Psych · public-community
Telepsychiatry
Also known as Telemental health · Videoconferencing psychiatry · Virtual psychiatry · Remote psychiatric consultation · Asynchronous telepsychiatry · Synchronous telepsychiatry · Store-and-forward psychiatry · e-Psychiatry · Digital psychiatry telehealth · Tele-mental health
Exam-exhaustive fellowship reference on telepsychiatry: modality taxonomy, effectiveness evidence, videoconferencing process standards, emergency and risk protocols, equity and digital exclusion, ethics and jurisdiction, primary-care integration, paediatric and forensic interfaces, and COVID-era scale-up lessons. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
1. Definitions and classification
Telepsychiatry is psychiatrist-delivered (or psychiatry-service-delivered) care using telecommunications technology. Broader telemental health includes psychology, counselling, and digital self-help. Nosology remains DSM-5-TR / ICD-11; what changes is medium, process safety, and system design.[1][7]
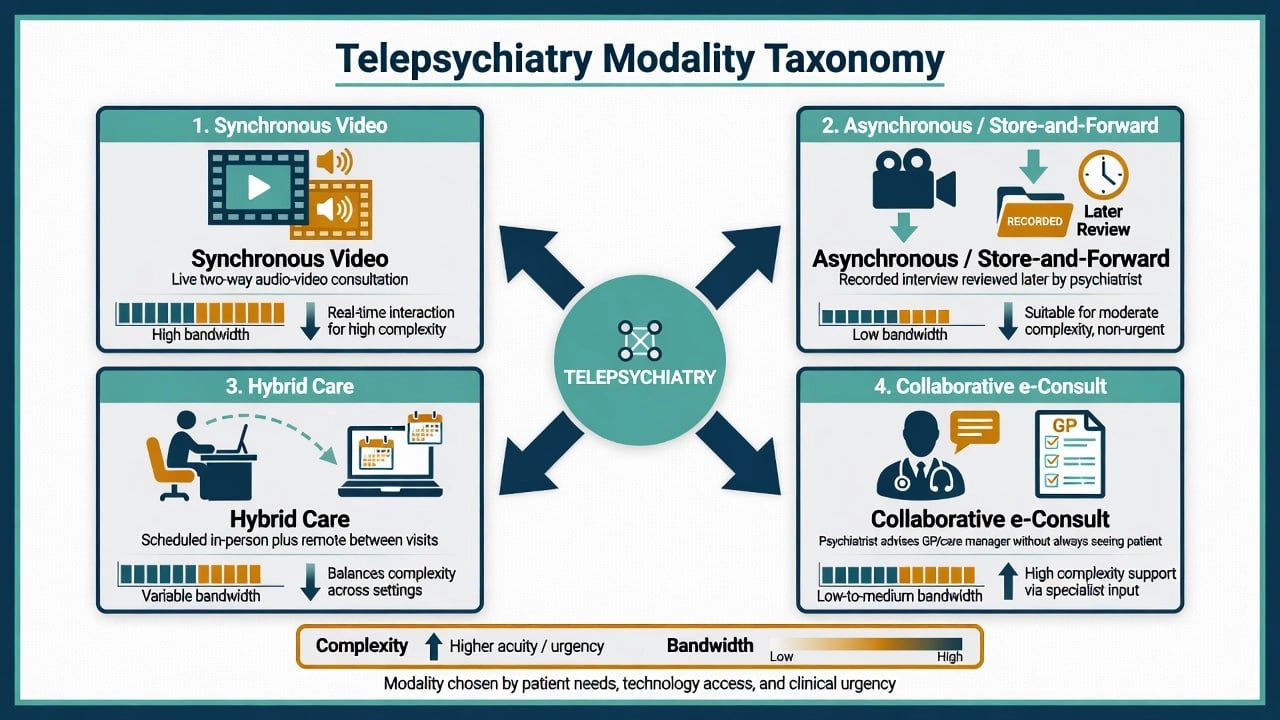
Modality taxonomy (viva must-state)
| Modality | Core feature | Exam use-case |
|---|---|---|
| Synchronous video | Live two-way audio-video | Default for diagnostic interviews, risk work, most therapy/med reviews |
| Telephone-only | Audio without video | Backup when video fails; limited MSE observation |
| Asynchronous / store-and-forward | Recorded interview reviewed later | Primary-care workflows; scheduling constraints; Yellowlees RCT support |
| Hybrid | Scheduled face-to-face + remote between visits | Complex illness needing periodic physical exam or alliance deepening |
| Collaborative e-consult | Psychiatrist advises GP/care manager | Measurement-based primary care without every patient on video |
| Modality choice should match acuity, complexity, and bandwidth rather than convenience alone; async and sync options are both evidence-supported in primary care when workflows fit.[6][7] |
Yellowlees and colleagues' RCT of asynchronous versus synchronous telepsychiatry in primary care supports both models as clinically viable when matched to workflow — do not dismiss async as "second class" by default.[6] Hubley and colleagues synthesised key telepsychiatry outcomes (satisfaction, reliability, clinical outcomes, access) that underpin board-level claims of effectiveness and acceptability.[7]
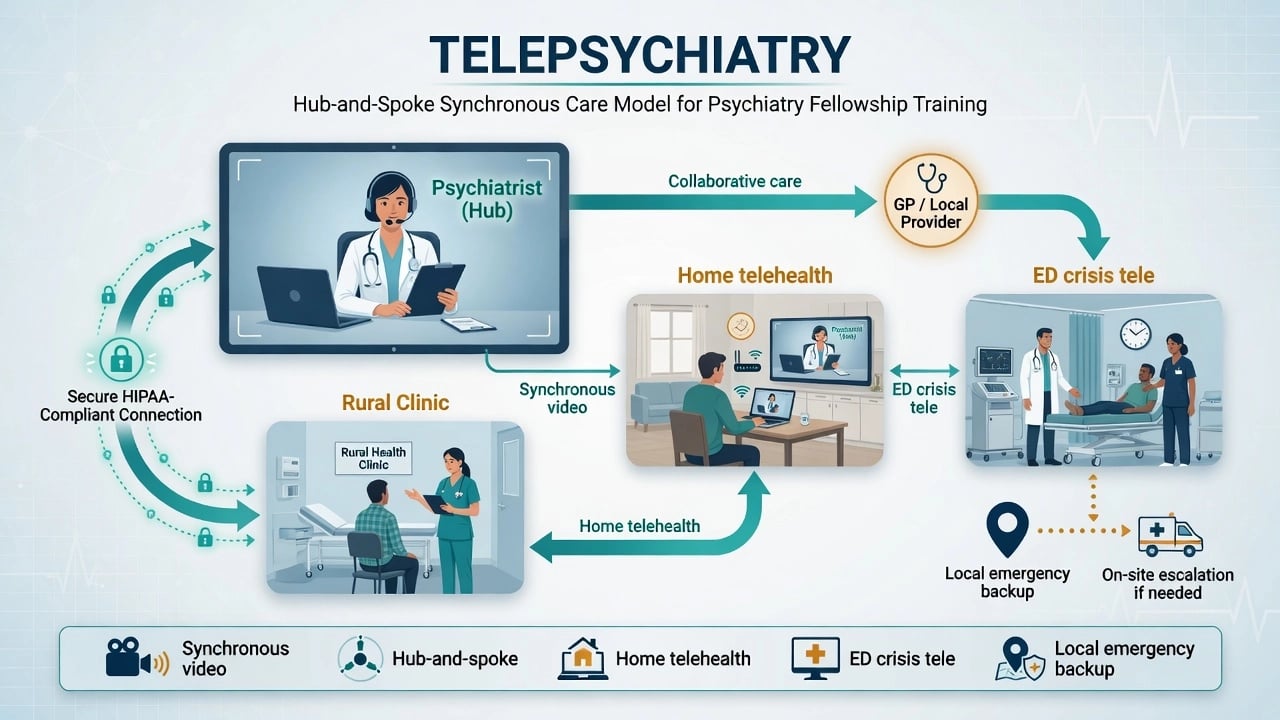
Setting taxonomy
Clinic-to-clinic hub-and-spoke; home-based video; ED/crisis telepsychiatry; inpatient consultation-liaison to distant hospitals; forensic/custody evaluation; collaborative care consultation embedded in primary care.[4][14]
2. Epidemiology, access, and scale-up
Large treatment gaps mean many people with mental disorders receive no care; telepsychiatry is one lever against scarcity and maldistribution of specialists, not a cure for social determinants alone.[16][4]
Telepsychiatry viva anchors
These anchors summarise the effectiveness, process-standard, primary-care integration, modality-choice, COVID scale-up, and ethics evidence base used in viva answers.[1][2][3][5][6][8][10]
COVID-19 forced a global pivot: mental health services were disrupted and many systems transitioned rapidly to telepsychiatry and remote care, with literature reviews documenting both operational feasibility and implementation strain.[8][9] Exam takeaway: scalability is proven; equity and quality control are not automatic.
3. Mechanisms of benefit and failure
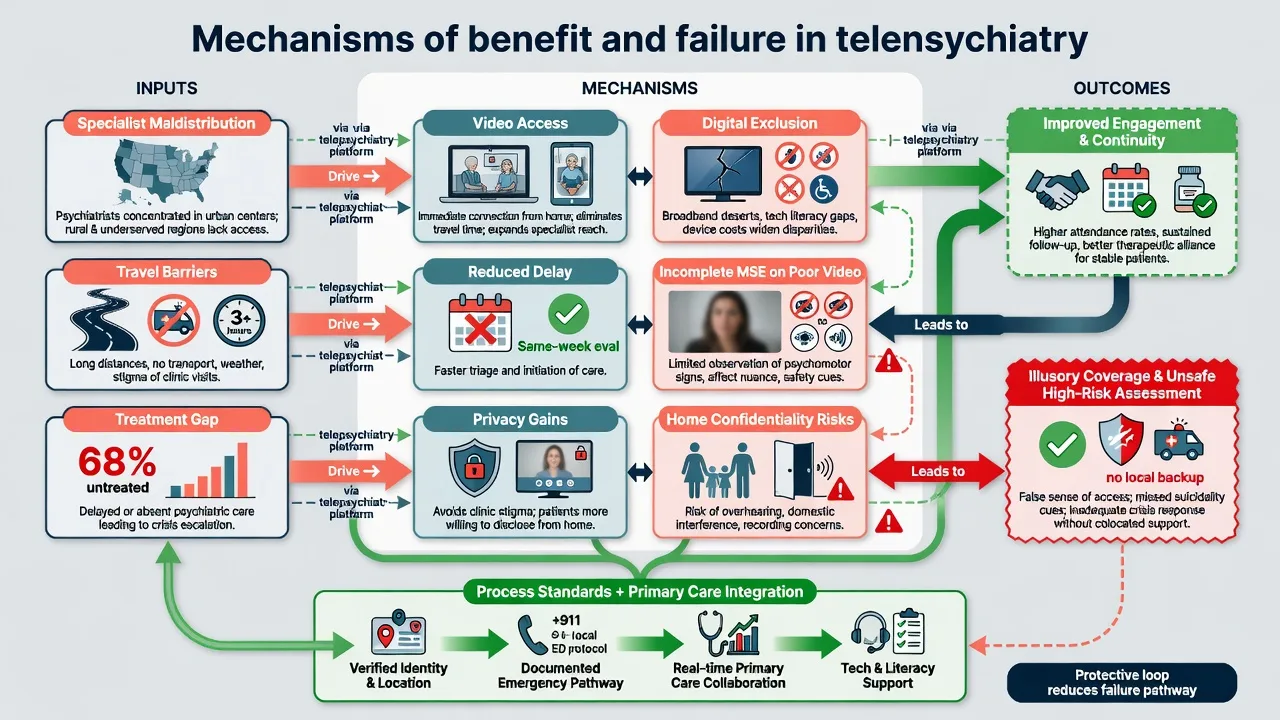
Benefit pathways. Reduced travel and time costs; shorter waits for specialist input; continuity between visiting clinics; primary-care integration that multiplies scarce psychiatrist time.[1][4][11]
Failure pathways. Incomplete MSE when video freezes or framing hides psychomotor signs; home confidentiality failures (family off-camera); emergency response impossible if address unknown; digital exclusion recreating the treatment gap under a modern label.[2][3][10]
Protective loop. Process standards (identity, location, emergency pathway) plus primary-care ownership and care management convert video into safe service design.[2][3][4]
4. Clinical presentation via tele
Presentations are the same syndromes (depression, psychosis, bipolar, anxiety, substance, trauma). The medium changes observation quality and safety process. Expect home environments, variable lighting, partial views, and third parties in the room — document these as assessment limits rather than ignoring them.[2][7]
Tele-MSE specifics. Confirm identity and location first. Frame camera for face and, when needed, full body (agitation, EPS, self-harm marks). Ask explicitly about weapons, medications in reach, substances, and who can overhear. If quality collapses mid-risk assessment, convert to phone backup only as a bridge while activating local safety — do not invent certainty you cannot observe.[2][3]
5. Differential and suitability traps
| Trap | Correct frame |
|---|---|
| "Looks fine on video" equals low risk | Risk formulation still needs intent, plan, means, supports, and local context |
| Poor video = "non-compliant patient" | Tech failure is a system problem; reschedule or convert modality |
| Any patient can be tele-managed | Medical instability, uncontrolled agitation, need for physical exam may mandate in-person/ED |
| Async is always inferior | Match to complexity and workflow (Yellowlees) |
| Tele diagnosis replaces investigations | Labs/ECG still local responsibilities before many psychotropics |
| Suitability traps matter because incomplete observation, tech failure, and missing investigations can be misread as low clinical risk or patient non-compliance.[2][6][7] |
Clinical differential (organic vs substance vs primary psychiatric) is unchanged by medium; process suitability is the additional layer examiners test.[2][6][7]
6. Assessment structure and process standards
Shore and colleagues' 2018 best-practice document for videoconferencing-based telemental health remains the process language examiners recognise: technology, clinical environment, emergency management, and documentation.[2] Mishkind and colleagues' 2024 resource document updates synchronous videoconferencing best practices for contemporary practice — cite the lineage, not a brand of software.[3]
Pre-session checklist (memorise). Identity and date of birth; exact address and callback number; emergency contacts; nearest ED/police pathway; privacy (alone? headphones? door closed?); technology test; call-drop reconnection plan; who is physically present.[2][3]
Consent for modality. Benefits, limits of remote observation, emergency plan, recording policy, third-party presence, and alternative in-person options where available.[10]
Scales. PHQ-9, GAD-7 and similar tools remain usable remotely when literacy and language allow; collaborative care depends on measurement-based follow-up, not one-off scores as suicide predictors.[4][5]
7. Investigations and monitoring logistics
Tele-review does not replace baseline metabolic panels, ECG when indicated, pregnancy testing, or clozapine/lithium monitoring. Name the local pathway (GP pathology, pharmacy, result escalation) before initiating high-monitoring agents. Neurological red flags on tele (new focal signs, severe cognitive change, fever with rigidity concern) lower the threshold for in-person ED work-up.[4][2]
Forensic tele-evaluations carry additional scrutiny of method reliability and documentation of limitations — Recupero's Daubert-focused discussion is the high-yield forensic interface paper for board stems.[15]
8. Acute and emergency management
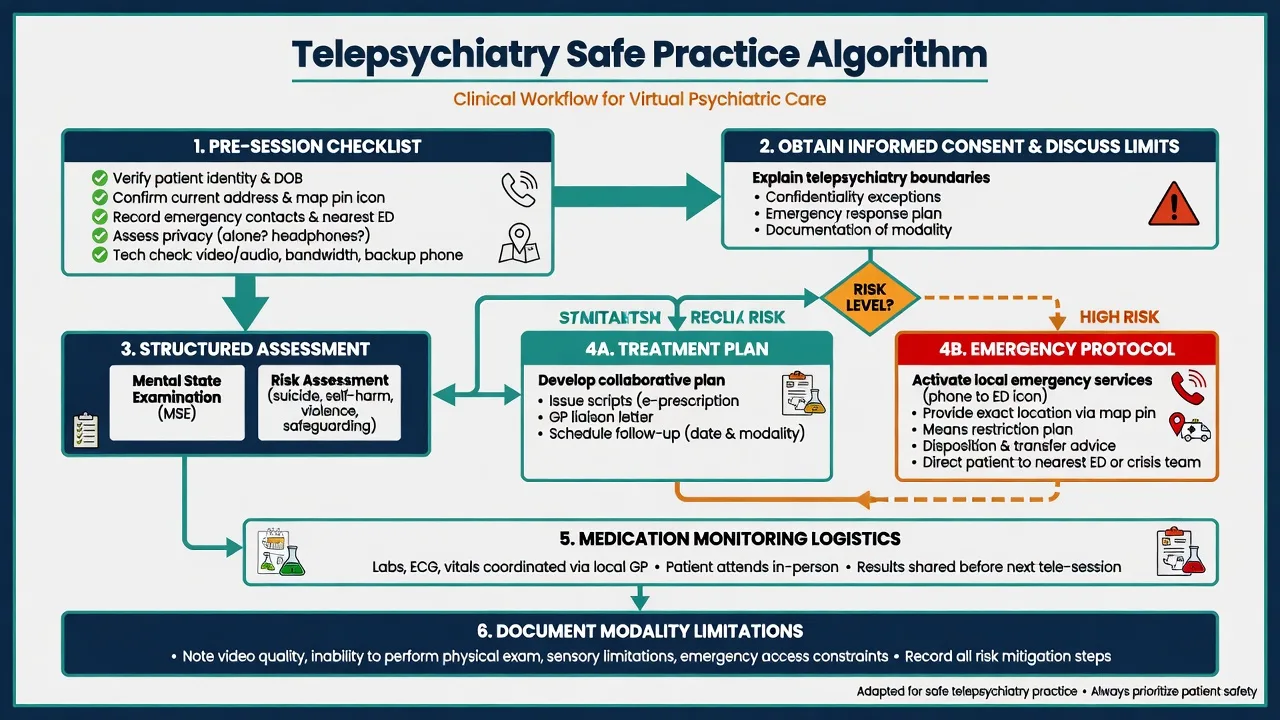
Local ED package with tele support. Medical clearance, environmental safety, observation level, means restriction plan, legal status advice appropriate to jurisdiction, and disposition (home with plan vs admit/transfer).[2][14]
Paediatric emergency telepsychiatry. Prospective programme data support urgent child and adolescent mental health delivery via telepsychiatry when embedded in ED/urgent pathways — developmental MSE, caregiver presence, and safeguarding remain mandatory.[14]
9. Definitive management and service design
Effectiveness and outcomes
Hilty and colleagues' 2013 review synthesised evidence that telemental health is effective across many diagnostic groups and can improve access, with diagnostic reliability broadly comparable to in-person care in well-designed systems.[1] Hubley's outcomes review reinforces satisfaction, clinical outcome, and access domains as the evidence pillars candidates should name.[7]
Synchronous standards
Use Shore 2018 and Mishkind 2024 as the process backbone for technology, environment, emergencies, and documentation — examiners prefer named standards over "we use Zoom carefully."[2][3]
Asynchronous and hybrid models
Yellowlees RCT: async and sync telepsychiatry in primary care can achieve clinical outcomes that support both as service options when workflows and staffing fit.[6] Hybrid care preserves periodic face-to-face depth for complex illness while using remote contact for interim risk checks and medication titration support.
Primary care integration and collaborative models
Fortney and colleagues describe telepsychiatry integration into rural primary care as a capacity and equity strategy when relocating specialists is not feasible.[4] The SPIRIT pragmatic comparative-effectiveness trial found teleintegrated care (collaborative care with telepsychiatry) and telereferral models both clinically relevant approaches for complex psychiatric disorders in primary care, with integrated models addressing care-manager workflows and measurement-based processes that simple referral often lacks — examiners expect the model names and the primary-care frame.[5] Clinician experience work on telepsychiatry collaborative care for PTSD and bipolar disorder highlights care-manager cadence and consultation structure as the operational core.[12] Queensland's Virtual Integrated Practice (VIP) pilot shows an Australian partnership model supporting rural general practice with virtual specialist input — useful FRANZCP systems language.[13]
Prescribing via tele
Same evidence-based agents and monitoring rules as in-person care. Practical exam points: arrange local labs before antipsychotics/mood stabilisers when indicated; avoid starting clozapine or lithium without named blood-monitoring contracts; LAIs still need local nursing capacity; controlled-substance and prescribing-authority rules are jurisdiction-specific. For alcohol withdrawal support via tele-advice to local teams, thiamine 100 mg orally or parenterally (route by severity and local protocol) remains part of Wernicke prevention packages delivered by the local site — tele does not replace bedside withdrawal care.[4][2]
Economics
Telepsychiatry cost analyses must account for technology, coordination time, no-shows, and travel averted — Hilty's economic cost analysis framework cautions against naive "tele is always cheaper" claims.[11]
10. Subtypes and scenarios
Home outpatient follow-up. Efficient for stable med reviews; privacy and domestic violence risk must be screened.[2]
Rural hub-and-spoke. Clinic-based video with local nurse/GP present improves vitals, collateral, and emergency response versus pure home video in high-risk cases.[4]
ED crisis tele. Short decision windows; lead structured risk and disposition with local team.[14]
Collaborative care e-consult. Psychiatrist multiplies impact through care managers for depression, PTSD, bipolar complexity without every patient on video.[5][12]
Child/adolescent. Developmental interview, caregiver role, school interfaces; emergency tele feasibility data exist.[14]
Forensic/custody. Security, privacy, recording, and method limitations for later legal scrutiny.[15]
11. Complications and pitfalls
Other traps: skipped emergency protocols; digital exclusion of older and poor patients; boundary blurring on personal devices; third parties off-camera; recording without consent; cross-border licensure errors; overclaiming alliance is always worse (or always equal) without nuance.[2][10][8]
12. Prognosis and disposition
Outcomes track model fidelity, continuity, care management, and equitable access more than platform brand. Disposition ladder: digital self-help adjuncts → GP collaborative care → tele-specialist → hybrid face-to-face → ED/inpatient with tele support → structured step-down with early post-discharge contact. Service KPIs: time-to-specialist, no-show rates, crisis conversion, 7-day follow-up, patient-reported access barriers.[5][7][11]
13. Special populations
Children/youth (developmental MSE, safeguarding); older adults (sensory/cognitive barriers, caregiver tech support); Indigenous and culturally diverse communities (interpreters, cultural brokers, small-community privacy); perinatal (home access vs face-to-face for high risk); intellectual disability (adapted communication, support person); forensic/custody; rural/remote stacking with retrieval pathways.[14][4][10]
14. Regional deltas
Australian answers should reference MBS-era telehealth norms, RANZCP telehealth practice expectations, rural workforce context, and models such as VIP supporting rural general practice.[13][4] Privacy law, state mental health acts, and emergency detention powers remain jurisdiction-specific even when advice is given by video.
15. Evidence map and controversies
Name at viva: Hilty 2013 (effectiveness); Hubley 2016 (outcomes domains); Shore 2018 and Mishkind 2024 (process standards); Yellowlees async vs sync RCT; Fortney rural integration and SPIRIT teleintegrated vs telereferral (JAMA Psychiatry); COVID transition reviews (Li; Duden); Sabin ethics framework; Hilty cost framework; Hoeft collaborative care experience; Lepre VIP; Roberts paediatric emergency tele; Recupero forensic Daubert considerations; Kohn treatment gap frame.[1][2][3][4][5][6][7][8][9][10][11][12][13][14][15][16]
Controversies for balanced answers: whether tele can substitute for rural training investment; async scope of practice; therapeutic alliance equivalence myths; home privacy vs access; forensic admissibility of remote evaluations; post-COVID hybrid sustainability and payment parity.[6][8][10][15]
16. Exam pearls
TELESAFE
Self-test: five viva openers
(1) Define telepsychiatry and name four modalities. (2) Run the pre-session emergency checklist. (3) Contrast teleintegrated care with bare telereferral (Fortney). (4) Summarise Yellowlees async vs sync. (5) List three ethical domains from Sabin-style frameworks (consent, privacy/confidentiality, jurisdiction/competence).[2][5][6][10]
References
- [1]Hilty DM, Ferrer DC, Parish MB, et al. The effectiveness of telemental health: a 2013 review Telemed J E Health, 2013.PMID 23697504
- [2]Shore JH, Yellowlees P, Caudill R, et al. Best Practices in Videoconferencing-Based Telemental Health April 2018 Telemed J E Health, 2018.PMID 30358514
- [3]Mishkind M, Shore JH, Barrett R, et al. Resource Document on Best Practices in Synchronous Videoconferencing-Based Telemental Health Telemed J E Health, 2024.PMID 38054938
- [4]Fortney JC, Pyne JM, Turner EE, et al. Telepsychiatry integration of mental health services into rural primary care settings Int Rev Psychiatry, 2015.PMID 26634618
- [5]Fortney JC, Bauer AM, Cerimele JM, et al. Comparison of Teleintegrated Care and Telereferral Care for Treating Complex Psychiatric Disorders in Primary Care: A Pragmatic Randomized Comparative Effectiveness Trial JAMA Psychiatry, 2021.PMID 34431972
- [6]Yellowlees PM, Parish MB, Gonzalez AD, et al. Clinical Outcomes of Asynchronous Versus Synchronous Telepsychiatry in Primary Care: Randomized Controlled Trial J Med Internet Res, 2021.PMID 33993104
- [7]Hubley S, Lynch SB, Schneck C, et al. Review of key telepsychiatry outcomes World J Psychiatry, 2016.PMID 27354970
- [8]Li H, Glecia A, Kent-Wilkinson A, et al. Transition of Mental Health Service Delivery to Telepsychiatry in Response to COVID-19: A Literature Review Psychiatr Q, 2022.PMID 34101075
- [9]Duden GS, Gersdorf S, Stengler K Global impact of the COVID-19 pandemic on mental health services: A systematic review J Psychiatr Res, 2022.PMID 36055116
- [10]Sabin JE, Skimming K A framework of ethics for telepsychiatry practice Int Rev Psychiatry, 2015.PMID 26493214
- [11]Hilty DM, Serhal E, Crawford A A Telehealth and Telepsychiatry Economic Cost Analysis Framework: Scoping Review Telemed J E Health, 2023.PMID 35639444
- [12]Hoeft TJ, Hall JD, Solberg LI, et al. Clinician Experiences With Telepsychiatry Collaborative Care for Posttraumatic Stress Disorder and Bipolar Disorder Psychiatr Serv, 2023.PMID 36444528
- [13]Lepre B, Job J, Martin Z, et al. The Queensland Virtual Integrated Practice (VIP) partnership program pilot study: an Australian-first model of care to support rural general practice BMC Health Serv Res, 2023.PMID 37907917
- [14]Roberts N, Hu T, Axas N, et al. Child and Adolescent Emergency and Urgent Mental Health Delivery Through Telepsychiatry: 12-Month Prospective Study Telemed J E Health, 2017.PMID 28426367
- [15]Recupero PR Daubert Considerations in Forensic Evaluations by Telepsychiatry J Am Acad Psychiatry Law, 2022.PMID 36175121
- [16]Kohn R, Saxena S, Levav I, et al. The treatment gap in mental health care Bull World Health Organ, 2004.PMID 15640922