Psych · public-community
Rural and remote psychiatry
Also known as Rural mental health · Remote psychiatry · Telepsychiatry rural · Hub-and-spoke psychiatry · Fly-in fly-out psychiatry · FIFO psychiatry · Regional mental health services · Modified Monash Model mental health · Telemental health rural
Exam-exhaustive fellowship reference on rural and remote psychiatry: geographic classification, suicide and workforce inequity, social determinants, telepsychiatry and collaborative care models, crisis transfer logistics, cultural safety, and rural training pipelines. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
1. Definitions and classification
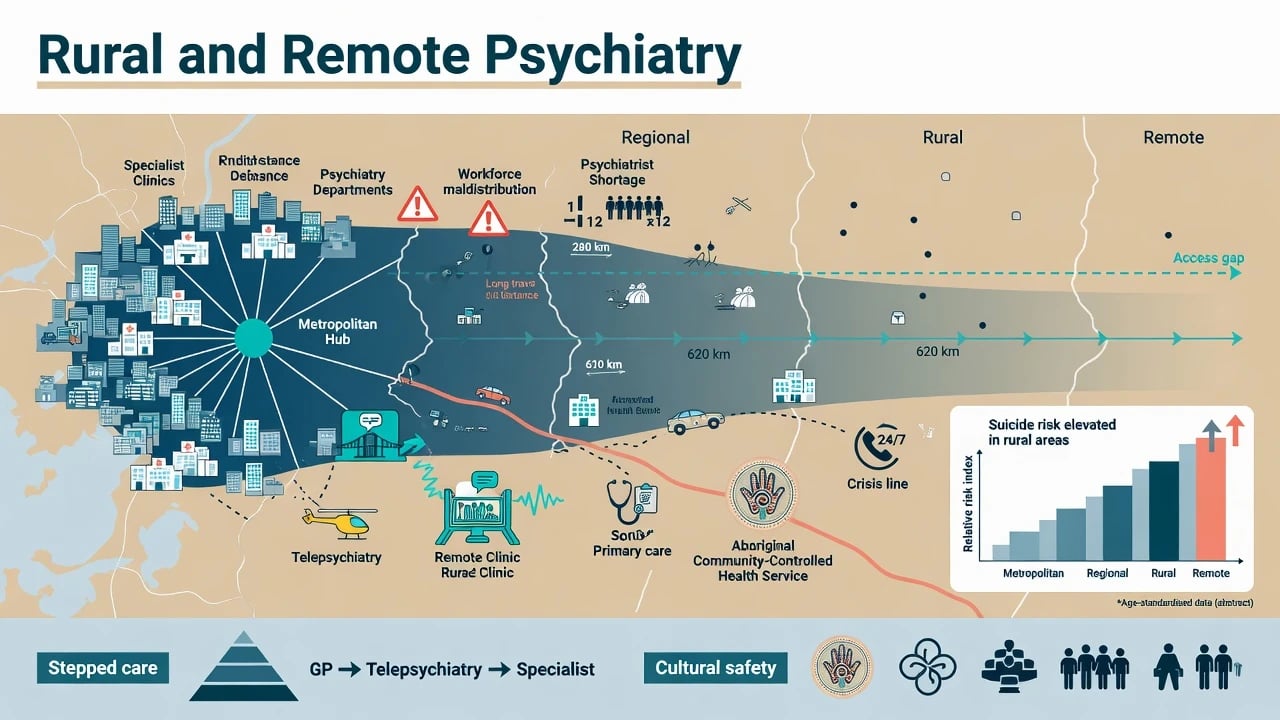
Rural and remote psychiatry is the practice of assessing, treating, and organising care for people with mental disorders when specialist density is low and travel time is high. It sits within public and community psychiatry, overlapping addiction, forensic, child, old-age, and Indigenous mental health. Nosology remains DSM-5-TR / ICD-11; what changes is service design, risk environment, and continuity models.[3][14]
Geographic frameworks (viva must-state)
| System | Use in exams |
|---|---|
| ASGS Remoteness Areas | Major Cities → Inner Regional → Outer Regional → Remote → Very Remote (Australian Bureau of Statistics geography) |
| Modified Monash Model (MMM) | MMM1 (metro) to MMM7 (very remote) — workforce incentive and training policy language |
| RUCA / frontier (US) | Rural–urban commuting areas; frontier for extreme sparsity |
| Rurality indices (UK/Canada) | Board-specific labels; principle is distance + density, not "farm equals rural" |
| These frameworks operationalise distance and density for policy and workforce planning rather than defining a separate psychiatric syndrome.[7][8] |
Do not equate "rural" with one lifestyle. A coastal regional city (MMM2–3) differs from a very remote community reachable only by air (MMM6–7) in workforce, broadband, cultural mix, and retrieval logistics.[7][8]
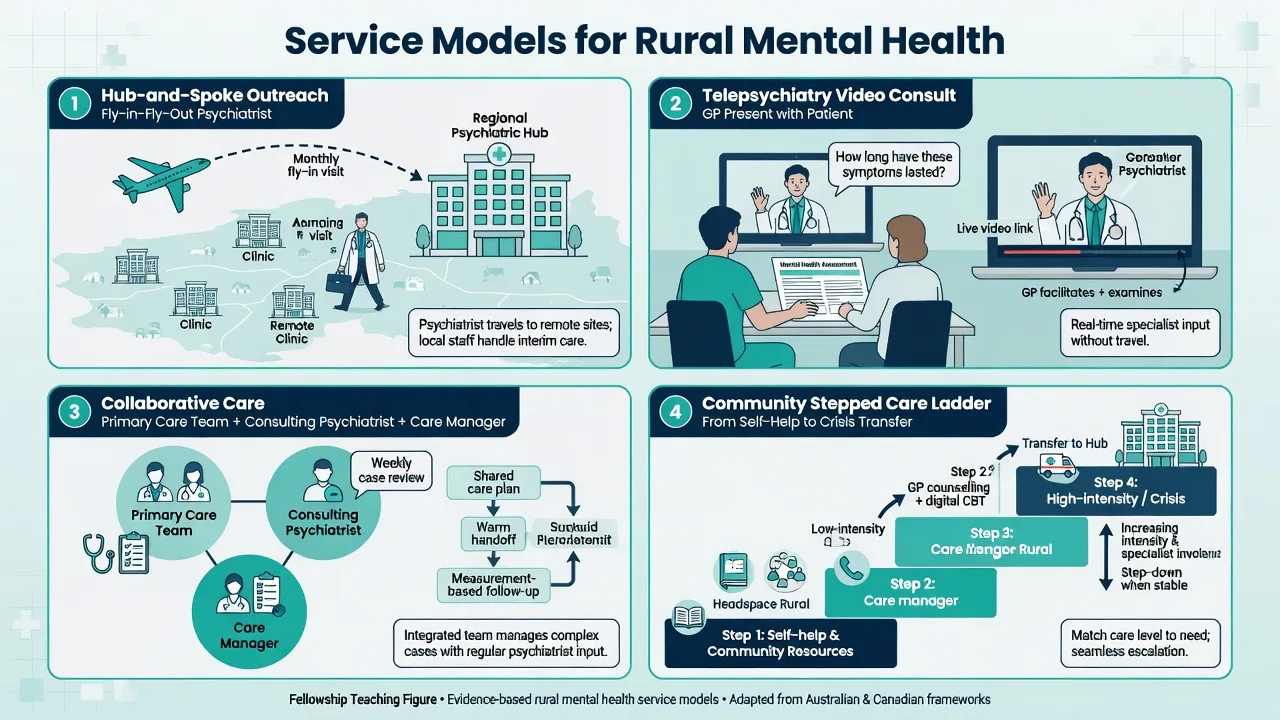
Service-model taxonomy
Resident specialist
- On-site psychiatrist/CMHT
- Best continuity when sustainable
- Rare in remote MMM6–7
- Still needs after-hours plan
Visiting / FIFO / outreach
- Scheduled clinics from hub
- Face-to-face depth for complex care
- Continuity risk between visits
- Pair with tele between visits
Telepsychiatry
- Synchronous video standard of care
- Asynchronous store-and-forward options
- Evidence for effectiveness and process standards
- Needs local emergency backup
Collaborative care
- GP + care manager + consulting psychiatrist
- Measurement-based primary care
- Extends capacity without relocating all specialists
- Fits rural primary care reality
2. Epidemiology and risk
Mental disorders generate large global disability burden (YLDs) across settings; rural inequity is primarily access, determinants, and lethality pathways, not immunity from illness.[20][13]
Rural viva numbers and patterns
Suicide. Classic NSW data showed urban–rural suicide differentials, with higher rates among many Australian-born rural populations in the study period.[9] Contemporary retrospective work on rural Australian suicides documents substantial mental health problems alongside limited help-seeking and service utilisation before death — the exam message is not "no illness," but late or absent engagement.[6] Farmer suicide qualitative synthesis clusters financial pressure, drought, isolation, masculine help-seeking norms, and access to lethal means.[10] Climate–drought scenarios project ongoing rural suicide risk under adverse environmental futures in NSW modelling work.[12] Community prevention programmes exist but evaluation quality is mixed; a recent scoping review maps rural and remote Australian initiatives without claiming a single magic programme.[11] Cross-national work on ideation, plans, and attempts (Nock) supports population framing while reminding candidates that individual prediction remains weak — especially in small rural denominators.[21]
Workforce. Australia's psychiatry workforce has grown overall, yet rural and remote regions remain under-served — maldistribution is the live problem, not only absolute headcount.[7] Rural workforce analyses ask why trainees and specialists do not stay rural and point to training design, generalism, lifestyle, and support systems.[8]
Treatment gap and resources. Globally, a large share of people with mental disorders receive no treatment; scarcity, inequity, and inefficiency of resources are the classic systems triad.[13][14] Rural settings concentrate all three.
3. Mechanisms of inequity
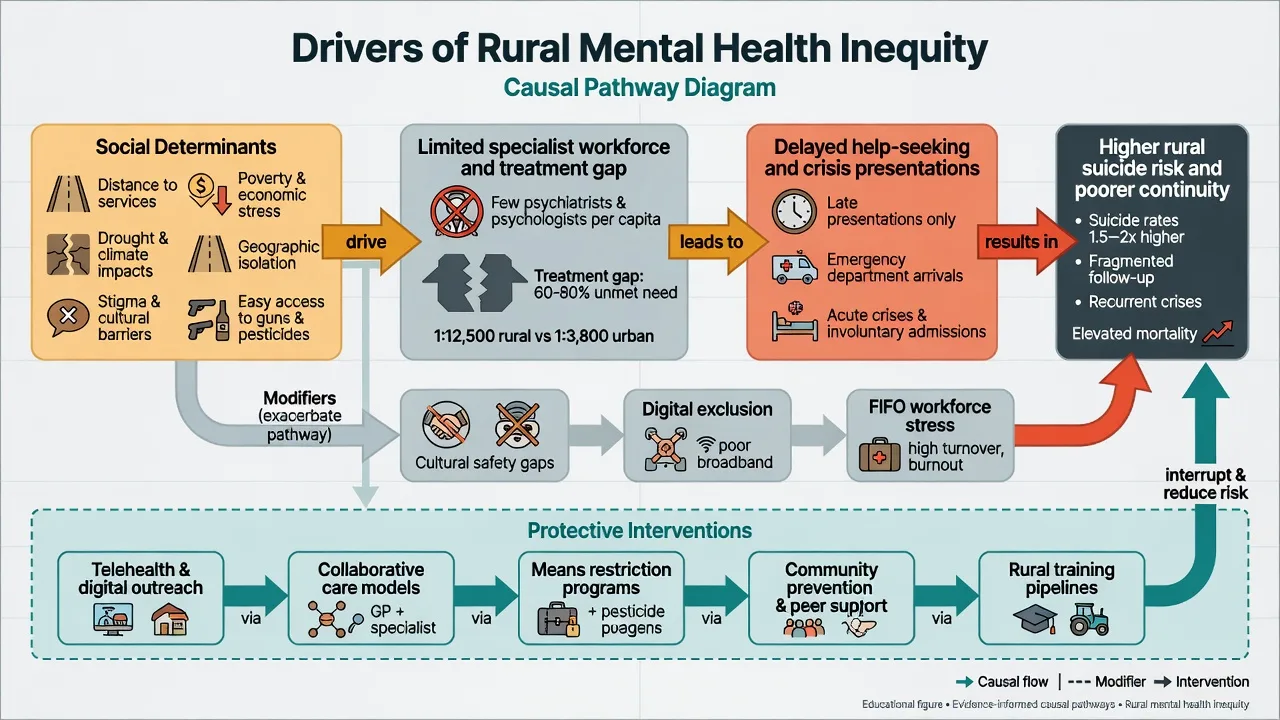
Structural. Specialist and psychotherapy supply concentrates in cities; travel cost and time convert treatable illness into untreated disability.[7][14]
Social determinants. Poverty, education, housing, violence, discrimination, climate stress, and employment volatility map onto mental disorder risk across the life course; rural drought and industry collapse are concrete local forms of these pathways.[15][12]
Stigma and privacy. In small towns, perceived visibility of clinic attendance and dual relationships suppress help-seeking; stigma interventions with social contact components have the best evidence base at population level.[16][6]
Means and rescue delay. Firearms, pesticides, isolation, and long emergency response times raise case fatality when attempts occur — a public-health lever (means restriction, safe storage) alongside clinical care.[10][21]
Digital exclusion. Telehealth only closes gaps when broadband, devices, privacy space, and digital literacy exist; otherwise it recreates inequity under a modern label.[1][2]
4. Clinical presentation
Patients rarely self-label as "rural psychiatry cases." They present via GP, ED, police, school, ACCHO, or workplace. Expect longer DUP (duration of untreated psychosis), crisis-first mood and substance presentations, and high medical comorbidity with limited local specialty backup.[3][6]
Tele-MSE specifics. Confirm identity, location, and privacy. Assess video quality for affect, psychomotor activity, and EPS. Explicitly ask about weapons, pesticides, and who is in the house. If risk escalates mid-session, activate local emergency services using the pre-confirmed address — Shore best-practice standards make emergency planning a process requirement, not an afterthought.[2]
Small-community dynamics. Staff may know the patient socially. Name the dual-relationship issue, document boundaries, and offer tele-options with non-local clinicians when appropriate.[8]
5. Differential and framing traps
| Trap | Correct frame |
|---|---|
| Low admissions = rare illness | Service contact ≠ incidence; treatment gap is large |
| "Just stress from the drought" | Drought is a determinant; still assess MDD, alcohol, suicide, psychosis |
| Tele-diagnosis equals full assessment | Needs local vitals, intoxication check, collateral, and investigations |
| Cultural content = non-psychotic | Consult culturally; never skip risk or medical work-up |
| One visit FIFO = full care | Continuity requires between-visit tele and primary care ownership |
| Framing traps matter because low service contact and drought narratives can hide unmet need, incomplete tele-assessment, and discontinuity between visiting clinics.[6][12][13][2] |
6. Assessment structure
History. Presenting problem; mood, psychosis, substance, trauma; prior admissions and legal status; medications and adherence logistics; social map (housing, work/FIFO roster, farm isolation, children, DV); cultural identity and preferred supports; firearms/pesticides access.[6][10][17]
Risk. Suicide, violence, vulnerability, children at risk, fire risk, driving. Rural modifiers: means, isolation, delayed response, alcohol/stimulant context, previous near-fatal attempts.[6][21]
Scales (pragmatic). PHQ-9, GAD-7, AUDIT, K10 in primary care; use for measurement-based collaborative care, not as standalone suicide predictors.[3][4]
Collateral. GP, family, police, school, Aboriginal health worker — often more decisive than another solitary interview hour when presentations are delayed and local knowledge fills tele-assessment blind spots.[2][3][6]
7. Investigations and monitoring logistics
Baseline FBC, UEC, LFT, glucose/lipids, TSH as indicated; ECG before antipsychotics or when QTc risk is present; beta-hCG when relevant. Remote practice fails when results cannot return or be acted on. Clozapine needs a named blood-monitoring pathway and red-flag action plan; lithium needs level logistics and education about dehydration in heat/drought work. First-episode atypical features warrant imaging/medical work-up — plan retrieval early rather than serial remote guesswork.[3]
8. Acute and emergency management
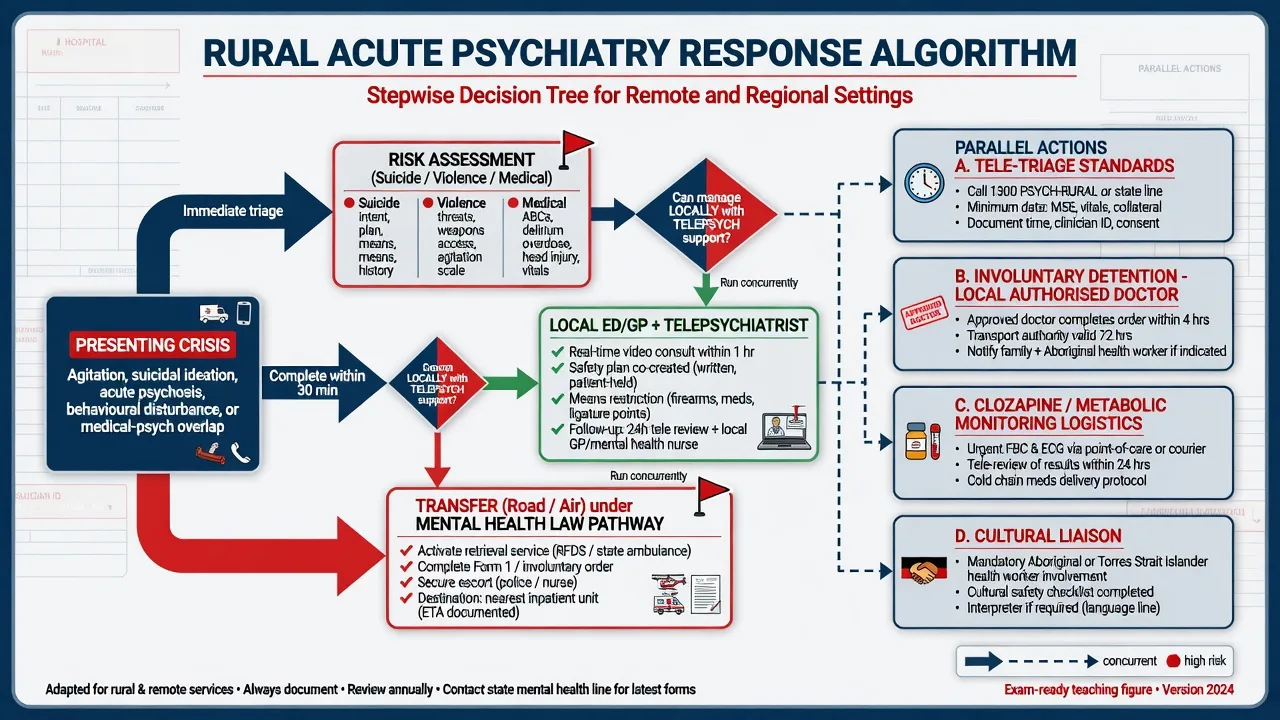
Local ED package. Medical clearance (glucose, alcohol/withdrawal, head injury, toxidromes); environmental safety; rapid tranquillisation per local protocol when needed; early telepsychiatrist consult; legal status documentation; destination bed search if transfer required.[2][3]
Retrieval. Road vs air depends on distance, weather, clinical stability, and escort. Sedation for flight requires airway-capable escort. Destination should include a step-down plan back to local services — otherwise the rural service becomes a one-way export system.[14]
Medical psych emergencies (NMS, serotonin syndrome, lithium toxicity, catatonia, delirium) follow the same recognition rules as urban practice, but ICU/psych bed scarcity shortens the threshold for retrieval under the scarcity–inequity–inefficiency resource frame.[14]
9. Definitive management and service design
Telepsychiatry
Hilty and colleagues' 2013 review synthesised evidence that telemental health is effective across many diagnostic groups and can improve access, with diagnostic reliability broadly comparable to in-person care when systems are well designed.[1] Shore and colleagues published best practices for videoconferencing-based telemental health covering technology, clinical environment, emergency protocols, and documentation standards that remain exam-standard process language.[2] Yellowlees and colleagues' RCT comparing asynchronous versus synchronous telepsychiatry in primary care supports both models as clinically viable options when matched to workflow — useful when bandwidth or scheduling limits live video.[5] Economic analyses need explicit frameworks for cost shifting (travel saved vs technology and coordination costs).[19]
Collaborative care and primary care integration
Fortney and colleagues describe how telepsychiatry integrates mental health into rural primary care, addressing capacity and equity when relocating psychiatrists is not feasible.[3] The SPIRIT trial design targets complex psychiatric disorders in rural primary care using telepsychiatry collaborative care approaches — examiners like the model name even when quoting results cautiously as a comparative-effectiveness programme.[4] Clinician experience papers on telepsychiatry collaborative care for PTSD and bipolar disorder highlight care-manager workflows, measurement-based care, and consultation cadence as the operational core.[22] Queensland's Virtual Integrated Practice (VIP) pilot shows an Australian partnership model supporting rural general practice with virtual specialist input.[18]
Pharmacotherapy practicalities
Standard evidence-based agents still apply, but rural logistics decide whether an evidence-based regimen is actually deliverable between visiting or tele clinics.[3]
Rural twists that examiners expect: prefer regimens with local injectable nursing capacity for LAIs when travel undermines oral adherence; avoid initiating clozapine or lithium without monitoring contracts; for alcohol withdrawal use local detox protocols with tele-advice and give thiamine 100 mg orally or parenterally (route by clinical severity and local protocol) for Wernicke prevention — full withdrawal algorithms sit in addiction topics; naloxone take-home and OAT continuity still matter in regional methamphetamine and opioid markets.[3][1]
Psychosocial and community interventions
CBT and other therapies can be delivered by telehealth when appropriate; low-intensity guided self-help and GP-based programmes expand coverage. Community suicide prevention should combine means restriction, gatekeeper training, and aftercare — evaluation literature is still developing for rural Australia.[11][16]
Stigma as a clinical intervention target
Anti-stigma programmes with social contact components have the strongest evidence synthesis; rural campaigns must protect confidentiality rather than publicly "outing" service users.[16]
10. Subtypes and scenarios
Very remote Indigenous community. Partner with ACCHO; cultural safety and SEWB frameworks; telepsych + visiting clinics; never use children as interpreters; high medical and trauma comorbidity awareness (link cultural formulation topic).[15][16]
Farming district in drought. Screen depression, alcohol, suicide, domestic stress; ask about firearms; financial counselling referral; community gatekeepers (agronomists, stock agents) as allies.[10][12]
FIFO mining camp. Roster-related sleep disruption, substance use, relationship strain; partners also carry burden — Gardner qualitative work documents wellbeing concerns for workers and partners.[17]
Regional youth. CAP scarcity; school tele-mental health; self-harm pathways to regional ED; family-based plans when privacy at home is limited — tele and collaborative models extend scarce specialist reach for younger people as for adults.[1][3]
Older rural adult. Transport barriers; grief and isolation; geriatric telepsychiatry; deprescribing polypharmacy with GP, using telemental health evidence and primary-care integration principles.[1][3]
Forensic/regional custody. Tele-assessments for fitness and medication; avoid incomplete risk formulation without collateral from custodial staff, with the same emergency-process standards as other high-risk tele assessments.[2]
11. Complications and pitfalls
Other traps: dual relationships; over-reliance on FIFO discontinuity; digital exclusion of older and poor patients; starting high-monitoring drugs without labs; underestimating alcohol/stimulant contributions; cultural stereotyping; equating English fluency with understanding of rights and consent.[8][2][16]
12. Prognosis and disposition
Prognosis tracks continuity, engagement, substance use, social supports, and treatment coverage. Disposition ladder: self-help/digital → GP collaborative care → tele-specialist → visiting clinic → regional inpatient → tertiary transfer → structured step-down with 7-day follow-up. Service metrics (time-to-psychiatrist, transfer rates, post-discharge contact) matter more for system viva than any single rating scale score.[3][14]
13. Special populations
Children/youth (CAP desert); perinatal (distance from mother–baby units); older adults; intellectual disability; Aboriginal and Torres Strait Islander remote communities; rural LGBTIQ+ people with privacy constraints; veterans in country towns; migrant farm workers with language barriers.[15][16]
14. Regional deltas
Australian answers should use ASGS/MMM language, acknowledge psychiatrist maldistribution, and integrate telehealth MBS-era norms with RANZCP rural training and generalism agendas.[7][8] Rural suicide and farmer/drought pathways are high-yield FRANZCP content.[6][10][12] Models such as VIP show virtual support to rural general practice.[18] Cultural safety and ACCHO partnership are non-optional for remote Indigenous care.
15. Evidence map and controversies
Name at viva: Hilty 2013 (effectiveness); Shore 2018 (process standards); Fortney (rural primary care telepsychiatry; SPIRIT design); Yellowlees async vs sync RCT; Hayter and Darmawan (AU workforce); Fitzpatrick, Morrell, Purc-Stephenson, Hanigan, Schineanu (rural suicide cluster); Kohn, Saxena, Lund, Thornicroft, GBD (population frame); Gardner (FIFO); Lepre VIP; Hilty cost framework; Hoeft collaborative care experience.[1][2][3][4][5][6][7][8][9][10][11][12][13][14][15][16][17][18][19][20][22]
Controversies for balanced answers: whether telehealth can substitute for rural training investment; privacy vs small-town dual relationships; involuntary transfer ethics when local alternatives are thin; scope of asynchronous psychiatry; evaluating suicide-prevention programmes with small numbers and confounding.[5][7][8][11]
16. Exam pearls
REMOTE
Self-test: five viva openers
(1) Define rural/remote psychiatry without inventing a new diagnosis. (2) Name one Australian workforce paper and one telepsychiatry effectiveness paper. (3) Run a tele-suicide assessment safety checklist. (4) Design a drought-district suicide response beyond "open a clinic." (5) Explain why MMM classification matters for training incentives.[1][2][7][10][12]
References
- [1]Hilty DM, Ferrer DC, Parish MB, et al. The effectiveness of telemental health: a 2013 review Telemed J E Health, 2013.PMID 23697504
- [2]Shore JH, Yellowlees P, Caudill R, et al. Best Practices in Videoconferencing-Based Telemental Health April 2018 Telemed J E Health, 2018.PMID 30358514
- [3]Fortney JC, Pyne JM, Turner EE, et al. Telepsychiatry integration of mental health services into rural primary care settings Int Rev Psychiatry, 2015.PMID 26634618
- [4]Fortney JC, Heagerty PJ, Bauer AM, et al. Study to promote innovation in rural integrated telepsychiatry (SPIRIT): Rationale and design of a randomized comparative effectiveness trial of managing complex psychiatric disorders in rural primary care settings Contemp Clin Trials, 2020.PMID 31678410
- [5]Yellowlees PM, Parish MB, Gonzalez AD, et al. Clinical Outcomes of Asynchronous Versus Synchronous Telepsychiatry in Primary Care: Randomized Controlled Trial J Med Internet Res, 2021.PMID 33993104
- [6]Fitzpatrick SJ, Handley T, Powell N, et al. Suicide in rural Australia: A retrospective study of mental health problems, health-seeking and service utilisation PLoS One, 2021.PMID 34288909
- [7]Hayter CM, Allison S, Bastiampillai T, et al. The changing psychiatry workforce in Australia: Still lacking in rural and remote regions Aust J Rural Health, 2024.PMID 38419201
- [8]Darmawan W, Harding C, Coleman M, et al. Rural workforce challenges: Why not rural psychiatry? Australas Psychiatry, 2023.PMID 36356575
- [9]Morrell S, Taylor R, Slaytor E, et al. Urban and rural suicide differentials in migrants and the Australian-born, New South Wales, Australia 1985--1994 Soc Sci Med, 1999.PMID 10414842
- [10]Purc-Stephenson R, Doctor J, Keehn JE Understanding the factors contributing to farmer suicide: a meta-synthesis of qualitative research Rural Remote Health, 2023.PMID 37633833
- [11]Schineanu A, Brabin J, McLaren S, et al. Evaluating community-based suicide prevention initiatives in rural and remote Australia: a scoping review Rural Remote Health, 2025.PMID 41207602
- [12]Hanigan IC, Chaston TB Climate Change, Drought and Rural Suicide in New South Wales, Australia: Future Impact Scenario Projections to 2099 Int J Environ Res Public Health, 2022.PMID 35805514
- [13]Kohn R, Saxena S, Levav I, et al. The treatment gap in mental health care Bull World Health Organ, 2004.PMID 15640922
- [14]Saxena S, Thornicroft G, Knapp M, et al. Resources for mental health: scarcity, inequity, and inefficiency Lancet, 2007.PMID 17804062
- [15]Lund C, Brooke-Sumner C, Baingana F, et al. Social determinants of mental disorders and the Sustainable Development Goals: a systematic review of reviews Lancet Psychiatry, 2018.PMID 29580610
- [16]Thornicroft G, Mehta N, Clement S, et al. Evidence for effective interventions to reduce mental-health-related stigma and discrimination Lancet, 2016.PMID 26410341
- [17]Gardner B, Alfrey KL, Vandelanotte C, et al. Mental health and well-being concerns of fly-in fly-out workers and their partners in Australia: a qualitative study BMJ Open, 2018.PMID 29519796
- [18]Lepre B, Job J, Martin Z, et al. The Queensland Virtual Integrated Practice (VIP) partnership program pilot study: an Australian-first model of care to support rural general practice BMC Health Serv Res, 2023.PMID 37907917
- [19]Hilty DM, Serhal E, Crawford A A Telehealth and Telepsychiatry Economic Cost Analysis Framework: Scoping Review Telemed J E Health, 2023.PMID 35639444
- [20]GBD 2019 Mental Disorders Collaborators Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019 Lancet Psychiatry, 2022.PMID 35026139
- [21]Nock MK, Borges G, Bromet EJ, et al. Cross-national prevalence and risk factors for suicidal ideation, plans and attempts Br J Psychiatry, 2008.PMID 18245022
- [22]Hoeft TJ, Hall JD, Solberg LI, et al. Clinician Experiences With Telepsychiatry Collaborative Care for Posttraumatic Stress Disorder and Bipolar Disorder Psychiatr Serv, 2023.PMID 36444528