Psych · Specialty psychiatry — eating disorders
Anorexia nervosa
Also known as AN · Anorexia · Restricting anorexia · Binge-purge anorexia · Atypical anorexia nervosa · Family-based treatment · FBT · MARSIPAN · MEED · Refeeding syndrome
Exam-exhaustive fellowship reference on anorexia nervosa — DSM-5-TR/ICD-11 criteria and BMI severity, medical complications, refeeding syndrome, FBT for adolescents, adult psychotherapies (CBT-E, MANTRA, SSCM), admission and MEED/MARSIPAN principles, capacity and compulsory care, and careful olanzapine adjunct evidence. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
6 MCQs with explanations
Target exams
Red flags
Anorexia nervosa (AN) is a high-stakes fellowship topic at the psychiatry–medicine interface. FRANZCP MEQs test admission thresholds, refeeding safety, therapy choice by age, and capacity. MRCPsych CASCs test explanation to patients and families and negotiation of nasogastric feeding plans. ABPN items test DSM severity, medical complications, and the limits of pharmacotherapy. A candidate who reads only this topic should defend diagnosis, medical risk, and stepped care at consultant depth.[2][3][17]
Overview and definition
AN is characterised by persistent energy restriction leading to significantly low body weight for age, sex, developmental trajectory and physical health; intense fear of gaining weight or persistent behaviour that interferes with weight gain; and disturbance in body weight/shape experience, undue influence of shape/weight on self-evaluation, or persistent lack of recognition of the seriousness of low weight.[2][3][17]
Clinical essence for viva. Starvation is both consequence and maintaining factor. Cognitive rigidity, overvaluation of thinness, and safety behaviours (restriction, purging, compulsive exercise, body checking) lock the disorder. Medical complications are multi-system and can kill while the patient minimises risk.[2][5]
DSM-5-TR placement. Feeding and eating disorders chapter. Specifiers: restricting versus binge-eating/purging type (last 3 months), and severity by adult BMI (mild to extreme). Insight and partial/full remission course descriptors are examinable. Amenorrhoea is no longer required for diagnosis (DSM-IV teaching trap).[2][17]
ICD-11. AN is defined by significantly low body weight and body image disturbance with behaviours preventing weight gain; always state which manual you are using when boundary cases (atypical AN, ARFID) are examined.[3]
Classification and severity
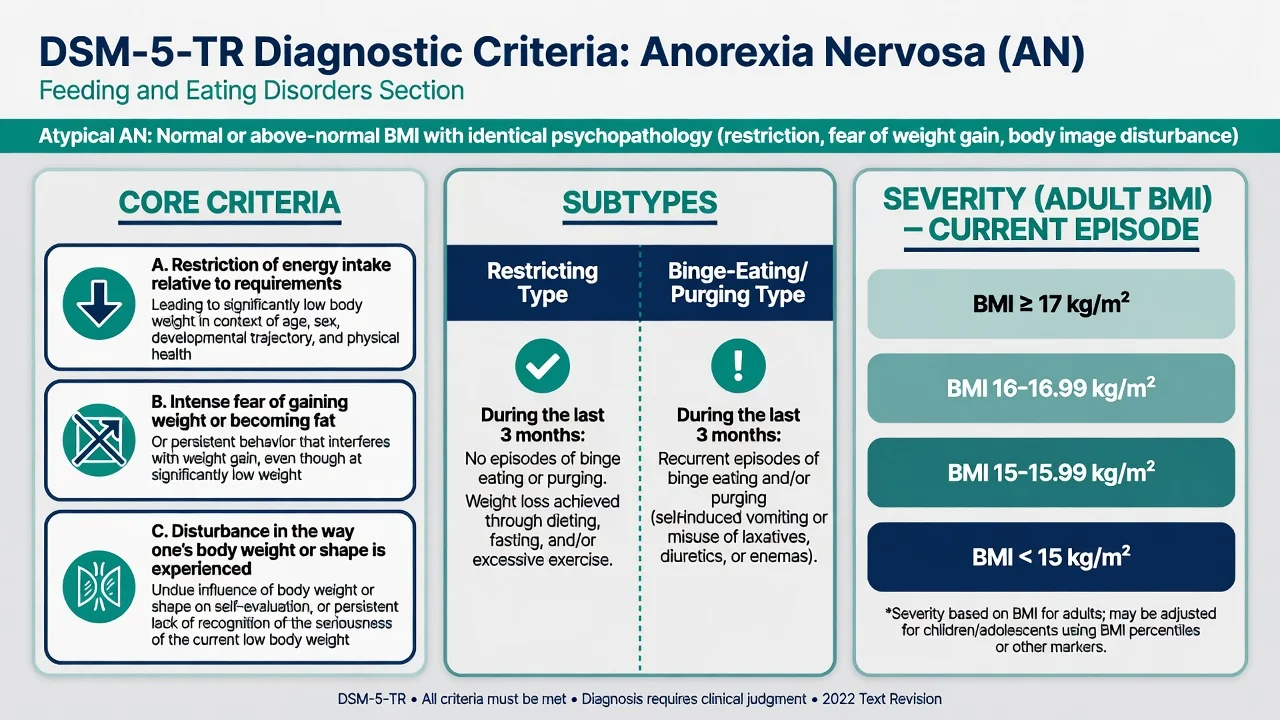
Core DSM-5-TR features
- Energy restriction → significantly low weight
- Fear of weight gain or interfering behaviours
- Body image disturbance or lack of seriousness recognition
- Amenorrhoea not required
Subtypes (3 months)
- Restricting: dieting, fasting, excessive exercise without binge/purge
- Binge-eating/purging: recurrent binge and/or purge (vomit, laxatives, diuretics)
- Still AN if underweight — not bulimia
- Subtype can switch over course
Adult BMI severity (exam bands)
- Mild: BMI ≥17 kg/m²
- Moderate: 16–16.99
- Severe: 15–15.99
- Extreme: BMI <15
Boundary diagnoses
- Atypical AN: same psychopathology, not underweight — still medical risk possible
- Bulimia nervosa: binge-purge at normal/overweight
- ARFID: restriction without shape/weight overvaluation
- Organic weight loss differentials
Severity by BMI is a current-episode specifier for adults; in children/adolescents use BMI centiles/growth charts. Clinical severity (rate of loss, cardiovascular instability, purging frequency, suicide risk) can exceed the BMI band — examiners punish BMI-only thinking.[2][8][17]
Epidemiology and risk factors
Headline epidemiology and risk (exam anchors)
Population data show AN is less common than bulimia or binge-eating disorder but carries disproportionate mortality and disability. Adolescent community cohorts using DSM-5 criteria still find AN and related presentations clinically important; under-recognition in males and in atypical AN at higher BMI is a modern teaching point.[23][24]
Meta-analysis of mortality in eating disorders found markedly elevated mortality in AN compared with other EDs, with medical complications and suicide as principal pathways — quote order-of-magnitude elevation rather than inventing a single SMR if not sure of the exact figure under exam stress, then cite Arcelus-order evidence.[1][26]
Risk factors examiners expect: genetic liability and family history of ED/mood/anxiety/OCD traits; perfectionism and cognitive rigidity; sociocultural thin ideals; elite sport/dance and weight-class pressures; early adversity; and iatrogenic reinforcement of dieting. Protective factors include early detection, family engagement, and access to evidence-based care.[2][3][4]
Pathophysiology
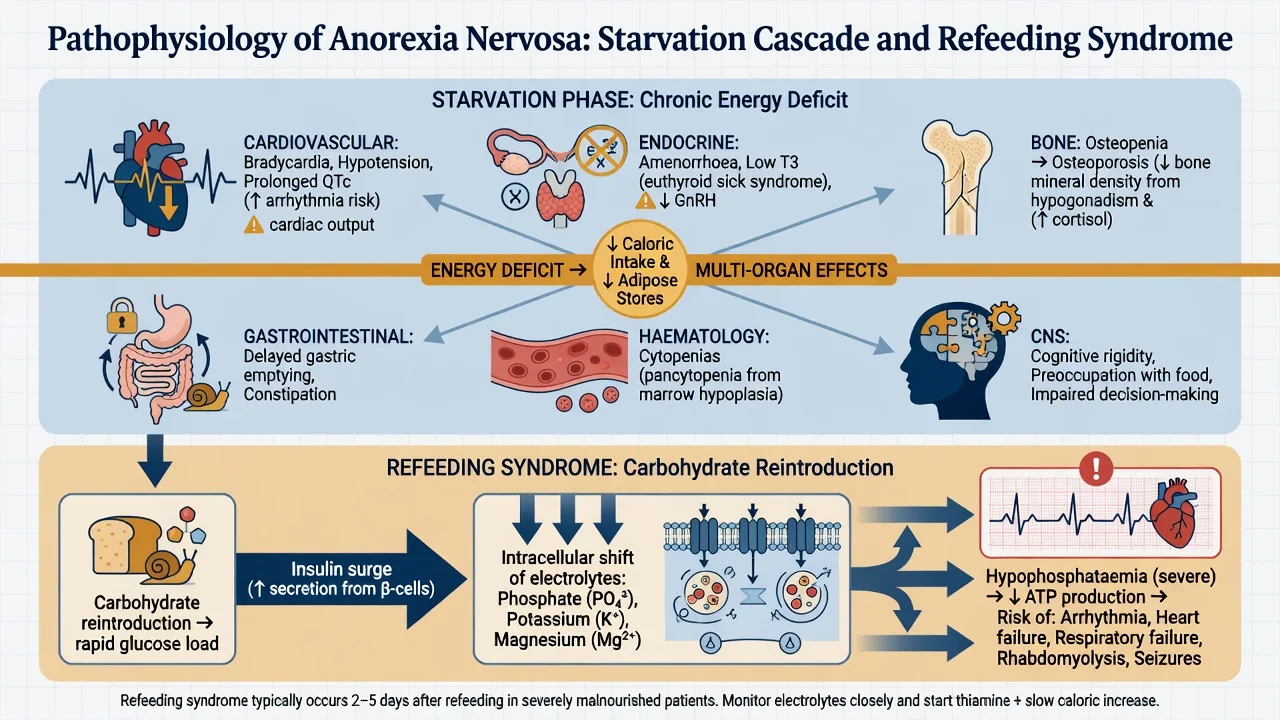
Starvation cascade. Chronic energy deficit reduces metabolic rate, cardiac output reserve, gonadotrophins (functional hypogonadism/amenorrhoea), and bone mineral density, and produces GI slowing, marrow suppression, and cognitive narrowing around food. These changes are largely consequences of malnutrition that improve with nutritional rehabilitation, though bone recovery can lag.[2][5][8]
Psychological maintaining model. Overvaluation of shape/weight drives dietary restraint; restraint plus life stress precipitates binge–purge cycles in some; checking, comparison, and compulsive exercise maintain fear. Family accommodation (meals adapted entirely around rituals) can maintain adolescent AN and is a therapy target in FBT.[2][9]
Refeeding syndrome mechanism. After prolonged restriction, carbohydrate reintroduction triggers insulin release, driving phosphate, potassium and magnesium intracellularly. Serum hypophosphataemia (with hypokalaemia/hypomagnesaemia) risks arrhythmia, cardiac failure, respiratory failure, rhabdomyolysis, delirium and seizures — typically early in refeeding in high-risk patients.[6][7]
Clinical presentation
Core behaviours: calorie counting, food group elimination, slow eating, hiding food, water loading before weigh-ins, compulsive exercise, laxative/diuretic/vomiting purging (binge-purge subtype), cold intolerance, constipation, dizziness, and social withdrawal around meals.[2][3]
Physical signs (bedside). Low BMI or rapid loss; bradycardia; orthostatic pulse/BP change; hypothermia; lanugo; dry skin; hair thinning; acrocyanosis; muscle wasting; parotid enlargement and dental enamel erosion if purging; Russell sign teaching if self-induced vomiting. Absence of cachexia does not exclude atypical AN with medical risk.[5][8]
MSE language. Preoccupation with food/shape; fear of fatness; minimisation of medical risk; possible depressive affect; anxiety at meal times; compulsive exercise planning; limited flexibility; preserved general cognition early but impaired concentration with starvation. Always assess suicide and self-harm.[1][2]
Atypical and high-yield presentations. Male AN (muscularity-oriented body image possible); elite athlete relative energy deficiency interface; later-onset; perinatal exacerbation; autistic sensory restriction overlapping AN psychopathology; chronic severe enduring AN (SE-AN) with long illness and prior treatment failure.[2][3]
Differential diagnosis
Bulimia nervosa
- Recurrent binge + compensatory behaviours
- Weight normal or overweight
- If underweight with binge/purge → binge-purge AN
- Different first-line therapy emphasis (CBT-ED)
ARFID
- Restriction from sensory/fear/interest
- No shape/weight overvaluation
- Can still cause malnutrition
- Different psychological targets
Organic weight loss
- IBD, coeliac, malignancy, hyperthyroid, DM1, Addison, TB, HIV
- Lack of fat-phobia structure
- Red-flag systemic symptoms
- Investigate before pure ED pathway
OCD / BDD / depression
- OCD: rituals not primarily weight control
- BDD: appearance defect focus not thinness goal
- Depression: appetite loss without fat phobia
- Comorbidity common — formulate both
Also discriminate stimulant misuse, chronic infection, and medication effects. Organic exclusion is mandatory when onset is late, progression is very rapid without psychological markers, or focal systemic signs are present.[2][8][17]
Clinical and bedside assessment
Structure: weight trajectory (highest, lowest, rate of recent loss); intake pattern; purge methods and frequency; exercise hours; menses/sexual function; prior treatments and admissions; trauma; substances; family accommodation; school/work function; suicide risk; medical red flags.[2][8]
Physical exam essentials. Height/weight/BMI (centiles in youth); sitting and standing HR/BP; temperature; hydration; cardiovascular exam; oedema (can appear in refeeding); skin/hair/teeth; neurological screen. Document exact vitals — vague “stable” fails viva.[5][8]
Capacity. Decision-specific (e.g. admission, nasogastric feeding, specific medication). Assess understanding, retention, weighing of risks/benefits, and communication of choice. Starvation and AN psychopathology can impair appreciation of medical risk without global “incompetence.” Statutes are jurisdiction-specific — name local Mental Health Act / guardianship frameworks; do not invent section numbers for another country.[20]
Investigations
Baseline (typical adult/adolescent set). FBC; U&E; phosphate; magnesium; calcium; LFT; glucose; TFT; ESR/CRP if organic concern; coeliac serology as indicated; pregnancy test when relevant; consider B12/folate, iron studies, vitamin D. ECG for bradycardia, conduction, QTc. Bone densitometry when prolonged underweight/amenorrhoea or recurrent fractures.[5][8][17]
Serial refeeding labs. Phosphate, potassium, magnesium (and clinical review) frequently in early refeeding of high-risk patients — protocols vary by unit; the exam principle is planned monitoring plus proactive replacement, not ad hoc reaction after arrhythmia.[6][7]
Neuroimaging only for atypical neurological features — not routine for classic adolescent AN.[2]
Management — resuscitation and medical emergency
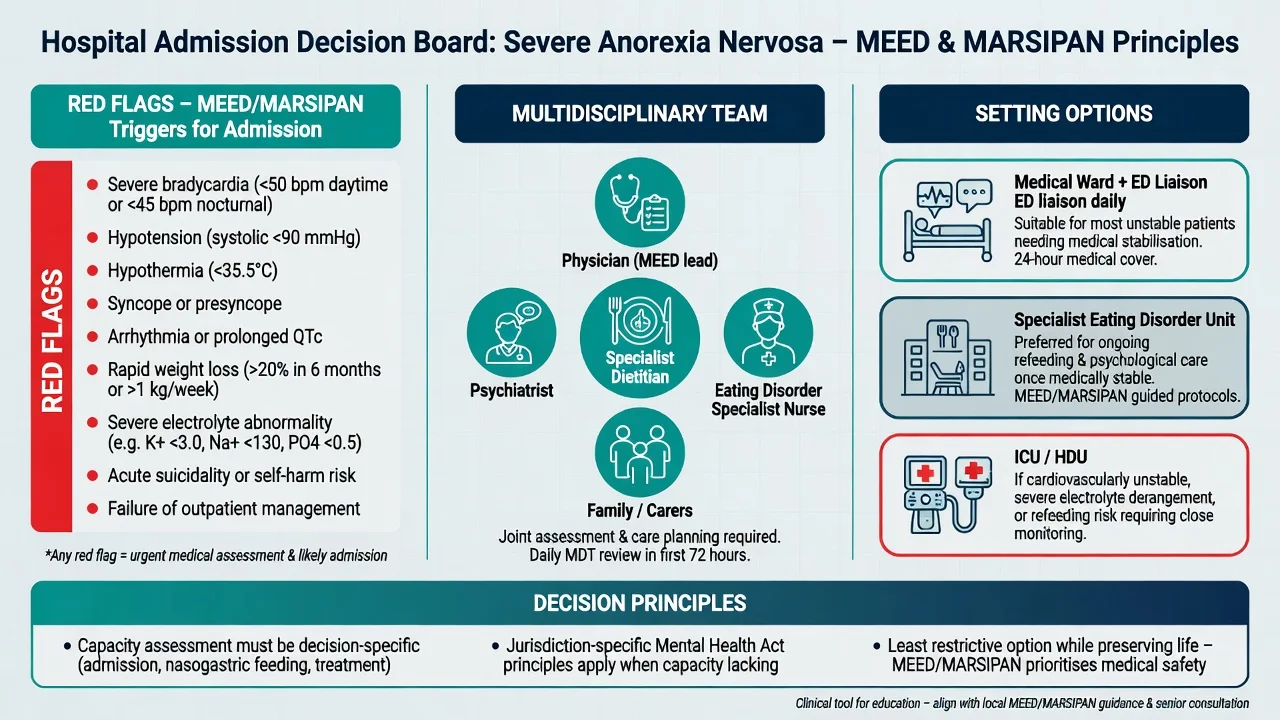
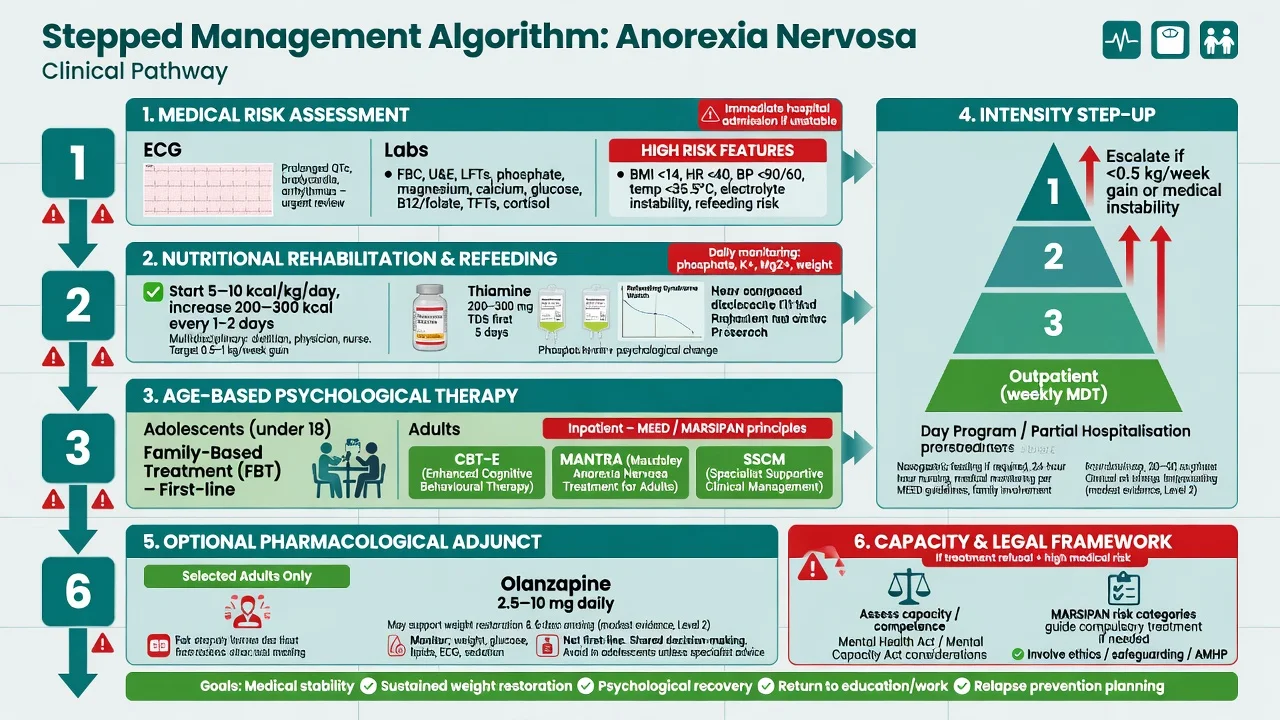
MEED / MARSIPAN principles (exam framing). UK guidance for the really sick patient with AN (MARSIPAN historically; MEED — Medical Emergencies in Eating Disorders — for adults in current UK practice language) emphasises: early recognition of medical risk; joint physician–psychiatrist–dietitian–nursing ownership; clear refeeding plans; appropriate ward setting (medical ward with ED liaison, specialist ED unit, HDU/ICU if needed); and escalation rather than false reassurance from a “normal” lab panel in a severely wasted patient.[21][22]
Australian/NZ practice aligns on medical stabilisation first, multidisciplinary care, and lawful frameworks for compulsory treatment when capacity and risk require it — cite local RANZCP-aligned clinical practice and hospital ED pathways in viva rather than memorising another country’s section numbers.[17][20]
Refeeding syndrome — prevention and treatment
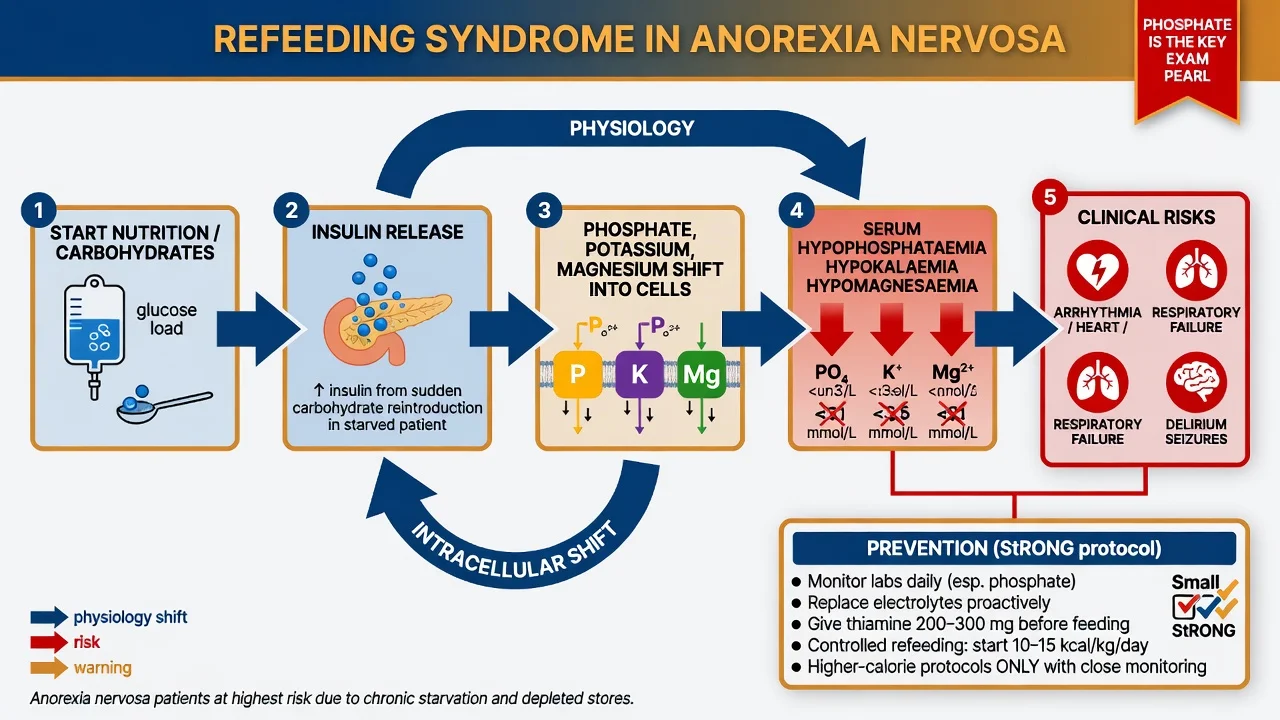
High-risk features. Very low BMI, rapid recent loss, little intake for days, pre-existing electrolyte abnormality, and medical comorbidity. Position statements highlight refeeding hypophosphataemia as a predictable complication in hospitalised adolescents with AN.[7][8]
Practical exam ladder. (1) Medical monitoring environment; (2) thiamine and multivitamin as per local protocol before/with refeeding; (3) structured nutrition plan (oral preferred if safe; nasogastric when indicated); (4) daily (or protocolised) phosphate/K/Mg with proactive replacement; (5) avoid unsupervised high-carbohydrate boluses; (6) watch fluid balance and oedema.[6][7][8]
Higher-calorie refeeding evidence. The StRONG randomised trial in hospitalised adolescents/young adults with AN found higher-calorie refeeding restored medical stability faster than lower-calorie approaches in the short term, with careful safety monitoring — exam stance: higher-calorie protocols are evidence-supported in selected inpatient youth when monitoring infrastructure exists, not a licence for unmonitored aggressive refeeding in a general ward without electrolyte surveillance.[6]
Exact kcal/kg start rates are protocol- and age-specific; quote your local MEED/hospital protocol under senior dietitian/physician guidance rather than inventing a universal number. Principle: planned increase, electrolyte vigilance, multidisciplinary review.[6][8][21]
Management — definitive and stepwise
Nutritional rehabilitation (core treatment)
Weight restoration and normalisation of eating are necessary for psychological recovery. Multidisciplinary team: physician, psychiatrist, dietitian, nursing, psychology, family. Individualise target weight/growth trajectory; restore menses often lags BMI; avoid colluding with under-fuelling “compromises” that leave the patient medically unsafe.[2][8][17]
Adolescents — family-based treatment (FBT)
FBT (Maudsley model) is first-line psychological treatment for most medically appropriate adolescents with AN. Parents are empowered to take charge of renourishment early (Phase 1), then control is returned to the adolescent (Phase 2), then adolescent developmental issues are addressed (Phase 3). Landmark RCT: Lock and colleagues showed FBT superior to adolescent-focused individual therapy for full remission at follow-up in adolescents with AN.[9][17]
Do not default adolescent AN to adult-style CBT-E alone without considering FBT access and family capacity. Hospital care may still be required for medical instability; FBT can resume/step down after stabilisation.[8][9]
Adults — CBT-E, MANTRA, SSCM
No single adult outpatient psychotherapy dominates all trials. Key evidence candidates are summarised below.[10][12][19]
| Approach | Core idea | Exam evidence anchor |
|---|---|---|
| CBT-E (enhanced CBT for ED) | Target overvaluation of shape/weight, restriction, binge-purge, body checking | Adult ED evidence base; weight restoration timelines studied in CBT-AN cohorts |
| MANTRA | Maudsley Model of AN Treatment for Adults — cognitive-interpersonal maintaining factors | MOSAIC trial lineage and follow-up comparing psychological treatments in adult outpatients |
| SSCM | Specialist Supportive Clinical Management — clinical management + supportive therapy, not “just chatting” | McIntosh three-psychotherapies RCT; long-term follow-up; SSCM definition papers |
Australian SWAN RCT compared three psychological treatments for AN and informs that structured specialist psychotherapies are deliverable options; network meta-analysis of adult outpatient psychological interventions synthesises comparative acceptability/efficacy with cautious interpretation.[12][19]
SSCM is a bona fide manualised approach combining AN-focused clinical management (weight, eating, medical risk) with supportive therapy elements — examiners may test that it is not unstructured generic support.[14]
Pharmacotherapy — careful, adjunctive, not primary
There is no first-line medication that replaces nutritional and psychological treatment for AN. Antidepressants (including fluoxetine) do not have a primary role for weight restoration in underweight AN; treat comorbid depression/anxiety carefully once nutritionally safer, watching activation and suicide risk.[17][25]
Olanzapine adjunct (must state evidence honestly). Earlier outpatient RCT suggested possible benefit versus placebo with tolerability considerations. The larger 2019 randomised trial (Attia et al., Am J Psychiatry) found olanzapine produced modestly greater BMI increase than placebo in adult outpatients with AN, without a corresponding large advantage on psychological AN symptom measures in the primary psychological outcome framing — sedation and metabolic effects matter. Exam stance: consider low-dose olanzapine as an adjunct in selected adults to support weight gain/anxiety around eating after shared decision-making, not as monotherapy, not a cure for psychopathology, and with monitoring of sedation, glucose/lipids, weight trajectory, and ECG context as clinically indicated. Example adult teaching range often discussed in literature and guidelines as low-dose oral titration (commonly starting in the low single-digit milligram range, e.g. 2.5 mg orally at night, individualising upward cautiously — verify local protocol and product information; Attia trial dosing was protocolised in the RCT).[15][16][17][25]
Other agents (e.g. anxiolytics for meal anxiety short-term) are symptomatic only; avoid benzodiazapine dependence patterns. Do not invent “AN-specific” high-dose SSRI algorithms from OCD teaching without evidence.[25]
Intensity of care and disposition
Step up when outpatient care fails, medical risk rises, or suicide risk requires containment: intensive outpatient / day programme → inpatient medical or specialist ED admission → residential step-down. Meta-review of ED treatments supports structured psychological and multi-level care rather than single-magic interventions.[17][18]
Specific subtypes and scenarios
Restricting vs binge-purge AN. Binge-purge subtype adds electrolyte, dental, parotid, and purging-substance risks (laxative/diuretic). Still diagnose AN if underweight — do not call it bulimia.[2][5]
Atypical AN. Normal/high BMI with AN psychopathology can still show bradycardia, electrolyte issues, and rapid loss from a higher baseline — medical risk assessment is clinical, not BMI-exclusive.[8][17]
Severe enduring AN (SE-AN). Long duration, multiple failed treatments, chronic medical risk. Goals may blend recovery-oriented care with harm reduction, quality of life, and ethical negotiation of compulsory care thresholds — not therapeutic nihilism.[2][20]
Compulsory treatment. When life-threatening AN meets incapacity criteria, lawful involuntary feeding/admission may be required. Discuss ethics of coercion, least restrictive option, second opinions, and legal process — Australian scholarship emphasises alignment of practice with guidelines and human rights framing.[20]
Complications and pitfalls
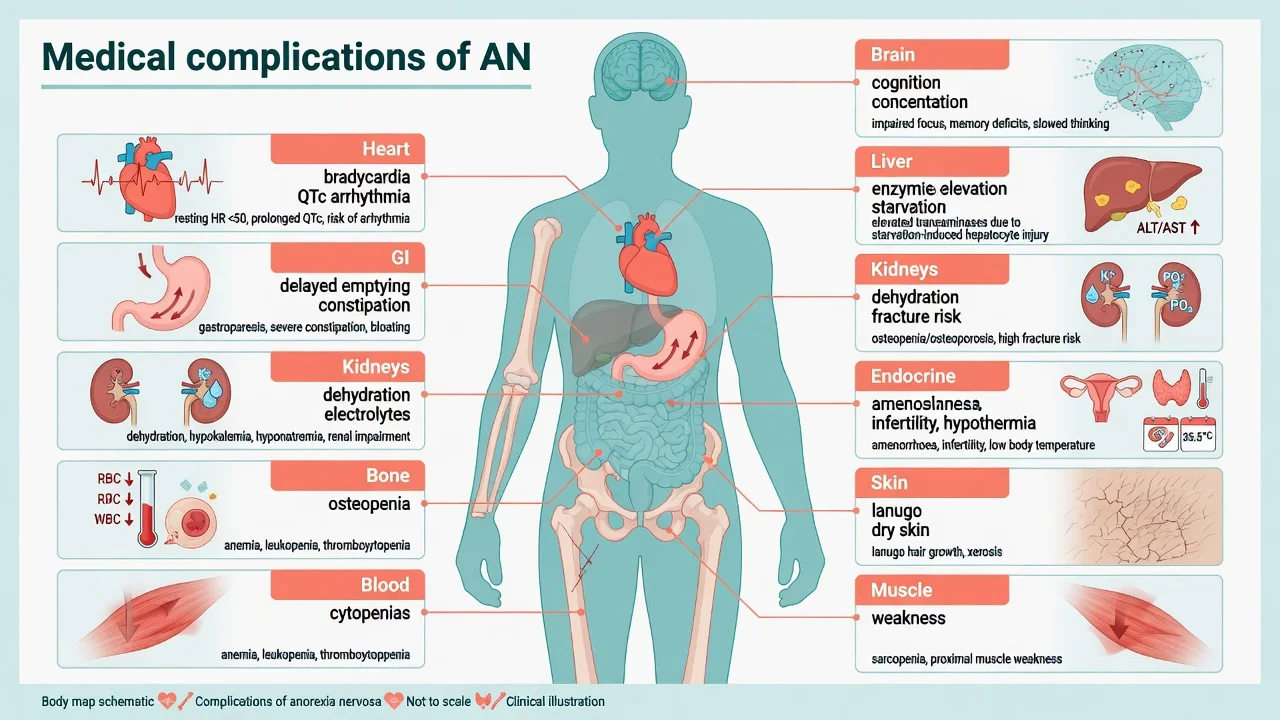
- Cardiac: bradycardia, hypotension, arrhythmia, QTc prolongation, sudden death risk especially with exercise when unstable.[5]
- Refeeding syndrome missed — phosphate is the classic trap.[6][7]
- Bone disease, infertility, growth failure in adolescents.[8]
- Suicide and self-harm under-assessed because the team focuses only on weight.[1]
- Pitfalls: colluding with dangerous exercise contracts; discharging while bradycardic; assuming capacity always intact; under-feeding from fear of refeeding without monitoring infrastructure; labelling all restriction as “lifestyle.”[8][20]
Prognosis and disposition
Many recover, especially with early intervention and family engagement in youth, but illness is often protracted and relapse is common after incomplete weight restoration. Mortality remains elevated years after presentation; ongoing risk monitoring matters.[1][23][26]
Disposition criteria: medical stability, adequate oral intake or safe plan, electrolyte stability, risk manageable, follow-up within days not months, bone/endocrine plan, school/work liaison, relapse signs taught to family (accelerating loss, purging return, SI, collapse).[8][17]
Special populations
Children/adolescents. Use growth charts; prioritise FBT; safeguarding if neglect or high-conflict feeding abuse dynamics; school meal plans; paediatric medical co-management.[8][9]
Pregnancy. Multidisciplinary obstetric–psychiatric–dietetic care; fetal growth risk; folate and nutrition; medication risk–benefit individualised.[3][17]
Males. Under-diagnosed; assess muscularity concerns and steroid misuse; same medical complications apply.[2]
Autism interface. Sensory eating vs shape overvaluation — both can co-exist; adapt therapy flexibility without abandoning renourishment goals.[2][3]
Athletes. Relative energy deficiency; involve sports medicine; return-to-play only when medically safe.[8]
Evidence, guidelines and regional differences
ANZ practice emphasises multidisciplinary ED services, medical stabilisation, FBT access for adolescents, and adult specialist psychotherapies (CBT-E/MANTRA/SSCM lineage). Compulsory treatment uses state/territory mental health and guardianship law — name the local Act. Align with RANZCP-informed clinical practice and hospital ED protocols; Australian literature on coercion stresses ethics, least restriction, and evidence-informed thresholds.[12][17][20]
Landmark trials to name. Lock FBT vs AFT (2010); McIntosh three psychotherapies (2005) and long-term follow-up; Byrne SWAN three treatments (2017); Schmidt MOSAIC MANTRA follow-up; Attia olanzapine RCTs (2011, 2019); Garber StRONG refeeding (2021); Arcelus mortality meta-analysis (2011).[1][6][9][10][12][13][15]
Exam pearls
- Amenorrhoea is not required for DSM-5-TR AN.[2]
- Underweight + binge/purge = binge-purge AN, not bulimia.[2]
- Phosphate is the refeeding exam answer; thiamine and K/Mg travel with it.[6][7]
- Adolescents → think FBT first, not adult CBT by default.[9]
- Adults → CBT-E / MANTRA / SSCM; no single universal winner.[12][19]
- Olanzapine: modest BMI effect in adult RCT; adjunct only; monitor metabolic/sedation; not a psychotherapy substitute.[15]
- Capacity is decision-specific; legal sections are jurisdiction-specific.[20]
- Highest ED mortality teaching → AN; pathways = medical + suicide.[1][26]
REFED-AN
Self-test: viva three-shot
Q1. Adult BMI severity bands for AN? A. Mild ≥17; moderate 16–16.99; severe 15–15.99; extreme <15 — plus clinical severity overrides.[2][17]
Q2. Why is phosphate central in week one of refeeding? A. Insulin-driven intracellular shift after carbohydrate load → hypophosphataemia → arrhythmia/heart failure/respiratory failure risk.[6][7]
Q3. Olanzapine role in adult AN? A. Adjunct with modest BMI gain evidence (Attia 2019); not first-line monotherapy; monitor metabolic/sedation; psychological care remains essential.[15]
References
- [1]Arcelus J, Mitchell AJ, Wales J, Nielsen S Mortality rates in patients with anorexia nervosa and other eating disorders. A meta-analysis of 36 studies Arch Gen Psychiatry, 2011.PMID 21727255
- [2]Zipfel S, Giel KE, Bulik CM, Hay P, Schmidt U Anorexia nervosa: aetiology, assessment, and treatment Lancet Psychiatry, 2015.PMID 26514083
- [3]Treasure J, Duarte TA, Schmidt U Eating disorders Lancet, 2020.PMID 32171414
- [4]Treasure J, Claudino AM, Zucker N Eating disorders Lancet, 2010.PMID 19931176
- [5]Sachs KV, Harnke B, Mehler PS, Krantz MJ Cardiovascular complications of anorexia nervosa: A systematic review Int J Eat Disord, 2016.PMID 26710932
- [6]Garber AK, Cheng J, Accurso EC, et al. Short-term Outcomes of the Study of Refeeding to Optimize Inpatient Gains for Patients With Anorexia Nervosa: A Randomized Clinical Trial JAMA Pediatr, 2021.PMID 33074282
- [7]Society for Adolescent Health and Medicine Refeeding hypophosphatemia in hospitalized adolescents with anorexia nervosa: a position statement of the Society for Adolescent Health and Medicine J Adolesc Health, 2014.PMID 25151056
- [8]Society for Adolescent Health and Medicine Medical Management of Restrictive Eating Disorders in Adolescents and Young Adults J Adolesc Health, 2022.PMID 36058805
- [9]Lock J, Le Grange D, Agras WS, et al. Randomized clinical trial comparing family-based treatment with adolescent-focused individual therapy for adolescents with anorexia nervosa Arch Gen Psychiatry, 2010.PMID 20921118
- [10]McIntosh VV, Jordan J, Carter FA, et al. Three psychotherapies for anorexia nervosa: a randomized, controlled trial Am J Psychiatry, 2005.PMID 15800147
- [11]Carter FA, Jordan J, McIntosh VV, et al. The long-term efficacy of three psychotherapies for anorexia nervosa: a randomized, controlled trial Int J Eat Disord, 2011.PMID 21997429
- [12]Byrne S, Wade T, Hay P, et al. A randomised controlled trial of three psychological treatments for anorexia nervosa Psychol Med, 2017.PMID 28552083
- [13]Schmidt U, Ryan EG, Bartholdy S, et al. Two-year follow-up of the MOSAIC trial: A multicenter randomized controlled trial comparing two psychological treatments in adult outpatients with broadly defined anorexia nervosa Int J Eat Disord, 2016.PMID 27061709
- [14]Jordan J, McIntosh VV, Bulik CM Specialist Supportive Clinical Management for anorexia nervosa: what it is (and what it is not) Australas Psychiatry, 2020.PMID 31523976
- [15]Attia E, Steinglass JE, Walsh BT, et al. Olanzapine Versus Placebo in Adult Outpatients With Anorexia Nervosa: A Randomized Clinical Trial Am J Psychiatry, 2019.PMID 30654643
- [16]Attia E, Kaplan AS, Walsh BT, et al. Olanzapine versus placebo for out-patients with anorexia nervosa Psychol Med, 2011.PMID 21426603
- [17]Crone C, Fochtmann LJ, Attia E, et al. The American Psychiatric Association Practice Guideline for the Treatment of Patients With Eating Disorders Am J Psychiatry, 2023.PMID 36722117
- [18]Monteleone AM, Pellegrino F, Croatto G, et al. Treatment of eating disorders: A systematic meta-review of meta-analyses and network meta-analyses Neurosci Biobehav Rev, 2022.PMID 36084848
- [19]Solmi M, Wade TD, Byrne S, et al. Comparative efficacy and acceptability of psychological interventions for the treatment of adult outpatients with anorexia nervosa: a systematic review and network meta-analysis Lancet Psychiatry, 2021.PMID 33600749
- [20]Touyz S, Aouad P, Carney T, et al. Clinical, legal and ethical implications of coercion and compulsory treatment in eating disorders: do rapid review findings identify clear answers or more muddy waters? J Eat Disord, 2024.PMID 39425146
- [21]Turner P Implementation of the medical emergencies in eating disorders in adults guidance on non-specialist units Br J Nurs, 2023.PMID 37410686
- [22]Sahimi HBMS, Selvarajoo S, Nik Jaafar NR, et al. Adaptability of "Management of Really Sick Patients with Anorexia Nervosa" (MARSIPAN) for extreme anorexia nervosa in a developing country: A case report Perspect Psychiatr Care, 2021.PMID 32918751
- [23]Smink FR, van Hoeken D, Hoek HW Epidemiology, course, and outcome of eating disorders Curr Opin Psychiatry, 2013.PMID 24060914
- [24]Smink FR, van Hoeken D, Oldehinkel AJ, et al. Prevalence and severity of DSM-5 eating disorders in a community cohort of adolescents Int J Eat Disord, 2014.PMID 24903034
- [25]Muratore AF, Attia E Psychopharmacologic Management of Eating Disorders Curr Psychiatry Rep, 2022.PMID 35576089
- [26]Lai ET, Lai B, Wong CS, et al. Systematic Review and Meta-Analysis of Mortality in Patients With Anorexia Nervosa Int J Eat Disord, 2026.PMID 41277145