Psych · Public and community psychiatry — school and workplace mental health
School and workplace mental health
Also known as School mental health · Workplace mental health · Occupational mental health · Multi-tiered systems of support · Social and emotional learning · SEYLE · Youth Aware of Mental Health · Good Behavior Game · Return to work mental health · Mentally healthy workplace · Job strain · Burnout occupational
Exam-exhaustive fellowship reference on school and workplace mental health: multi-tiered school systems, SEL, SEYLE/YAM, Good Behavior Game, school prevention meta-analyses, workplace psychosocial risk models (demand-control, ERI, JD-R, burnout), organisational vs individual interventions, return-to-work evidence, disclosure and stigma, and psychiatrist roles. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Schools and workplaces are the two settings where most people spend their days and where common mental disorders often declare themselves as attendance failure, performance change, conflict, or suicide risk. Fellowship examiners expect you to operate as a systems psychiatrist: define multi-tiered school models and landmark trials (SEYLE, SEL meta-analyses, Good Behavior Game lineage), model workplace pathogenesis (demand-control, effort-reward imbalance, JD-R, burnout), prefer organisational primary prevention over individual-only programmes, and coordinate graded return-to-work with clinical care.[1][2][3][6][7][8]

Overview and definition
Settings-based mental health redesigns environments (school, workplace) rather than waiting for clinic presentation. It sits within public and community psychiatry alongside primary care collaborative care and population prevention.[4][13]
School mental health spans: (1) promotion of social-emotional skills and climate; (2) prevention of depression, anxiety, substance harm, and suicide behaviour; (3) early identification and pathway to care; (4) support for students with established disorders to remain engaged in learning. It is not a substitute for specialist CAMHS when indicated care is needed.[4][5]
Workplace mental health spans: (1) primary prevention via job design and culture; (2) secondary prevention (early support, manager training); (3) treatment access for clinical disorders; (4) return-to-work (RTW) and disability management; (5) stigma and disclosure support.[6][7][13]
| Frame | Core idea | Exam discriminator |
|---|---|---|
| Usual care | Episodic clinic after crisis | Misses population reach |
| Awareness only | Posters, one-off talks | Weak without pathways and redesign |
| Multi-tier school (MTSS) | Universal → selective → indicated | Intensity matches risk |
| Organisational workplace model | Change demands/control/rewards/support | Targets pathogen, not only person |
| Individual-only workplace model | Stress management, mindfulness alone | Necessary adjunct, insufficient if job is toxic |
Classification — school MTSS and workplace intervention levels
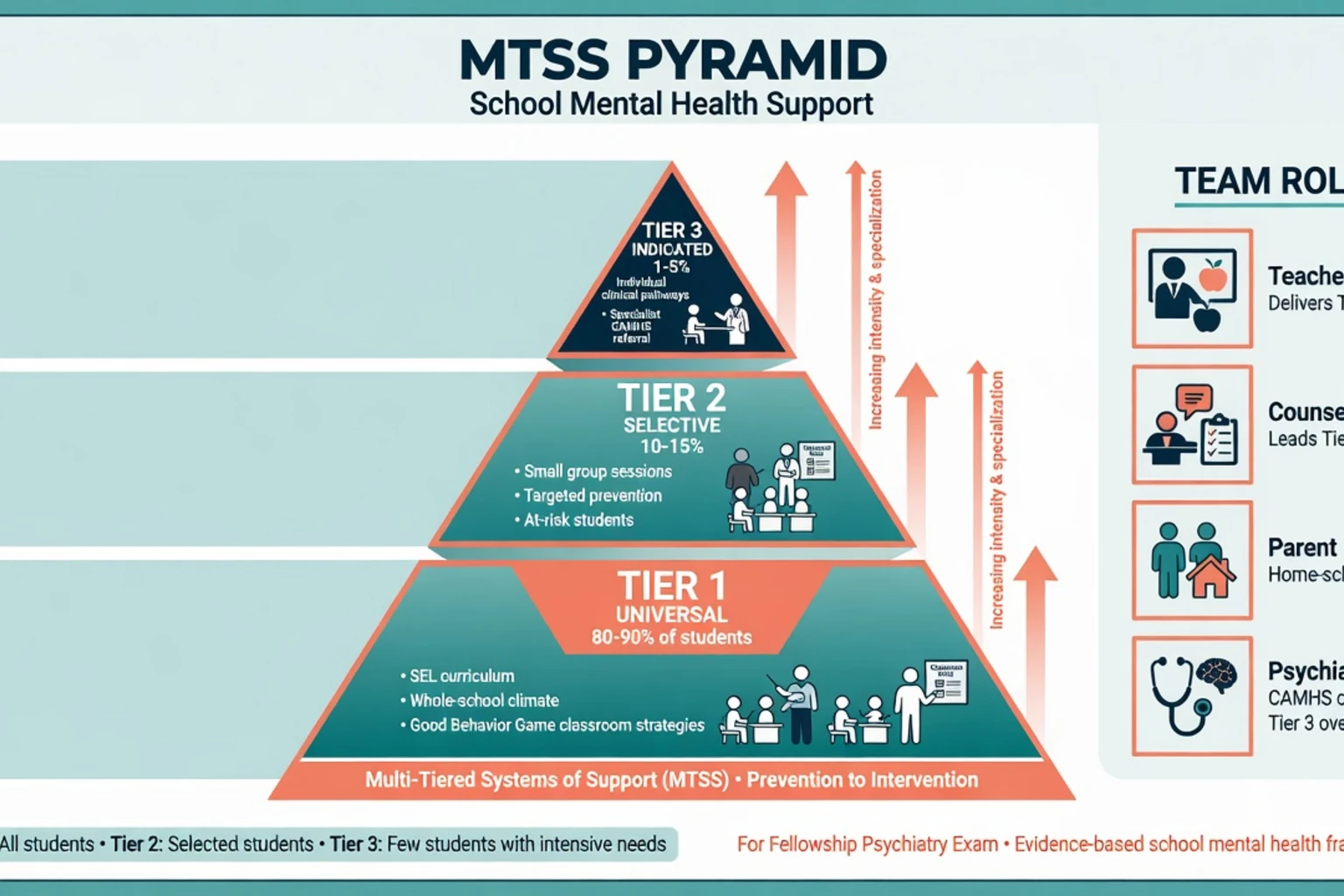
School: multi-tiered systems of support (MTSS)
- Tier 1 — Universal. Whole-school climate, social and emotional learning (SEL), classroom behaviour systems (Good Behavior Game lineage), teacher practices, anti-bullying policy, mental health literacy.[2][3][4]
- Tier 2 — Selective. Small-group skill programmes, mentoring, targeted support for elevated risk (bullying victims, early anxiety, parental mental illness context) without full clinical diagnosis required.[4][5]
- Tier 3 — Indicated. Students with disorders or high risk: individual counselling, clinical pathways, specialist CAMHS, safety planning, education adjustments.[4][5]
SEL trains self-awareness, self-management, social awareness, relationship skills, and responsible decision-making as universal classroom curricula. Meta-analysis of school-based universal SEL programmes shows gains in social-emotional skills, attitudes, behaviour, and academic performance relative to controls.[3]
Whole-school evidence principles (Weare and Nind): multi-component approaches that combine skills teaching, climate, teacher involvement, and parent engagement outperform fragmented one-off sessions; implementation quality is decisive.[4]
Workplace: prevention levels and burnout nosology
- Organisational (primary): redesign demands, increase control and support, fair rewards, anti-bullying, safe hours, role clarity.[6][7][13]
- Manager/team (secondary): mental health literacy for supervisors, early supportive conversation, reasonable adjustments.[13]
- Individual: stress management, CBT skills, EAP access — adjuncts, not sole strategy when psychosocial design is pathogenic.[6][11]
- Clinical/RTW: treat disorders; coordinate graded work resumption.[10][14]
Burnout (Maslach): emotional exhaustion, cynicism/depersonalisation, and reduced professional efficacy. ICD-11 frames burnout as an occupational phenomenon, not a free-standing psychiatric diagnosis synonym — always assess for major depression, anxiety, trauma, and substance use.[8][9]
Epidemiology and risk
School and workplace headlines
National Comorbidity Survey Replication age-of-onset data show that a large fraction of lifetime mental disorders begin by adolescence and early adulthood — the school years are a critical prevention window, not a waiting room for adult psychiatry.[16] Workplace meta-review evidence links high job demands with low control (job strain), low social support, effort-reward imbalance, organisational injustice, job insecurity, long working hours, and bullying to elevated risk of common mental health problems.[7] Conversely, systematic meta-review evidence supports mental health benefits of employment relative to unemployment when work quality is considered, reinforcing supported employment and RTW as recovery interventions rather than optional extras.[12]
Pathophysiology and systems mechanisms
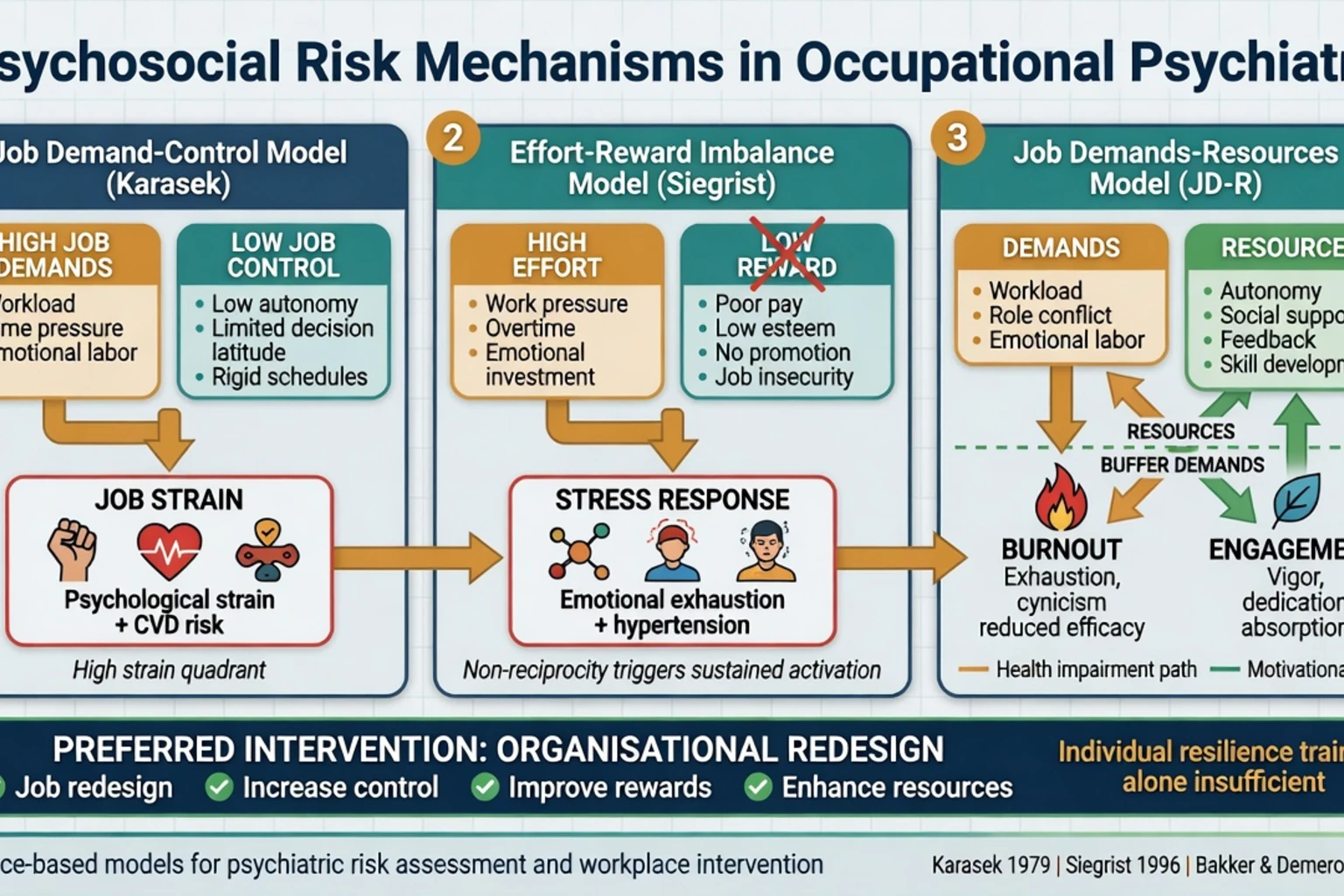
Examiners want mechanistic models, not slogans — job strain, effort-reward imbalance, and related psychosocial exposures are the pathways synthesised in work-risk meta-reviews.[7]
Job demand-control (Karasek lineage). High psychological demands combined with low decision latitude produce job strain; high support buffers strain (iso-strain when support is also low). Strain is a pathway to distress, depression risk, and reduced recovery capacity.[7]
Effort-reward imbalance (Siegrist). High effort with low reward (salary, esteem, career opportunities, job security) produces sustained stress responses and is linked to adverse health outcomes including mental health sequelae in the occupational literature summarised in risk meta-reviews.[7]
Job demands-resources (JD-R). Job demands deplete energy (burnout path); job resources (autonomy, feedback, support, meaning) foster engagement and buffer demands. Burnout research for psychiatry emphasises the three-dimension experience and organisational drivers.[8][9]
School mechanisms. Peer rejection, bullying, academic pressure, and poor teacher-student climate amplify risk; social-emotional skills, belonging, and predictable classroom behaviour systems are protective levers targeted by universal programmes.[2][3][4] Developmental timing matters: untreated adolescent depression and anxiety impair education trajectories and embed disability into adult working life.[5][16]
Clinical presentation
School signals: falling grades, non-attendance or school refusal interface, withdrawal from peers, irritability, somatic complaints, online conflict spill-over, self-harm content shared with peers or teachers, and sudden identity or appearance changes that worry staff.[4][5]
Workplace signals: presenteeism, rising error rates, conflict with supervisors, sick-leave clusters after weekends or night shifts, alcohol or stimulant use to cope, cynicism about patients/clients (health and human services), and the burnout triad of exhaustion, detachment, and inefficacy.[8][9] High-functioning professionals may mask until a near-miss, complaint, or suicidal crisis — do not equate high performance with low risk.
Differential
| Presentation | Prefer organisational or school system response | Prefer clinical specialty/crisis |
|---|---|---|
| Mild distress with clear job redesign target | Manager support, job redesign, brief skills | If no response or escalating risk |
| Tier 1–2 school need | SEL, small group, pastoral care | Active plan/intent, psychosis, severe ED, abuse |
| "Burnout" label | Still screen depression/substance | Major depression, mania, psychosis, SUD |
| Interpersonal conflict at work | Mediation, anti-bullying process | Trauma syndromes, severe personality crisis, violence risk |
| Long sick leave with CMD | Work-focused RTW + treatment | If risk high or diagnosis unclear |
School refusal is a behaviour, not a diagnosis: differential includes separation anxiety, social anxiety, depression, bullying, learning disability, autism, family systems factors, and rare organic causes — multi-informant assessment is mandatory (cross-link school-refusal topic).[4][5]
Assessment
School consultation structure. Multi-informant history (student, parent/carer, teacher), developmental and learning history, bullying and online risk, substance use, family mental health, MSE, suicide/self-harm risk, safeguarding screen, and functional impact on attendance and peer life. Clarify consent and confidentiality limits with adolescents early.[4][5]
Workplace assessment structure. Symptom diagnosis plus job analysis: demands, control, support, rewards, hours, shift patterns, bullying/harassment, role conflict, and RTW barriers. Ask about disclosure history and feared discrimination.[7][15] Tools (PHQ-9, GAD-7, burnout inventories) measure severity and trajectory; they do not replace diagnosis or risk formulation.
Dual roles. Occupational assessments requested by employers create dual-agency tensions: state who the client is, what will be disclosed, and obtain appropriate consent. Fitness-for-work language should be functional and evidence-based within competence, with disclosure risks understood in light of workplace stigma literature.[15]
Investigations
Targeted medical work-up when fatigue, cognitive change, or mood shift may be organic (TSH, FBC, metabolic panel, sleep apnoea screening history, substance screen as indicated). Educational psychology assessment when learning disability is plausible. Serial symptom and functional measures track school programme response and RTW progress.[5][10] Imaging and advanced tests follow organic red flags — not routine for psychosocial job strain alone.
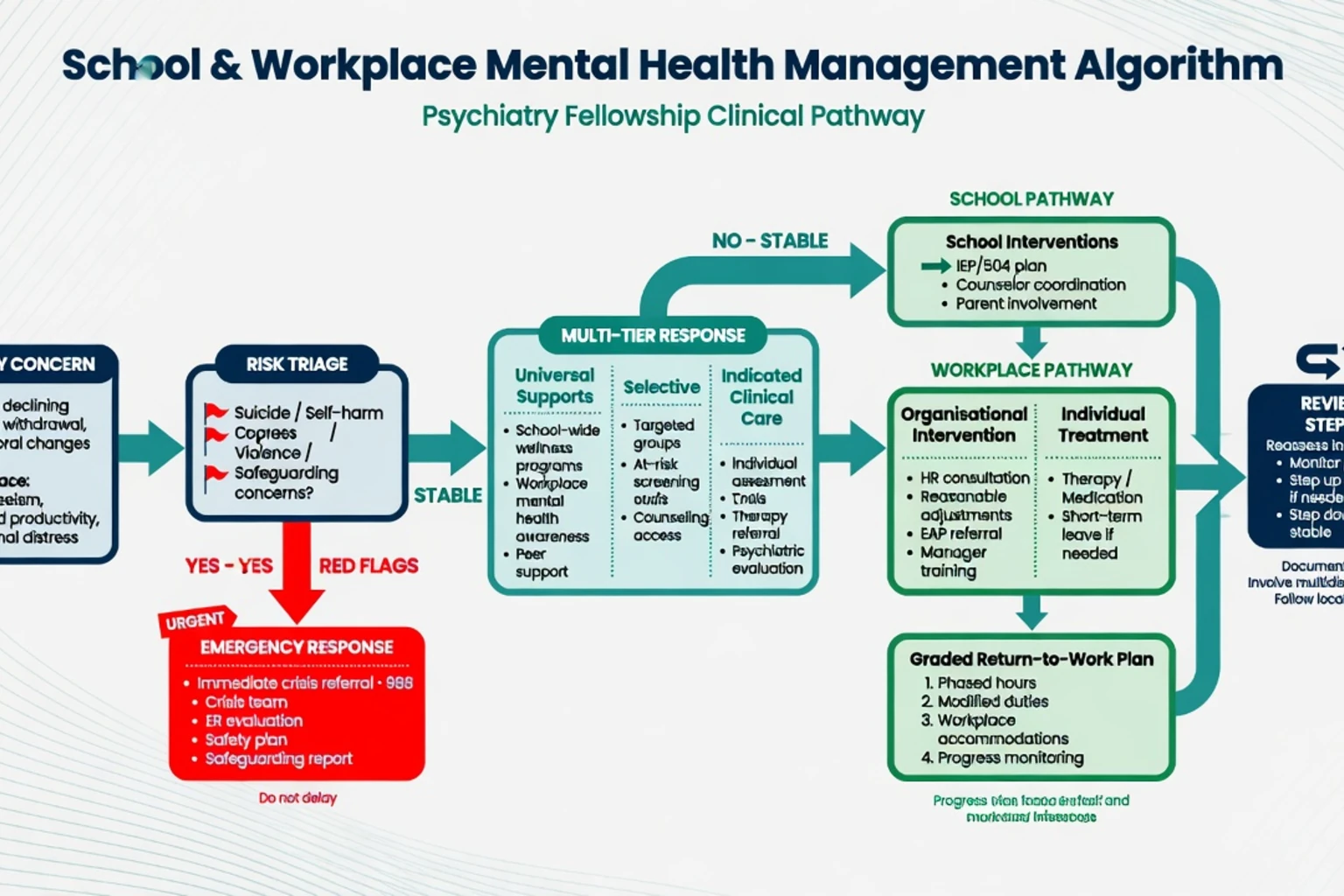
Acute and emergency management
[1] [5]In schools: secure immediate safety, notify parents/carers when appropriate under local law and risk, use crisis services, document, and plan re-entry with supports. In workplaces: remove immediate hazards, activate crisis care, notify duty-of-care contacts as required after consent/risk calculus, and avoid forcing public disclosure to the whole team.[1][15]
Definitive management
School programmes with landmark evidence
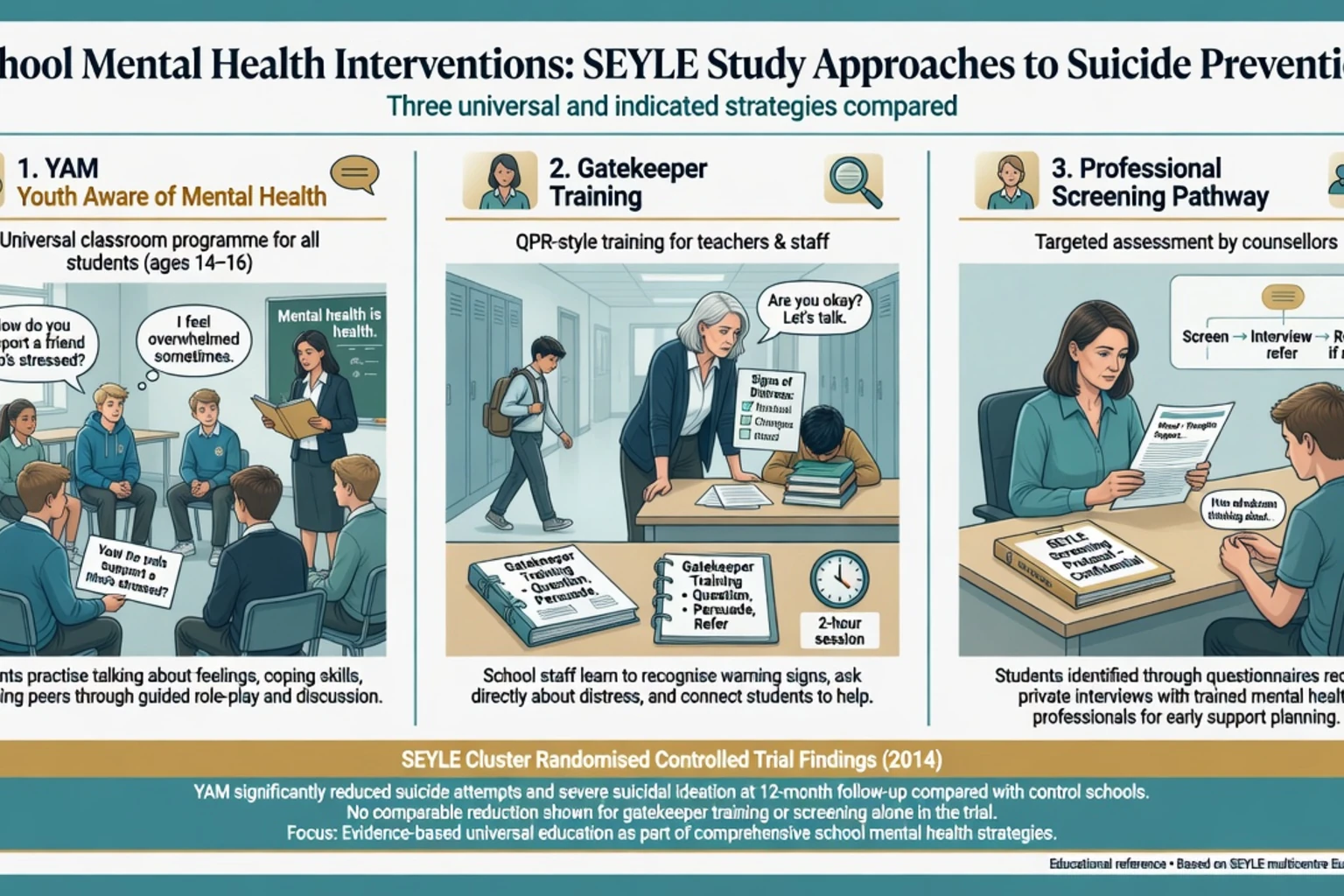
SEYLE (Wasserman et al., 2015). Large European school-based cluster RCT of suicide prevention. Youth Aware of Mental Health (YAM) — a universal interactive awareness and skills programme — reduced incident suicide attempts and severe suicidal ideation at 12 months compared with control. In the primary analysis, the Question, Persuade, Refer (QPR) gatekeeper arm and the professional screening arm did not show the same superiority on those primary outcomes. Exam pearl: name YAM and do not claim all three arms were equally effective.[1]
Good Behavior Game (GBG). Universal classroom behaviour management in early grades with longitudinal prevention literature linking improved classroom behavioural ecology to later reductions in high-risk trajectories (substance and related outcomes in follow-up studies). Kellam and colleagues position GBG as a foundational universal prevention technology, not a psychotherapy brand.[2]
SEL meta-analysis (Durlak et al.). Universal school-based SEL improves social-emotional skills, attitudes, positive social behaviour, conduct problems, emotional distress, and academic performance versus controls — the quantitative backbone for Tier 1 advocacy.[3]
Depression and anxiety prevention (Werner-Seidler et al.). School-based programmes reduce depression and anxiety symptoms with small-to-moderate effects overall; design, targeting, and implementation quality modify benefit. Universal programmes cast a wide net; indicated programmes may yield larger effects in some contexts but require identification systems.[5]
Whole-school synthesis (Weare and Nind). Best evidence supports comprehensive, multi-component, skills-based approaches embedded in school life rather than isolated lessons without climate change.[4]
Workplace interventions
Risk reduction. Address the exposures in Harvey meta-review: high demands with low control, low support, ERI, injustice, insecurity, long hours, bullying.[7]
Intervention evidence. Joyce meta-review of workplace interventions for common mental disorders finds stronger support for certain CBT-based and multicomponent approaches; effect sizes and quality vary, and organisational interventions remain under-studied relative to individual programmes despite theoretical priority.[6] Tan and colleagues found that universal workplace interventions can reduce depression symptoms, with CBT-based programmes among more promising approaches in meta-analysis — still not a licence to ignore job redesign.[11]
Mentally healthy workplace frameworks (Petrie et al. and related Australian research groups) integrate: design work to minimise harm, build organisational resilience culture, support early help-seeking, provide recovery-oriented RTW, and reduce stigma.[13]
Return to work
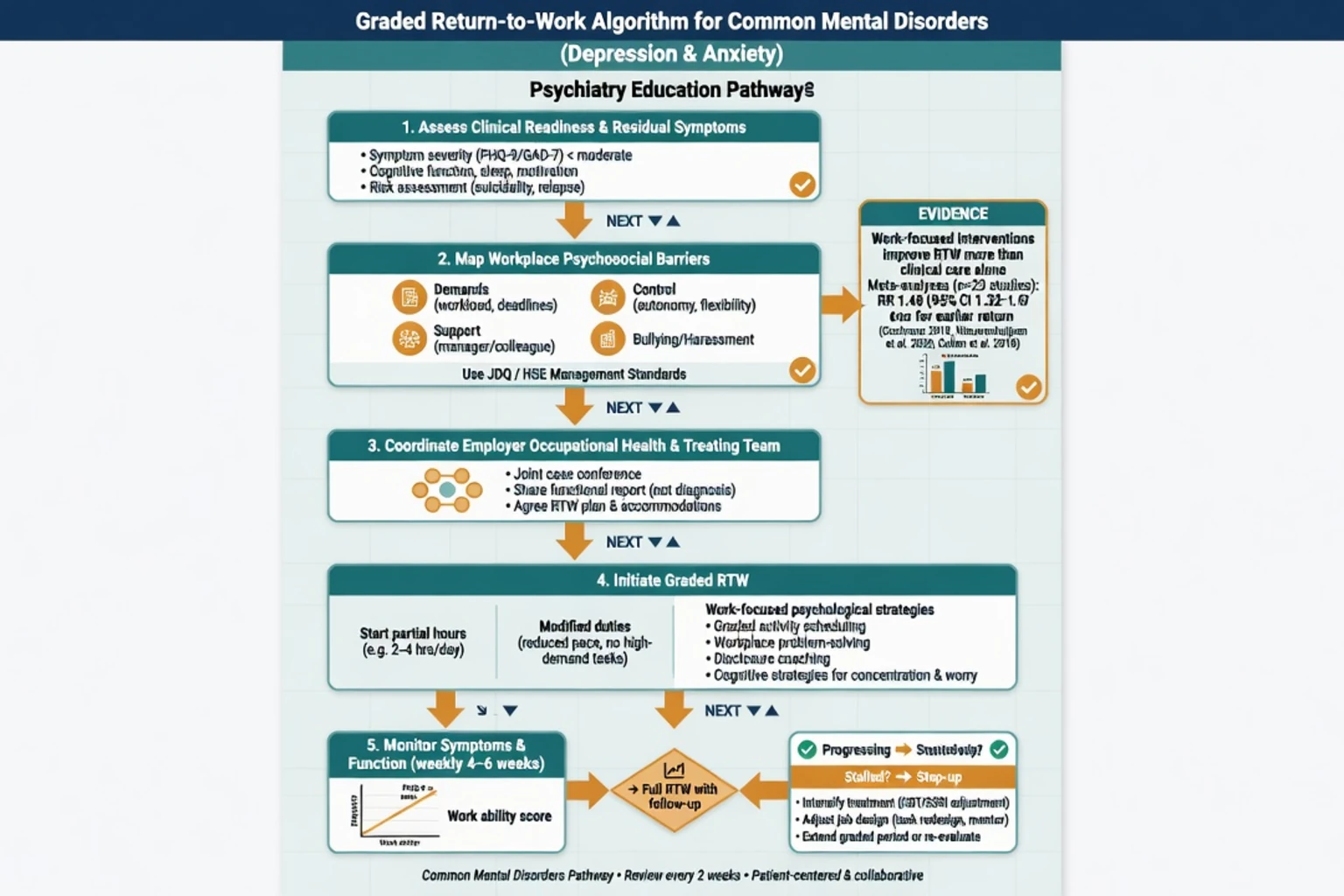
Clinical recovery without work-focused planning often fails RTW. Cochrane review evidence on interventions to improve RTW in depressed people supports work-directed and multicomponent strategies in context; interpret effect sizes carefully and avoid claiming a single universal protocol.[10] Meta-analysis of RTW interventions for common mental illness shows that adding work-focused components improves RTW outcomes beyond clinical care alone in pooled estimates, though heterogeneity is high.[14] Prognostic factors for RTW include symptom severity, age, and work-related factors — assess barriers explicitly rather than only titrating medication.[14]
Practical RTW sequence: confirm diagnosis and risk; treat actively; map job demands and supports with employer/occupational health; graded hours and modified duties; work-focused CBT elements (problem-solving, behavioural activation toward work tasks); review every 1–2 weeks early; step up treatment or redesign if stalled.[10][14]
Pharmacotherapy for clinical depression or anxiety follows standard monographs (adequate dose, duration, monitoring). Time sedating agents away from safety-critical duties when possible; discuss driving and machine-operation risks. Do not use medication as the sole RTW plan when bullying or impossible workload is the main pathogen.[6][7]
Subtypes and scenarios
| Scenario | High-yield approach |
|---|---|
| Primary classroom aggression/disruption | Universal behaviour ecology (GBG lineage) + selective supports |
| Secondary school suicide cluster fear | Evidence-based postvention principles + YAM-style universal literacy; avoid sensational assemblies |
| Healthcare worker burnout | Organisational load and culture first; screen depression/suicide; cross-link doctor-health topic |
| Construction/high-risk male industries | Stigma-aware, peer-based, practical pathways; address job insecurity and injury pain |
| FIFO/shift work | Sleep, roster design, isolation, substance risk |
| First-episode psychosis RTW/study | Supported education/employment, low EE family work, medication adherence, graded goals |
| Small business, no EAP | GP collaborative care + clear crisis plan + manager education lite |
Complications and pitfalls
- Fidelity decay of school programmes (manual left on shelf).[4]
- Screening without capacity in schools or workplaces.[1][5]
- Burnout mislabel masking major depression.[8][9]
- Resilience training only while demands stay extreme.[6][7]
- Forced disclosure and discrimination after workplace mental health "awareness" campaigns.[15]
- Ignoring bullying as a clinical perpetuating factor.
- Over-medicalising normal distress while under-treating true disorders.
- Inventing jurisdiction-specific employment statutes or MBS item numbers in exams.
Prognosis and disposition
SEL universal programmes improve multi-domain youth outcomes when well implemented.[3] SEYLE shows that carefully designed universal suicide-prevention curricula (YAM) can reduce suicide attempts and severe ideation at 12 months at population school level.[1] School depression/anxiety prevention yields small-moderate average effects — clinically meaningful at scale, not a cure-all.[5] Workplace trajectories depend on whether psychosocial risks are modified and whether RTW is work-focused.[7][10][14]
Disposition ladder: universal supports → selective school/work programmes → primary care/collaborative care → specialty psychiatry/psychology → crisis services. Step up early for risk, psychosis, mania, severe anorexia, or failed RTW despite adequate treatment.[1][5][10][13]
Special populations
Neurodevelopmental disorders. Classroom and workplace adjustments (structure, sensory load, executive supports) are core, not optional kindness. LGBTQ+ youth face elevated bullying-related risk — anti-bullying climate is clinical prevention. Indigenous and culturally diverse students/workers need culturally governed programmes, not imported manuals without adaptation.[4] Severe mental illness: supported employment models (e.g. IPS principles) outperform stepwise "train then place" philosophies for many — cross-link rehabilitation topics. Rural settings: telepsychiatry and school/work digital literacy programmes extend reach but still need local crisis pathways.[13]
Evidence and guidelines
| Landmark | Message |
|---|---|
| SEYLE 2015 | YAM reduced suicide attempts and severe ideation vs control; QPR and screening not superior on primary outcomes in main analysis |
| Durlak SEL 2011 | Universal SEL improves skills, behaviour, academics |
| Weare and Nind 2011 | Whole-school multi-component approaches |
| Werner-Seidler 2017 | School depression/anxiety prevention MA |
| Kellam GBG reviews | Universal classroom prevention lineage |
| Harvey 2017 | Work psychosocial risks for CMD |
| Joyce 2016 | Workplace intervention meta-review |
| Tan 2014 | Universal workplace depression prevention |
| Modini 2016 | Employment mental health benefits meta-review |
| Petrie 2018 | Mentally healthy workplace framework |
| Nieuwenhuijsen 2020 | Cochrane RTW in depression |
| Nigatu 2016 | RTW interventions for CMD |
| Maslach 2001/2016 | Burnout dimensions and psychiatry implications |
| Brohan 2012 | Workplace disclosure beliefs and behaviours |
| Kessler 2005 | Early age of onset — school window |
ANZ (RANZCP-facing). Use multi-tier school mental health language aligned with education systems and headspace/primary care interfaces; workplace essays should cite organisational risk control and RTW coordination with GPs and occupational providers. Mentally healthy workplace frameworks from Australian research groups are high-yield for local viva colour without inventing funding codes.[13]
UK (NICE / MRCPsych). School and workplace wellbeing guidance emphasises whole-setting approaches, early help, and evidence-based psychological interventions; RTW and fit-note culture are common Paper B/CASC themes. Cite principles rather than memorising every NICE code number unless the stem supplies them.[6][10]
US (APA / ABPN). MTSS/SEL and multi-tier PBIS-adjacent language appears in systems questions; occupational burnout literature is extensive in health workers. SEYLE remains the cleanest named school suicide-prevention RCT for exams.[1][3][9]
India / MD-DNB / NEET-SS. School mental health and district programme task-sharing are the scalable cousins; workplace formal EAP is uneven — emphasise teacher gatekeeping, family engagement, and primary care links without assuming European trial infrastructure.[4][5]
Exam pearls
[1]- MTSS: Tier 1 universal, Tier 2 selective, Tier 3 indicated.[4]
- Durlak SEL meta-analysis = skills + behaviour + academics.[3]
- GBG = universal classroom behaviour prevention lineage.[2]
- Burnout triad ≠ depression diagnosis; still screen and treat depression.[8][9]
- Harvey: job strain, low support, ERI, bullying, insecurity, long hours.[7]
- Prefer organisational redesign; individual CBT-based programmes help but do not fix toxic design alone.[6][11][13]
- RTW needs work-focused components (Nieuwenhuijsen, Nigatu).[10][14]
- Plan workplace disclosure; anticipated discrimination shapes concealment (Brohan).[15]
- Never use school or workplace programmes as the only response to active suicidal intent.[1]
Related topics
Prevention and early intervention; doctor health and burnout; stigma and rights-based care; suicide risk assessment; school refusal; major depression and anxiety disorders; rehabilitation and recovery services; collaborative care — use this topic for the settings architecture and named trials above.[1][6][13]
References
- [1]Wasserman D, Hoven CW, Wasserman C, et al. School-based suicide prevention programmes: the SEYLE cluster-randomised, controlled trial Lancet, 2015.PMID 25579833
- [2]Kellam SG, Mackenzie AC, Brown CH, et al. The good behavior game and the future of prevention and treatment Addict Sci Clin Pract, 2011.PMID 22003425
- [3]Durlak JA, Weissberg RP, Dymnicki AB, et al. The impact of enhancing students' social and emotional learning: a meta-analysis of school-based universal interventions Child Dev, 2011.PMID 21291449
- [4]Weare K, Nind M Mental health promotion and problem prevention in schools: what does the evidence say? Health Promot Int, 2011.PMID 22079935
- [5]Werner-Seidler A, Perry Y, Calear AL, et al. School-based depression and anxiety prevention programs for young people: A systematic review and meta-analysis Clin Psychol Rev, 2017.PMID 27821267
- [6]Joyce S, Modini M, Christensen H, et al. Workplace interventions for common mental disorders: a systematic meta-review Psychol Med, 2016.PMID 26620157
- [7]Harvey SB, Modini M, Joyce S, et al. Can work make you mentally ill? A systematic meta-review of work-related risk factors for common mental health problems Occup Environ Med, 2017.PMID 28108676
- [8]Maslach C, Schaufeli WB, Leiter MP Job burnout Annu Rev Psychol, 2001.PMID 11148311
- [9]Maslach C, Leiter MP Understanding the burnout experience: recent research and its implications for psychiatry World Psychiatry, 2016.PMID 27265691
- [10]Nieuwenhuijsen K, Verbeek JH, Neumeyer-Gromen A, et al. Interventions to improve return to work in depressed people Cochrane Database Syst Rev, 2020.PMID 33052607
- [11]Tan L, Wang MJ, Modini M, et al. Preventing the development of depression at work: a systematic review and meta-analysis of universal interventions in the workplace BMC Med, 2014.PMID 24886246
- [12]Modini M, Joyce S, Mykletun A, et al. The mental health benefits of employment: Results of a systematic meta-review Australas Psychiatry, 2016.PMID 26773063
- [13]Petrie K, Joyce S, Tan L, et al. A framework to create more mentally healthy workplaces: A viewpoint Aust N Z J Psychiatry, 2018.PMID 28835112
- [14]Nigatu YT, Liu Y, Uppal M, et al. Interventions for enhancing return to work in individuals with a common mental illness: systematic review and meta-analysis of randomized controlled trials Psychol Med, 2016.PMID 27609709
- [15]Brohan E, Henderson C, Wheat K, et al. Systematic review of beliefs, behaviours and influencing factors associated with disclosure of a mental health problem in the workplace BMC Psychiatry, 2012.PMID 22339944
- [16]Kessler RC, Berglund P, Demler O, et al. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication Arch Gen Psychiatry, 2005.PMID 15939837