Psych · Public and community psychiatry — rehabilitation and recovery services
Psychiatric rehabilitation and recovery services
Also known as Psychosocial rehabilitation · Psychiatric rehabilitation · Recovery-oriented services · Individual Placement and Support IPS · Supported employment mental illness · Assertive Community Treatment ACT · Intensive case management · Housing First mental health · Clubhouse model · Community mental health rehabilitation
Exam-exhaustive fellowship topic on psychiatric rehabilitation and recovery services: clinical, functional and personal recovery (CHIME); evidence-based packages including ACT/ICM, IPS supported employment, Housing First, family psychoeducation, IMR, cognitive remediation, peer support and Clubhouse; fidelity, stepped intensity and recovery-oriented service design. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags

Definition and classification
What psychiatric rehabilitation is
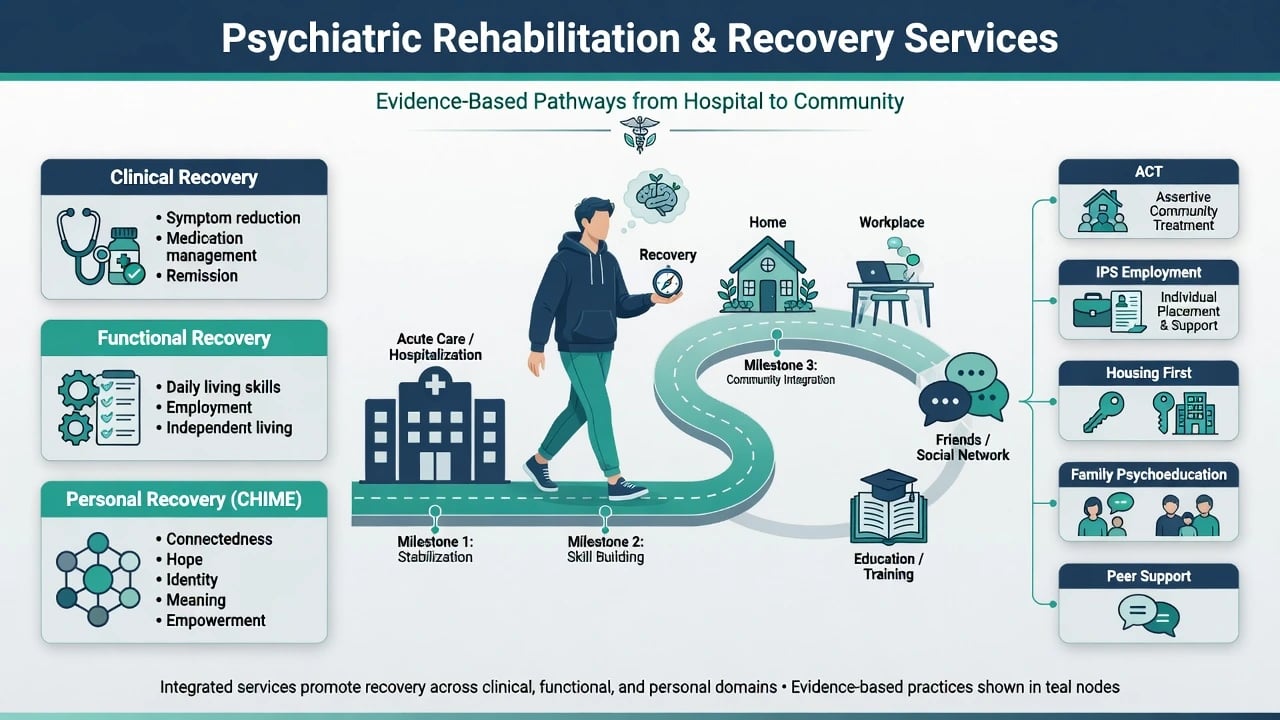
Psychiatric (psychosocial) rehabilitation is a set of coordinated interventions that reduce disability and enable valued social roles for people with SMI. It addresses skills, supports, environments and opportunity structures — not symptoms alone. Acute pharmacotherapy and crisis care are necessary but not sufficient for community tenure and citizenship.[4][12]
Three recovery constructs examiners test
| Construct | Focus | Typical metrics | Exam trap |
|---|---|---|---|
| Clinical recovery | Symptoms, relapse, insight | CGI, PANSS-type scores, hospital days | Treating scores as the only goal |
| Functional recovery | Work, study, housing, ADLs, relationships | Employment rate, independent living | Assuming function follows symptoms automatically |
| Personal recovery | Person-defined meaningful life | CHIME domains, goal attainment | Using "recovery" as KPI for premature discharge |
Examiners expect these three constructs to be named separately because they can diverge in the same person.[10][11]
CHIME (Leamy and colleagues): Connectedness, Hope, Identity, Meaning, Empowerment.[10] Recovery-oriented practice guidance emphasises hope, partnership, strengths and community inclusion.[12] Slade and colleagues warn of uses and abuses of recovery — including using recovery rhetoric to deny evidence-based care or force premature discharge.[11]
Core service models (taxonomy)
| Model | Core idea | Primary target | Main outcome signal |
|---|---|---|---|
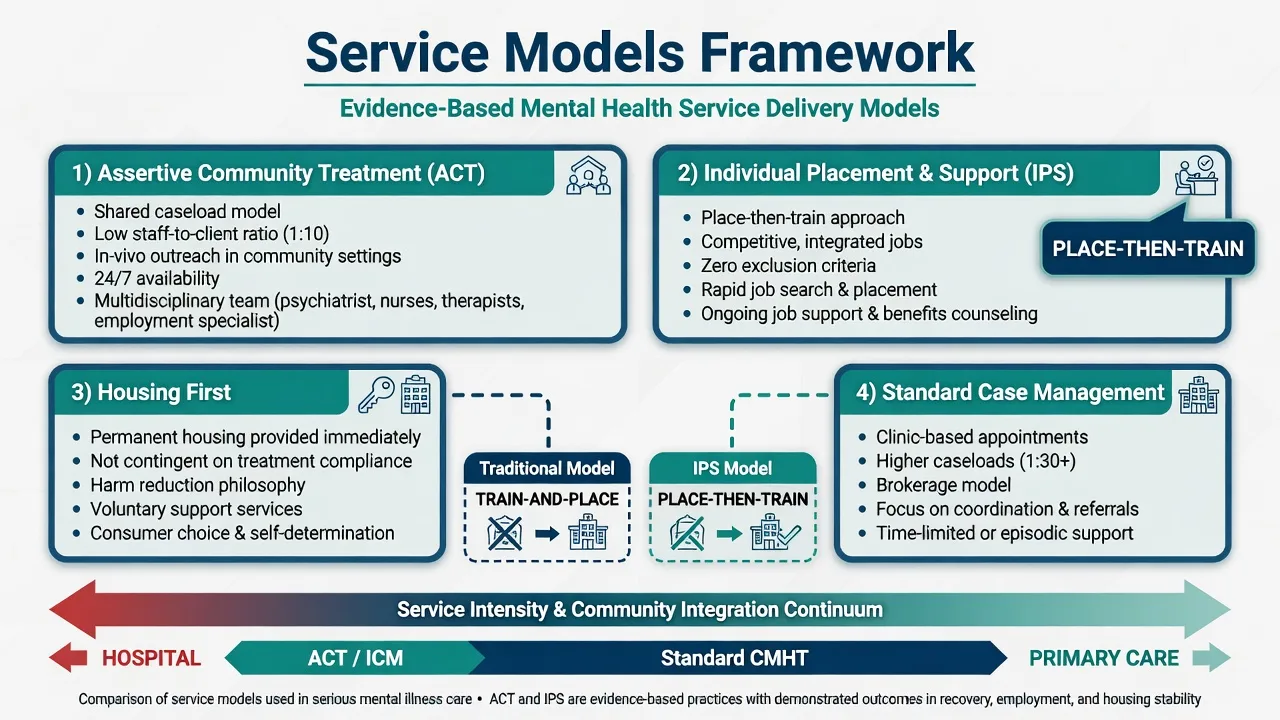
| ACT / PACT | Shared multidisciplinary caseload, low ratio, in-vivo, high intensity, fixed responsibility | Hard-to-engage, high hospital users with SMI | Engagement, reduced hospital use |
| Intensive case management (ICM) | Higher intensity than standard CM; continuum with ACT-like features when fidelity high | Similar high-need groups | Hospital days, contact continuity |
| Standard CMHT / case management | Clinic-based, higher caseloads, lower outreach | Stable, engaged patients | Maintenance care |
| IPS supported employment | Place-then-train; competitive jobs; zero exclusion; integrated MH + vocational staff | People with SMI who want work | Competitive employment |
| Traditional vocational rehab | Train-and-place; prolonged pre-vocational readiness | Often selected "ready" clients | Delayed competitive work |
| Housing First | Permanent housing without treatment preconditions + support | Homeless SMI / dual diagnosis | Housing stability |
| Continuum / treatment-first housing | Housing contingent on compliance / sobriety steps | Same populations historically | More housing loss if rules fail |
| Family psychoeducation | Structured education, communication, problem-solving, EE reduction | Families of people with schizophrenia/SMI | Relapse reduction |
| IMR | Illness management skills + recovery goals | SMI needing self-management | Knowledge, coping, goal work |
| Cognitive remediation | Practice-based cognitive training ± strategy coaching | Cognitive barriers to function | Cognition and functioning |
| Peer support | Lived-experience roles for hope, navigation, engagement | Broad SMI | Engagement, hope (role-quality dependent) |
| Clubhouse | Membership community, work-ordered day, transitional employment pathways | SMI seeking community/work identity | QoL, employment, hospital use (mixed designs) |
Epidemiology and service need
People with SMI experience high rates of unemployment, under-employment, social isolation and premature mortality from physical disease. Competitive employment remains low in many systems despite preference for work among a substantial minority to majority of service users — a central public-health and rights gap that IPS was designed to close.[5][8]
Homelessness and housing instability concentrate among people with SMI and co-occurring substance use. Housing First trials in dual diagnosis populations demonstrate that permanent housing with support can be achieved without requiring sobriety or treatment compliance as a precondition.[9]
"Revolving door" hospitalisation clusters with disengagement, substance use, homelessness, inadequate community intensity and fragmented responsibility. ACT and ICM were developed to provide a fixed point of responsibility and intensive outreach for these groups.[1][2][3]
Mechanisms — why rehabilitation works
Disability in SMI is multi-determined: positive symptoms, negative symptoms, cognitive deficits, skill gaps, self-stigma, family environment (including high expressed emotion), poverty and opportunity barriers interact. Treating symptoms alone often leaves role disability intact.[4][15]
Place-then-train (IPS) assumes competitive work is learned best in real jobs with ongoing support, rather than after lengthy sheltered training. Zero exclusion rejects cream-skimming of only "work-ready" clients.[5][8]
In-vivo care (ACT) assumes skills and engagement generalise poorly from office appointments alone; outreach to homes, streets and workplaces delivers support where disability is lived.[1][2]
Housing First treats housing as a platform for recovery and harm reduction, not a reward for compliance — reducing the instability that undermines every other intervention.[9]
CHIME processes (hope, identity reconstruction, connectedness) mediate personal recovery beyond clinician-rated symptoms.[10]
Clinical presentation and exam stems
Classic stems include the revolving-door patient with multiple admissions and DNA clinic attendances; the person with residual schizophrenia who wants paid work but is offered only pre-vocational groups; dual diagnosis homelessness; family high EE after discharge; FEP packages with integrated supported employment/education; and service rhetoric of "recovery" used to justify early discharge without housing or follow-up intensity.[1][6][11][16]
Bedside discrimination: amotivation from negative symptoms versus skill deficit versus lack of opportunity versus sedation side-effects blocking work. Medication decisions should be shared against person-defined goals (for example, morning sedation vs apprenticeship).[18]
Differential distinctions
| Compare | Discriminator |
|---|---|
| IPS vs train-and-place | Rapid competitive placement + ongoing support vs prolonged readiness training; superior competitive employment for IPS |
| ACT vs standard CMHT | Shared caseload, low ratio (~1:10 classically), in-vivo, 24/7 capability, high contact frequency vs clinic model |
| ACT vs any "outreach nurse" | Critical ingredients and fidelity, not branding |
| Housing First vs treatment-first | Housing not contingent on sobriety/treatment compliance |
| Personal vs clinical recovery | Person-defined meaningful life vs symptom scores alone |
| Recovery-oriented care vs under-treatment | Partnership + EBPs + hope vs denial of care under recovery rhetoric |
| Peer support vs case management | Complementary lived-experience role; does not replace medical risk responsibility |
Assessment — map function and goals
Structure assessment as a multi-domain functional and recovery map rather than a symptom checklist alone.[4][10]
- Person-defined goals (work, study, housing, relationships, meaning) using CHIME language without abandoning risk assessment.[10]
- Functional domains — housing stability, ADLs/IADLs, finances/benefits, social network, education/work history and preferences, community participation, physical health.[4]
- Clinical barriers — residual positive symptoms, negative symptoms, cognition, substance use, side-effects, comorbidity.[4][15]
- Engagement and intensity fit — DNAs, crisis use, need for ACT/ICM vs standard care.[2][3]
- Vocational IPS screen — primary eligibility is desire to work, not a battery that excludes people as "not ready".[5][8]
- Family — EE, knowledge, carer burden, psychoeducation readiness.[14]
- Legal/status and capacity principles — jurisdiction-specific; no invented statute numbers.
Investigations and service evaluation
There is no laboratory test for rehabilitation need; investigation means service, function and fidelity mapping alongside routine physical health care for SMI.[2][4]
- Map current service intensity, DNAs, hospital days, housing status.[3]
- Screen physical health (metabolic, cardiovascular) as part of SMI care while rehab proceeds.[4]
- Consider cognitive assessment when remediation is contemplated.[15]
- Evaluate program fidelity conceptually (IPS principles; ACT critical ingredients) rather than inventing local accreditation codes.[2][5]
- Track outcomes that matter: competitive employment, education enrolment, housing stability, hospital days, goal attainment, personal recovery domains — not CGI alone.[4][10]
Acute and crisis interface
Rehabilitation does not replace emergency psychiatry. Suicidality, violence risk, catatonia, NMS, severe self-neglect and medical instability take priority. After stabilisation, disposition must include housing and intensity planning — "discharge to community" without a package is a systems failure, not recovery-oriented care.[11]
Definitive management — build the package
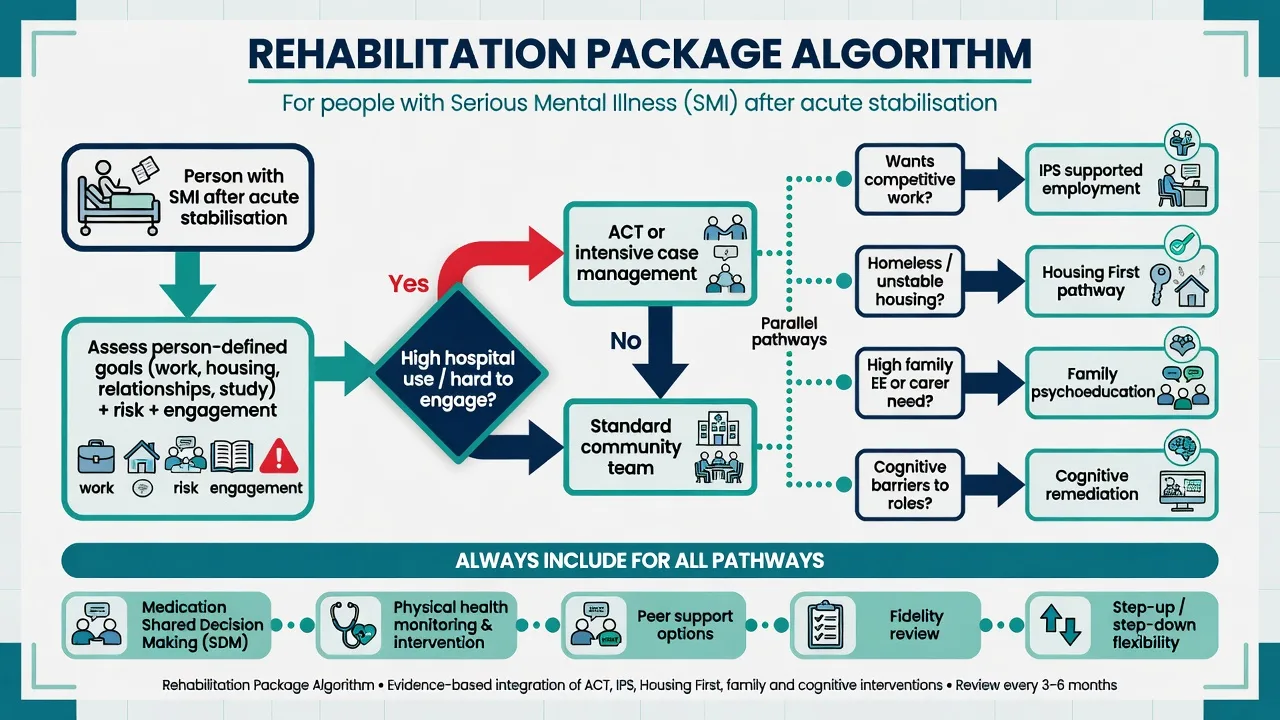
1. Match intensity of community care
- ACT: multidisciplinary shared caseload, low client-to-staff ratios, services in vivo, high contact frequency, time-unlimited continuous care, 24-hour responsibility as designed, focus on hard-to-engage high users. Foundational Stein and Test model; Bond and Drake summarise critical ingredients and warn that diluted models underperform.[1][2]
- ICM: Cochrane synthesis shows intensive case management reduces hospitalisation and increases retention in care compared with standard care, with effects related to baseline hospital use and model features overlapping ACT when intensive.[3]
- Step-down to standard CMHT when engagement and stability allow; step-up when revolving door returns.
2. IPS supported employment (if competitive work is a goal)
Core IPS principles examiners expect: competitive employment as the goal; zero exclusion; rapid job search (place-then-train); attention to client preferences; integrated mental health and employment services; benefits counselling; time-unlimited follow-along support; systematic job development.[5]
Evidence: multiple RCTs show IPS superiority over traditional vocational approaches; European EQOLISE trial extended effectiveness beyond the US; non-US generalizability reviews support international use; meta-analysis finds roughly doubled odds of competitive employment versus controls.[5][6][7][8]
3. Housing First (if homeless / unstable housing)
Provide permanent independent housing with support and consumer choice, without requiring sobriety or treatment compliance first. RCT evidence in dual diagnosis homelessness shows superior housing stability without compromising psychiatric or substance outcomes on average versus continuum models.[9]
4. Family psychoeducation
Structured multi-session programs reduce relapse and rehospitalisation for schizophrenia-spectrum illness; address EE, communication and problem-solving; single- and multi-family formats exist.[4][14]
5. Illness management and recovery (IMR) and psychoeducation
IMR packages psychoeducation, behavioural tailoring for medication, relapse prevention, coping skills and recovery goal setting — bridging clinical self-management with personal recovery.[13]
6. Cognitive remediation
Meta-analysis shows durable small-to-moderate effects on global cognition and functioning in schizophrenia; best framed as part of a functional package, not a standalone cure.[15]
7. Peer support and Clubhouse / recovery education
Peer support can improve engagement, hope and practical navigation when roles are real (pay, supervision, integration) rather than token.[17] Clubhouse and recovery-college models provide community, identity and work-ordered structure as complementary options; competitive employment outcomes still often best served by IPS when work is the goal.[4][5]
8. Medication within recovery goals (SDM)
Shared decision-making links formulation choice, dosing schedule and side-effect trade-offs to roles (work, parenting, study). Recovery-oriented medication management is partnership, not forced concordance theatre.[18]
9. PORT-aligned psychosocial bundle
Schizophrenia PORT psychosocial recommendations endorse supported employment, family interventions, ACT for appropriate populations, skills training and related EBPs — a standard checklist for exam answers on comprehensive SMI care.[4]
10. First-episode coordinated specialty care
RAISE Early Treatment Program (NAVIGATE-type comprehensive care including medication, family psychoeducation, individual resiliency training, supported employment/education) improved outcomes versus usual community care over two years — exam anchor for early multi-component rehab.[16]
Subtypes and scenarios
- FEP / youth: early IPS/education support; coordinated specialty care reduces duration of untreated functional loss.[16]
- Long-term schizophrenia with negative/cognitive disability: combine optimised antipsychotics, remediation, skills training, IPS if work-interested, family PE.[4][15]
- Dual diagnosis homelessness: Housing First + integrated substance and mental health support; harm-reduction stance compatible with housing stability goals.[9]
- High EE family system: family psychoeducation, not blame.[14]
- Rural/low-resource: flexible assertive outreach / hybrid tele-enabled models; preserve principles (continuity, outreach, fixed responsibility) even if classic ACT staffing is unavailable.[2][3]
- Forensic interface: dual stigma, housing barriers, need for clear risk plans alongside rehab goals.
- Indigenous and culturally diverse: culturally safe community supports; recovery meanings may include kinship and land connection — do not impose a single Western metric of "independence".
Complications and pitfalls
- Recovery KPI culture that pressures unsafe discharge.[11]
- Branding low-intensity clinic care as "ACT".[2]
- Endless pre-vocational training without competitive job access.[5]
- Treatment-contingent housing that recreates homelessness after any lapse.[9]
- Ignoring metabolic and physical health while celebrating "roles only".
- Token peer workers without power or pay equity.[17]
- Fragmented multi-agency care with no fixed clinical responsibility.[1][2]
Prognosis and disposition
| Package | Best-supported effect | Disposition note |
|---|---|---|
| IPS | Competitive employment ~2× controls | Continue time-unlimited support after job start |
| ACT/ICM | Less hospital use, better engagement | Step-down when stable; re-intensify if revolving door returns |
| Housing First | Housing stability | Do not make housing contingent on perfect adherence |
| Family PE | Relapse reduction | Engage early post-discharge |
| Cognitive remediation | Cognition/function gains | Pair with real-world practice |
| RAISE-type CSC | Better early FEP outcomes vs usual care | Do not wait for "chronicity" before rehab |
Personal recovery is non-linear. Measure what the person values as well as hospital days.[10][11]
Special populations
Youth and FEP; older adults (therapeutic nihilism is structural stigma); perinatal role supports; intellectual disability dual diagnosis (adapted rehab); forensic dual stigma; rural access; culturally diverse recovery concepts. Same model principles, adapted delivery.[11][16]
Evidence and regional deltas
Landmarks to name: Stein and Test ACT; Bond/Drake ACT ingredients; Dieterich ICM Cochrane; Dixon PORT psychosocial; Bond IPS RCT synthesis; Burns EQOLISE; Bond non-US IPS generalizability; Modini IPS meta-analysis; Tsemberis Housing First; Leamy CHIME; Slade uses/abuses; Mueser IMR; McFarlane family PE; Wykes remediation; Kane RAISE; Davidson peer support; Deegan/Drake SDM.[1][2][3][4][5][6][8][9][10][11][16]
Exam pearls
- Name clinical / functional / personal recovery and CHIME in any recovery stem.[10]
- IPS = place-then-train; desire to work is eligibility; ~2× competitive employment.[5][8]
- ACT ingredients: shared caseload, low ratio, in vivo, intensity, fixed responsibility — fidelity or it is not ACT.[2]
- Housing First ≠ treatment-first continuum.[9]
- PORT psychosocial checklist for schizophrenia rehab answers.[4]
- Recovery language never cancels risk care or EBPs.[11]
- FEP: multi-component CSC including employment/education support early.[16]
- SDM links medication side-effects to work and life goals.[18]
References
- [1]Stein LI, Test MA Alternative to mental hospital treatment. I. Conceptual model, treatment program, and clinical evaluation Arch Gen Psychiatry, 1980.PMID 7362425
- [2]Bond GR, Drake RE The critical ingredients of assertive community treatment World Psychiatry, 2015.PMID 26043344
- [3]Dieterich M, Irving CB, Bergman H, et al. Intensive case management for severe mental illness Cochrane Database Syst Rev, 2017.PMID 28067944
- [4]Dixon LB, Dickerson F, Bellack AS, et al. The 2009 schizophrenia PORT psychosocial treatment recommendations and summary statements Schizophr Bull, 2010.PMID 19955389
- [5]Bond GR, Drake RE, Becker DR An update on randomized controlled trials of evidence-based supported employment Psychiatr Rehabil J, 2008.PMID 18407876
- [6]Burns T, Catty J, Becker T, et al. The effectiveness of supported employment for people with severe mental illness: a randomised controlled trial Lancet, 2007.PMID 17905167
- [7]Bond GR, Drake RE, Becker DR Generalizability of the Individual Placement and Support (IPS) model of supported employment outside the US World Psychiatry, 2012.PMID 22295007
- [8]Modini M, Tan L, Brinchmann B, et al. Supported employment for people with severe mental illness: systematic review and meta-analysis of the international evidence Br J Psychiatry, 2016.PMID 27103678
- [9]Tsemberis S, Gulcur L, Nakae M Housing First, consumer choice, and harm reduction for homeless individuals with a dual diagnosis Am J Public Health, 2004.PMID 15054020
- [10]Leamy M, Bird V, Le Boutillier C, et al. Conceptual framework for personal recovery in mental health: systematic review and narrative synthesis Br J Psychiatry, 2011.PMID 22130746
- [11]Slade M, Amering M, Farkas M, et al. Uses and abuses of recovery: implementing recovery-oriented practices in mental health systems World Psychiatry, 2014.PMID 24497237
- [12]Le Boutillier C, Leamy M, Bird VJ, et al. What does recovery mean in practice? A qualitative analysis of international recovery-oriented practice guidance Psychiatr Serv, 2011.PMID 22193795
- [13]Mueser KT, Corrigan PW, Hilton DW, et al. Illness management and recovery: a review of the research Psychiatr Serv, 2002.PMID 12364675
- [14]McFarlane WR, Dixon L, Lukens E, et al. Family psychoeducation and schizophrenia: a review of the literature J Marital Fam Ther, 2003.PMID 12728780
- [15]Wykes T, Huddy V, Cellard C, et al. A meta-analysis of cognitive remediation for schizophrenia: methodology and effect sizes Am J Psychiatry, 2011.PMID 21406461
- [16]Kane JM, Robinson DG, Schooler NR, et al. Comprehensive Versus Usual Community Care for First-Episode Psychosis: 2-Year Outcomes From the NIMH RAISE Early Treatment Program Am J Psychiatry, 2016.PMID 26481174
- [17]Davidson L, Bellamy C, Guy K, et al. Peer support among persons with severe mental illnesses: a review of evidence and experience World Psychiatry, 2012.PMID 22654945
- [18]Deegan PE, Drake RE Shared decision making and medication management in the recovery process Psychiatr Serv, 2006.PMID 17085613