Psych · Public and community psychiatry — refugee and asylum seeker mental health
Refugee and asylum seeker mental health
Also known as Refugee psychiatry · Asylum seeker mental health · Forced displacement psychiatry · Torture survivor mental health · Immigration detention mental health · Post-migration living difficulties · Narrative exposure therapy NET · Unaccompanied refugee minors · Resettlement mental health
Exam-exhaustive fellowship reference on refugee and asylum seeker mental health — legal status versus diagnosis, pre/peri/post-migration determinants, epidemiology of PTSD and depression, detention and temporary protection harm, culturally safe assessment with interpreters, trauma-focused and WHO low-intensity interventions, pharmacotherapy adjuncts, and child/torture-survivor scenarios. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
This topic is high-yield for FRANZCP MEQs and CASC communication stations, MRCPsych cultural and trauma items, and ABPN public-mental-health blueprints. Examiners test definitions, named epidemiology papers, detention/temporary-protection evidence, interpreter skills, and whether candidates can treat both trauma memory and the living conditions that maintain distress.[3][6][16]
Overview and definition
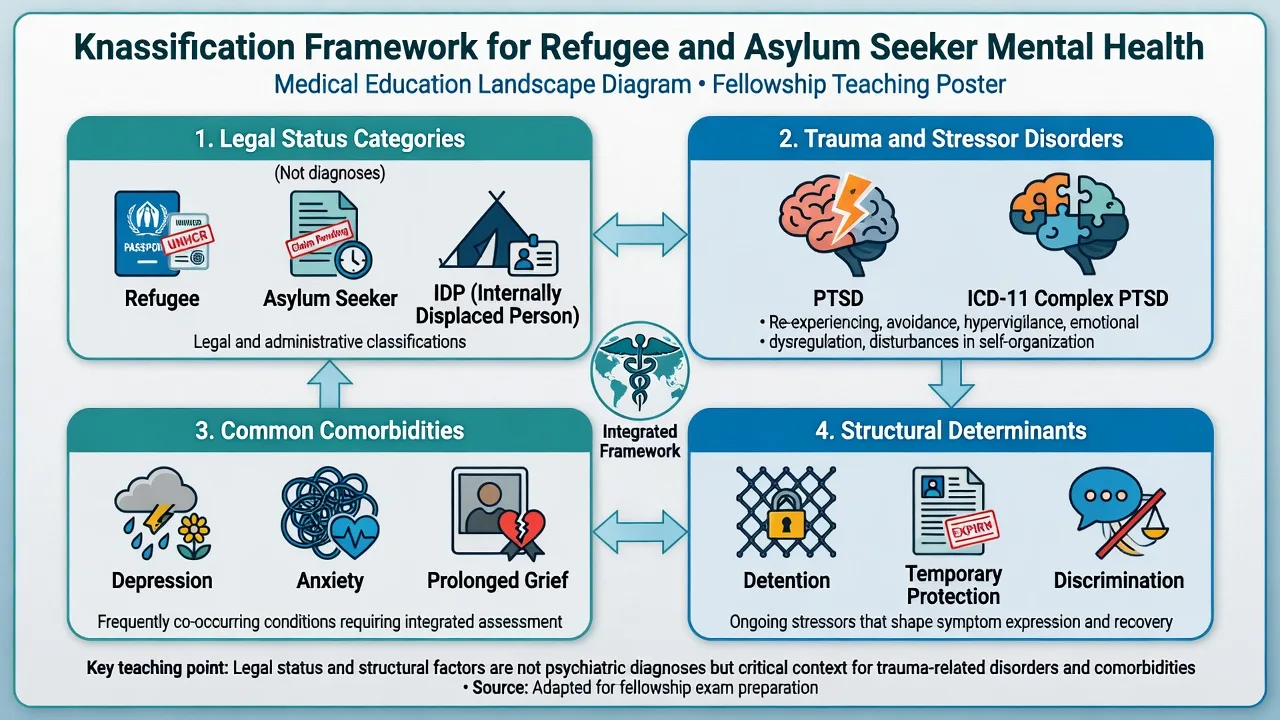
Refugee, asylum seeker, and internally displaced person (IDP) are legal and policy status categories, not psychiatric diagnoses. At the bedside, the clinical task is to assess symptoms, risk, capacity, and social determinants — not to adjudicate a protection claim. Forced displacement is associated with elevated psychiatric morbidity, but most displaced people do not meet criteria for PTSD, and resilience and recovery are common when safety and supports improve.[1][3]
Clinical framing. Think in three phases: pre-migration (war, persecution, torture, sexual violence), peri-migration (flight, trafficking risk, transit detention, separation), and post-migration living difficulties (PMLD) — visa uncertainty, detention, unemployment, language barriers, discrimination, housing instability, and family separation. PMLD are not "background noise"; they are active maintainers of morbidity after arrival.[12][4]
Nosology. Use DSM-5-TR PTSD (four clusters) or ICD-11 PTSD / complex PTSD when symptom structure fits, plus depressive, anxiety, prolonged grief, adjustment, and substance-related diagnoses as indicated. Complex PTSD (PTSD core plus disturbances of self-organisation) is particularly relevant after prolonged captivity or repeated interpersonal violence, including torture — diagnose by symptoms, not by refugee label alone.[2]
Classification
Refugee (policy sense)
- Recognised protection status
- Resettlement pathways vary by state
- Not a clinical syndrome
- Access still often fragmented
Asylum seeker
- Claim pending determination
- Prolonged uncertainty common
- Detention/TPV risk in some systems
- High PMLD burden
ICD-11 PTSD / CPTSD
- Symptom-structure diagnoses
- CPTSD adds DSO triad
- Typical after prolonged trauma
- Independent of visa label
PMLD maintainers
- Visa insecurity, detention
- Unemployment, language
- Racism and discrimination
- Treat as clinical targets
Epidemiology and risk factors
Headline epidemiology candidates must own
Landmark anchors. Fazel, Wheeler and Danesh (2005) synthesised data from thousands of resettled refugees in Western countries and reported substantially higher rates of PTSD and major depression than in host-population comparisons, with marked between-study heterogeneity — never quote a single false-precision percentage as "the" refugee rate.[1]
Steel and colleagues (2009) meta-analysed populations exposed to mass conflict and displacement and showed robust associations of torture and cumulative potentially traumatic events with PTSD and depression, supporting a dose-response conceptual model examiners love.[2]
Blackmore and colleagues (2020) updated prevalence estimates for refugees and asylum seekers with systematic review and meta-analysis methods, reinforcing high rates of PTSD, depression, and anxiety with continued heterogeneity by sample and measure.[3]
Detention and temporary protection (ANZ high-yield). Australian observational evidence links immigration detention and temporary protection visa status with worse mental health compared with more secure permanent pathways; Silove, Steel and Mollica framed detention as a human-rights and health assault with developmental consequences for communities.[4][5][6]
Children. Paired Lancet reviews map risk and protective factors for displaced children in high-income and low/middle-income settings; child-adolescent meta-analysis and unaccompanied minor (UAM) reviews show high psychiatric burden, especially with family separation and insecure care arrangements.[7][8][9][10]
Protective factors. Secure legal status, family reunification, social support, school engagement, meaningful activity, language access, and culturally safe services buffer risk — name these in viva answers, not only trauma lists.[7][12]
Pathophysiology and mechanisms
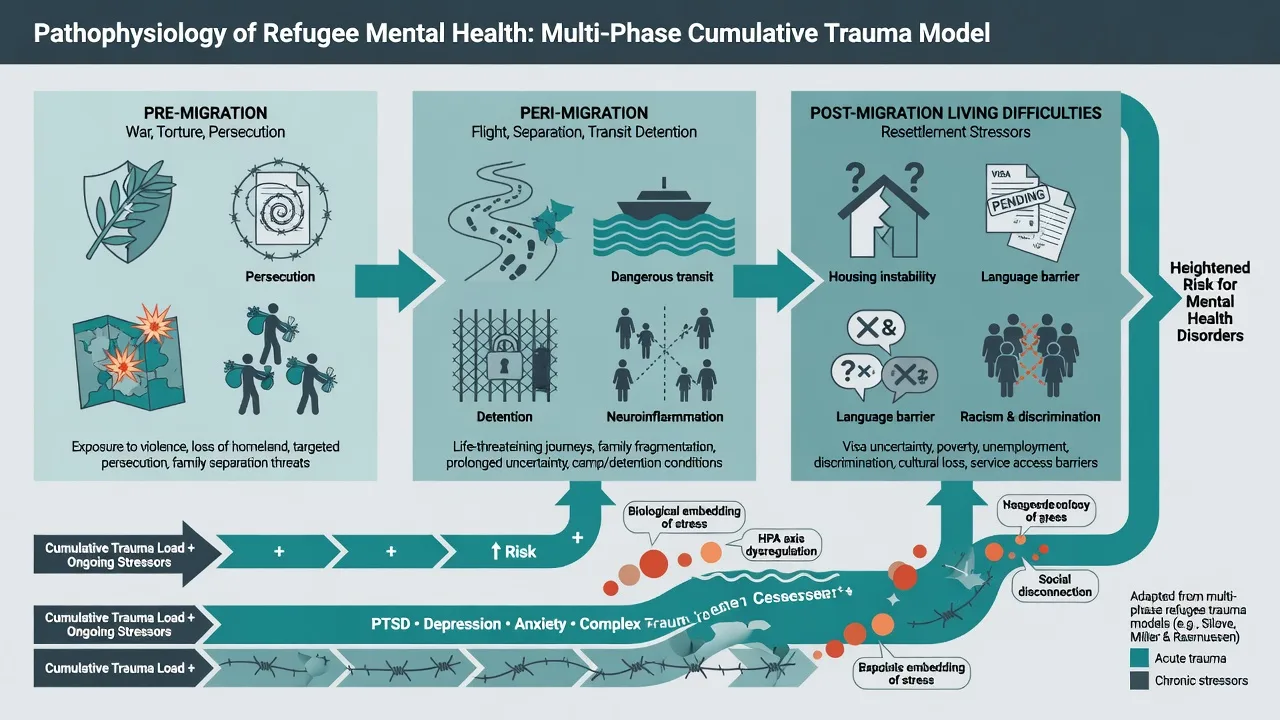
Multi-phase model. Pre-migration persecution and torture seed conditioned fear, shame, and grief. Peri-migration adds secondary trauma, unpredictability, and attachment disruption. Post-migration stressors maintain current threat appraisals — visa letters, detention reviews, racist encounters, and news of ongoing conflict can rekindle intrusion and hyperarousal even years later.[12][2]
Racism and xenophobia. Discrimination operates through structural exclusion and interpersonal hostility; mapped pathways link racism and xenophobia to adverse health outcomes and are clinically relevant to help-seeking, trust, and symptom load after resettlement.[22]
Symptom profiles. Population work in resettled refugees identifies distinctive psychological symptom profiles rather than a single "refugee syndrome," supporting individualised formulation over ethnic stereotyping.[13]
Long-term course. Systematic review of war-refugees years after conflict shows that elevated rates of PTSD, depression, and anxiety can persist long after resettlement when trauma load and ongoing adversity remain high.[11]
Clinical presentation
Classic adult vignette: adult with history of political detention and torture, now on a temporary or pending status, presenting with nightmares, hypervigilance, avoidance of police or uniforms, low mood, somatic pain, and despair tied to visa uncertainty. Quote the patient ("Every letter is a bomb"; "I am still in the cell when I sleep").[2][4]
MSE focus. Affect may be restricted, tearful, or irritable; thought content often includes trauma-linked guilt, foreshortened future, and immigration-related hopelessness; perception may include trauma flashbacks that must be distinguished from primary psychotic hallucinations; insight into the trauma link is often present; risk assessment is mandatory every contact with an interpreter when language is a barrier.[3]
Torture sequelae. Chronic pain, sexual dysfunction after sexual torture, head injury symptoms, and profound mistrust of authority figures — including health services — are clinical, not merely "cultural."[2][19]
Children and UAMs. Regression, sleep disturbance, school refusal, separation anxiety, behavioural dysregulation, and high rates of PTSD/depression/anxiety; unaccompanied minors face additional isolation, trafficking risk, and care-system strain.[7][9][10]
Differential diagnosis
| Discriminator | Favours trauma/PTSD-spectrum | Favours alternative |
|---|---|---|
| Intrusions linked to specific events, avoidance, hyperarousal | PTSD / CPTSD | Non-specific distress without trauma linkage |
| Ongoing visa/detention despair without full PTSD clusters | PMLD-driven depression / adjustment | Pure pre-migration PTSD alone |
| Pseudo-hallucinatory flashbacks vs novel psychotic percepts with thought disorder | Trauma-related | Primary psychosis / substance-induced |
| Spiritual or culturally sanctioned experiences | Cultural formulation first | Pathologising culture without distress/dysfunction |
| Cognitive change after head trauma | TBI work-up | "All psychological" assumption |
Also discriminate major depression, prolonged grief, substance-induced states, malingering concerns in medico-legal contexts (assess carefully without default disbelief), and organic causes including endocrine and infectious differentials when history indicates.[3]
Clinical and bedside assessment
Trauma-informed, culturally safe stance. Prioritise safety, trustworthiness, choice, collaboration, and cultural humility. Obtain enough detail to establish exposure and symptom linkage without forcing a graphic first-session retelling. Offer control over pacing, breaks, clinician gender preference, and who is in the room.[21]
Professional interpreters. Use trained interpreters for clinical content, risk, and consent. Brief the interpreter; speak in the first person; maintain eye contact with the patient; debrief if material is graphic. Never use children as interpreters. Family may provide collateral with consent but are not a substitute for professional language access when fluency is limited.[21]
Cultural formulation. Use DSM-5 Cultural Formulation Interview principles and Kleinman-style explanatory model questions: what the person calls the problem, what caused it, why now, what it does, how serious it is, what treatment helps, and who should be involved. CFI field-trial data support feasibility, acceptability, and clinical utility when used as a person-centred interview rather than checklist ethnography.[21]
Risk. Suicide, self-harm, violence, vulnerability to exploitation/trafficking/IPV, and child protection. Collaborative safety planning with means restriction and clear follow-up. Capacity is decision-specific. Involuntary care uses local Mental Health Act principles — least restrictive; do not invent section numbers for the wrong jurisdiction.[3]
Measures. Harvard Trauma Questionnaire lineage instruments measure torture/trauma exposure and PTSD-related symptoms in refugee research traditions; PCL-5 supports severity monitoring with language-validation caution; interpret cut-offs carefully across translations.[19]
Investigations
There is no refugee-specific diagnostic biomarker. Investigate to exclude mimics and prepare for medication: TSH, FBC, U&E, LFT as indicated; ECG when cardiac risk; pregnancy test when relevant; urine drug screen when substance contribution is plausible; neuroimaging only with neurological red flags (including possible TBI after torture or blast). Document legal, housing, and language needs as formulation data, not only lab results.[2][19]
Management — acute / resuscitation
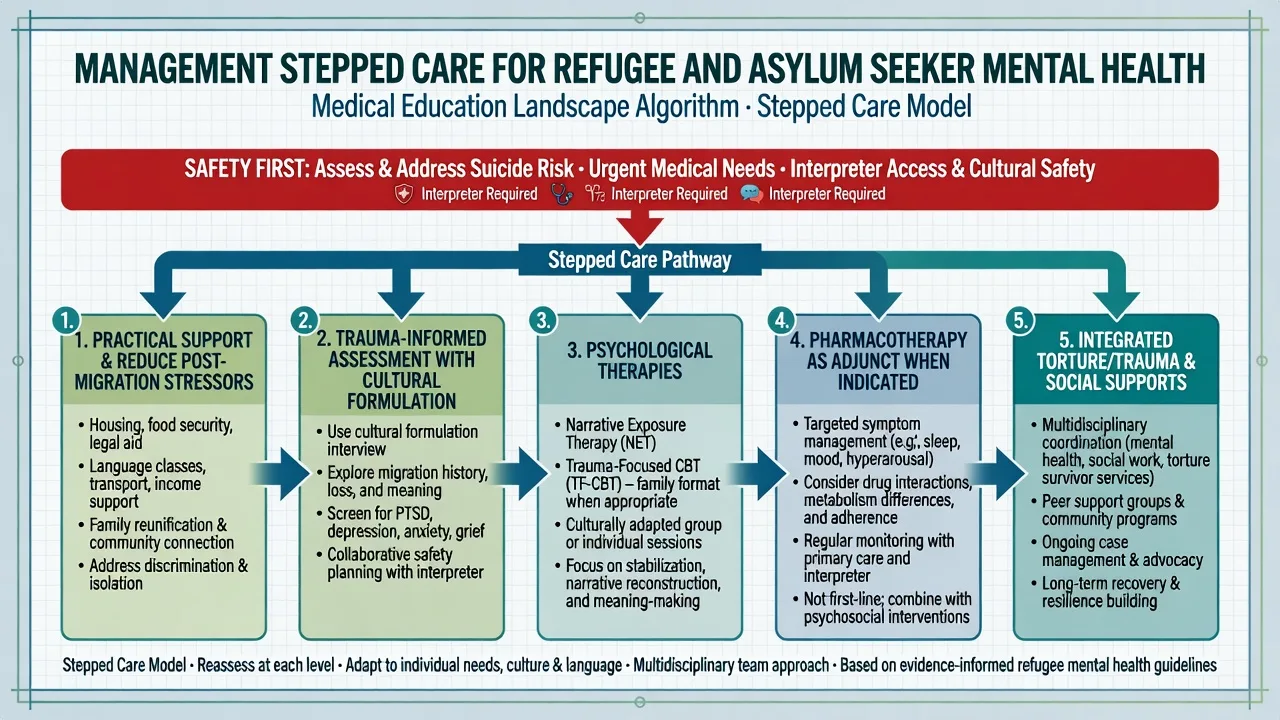
Immediate priorities. Physical safety, medical needs, interpreter access, and psychological first-aid principles (calm information, contact restoration, practical support). Avoid mandatory single-session debriefing of all arrivals as universal prevention. Manage acute suicidality and agitation through usual pathways while minimising retraumatising coercion where safe alternatives exist.[3][6]
Management — definitive and stepwise
Treat trauma and treat living conditions
Evidence reviews consistently show that post-migration stress is associated with psychological disorders independent of — and interacting with — past trauma. Clinical plans that only "process memories" while ignoring housing, legal advocacy pathways, language, work rights, and racism miss major maintainers of illness.[12][4]
Psychological therapies
Narrative exposure therapy (NET). Foundational RCT evidence in an African refugee settlement compared NET with supportive counselling and psychoeducation for PTSD; NET produced greater PTSD symptom improvement, establishing a named, examiner-friendly trauma-focused option for multiple-trauma refugee presentations.[14]
Broader psychosocial evidence. Systematic reviews of PTSD treatments in refugees and asylum seekers support trauma-focused approaches with methodological caveats; network meta-analyses of psychosocial interventions for refugees/asylum seekers with PTSD, and updated comparative network meta-analyses across PTSD, depression, and anxiety in migrant populations, guide choice among available modalities when access and language allow.[15][16][17]
Scalable WHO-informed care. A randomised trial of a WHO self-help psychological intervention among Syrian refugees in Turkey demonstrated preventive benefit for mental disorders, supporting stepped-care interest in low-intensity, scalable options alongside specialist trauma therapy for severe illness.[18]
Pharmacotherapy — agent, dose, monitoring
Medication does not replace trauma-focused psychological treatment when that treatment is available and acceptable. When chosen (preference, limited therapy access, severe comorbid depression/anxiety, partial response), sertraline has RCT support for PTSD symptoms in general adult populations and is commonly used as an adjunct in trauma clinics.[20]
| Agent | Typical adult start | Common range | Monitoring notes |
|---|---|---|---|
| Sertraline | 25–50 mg orally daily | 50–200 mg daily | Sexual dysfunction, GI effects; early review for activation/suicidality; use interpreter for side-effect education |
| Other SSRI/SNRI options | Per PTSD/depression protocols | Individualise | Same metabolic/interaction cautions as host-population prescribing |
Avoid reflexive long-term benzodiazepines for core trauma symptoms (dependence risk; interference with extinction learning). Titrate slowly when somatic hypervigilance is high; check pregnancy status and drug interactions; document shared decision-making with interpreter-mediated consent.[20]
Integrated and service-level care
Torture and trauma services (specialist multidisciplinary models), primary-care collaborative care, school liaison for children, peer/community supports, and legal/housing advocacy partners form the real system of care. Cultural adaptation should preserve active therapeutic ingredients rather than dilute them into unsupported "cultural counselling" alone.[15][16][21]
ANZ: Detention and temporary protection literature is high-yield; know Steel/Momartin/Silove anchors; engage local torture/trauma services and interpreter systems. UK/Europe: Asylum process length and UAM pathways often drive presentations; NICE trauma principles still apply with cultural adaptation. US/Canada: Refugee resettlement and asylum tracks differ; APA trauma-informed and cultural psychiatry principles apply — do not invent statute section numbers. Global South: Most displaced people live in low/middle-income settings (Reed/Fazel child review); resource-adapted and WHO-informed interventions are particularly relevant.[4][5][8][18]
Subtypes and clinical scenarios
- Permanent resettlement: focus on integration, residual PTSD/depression, family systems, and long-term morbidity risk.[11][13]
- Protracted asylum process: PMLD-dominant despair; legal uncertainty as ongoing threat cue.[12]
- Detention / TPV: expect higher symptom burden; advocacy and status security are clinical levers.[4][5]
- Torture survivors: integrated pain, sexual health, TBI, and trauma psychology care.[2][19]
- Children / UAMs: developmental assessment, school, safeguarding, caregiver mental health.[7][10]
- Perinatal refugee care: screen mood/anxiety/PTSD with interpreter; safeguarding and attachment supports.
- Medico-legal interface: clear dual-role ethics; clinical care is not the same as writing a protection-claim report unless instructed and competent.
Complications and pitfalls
Stereotyping ("all refugees have PTSD"); using child interpreters; ignoring PMLD; pathologising political grief or spiritual practice; missing organic disease; undertreating because of "resilience" narratives or access barriers; overusing benzodiazepines; forcing graphic disclosure for paperwork; inventing immigration law sections in exams; equating language fluency with cultural safety.[12][21][22]
Prognosis and disposition
Many people improve substantially when legal status secures, family reunifies, and evidence-based care is delivered. Long-term reviews show that elevated psychiatric morbidity can persist in war-refugee cohorts, so disposition must plan continuity rather than single-session crisis only.[11][3]
Step-up for high suicide risk, psychosis, severe dissociation with self-neglect, unsafe housing/detention crisis, or failed outpatient engagement. Step-down when risk is managed, symptoms improve on measurement, and social supports are stable. Follow-up intensity tracks risk and PMLD, not ethnicity.[4][16]
Special populations
Children and adolescents; unaccompanied minors; women survivors of sexual and gender-based violence; LGBTQIA+ people fleeing persecution; older adults with cumulative loss; people with disability needing communication supports; perinatal patients; dual cultural formulation when Indigenous host-community intersections arise.[7][9][10][21]
Evidence and guidelines
Anchor answers to named papers: Fazel 2005; Steel 2009; Blackmore 2020; Steel/Momartin detention-TPV; Fazel/Reed child pair; Bogic long-term; Li/Nickerson PMLD; Neuner NET; Crumlish and Turrini treatment syntheses; Acarturk WHO self-help; HTQ; CFI; Selvarajah racism pathways. Know that RANZCP, NICE, and APA trauma and cultural frameworks inform practice — cite principles, not invented page numbers.[1][2][3][14][16][17][18][22]
Exam pearls
REFUGEE care checklist
References
- [1]Fazel M, Wheeler J, Danesh J Prevalence of serious mental disorder in 7000 refugees resettled in western countries: a systematic review Lancet, 2005.PMID 15823380
- [2]Steel Z, Chey T, Silove D, Marnane C, et al. Association of torture and other potentially traumatic events with mental health outcomes among populations exposed to mass conflict and displacement: a systematic review and meta-analysis JAMA, 2009.PMID 19654388
- [3]Blackmore R, Boyle JA, Fazel M, Ranasinha S, et al. The prevalence of mental illness in refugees and asylum seekers: A systematic review and meta-analysis PLoS Med, 2020.PMID 32956381
- [4]Steel Z, Silove D, Brooks R, Momartin S, et al. Impact of immigration detention and temporary protection on the mental health of refugees Br J Psychiatry, 2006.PMID 16388071
- [5]Momartin S, Steel Z, Coello M, Aroche J, et al. A comparison of the mental health of refugees with temporary versus permanent protection visas Med J Aust, 2006.PMID 17014402
- [6]Silove D, Steel Z, Mollica R Detention of asylum seekers: assault on health, human rights, and social development Lancet, 2001.PMID 11356469
- [7]Fazel M, Reed RV, Panter-Brick C, Stein A Mental health of displaced and refugee children resettled in high-income countries: risk and protective factors Lancet, 2012.PMID 21835459
- [8]Reed RV, Fazel M, Jones L, Panter-Brick C, Stein A Mental health of displaced and refugee children resettled in low-income and middle-income countries: risk and protective factors Lancet, 2012.PMID 21835460
- [9]Blackmore R, Gray KM, Boyle JA, Fazel M, et al. Systematic Review and Meta-analysis: The Prevalence of Mental Illness in Child and Adolescent Refugees and Asylum Seekers J Am Acad Child Adolesc Psychiatry, 2020.PMID 31778780
- [10]Daniel-Calveras A, Baldaquí N, Baeza I Mental health of unaccompanied refugee minors in Europe: A systematic review Child Abuse Negl, 2022.PMID 36095862
- [11]Bogic M, Njoku A, Priebe S Long-term mental health of war-refugees: a systematic literature review BMC Int Health Hum Rights, 2015.PMID 26510473
- [12]Li SS, Liddell BJ, Nickerson A The Relationship Between Post-Migration Stress and Psychological Disorders in Refugees and Asylum Seekers Curr Psychiatry Rep, 2016.PMID 27436307
- [13]Nickerson A, Hadzi-Pavlovic D, Edwards B, O'Donnell M, et al. Identifying distinctive psychological symptom profiles among a nationally representative sample of refugees resettled in Australia Aust N Z J Psychiatry, 2019.PMID 31032626
- [14]Neuner F, Schauer M, Klaschik C, Karunakara U, Elbert T A comparison of narrative exposure therapy, supportive counseling, and psychoeducation for treating posttraumatic stress disorder in an African refugee settlement J Consult Clin Psychol, 2004.PMID 15301642
- [15]Crumlish N, O'Rourke K A systematic review of treatments for post-traumatic stress disorder among refugees and asylum-seekers J Nerv Ment Dis, 2010.PMID 20386252
- [16]Turrini G, Tedeschi F, Cuijpers P, Del Giovane C, et al. A network meta-analysis of psychosocial interventions for refugees and asylum seekers with PTSD BMJ Glob Health, 2021.PMID 34088735
- [17]Turrini G, Purgato M, Cadorin C, Bartucz M, et al. Comparative efficacy and acceptability of psychosocial interventions for PTSD, depression, and anxiety in asylum seekers, refugees, and other migrant populations: a systematic review and network meta-analysis Lancet Reg Health Eur, 2025.PMID 39687671
- [18]Acarturk C, Uygun E, Ilkkursun Z, Carswell K, et al. Effectiveness of a WHO self-help psychological intervention for preventing mental disorders among Syrian refugees in Turkey: a randomized controlled trial World Psychiatry, 2022.PMID 35015365
- [19]Mollica RF, Caspi-Yavin Y, Bollini P, Truong T, et al. The Harvard Trauma Questionnaire. Validating a cross-cultural instrument for measuring torture, trauma, and posttraumatic stress disorder in Indochinese refugees J Nerv Ment Dis, 1992.PMID 1737972
- [20]Brady K, Pearlstein T, Asnis GM, Baker D, et al. Efficacy and safety of sertraline treatment of posttraumatic stress disorder: a randomized controlled trial JAMA, 2000.PMID 10770145
- [21]Lewis-Fernández R, Aggarwal NK, Lam PC, Galfalvy H, et al. Feasibility, acceptability and clinical utility of the Cultural Formulation Interview: mixed-methods results from the DSM-5 international field trial Br J Psychiatry, 2017.PMID 28104738
- [22]Selvarajah S, Corona Maioli S, Deivanayagam TA, et al. Racism, xenophobia, and discrimination: mapping pathways to health outcomes Lancet, 2022.PMID 36502849