Psych · Public and community psychiatry — restrictive practices
Seclusion, restraint and least-restrictive care
Also known as Restrictive practices psychiatry · Mechanical restraint · Physical restraint · Chemical restraint · Seclusion room · Least restrictive alternative · Six Core Strategies · Safewards · Project BETA seclusion · Trauma-informed containment
Exam-exhaustive fellowship reference on seclusion, physical/mechanical/chemical restraint, and least-restrictive care — definitions, harms evidence, indication thresholds, monitoring and positional safety, Six Core Strategies, Safewards, Project BETA avoidance principles, trauma-informed reduction, special populations, governance and documentation. Principles only; no invented statute section numbers. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags

Definition and classification
Restrictive care practices sit at the sharp end of psychiatry: they can prevent catastrophe and can also injure, kill, retraumatise, and destroy trust. Fellowship examiners expect precise definitions, a least-restrictive ladder, named reduction frameworks, and honest harm evidence — not theatre about invented legal maximums.[1][7][15]
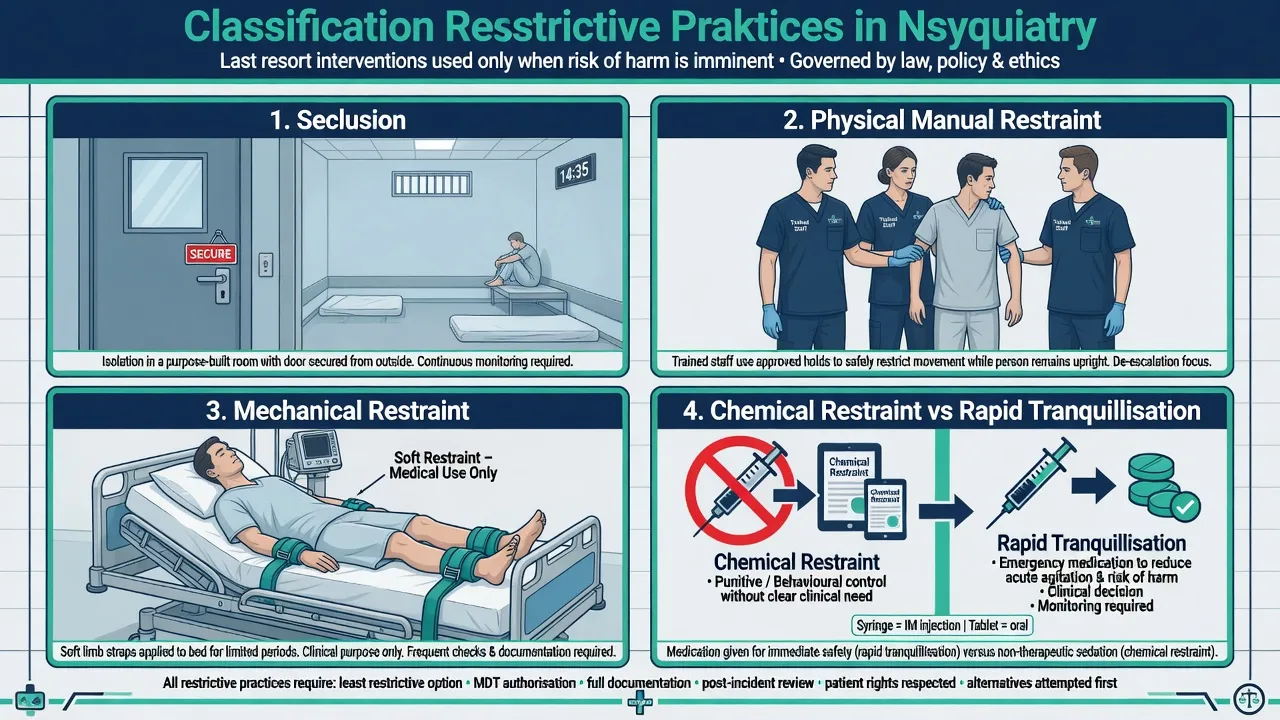
Seclusion is the involuntary confinement of a person alone in a room or area from which free exit is prevented. It is not the same as voluntary use of a quiet room or sensory space when the person can leave. Physical (manual) restraint is restriction of movement by staff using bodily force. Mechanical restraint uses devices (belts, cuffs, chairs, or improvised devices) to restrict free movement. Chemical restraint is a contested term: broadly, medication used primarily to control behaviour or restrict freedom of movement rather than to treat a diagnosed condition — overlapping awkwardly with legitimate rapid tranquillisation (RT) for severe agitation or psychosis under protocol.[7][15]
Environmental restraint (locked wards, restricted egress for a unit population) and other restricted practices (e.g. restricting belongings) are related governance domains but are not identical to an individual seclusion episode. Systematic review shows definitions vary across literature and services — always map local operational definitions when auditing rates.[15]
Least-restrictive care means choosing the intervention that achieves necessary safety (and lawful treatment) aims with the least intrusion on liberty, privacy, dignity, and bodily integrity. Least restrictive is not least convenient for the roster.[7][10]
| Modality | Core definition | High-yield discriminator |
|---|---|---|
| Seclusion | Alone; free exit prevented | Vs voluntary quiet/sensory room |
| Physical restraint | Staff body force restricts movement | Trained holds only; positional safety |
| Mechanical restraint | Device restricts movement | Highest scrutiny; many systems aim to eliminate |
| Chemical restraint | Medication primarily for behavioural control | Vs RT with therapeutic indication + protocol |
| Environmental | Unit-level restriction of freedom | Not a substitute for individual clinical review |
Epidemiology and risk
Rates of seclusion and restraint vary enormously across countries, hospitals, and wards. Case-mix matters, but so do leadership, staffing models, physical environment, training, and whether restrictive practice is culturally normal or exceptional. Multinational reduction programmes show that large falls are achievable without claiming a single universal zero overnight.[4][13][16]
Correlates of higher use in clinical series commonly include acute psychosis and mania, severe behavioural disturbance, intellectual disability and dual diagnosis, forensic settings, staffing strain, and younger age in some child/adolescent samples. Equity: Indigenous and ethnic minority over-representation appears in some ANZ and international systems; reduction strategies for Māori mental health service users emphasise cultural safety and specific organisational strategies, not colour-blind rate targets alone.[17][18]
Organisational trajectory data from the Pennsylvania state hospital system (2011–2020) document effects of ending seclusion and mechanical restraint use at scale — proof-of-concept that sustained system change is possible.[13] Contemporary commentary calls for regulatory action toward cessation of seclusion and mechanical restraint in psychiatric hospitals, reflecting a rights and safety agenda rather than a claim that all behavioural emergencies vanish.[14]
Mechanisms of harm and of escalation
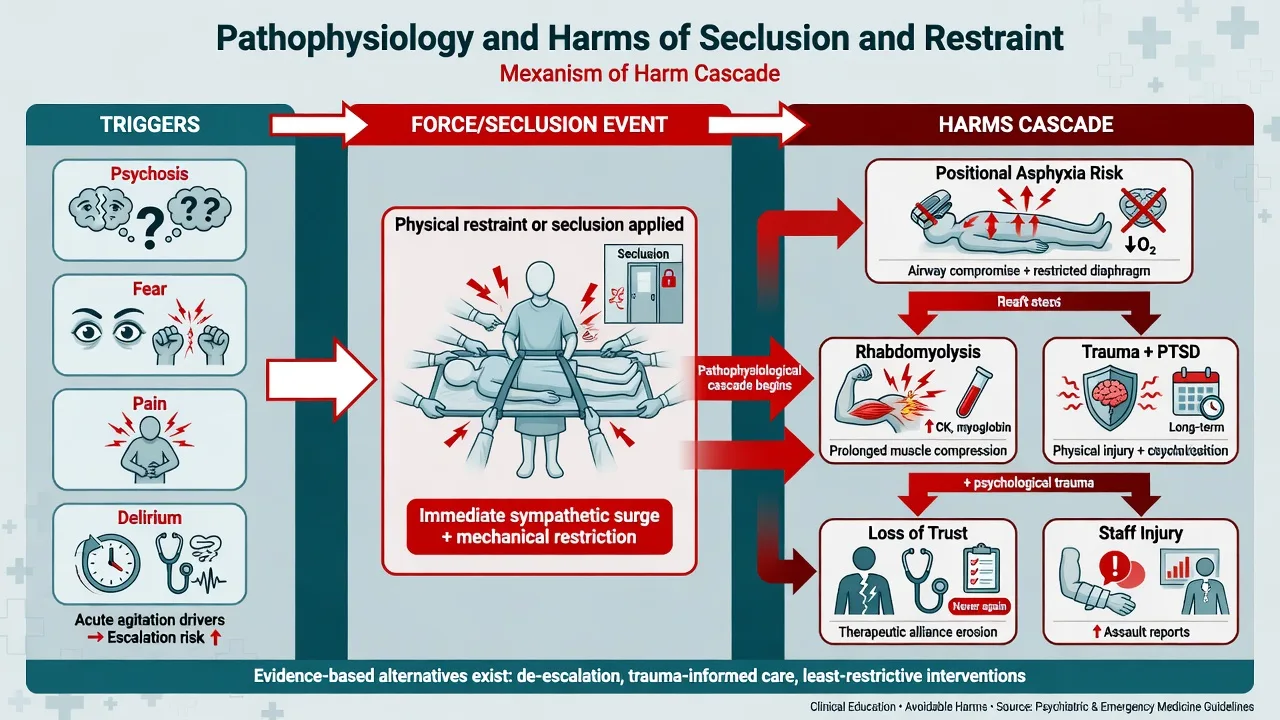
Behavioural emergencies are a final common pathway: psychosis, mania, fear, pain, intoxication, withdrawal, delirium, akathisia misread as agitation, and trauma triggers can all produce aggression or self-harm risk. Containment without diagnosis is how medical emergencies are missed.[7][9]
Physical pathways: struggle and restraint increase catecholamine surge, hyperthermia risk, rhabdomyolysis, aspiration, venous thromboembolism with prolonged immobility, fractures and soft-tissue injury, and positional asphyxia — especially with prolonged prone restraint, pressure on chest/abdomen, or airway compromise. Death during restraint is rare relative to episode counts but is a catastrophic, often preventable, system failure.[1][7]
Psychological pathways: humiliation, powerlessness, retraumatisation (especially with prior sexual or physical abuse), post-traumatic symptoms, anger, and eroded trust. Systematic review of seclusion and restraint effects in adult psychiatry documents significant adverse effects and weak evidence of benefit, supporting last-resort framing with safeguards.[1] Coercion literature shows process quality — respect, fairness, explanation — shapes whether force is later judged necessary or abusive.[10][11][12]
Organisational pathway: when restrictive practice is default, de-escalation skill atrophies, staffing models assume force, and rates stay high. Conversely, leadership, data transparency, and workforce development reverse the cycle (Six Core Strategies logic).[3][4]
Clinical presentation and when force is considered
Classic stems: acute psychotic or manic assault after failed de-escalation; severe self-injury that cannot be interrupted; ED severe behavioural disturbance with weapons or uncontrolled violence; forensic high-secure incident under dual security-clinical governance; child/adolescent unit escalation; dual diagnosis intellectual disability crisis where seclusion has become an unexamined "behaviour plan". Project BETA frameworks and reduction literature treat these as high-risk flashpoints requiring de-escalation-first pathways, not default force.[5][7][17]
Presentation skill includes scene reading: instrumental vs disorganised aggression; panic/PTSD flashback; delirium fluctuation; akathisia; substance intoxication. Staff moral distress and secondary trauma after prolonged holds are part of the clinical system presentation — ignore them and rates stay high.[7][8]
Differential: what is this intervention actually?
- Alone; exit prevented
- Time-limited safety
- Continuous/frequent observation
- Not voluntary quiet room
- Manual holds
- Trained technique only
- Avoid prolonged prone
- Airway always first
- Name the therapeutic aim
- Protocol + monitoring
- Primary purpose test
- Document indication
Also separate: locked-ward environmental restriction vs individual seclusion; security/police restraint in ED vs clinical restrictive practice under health policy; guardianship/safeguarding pathways vs mental health restrictive practice authorisation. Definitions of restrictive practices are not uniform internationally — state the definition you are using.[15]
Bedside assessment before and during crisis
- ABCDE, glucose, SpO2 — concurrent with behavioural management, not after the seclusion door closes.[9]
- Imminence and severity of harm — who is at risk, with what weapons, how soon?
- What less restrictive options are still available — space, one calm communicator, remove audience, sensory tools, oral medication offer, increased staffing observation?
- Legal status and local authorisation rules for seclusion/restraint — principles: necessity, proportionality, least restriction; verify local forms, never invent sections.[7][10]
- Trauma, culture, language, sensory needs — interpreter; cultural support; known triggers.
- Team plan — lead communicator; roles; exit criteria for the intervention before it starts.
- Capacity and communication — explain as much as possible even under force; process quality matters later.[11][12]
RESTRICT
Investigations
No laboratory test authorises seclusion. Investigate for organic contributors when indicated (metabolic panel, blood gas if respiratory concern, CK after prolonged struggle, ECG when antipsychotics or cardiac risk, toxicology as clinically driven, pregnancy test when relevant). Post-episode injury survey is mandatory. Documentation is part of the "investigation" of the event for governance: indication, alternatives, start/stop times, staff present, observations, injuries, debrief.[1][7]
Immediate management — safety without culture of force
Project BETA ladder (ED and transferable principles)
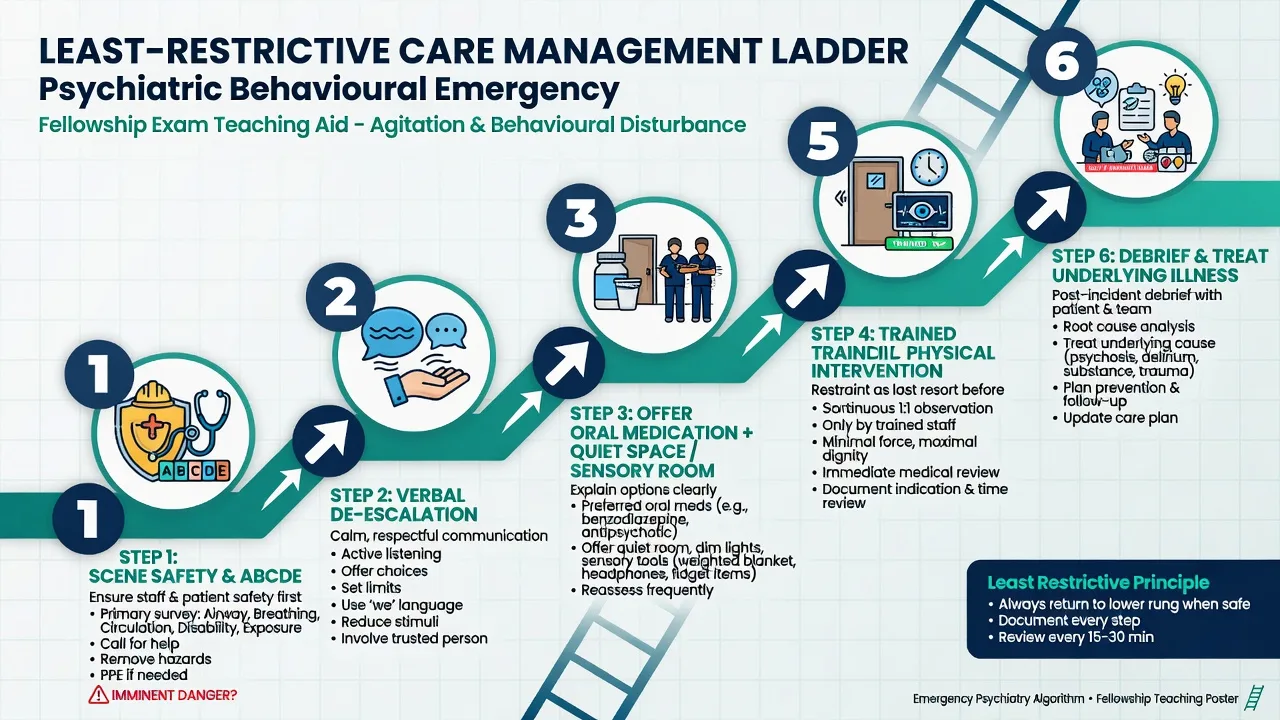
Project BETA frames best practices for evaluation and treatment of agitation: medical evaluation and triage, psychiatric evaluation, verbal de-escalation, psychopharmacology when needed, and use and avoidance of seclusion and restraint.[7][8][9] Verbal de-escalation is first-line interpersonal technology: respect personal space, one lead communicator, concise language, set clear limits with choices, listen, agree where possible, and avoid power struggles.[8]
If physical intervention is unavoidable
- Use trained holds only; call the response team early rather than improvising.
- Prefer positions that protect airway and chest expansion; avoid prolonged prone restraint; do not pile bodies on the torso.
- Continuous observation of airway, colour, respiratory rate, consciousness, and distress.
- Shortest duration; release stepwise as soon as safe.
- Concurrent plan for medication that treats the driver (e.g. protocolised RT) rather than endless wrestling.[7]
If seclusion is used
- Lawful authority and local policy compliance.
- State exit criteria at initiation (what calm/rousable/cooperative threshold ends seclusion).
- Observation frequency per local policy — continuous when risk is high; never "park and forget".
- Meet basic needs: hydration, toileting, temperature, dignity of clothing as safe.
- Medical review for injury and physiological compromise.
- Immediate step-down plan and senior notification for prolonged episodes.[1][7]
Chemical restraint vs rapid tranquillisation
State the primary purpose. Medication given under an agitation/psychosis protocol to restore calm for assessment and treatment, with monitoring, is framed as RT (see sister topic on acute agitation and rapid tranquillisation). Medication used primarily to restrict freedom or silence without a treatment aim is the ethical core of the chemical restraint critique. Document indication, agent, dose, route, response, and monitoring; avoid polypharmacy that produces unrousable sedation as a substitute for nursing observation.[7][9][15]
Definitive management — reduction systems (exam high-yield)
Six Core Strategies (Huckshorn)
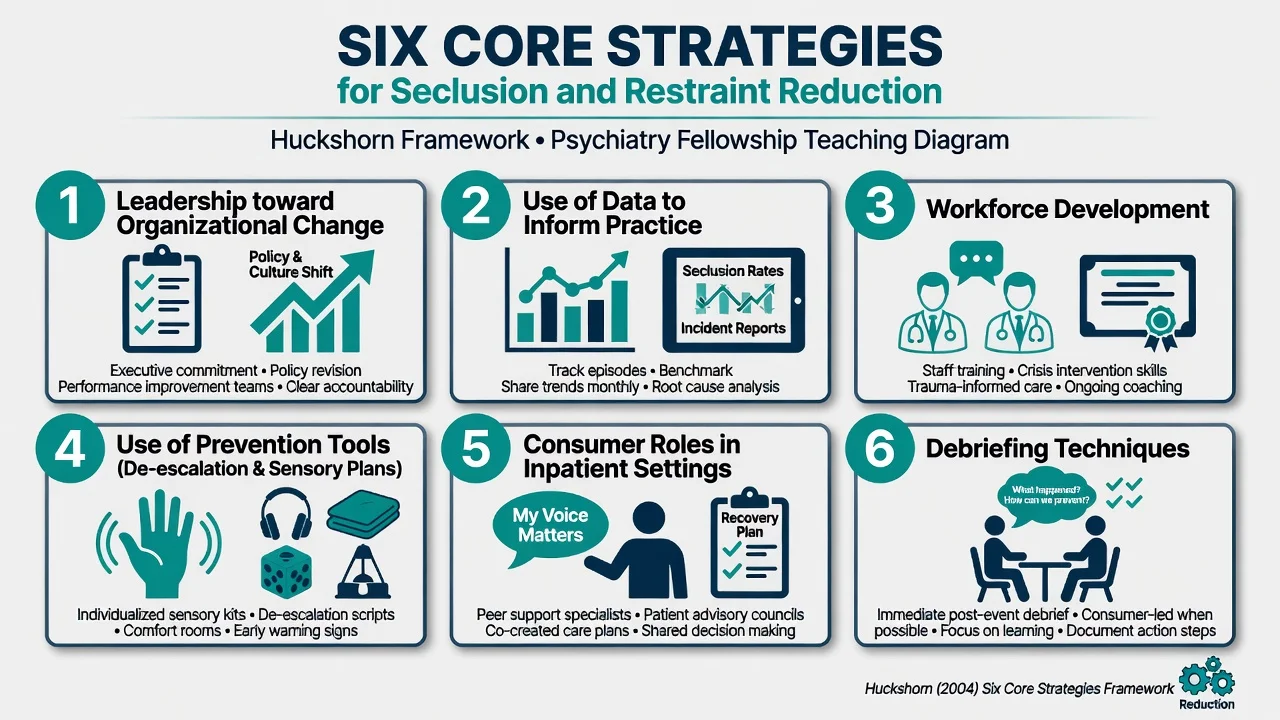
Huckshorn's Six Core Strategies for reducing seclusion and restraint are: (1) leadership toward organisational change; (2) use of data to inform practice; (3) workforce development; (4) use of prevention tools (risk formulation, de-escalation, sensory and environmental design, collaborative crisis plans); (5) consumer roles in inpatient settings; and (6) debriefing techniques for patient and staff with rigorous event analysis.[3]
Multisite implementation study of this evidence-based practice demonstrated reductions in seclusion and restraint in psychiatric inpatient facilities when the package is actually implemented — not laminated and ignored.[4] Multinational experience papers reinforce that reduction is a systems problem, not a personal moral failing of individual nurses.[16]
Safewards
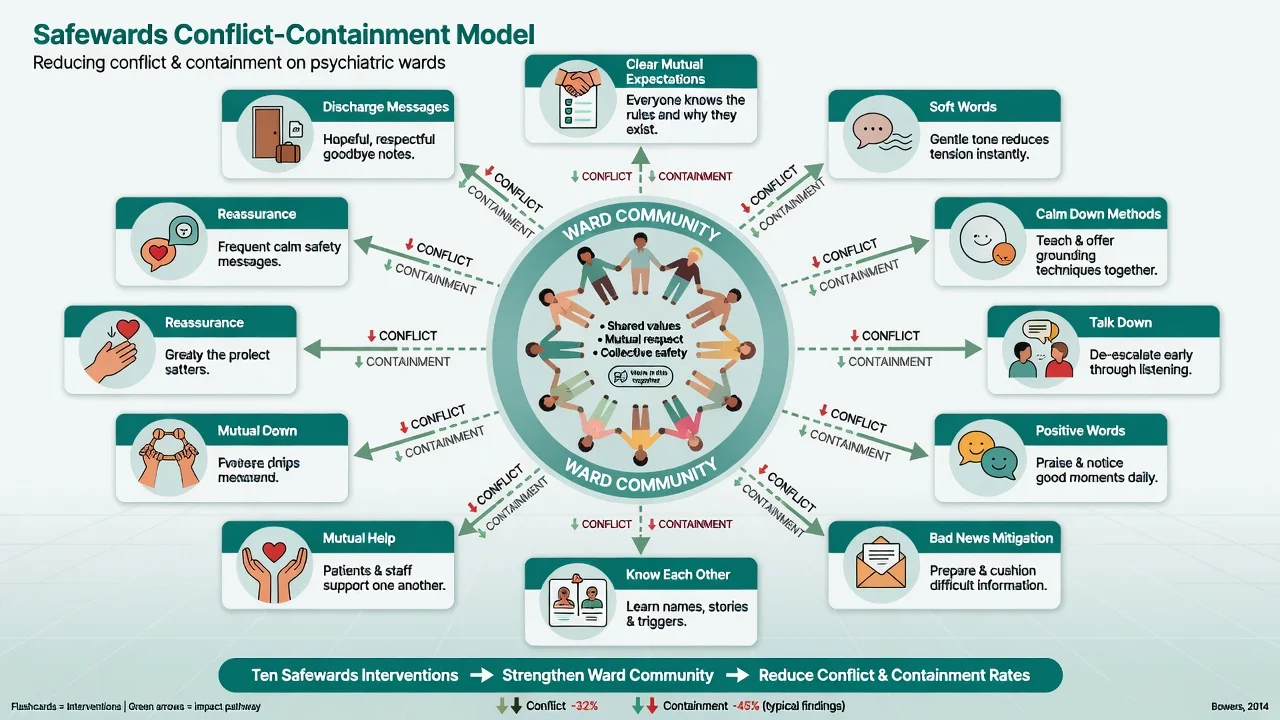
Bowers' Safewards model theorises how staff modifiers can interrupt the cascade from flashpoints to conflict to containment on acute wards.[6] The Safewards cluster randomised controlled trial found that implementing the interventions reduced conflict and containment rates compared with control wards — a rare experimental foothold in a field often limited to before-after quality projects.[5]
Trauma-informed and rights-based practice
Assume high prevalence of trauma; minimise coercive process; explain; offer choices within safety limits; involve peer workers and families where appropriate; repair alliance after any force. Perceived coercion is shaped by process, not only legal paperwork.[10][11][12] Cultural safety strategies matter where Indigenous seclusion rates are elevated.[18]
Treat the illness aggressively and kindly
The best "anti-seclusion" intervention is often effective treatment of psychosis, mania, delirium, withdrawal, pain, and akathisia — plus enough skilled staff and a physical environment that does not manufacture flashpoints.[5][9]
Subtypes and scenarios
| Scenario | Fellowship focus |
|---|---|
| Adult acute ward | Six Core Strategies + Safewards; debrief every episode |
| ED | Project BETA avoidance; medical clearance; RT protocols |
| Forensic | Dual security-clinical policy; transparency of indication |
| Child/adolescent | Developmental communication; family; reduction methods review |
| ID / autism | PBS and sensory strategies; seclusion must not be the behaviour plan |
| Older adult | Delirium first; restraint high morbidity; falls and frailty |
| Pregnancy | Avoid prolonged prone; obstetric liaison; drug teratogenicity awareness |
| Indigenous | Equity audit of rates; cultural support; co-designed reduction |
Complications and pitfalls
- Death, injury, rhabdomyolysis, aspiration, VTE, psychological trauma.[1]
- Seclusion as punishment or staffing shortcut.
- Under-reporting that creates fake reduction curves.
- Invented legal maxima or section numbers in exams.
- No exit criteria; multi-day seclusion without relentless senior review.
- Skipping debrief — same flashpoint repeats tomorrow.
- Confusing voluntary quiet room statistics with seclusion rates.[15]
Prognosis and disposition after an episode
Most episodes should be brief. Prolonged restriction is a clinical governance alarm. After release: medical check; step-down observation; revise formulation and care plan; address triggers (noise, crowding, medication side-effects, interpersonal conflict); offer patient narrative space; staff support and learning review. Organisational prognosis is favourable where leadership sustains Six Core Strategies and Safewards-type work; PA system data and multisite studies support feasibility of major reduction.[4][5][13]
Alliance repair after coercion predicts future help-seeking; process quality determines whether patients later judge force as necessary or abusive.[11][12]
Special populations
Children and adolescents. Higher developmental and trauma sensitivity; family inclusion; specific reduction literature is growing though still underdeveloped relative to adult systems.[17]
Older adults. Delirium and medical drivers first; mechanical restraint for "wandering" is high-harm low-value; falls and aspiration risk soar — physical complications of restraint are a core theme of harm reviews.[1][7]
Intellectual disability / autism. Positive behaviour support, sensory modulation, and communication access first; seclusion as chronic behaviour management is a red flag in reduction and special-population literature.[16][17]
Pregnancy. Positional safety non-negotiable (avoid prolonged prone); pharmacology and obstetrics jointly planned when restrictive practices or parenteral sedation are considered.[1][7]
Indigenous peoples. Cultural safety, whānau/family inclusion, and equity monitoring of restrictive practice rates are clinical duties.[18]
Evidence and guidelines (named)
- Chieze et al., 2019 — systematic review of effects of seclusion and restraint in adult psychiatry: significant adverse effects; last-resort framing.[1]
- Sailas and Fenton, Cochrane — insufficient evidence of therapeutic benefit of seclusion/restraint for serious mental illness.[2]
- Huckshorn Six Core Strategies; Wieman et al. multisite reduction outcomes.[3][4]
- Safewards model + cluster RCT (Bowers and colleagues).[5][6]
- Project BETA consensus on seclusion/restraint avoidance and verbal de-escalation.[7][8][9]
- Smith et al., 2023 — ending seclusion and mechanical restraint in PA state hospitals.[13]
- Atdjian and Huckshorn, 2024 — regulatory call toward cessation.[14]
- Muluneh et al. — definition variation of restrictive practices.[15]
ANZ: Apply local Mental Health Act principles, health service seclusion/restraint standards, and RANZCP ethical framing; report and review episodes under local quality systems; cultural equity for Aboriginal and Torres Strait Islander and Māori peoples is non-optional.[18] UK: NICE violence and aggression guidance principles — prevention, de-escalation, restrictive interventions as last resort with governance (pair with Safewards-type ward work).[5] US: CMS/Joint Commission restraint and seclusion rules are detailed and punitive for non-compliance; Project BETA is high-yield ED language.[7][9] India/MD-DNB: Principles of least restriction and documentation under local mental health legislation — do not import foreign section numbers; teach purpose, monitoring, and debrief as universal clinical standards.[1][10]
Exam pearls
References
- [1]Chieze M, Hurst S, Kaiser S, et al. Effects of Seclusion and Restraint in Adult Psychiatry: A Systematic Review Front Psychiatry, 2019.PMID 31404294
- [2]Sailas E, Fenton M Seclusion and restraint for people with serious mental illnesses Cochrane Database Syst Rev, 2000.PMID 10796606
- [3]Huckshorn KA Reducing seclusion restraint in mental health use settings: core strategies for prevention J Psychosoc Nurs Ment Health Serv, 2004.PMID 15493493
- [4]Wieman DA, Camacho-Gonsalves T, Huckshorn KA, et al. Multisite study of an evidence-based practice to reduce seclusion and restraint in psychiatric inpatient facilities Psychiatr Serv, 2014.PMID 24292685
- [5]Bowers L, James K, Quirk A, et al. Reducing conflict and containment rates on acute psychiatric wards: The Safewards cluster randomised controlled trial Int J Nurs Stud, 2015.PMID 26166187
- [6]Bowers L Safewards: a new model of conflict and containment on psychiatric wards J Psychiatr Ment Health Nurs, 2014.PMID 24548312
- [7]Knox DK, Holloman GH Jr Use and avoidance of seclusion and restraint: consensus statement of the American Association for Emergency Psychiatry Project BETA seclusion and restraint workgroup West J Emerg Med, 2012.PMID 22461919
- [8]Richmond JS, Berlin JS, Fishkind AB, et al. Verbal De-escalation of the Agitated Patient: Consensus Statement of the American Association for Emergency Psychiatry Project BETA De-escalation Workgroup West J Emerg Med, 2012.PMID 22461917
- [9]Holloman GH Jr, Zeller SL Overview of Project BETA: Best practices in Evaluation and Treatment of Agitation West J Emerg Med, 2012.PMID 22461914
- [10]Newton-Howes G, Mullen R Coercion in psychiatric care: systematic review of correlates and themes Psychiatr Serv, 2011.PMID 21532070
- [11]Katsakou C, Rose D, Amos T, et al. Psychiatric patients' views on why their involuntary hospitalisation was right or wrong: a qualitative study Soc Psychiatry Psychiatr Epidemiol, 2012.PMID 21863281
- [12]Lidz CW, Hoge SK, Gardner W, et al. Perceived coercion in mental hospital admission. Pressures and process Arch Gen Psychiatry, 1995.PMID 7492255
- [13]Smith GM, Altenor A, Altenor RJ, et al. Effects of Ending the Use of Seclusion and Mechanical Restraint in the Pennsylvania State Hospital System, 2011-2020 Psychiatr Serv, 2023.PMID 35855620
- [14]Atdjian S, Huckshorn KA Toward the Cessation of Seclusion and Mechanical Restraint Use in Psychiatric Hospitals: A Call for Regulatory Action Psychiatr Serv, 2024.PMID 37461820
- [15]Muluneh ZB, Chavulak J, Lee DA, et al. Variations in definitions used for describing restrictive care practices (seclusion and restraint) in adult mental health inpatient units: a systematic review Soc Psychiatry Psychiatr Epidemiol, 2025.PMID 39080007
- [16]LeBel JL, Duxbury JA, Putkonen A, et al. Multinational experiences in reducing and preventing the use of restraint and seclusion J Psychosoc Nurs Ment Health Serv, 2014.PMID 25310674
- [17]Perers C, Bäckström B, Johansson BA, et al. Methods and Strategies for Reducing Seclusion and Restraint in Child and Adolescent Psychiatric Inpatient Care Psychiatr Q, 2022.PMID 33629229
- [18]Wharewera-Mika J, Cooper E, Wiki N, et al. Strategies to reduce the use of seclusion with tāngata whai i te ora (Māori mental health service users) Int J Ment Health Nurs, 2016.PMID 27219838