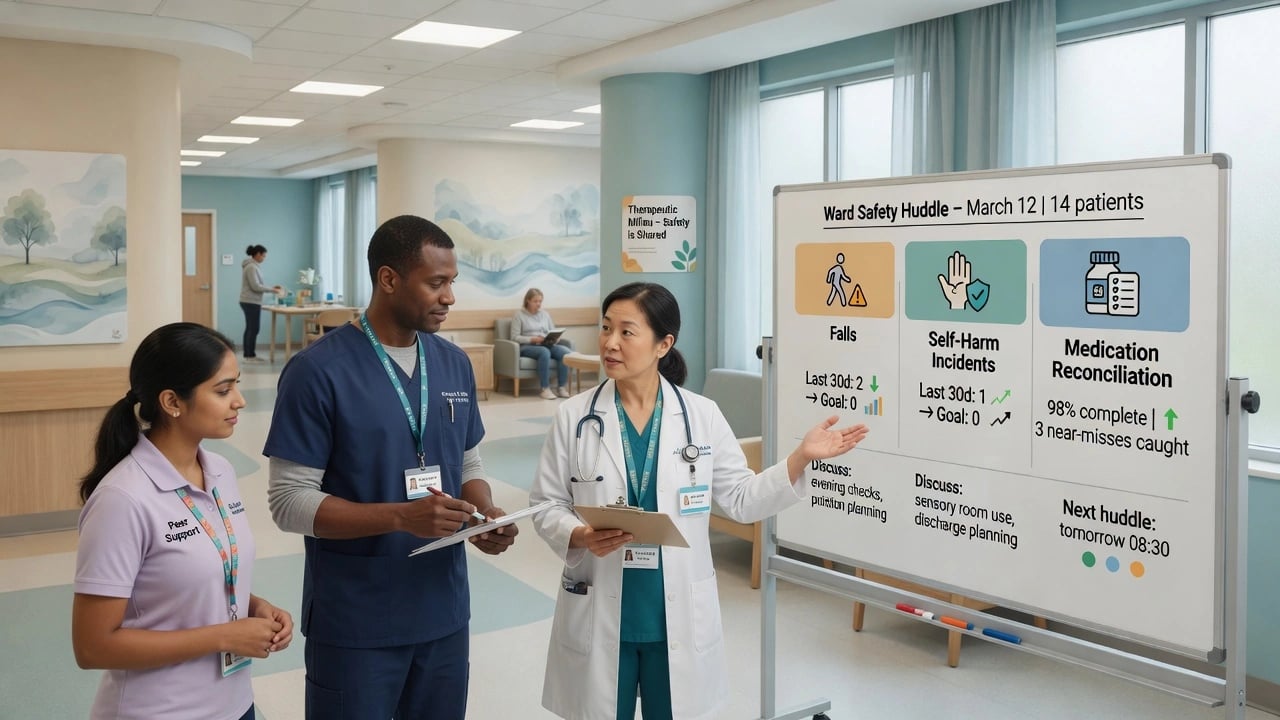
Safety huddle structure: known high-risk patients; observation/leave status; environmental hazards; staffing and skill-mix; pending high-risk meds (clozapine, lithium, depots); contingency for violence or absconding; learning from yesterday's near misses. Huddles operationalise continuous improvement and situational awareness at the sharp end.[4][12]
Suicide environment check: ligature survey mindset informed by what is actually used in fatal hanging events; observation quality (engagement, not tick-box); leave and off-ward risk.[14]
Medication safety: reconciliation at transitions; high-alert list; allergy and interaction checks; metabolic and ECG monitoring as process reliability problems, not optional extras.[13]
Communication: ISBAR/SBAR for escalation; closed-loop orders; documented crisis and safety plans that patients can actually use after discharge.[10]
"Investigations" — measurement and review methods
QI lives or dies on measurement. For any project, pre-specify outcome, process, and balancing measures as core improvement science practice.[12]
- Outcome measures — what matters to patients (e.g. self-harm incidents, seclusion episodes, 7-day post-discharge follow-up completed, metabolic panel completion).
- Process measures — whether the change is actually happening (huddle fidelity, Safewards intervention delivery, med rec completion).
- Balancing measures — unintended consequences (assaults when seclusion falls; therapeutic contact time when observation intensity rises; staff injury).
Use run charts conceptually to separate common-cause from special-cause variation; do not declare victory on a single month. Root cause analysis / serious incident review is for learning after severe harm, but classic traps include hindsight bias, stopping at the individual, and producing recommendations that are not SMART or resourced. Pair deep dives with continuous improvement, not instead of it.[2][12]
Acute response after harm
When harm occurs: stabilise the patient clinically; ensure scene safety; support family with open disclosure principles (what is known, apology for harm, next steps) under local duty-of-candour frameworks without inventing statute names; support staff second victims; preserve facts for learning; escalate via local serious-incident pathway. Immediate "stop the line" redesign may be needed for an ongoing hazard (active ligature point, wrong-route risk, broken monitoring pathway) — the systems response after harm is part of safety, not an optional add-on.[2][3][14]
Definitive management: how to run QI that works
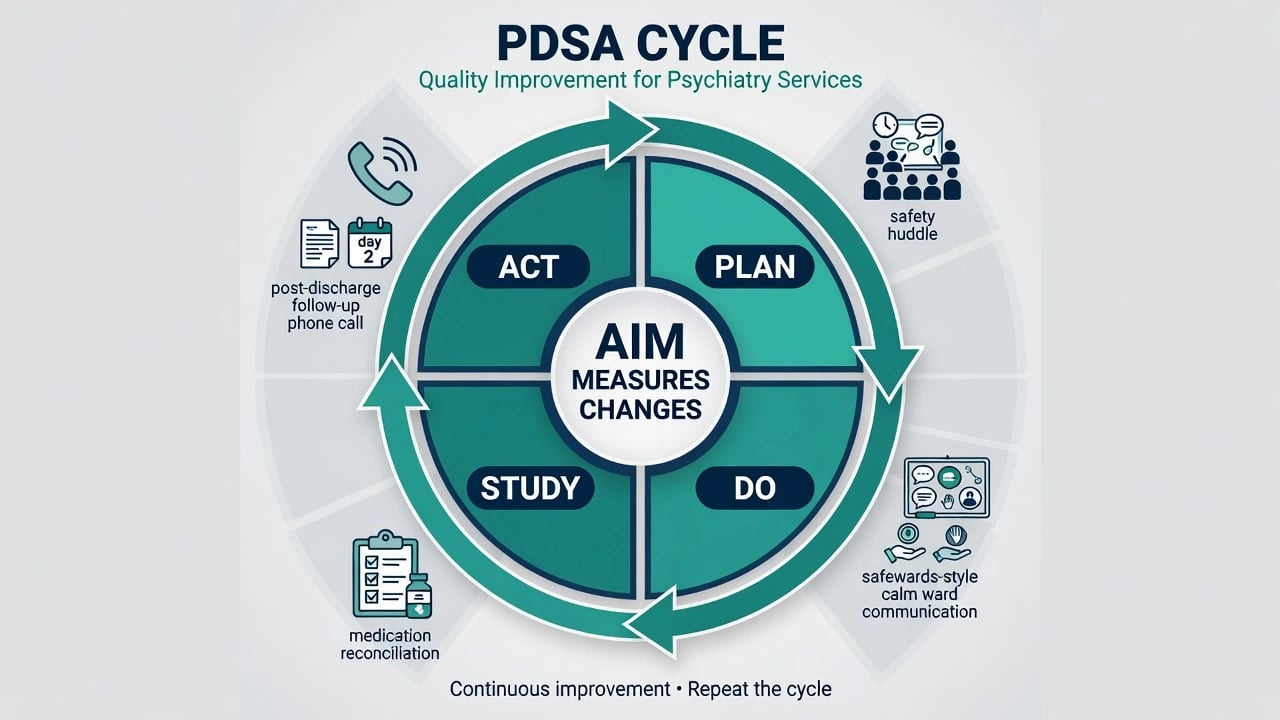
Model for Improvement (three questions + PDSA): What are we trying to accomplish? How will we know a change is an improvement? What changes can we test? Then Plan-Do-Study-Act in small cycles, scale what works, abandon what does not.[4][12] Continuous improvement as a cultural ideal beats episodic inspection alone.[4]
Change packages with psychiatric evidence anchors combine general safety science with mental-health-specific trials and service studies:[6][7][8]
- Safewards — a model of conflict and containment on psychiatric wards with a set of low-cost interventions aimed at staff skills and relationships; cluster RCT evidence of reduced conflict and containment rates when delivered with fidelity.[7][8]
- Suicide-prevention service recommendations — organisational actions (e.g. assertive follow-up after discharge/missed contact, removing ligature risks, dual diagnosis focus, 24-hour crisis arrangements — as framed in NCI-type recommendations) whose broader implementation was associated with lower suicide rates in national observational analysis.[9][10]
- Checklist/system standardisation logic — Pronovost's ICU central-line bundle is the general exemplar that reliable processes beat heroism; adapt carefully to mental health (do not cargo-cult ICU forms onto therapeutic relationships).[6]
- Medication safety redesign — double-checks, reconciliation at transitions, formulary decision support, pharmacist integration, PRN governance.[13]
Leadership and culture: visible executive sponsorship, transparent data, consumer co-design, training that includes human factors, and feedback loops so reporters see that reporting changes care — continuous improvement as a cultural ideal, not a quarterly project.[2][4]
Subtypes and scenarios
Safety priorities shift by setting, but the same measurement and systems methods apply across the pathway from ward to community to shared care.[9][10][11]
| Setting | Typical safety QI focus |
|---|---|
| Acute inpatient | Conflict/containment (Safewards), observation quality, absconding, falls, environment |
| Post-discharge | 48–72 h contact, crisis plan, med continuity, family involvement |
| CMHT / community | Missed visits, depot reliability, lone working, carer alerts |
| ED / liaison | Boarding, medical clearance gaps, behavioural emergency pathways |
| Clozapine / high-alert clinics | Blood monitoring reliability as a never-miss process |
| Old-age | Falls, delirium, polypharmacy, choking |
| CAMHS | Restrictive practice culture, self-harm contagion, family communication |
| Forensic | Dual clinical-security governance, equity in containment |
| Shared care | Lithium/level monitoring across primary–secondary interfaces |
Complications and pitfalls
Other traps: ignoring balancing measures; Safewards branding without intervention fidelity; physical health framed as "not psychiatry"; confidentiality used to avoid open disclosure; endless individual training while latent design flaws remain; copying ICU checklists without human-factors fit to relational MH care.[6][7][8]
Prognosis and disposition of improvement work
Success is sustained shift on a run chart with acceptable balancing measures, not a trophy audit. After serious incidents, disposition includes clinical aftercare, organisational learning products that frontline staff can use, and staff support. Scale local PDSA wins only when context and fidelity can travel; otherwise spread the principles, not the PowerPoint. Continuous improvement cultures outperform one-off inspection cycles.[4][12]
Special populations
Children and adolescents need developmentally appropriate environments and family-inclusive safety design; older adults combine falls, frailty, and sedative load; intellectual disability care must counter diagnostic overshadowing and communication barriers; Indigenous and minority populations require equity metrics because coercion and access gaps are quality issues; perinatal services must document mother–infant safety planning; forensic and dual-diagnosis services carry higher baseline containment risk and need stronger governance transparency. Equity and setting-specific design are quality domains, not optional extras to the safety agenda.[9][11]
Evidence and regional guidelines
Safety science landmarks: Donabedian measurement architecture; Leape on error in medicine; Reason on models of error; Vincent et al. on hospital adverse events; Pronovost as systems-intervention exemplar.[1][2][3][5][6]
Psychiatry-specific: Safewards model and cluster RCT; Thibaut inpatient MH safety systematic review; Grasso on medication errors; Hunt on ligature points; Appleby on suicides after service contact; While on recommendation implementation and suicide rates.[7][8][9][10][11][13][14]
Exam pearls
- Donabedian triad with a psych example each is almost always rewarded.[1]
- PDSA means iterative small tests, not a rebranded audit.[12]
- While 2012 pearl: more implemented service recommendations, lower suicide rates — organisational QI can move mortality signals.[9]
- Safewards has model + cluster RCT; do not claim it cures all aggression or replaces individual risk work.[7][8]
- Post-contact/post-discharge windows are classic suicide QI targets.[10]
- Just culture ≠ no accountability.
- Fix systems; train people; measure both.
References
- [1]Donabedian A Evaluating the quality of medical care Milbank Mem Fund Q, 1966.PMID 5338568
- [2]Reason J Human error: models and management BMJ, 2000.PMID 10720363
- [3]Leape LL Error in medicine JAMA, 1994.PMID 7503827
- [4]Berwick DM Continuous improvement as an ideal in health care N Engl J Med, 1989.PMID 2909878
- [5]Vincent C, Neale G, Woloshynowych M Adverse events in British hospitals: preliminary retrospective record review BMJ, 2001.PMID 11230064
- [6]Pronovost P, Needham D, Berenholtz S, et al. An intervention to decrease catheter-related bloodstream infections in the ICU N Engl J Med, 2006.PMID 17192537
- [7]Bowers L Safewards: a new model of conflict and containment on psychiatric wards J Psychiatr Ment Health Nurs, 2014.PMID 24548312
- [8]Bowers L, James K, Quirk A, et al. Reducing conflict and containment rates on acute psychiatric wards: The Safewards cluster randomised controlled trial Int J Nurs Stud, 2015.PMID 26166187
- [9]While D, Bickley H, Roscoe A, et al. Implementation of mental health service recommendations in England and Wales and suicide rates, 1997-2006: a cross-sectional before-and-after observational study Lancet, 2012.PMID 22305767
- [10]Appleby L, Shaw J, Amos T, et al. Suicide within 12 months of contact with mental health services: national clinical survey BMJ, 1999.PMID 10231250
- [11]Thibaut B, Dewa LH, Ramtale SC, et al. Patient safety in inpatient mental health settings: a systematic review BMJ Open, 2019.PMID 31874869
- [12]Silver SA, Harel Z, McQuillan R, et al. How to Begin a Quality Improvement Project Clin J Am Soc Nephrol, 2016.PMID 27016497
- [13]Grasso BC, Rothschild JM, Genest R, Bates DW What do we know about medication errors in inpatient psychiatry? Jt Comm J Qual Saf, 2003.PMID 12953603
- [14]Hunt IM, Windfuhr K, Shaw J, et al. Ligature points and ligature types used by psychiatric inpatients who die by hanging: a national study J Affect Disord, 2012.PMID 22343063