Psych · Specialty psychiatry — eating disorders
Bulimia nervosa and binge-eating disorder
Also known as Bulimia nervosa · Binge-eating disorder · BED · BN · CBT-E · Purging disorder · Eating disorders · Fluoxetine 60 mg · Lisdexamfetamine binge eating
Exam-exhaustive fellowship reference on bulimia nervosa and binge-eating disorder — DSM-5-TR and ICD-11 criteria; AN-purging differential; medical complications and electrolytes; CBT-E and guided self-help; fluoxetine 60 mg BN evidence; lisdexamfetamine for moderate–severe BED; stepped care; RANZCP/NICE/APA regional framing. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Bulimia nervosa (BN) and binge-eating disorder (BED) are high-yield specialty eating-disorder topics for FRANZCP MEQ and clinical reasoning, MRCPsych theory and CASC explanation stations, and ABPN blueprint items. Examiners test criteria discriminators (especially versus anorexia nervosa binge-purge type), medical complications of purging, stepped psychological care (guided self-help and CBT-E), the fluoxetine 60 mg BN dose, and region-aware pharmacotherapy for BED. A candidate who reads only this topic should defend diagnosis, acute medical risk, and definitive stepped care at consultant depth.[18][19]
Overview and definition
Russell’s classic description framed bulimia nervosa as an ominous variant of anorexia nervosa — binge–purge cycles with intense shape/weight concern — and modern nosology retains that clinical gravity while separating BN from anorexia nervosa (AN) and from BED as a distinct diagnosis.[1][19]
Objective binge eating means eating, in a discrete period (commonly about two hours), an amount of food that is definitely larger than most people would eat in a similar period under similar circumstances, plus a sense of loss of control. Both the amount and the loss of control matter in exam stems; “subjective binges” (feeling out of control without objectively large intake) still need clinical attention but do not alone complete BN/BED criteria.[18][19]
Bulimia nervosa (DSM-5-TR structure to reproduce). Recurrent episodes of binge eating; recurrent inappropriate compensatory behaviours to prevent weight gain (self-induced vomiting, misuse of laxatives/diuretics/other medications, fasting, or excessive exercise); both binge eating and compensatory behaviours occur, on average, at least once a week for three months; self-evaluation is unduly influenced by body shape and weight; the disturbance does not occur exclusively during episodes of anorexia nervosa.[18][19]
Binge-eating disorder (DSM-5-TR structure to reproduce). Recurrent binge-eating episodes occurring, on average, at least once a week for three months, associated with three or more of: eating much more rapidly than normal; eating until uncomfortably full; eating large amounts when not physically hungry; eating alone because of embarrassment; feeling disgusted with oneself, depressed, or very guilty afterward; marked distress regarding binge eating; binge eating is not associated with regular inappropriate compensatory behaviours and does not occur exclusively during the course of BN or AN.[5][13][19]
ICD-11. BN and BED are recognised with similar core features (recurrent binge eating; BN with regular compensation; BED without). Always name which manual you are applying when frequency language or residual categories (other specified feeding or eating disorder) are examined.[18][19]
Classification and severity
BN severity (exam teaching by compensatory episode frequency per week): mild 1–3; moderate 4–7; severe 8–13; extreme 14 or more. BED severity uses binge-episode frequency bands with the same numerical structure. Severity guides intensity of care but does not replace medical risk assessment — a “mild” frequency BN can still present with dangerous hypokalaemia.[15][18]
BN subtypes (clinical teaching). Purging type (vomiting, laxatives, diuretics) versus non-purging type (fasting, excessive exercise) remains useful for medical risk framing even when manuals emphasise specifiers of severity and remission rather than historical subtype labels alone.[14][15]
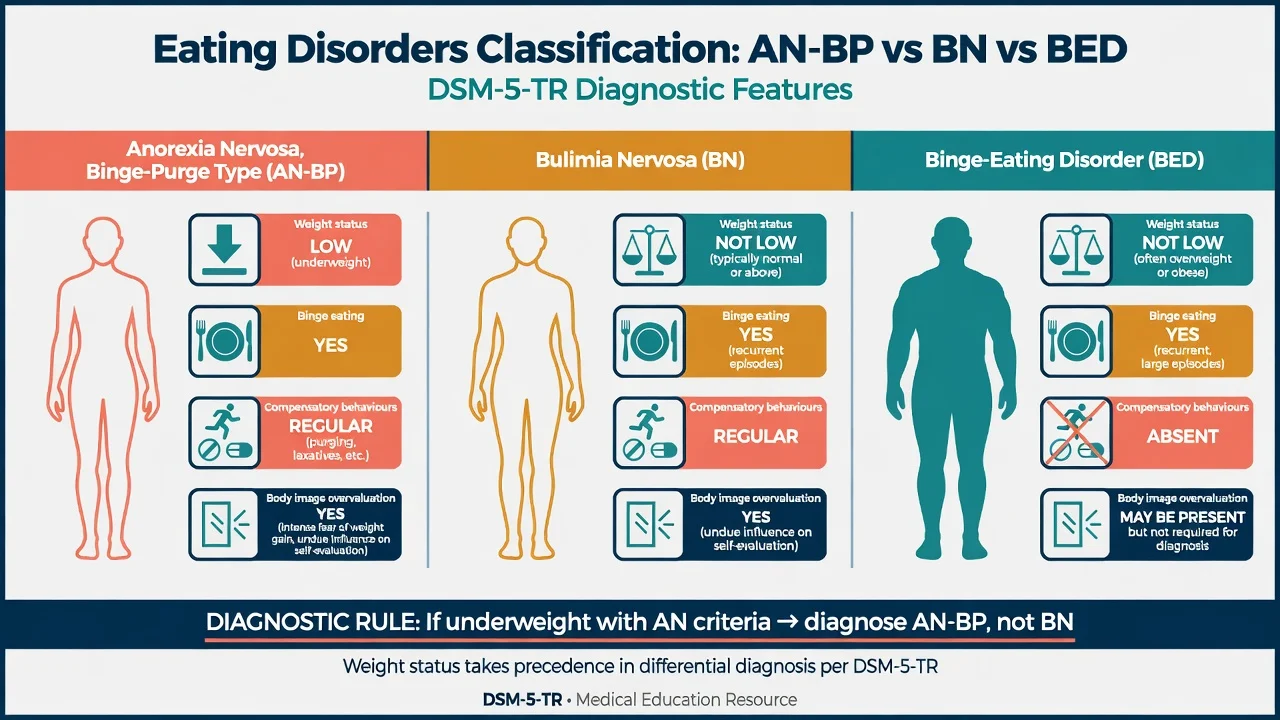
AN binge-purge type
- Significantly low weight + AN criteria
- May binge and/or purge
- Diagnose AN-BP — not BN
- Highest medical risk pathway among this triad
Bulimia nervosa
- Weight not in the significantly low AN range
- Recurrent binge + regular compensation
- Shape/weight overvaluation required
- Normal BMI ≠ medical safety
Binge-eating disorder
- Recurrent loss-of-control binges + distress
- No regular compensatory behaviours
- Overweight/obesity common, not required
- Shape overvaluation common but not core criterion
OSFED / residual
- Subthreshold frequency or mixed features
- Still impairing — treat the presentation
- Do not dismiss as 'not real ED'
- Reassess diagnosis as symptoms evolve
Epidemiology and risk factors
Headline epidemiology (exam order-of-magnitude)
In the National Comorbidity Survey Replication, lifetime prevalence of DSM-IV eating disorders showed BN and BED as clinically important disorders with substantial comorbidity and role impairment; BED was not rare in community samples.[4] WHO World Mental Health Surveys confirmed BED as a prevalent, impairing condition across countries with high psychiatric comorbidity.[5]
Risk and maintaining factors. Dieting and thin-ideal internalisation, body dissatisfaction, perfectionism, adverse childhood experiences, familial aggregation, and sociocultural pressure. BED associates with obesity and metabolic disease more than BN does, but neither diagnosis is defined by BMI alone.[4][5][19]
Mortality and suicide. Meta-analytic data show elevated mortality across eating disorders, with AN carrying the highest standardised mortality ratios and BN also showing excess deaths compared with the general population.[16] Crow and colleagues reported increased mortality in BN and other eating disorders in a long-term cohort, reinforcing that “normal weight” does not equal low risk.[17] Suicide risk assessment is mandatory at every meaningful contact.[16][17][18]
Pathophysiology
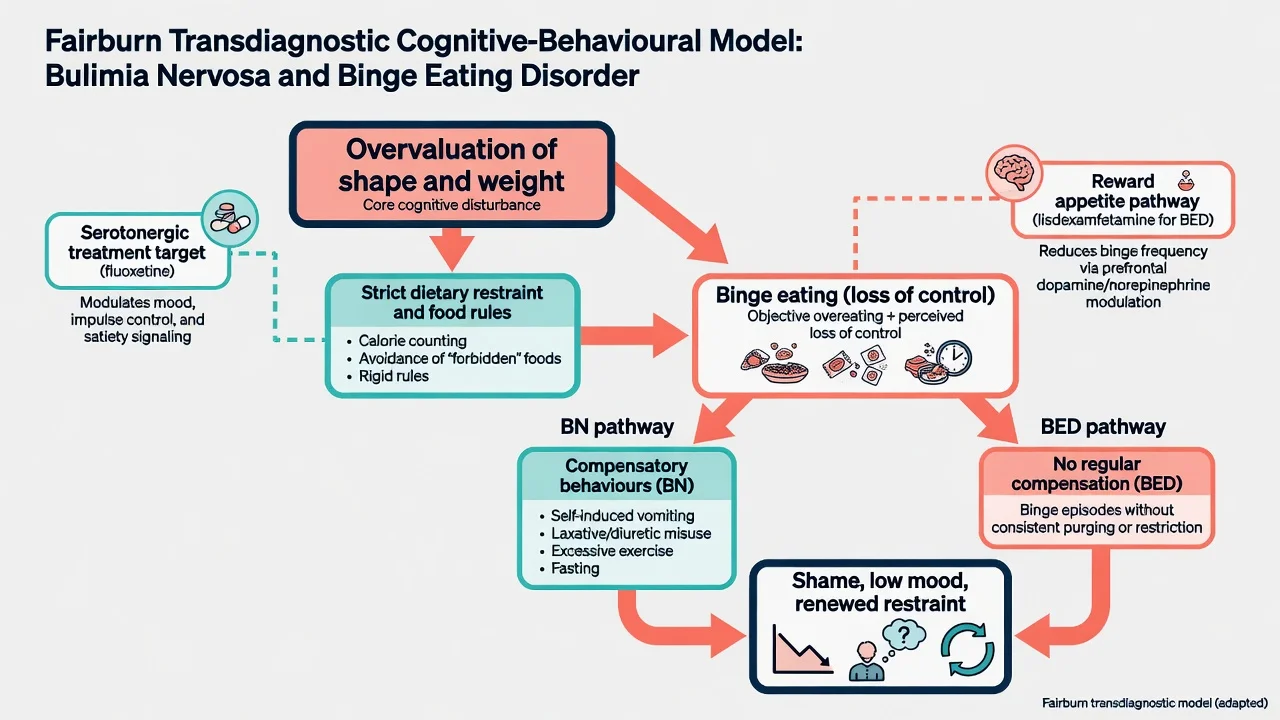
Transdiagnostic cognitive-behavioural model (viva-ready). Overvaluation of shape and weight drives strict dietary restraint and food rules; restraint and emotional triggers precipitate binge eating with loss of control; in BN, compensatory behaviours temporarily reduce anxiety about weight gain but reinforce the cycle and medical risk; in BED, binge episodes recur with distress without regular compensation, often amplifying shame and further chaotic eating.[6][9][19]
Neurobiology and pharmacology links (not reductionist). Serotonergic agents, especially fluoxetine at BN doses, reduce binge–purge frequency, supporting serotonergic modulation as a treatment pathway rather than a simple “serotonin deficiency.” For BED, lisdexamfetamine (a prodrug stimulant) reduces binge frequency in moderate–severe illness where licensed, implicating catecholaminergic and appetite/reward pathways — frame as treatment pharmacology, not a complete aetiology.[2][10][13]
Medical pathophysiology of purging. Recurrent vomiting causes volume depletion, metabolic alkalosis, and urinary potassium wasting; hypokalaemia and acid–base disturbance drive arrhythmia risk. Laxative and diuretic misuse add further electrolyte chaos and secondary hyperaldosteronism (pseudo-Bartter physiology after abrupt cessation).[14][15]
Clinical presentation
Bulimia nervosa. Often secretive binge–purge cycles; intense shame; shape/weight overvaluation; frequent normal or above-normal BMI; dental enamel erosion (especially lingual surfaces), bilateral parotid enlargement, Russell sign (dorsal knuckle calluses from inducing vomiting), reflux symptoms, irregular menses, and mood instability. Patients may present first to dentistry, gastroenterology, or emergency medicine with electrolyte disturbance rather than to psychiatry.[14][15][19]
Binge-eating disorder. Recurrent large episodes with loss of control and marked distress, often evening or solitary eating, without regular purge/fasting/exercise compensation. Overweight and obesity are common but not required. Associated depressive and anxiety symptoms, functional impairment, and cardiometabolic comorbidity are frequent.[5][12][13]
MSE language examiners reward. Describe binge content and triggers in the patient’s words; quantify weekly frequency; document compensatory methods; mood, anhedonia, and suicide risk; insight into the cycle; cognitive overvaluation of shape/weight; absence or presence of psychotic features (rare as primary explanation).[18][19]
High-yield atypical stems. Male athletes with purging or extreme training; insulin omission for weight control in type 1 diabetes; late first presentation; post-AN weight restoration with persistent binge–purge (diagnostic label may shift from AN-BP toward BN once weight is restored and AN criteria no longer met).[15][18]
Differential diagnosis
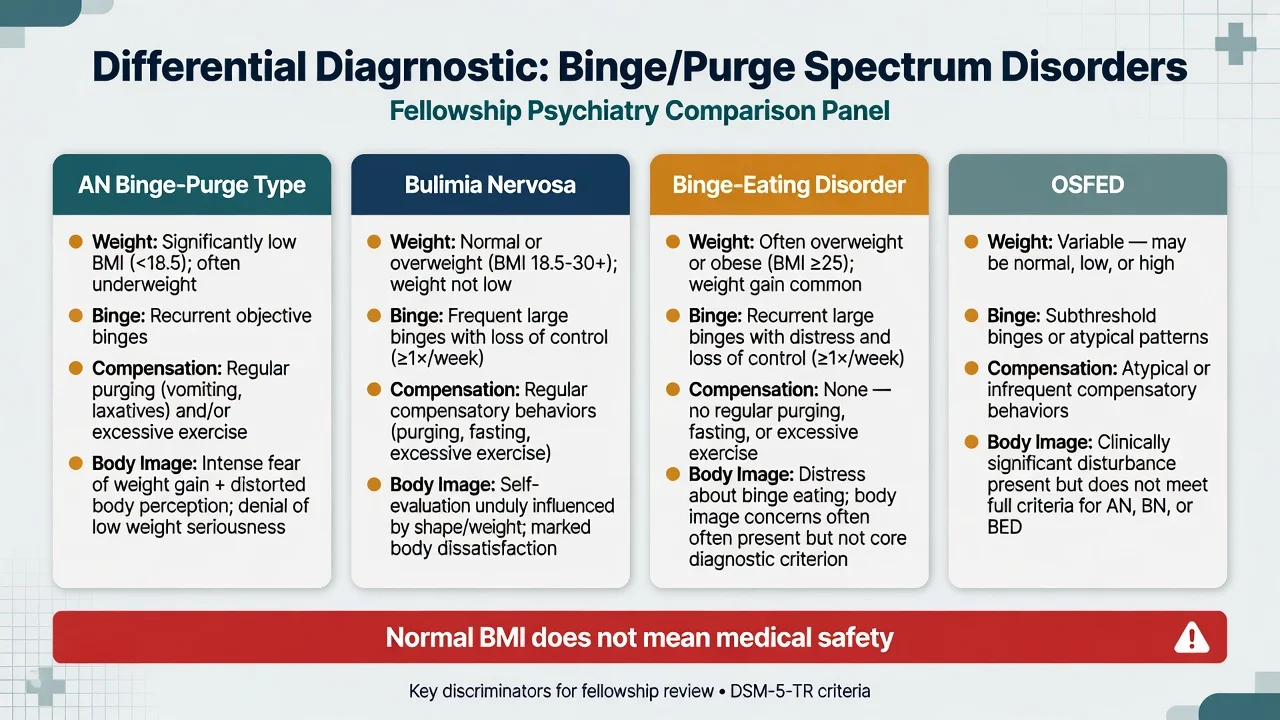
| Diagnosis | Weight | Binge | Regular compensation | Key discriminator |
|---|---|---|---|---|
| AN binge-purge type | Significantly low | Often | Often | AN criteria + low weight trump BN |
| Bulimia nervosa | Not significantly low | Yes | Yes | Shape/weight overvaluation + compensation |
| Binge-eating disorder | Any (often high) | Yes | No | Distress without regular compensation |
| OSFED / residual | Variable | Subthreshold/mixed | Variable | Impairment without full BN/BED/AN |
| ARFID | Variable | No body-image drive | No | Avoidance not driven by shape/weight |
| Always re-check weight trajectory: a patient who binges and purges at low weight is managed on the AN-BP pathway until AN criteria no longer apply.[18][19] |
Also discriminate major depression with appetite change (no discrete loss-of-control binge structure), substance-related overeating (stimulant crash), medication-induced hyperphagia, medical polyphagia (uncontrolled diabetes), and impulsive bingeing in personality pathology — formulate comorbidity rather than forcing a single label when both are present.[4][19]
Clinical and bedside assessment
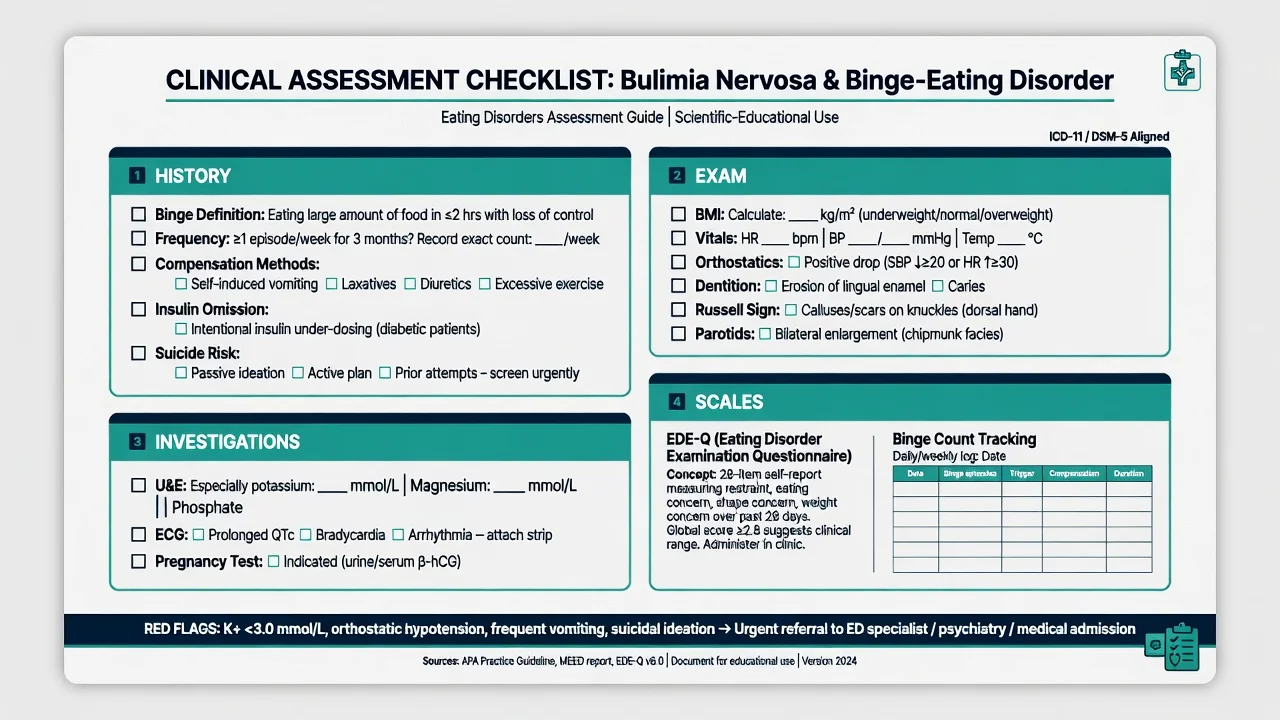
History structure. Onset and course; operational binge definition; weekly frequency; full list of compensatory methods (vomiting, laxatives, diuretics, diet pills, excessive exercise, fasting, insulin omission); body image and weight history; lowest/highest adult weights; menstrual history; dental symptoms; substances; trauma; prior therapy fidelity (was it true CBT-E?); medication trials with dose and duration; suicide and self-harm; social/occupational function; carer accommodation of food rules.[14][15][18]
Physical exam. BMI and weight trend; heart rate and blood pressure including orthostatics; hydration; dentition; parotid enlargement; Russell sign; abdominal exam; oedema; self-harm scars; signs of low weight that would reclassify toward AN (lanugo, bradycardia extremes, marked cachexia).[14][15]
Risk. Suicide risk is elevated and independent of the reassuring BMI. Medical risk is driven by purging intensity, electrolytes, ECG, and diabetes behaviours. Capacity is decision-specific; compulsory treatment statutes are jurisdiction-specific — state principles and name the local Mental Health Act framework without inventing foreign section numbers.[16][17][18]
Measurement-based care. Track binge and purge counts weekly. Eating Disorder Examination / EDE-Q is the research and specialist-clinic standard concept for psychopathology severity; use what your service supports consistently rather than collecting unused scales.[9][18]
Investigations
Baseline for purging or any moderate–severe presentation. Urea and electrolytes with potassium, sodium, magnesium, phosphate; glucose; full blood count; liver function; consider amylase if abdominal pain; ECG for arrhythmia and QTc context; pregnancy test when relevant. Abnormal potassium or ECG change triggers medical pathway, not “return if worse” alone.[14][15]
Before pharmacotherapy. Fluoxetine: discuss sexual side-effects, activation, interactions, suicidality monitoring with comorbid depression. Lisdexamfetamine (where used for BED): baseline cardiovascular history, blood pressure and heart rate, substance-use history, misuse/diversion risk. Topiramate (off-label niche): cognitive effects, teratogenicity (contraception and pregnancy planning essential).[2][10][11]
Neuroimaging is not routine for classic BN/BED without neurological red flags.[18]
Management — acute risk and resuscitation
Medical priorities. Check and replace potassium under medical protocols; ECG monitoring when indicated; careful management of laxative/diuretic cessation (rebound oedema and secondary hyperaldosteronism); treat dehydration; involve cardiology if significant arrhythmia. Insulin omission requires urgent diabetes and medical input.[14][15]
Psychiatric priorities. Structured suicide risk assessment, means restriction, safety planning, and appropriate setting (outpatient with close review, crisis team, or admission). Do not minimise distress because the patient “looks well nourished.”[16][17][18]
Management — definitive and stepwise
Psychological treatments (first-line for both)
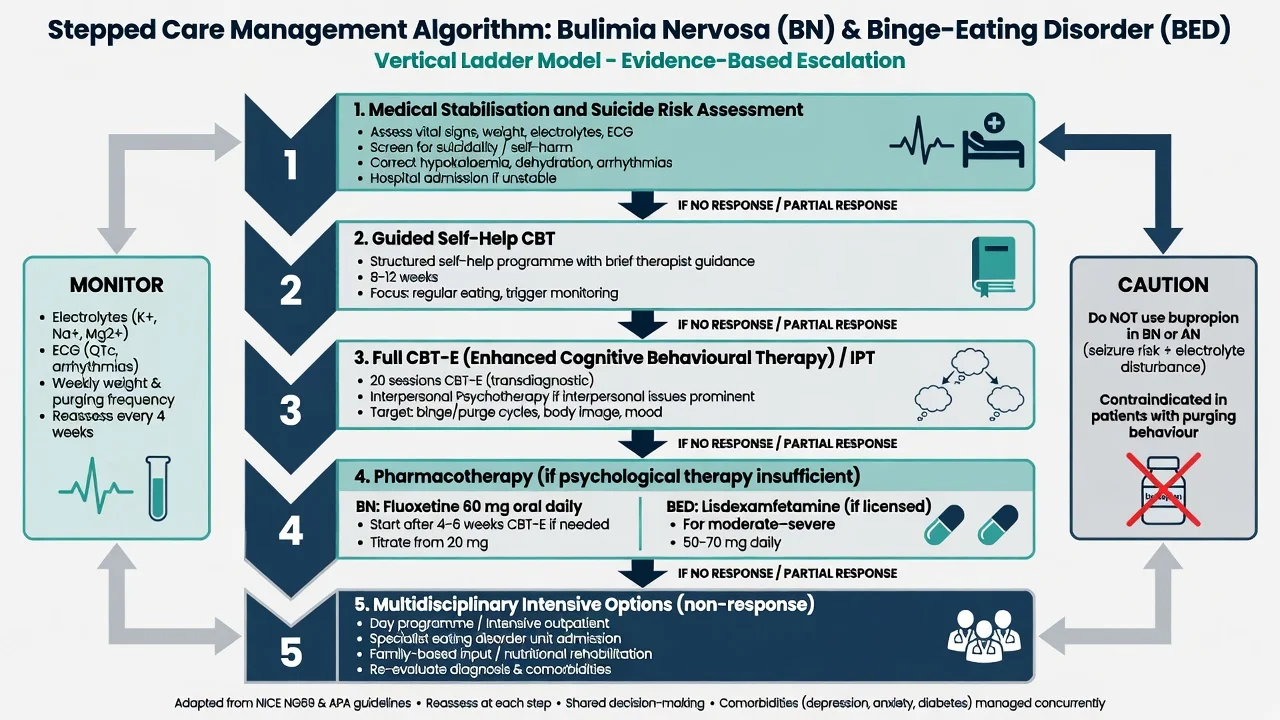
CBT-E (enhanced cognitive behaviour therapy) is the leading evidence-based psychological treatment for non-underweight eating disorders, including BN and many BED presentations. Core targets: regularised eating (typically planned meals/snacks to reduce restriction-triggered bingeing), self-monitoring, formulation of the binge cycle, reduction of shape/weight overvaluation, and relapse prevention. Fairburn and colleagues demonstrated efficacy of a transdiagnostic CBT protocol with durable follow-up gains in a two-site randomised trial of eating-disorder patients who were not severely underweight.[6][9][18]
Guided self-help CBT is an evidence-supported first step for many people with BN or BED (structured manual plus brief therapist guidance). Meta-analytic work on manualised self-help shows meaningful participation-dependent outcomes; it is not “doing nothing” and is embedded in stepped-care logic.[7][8][18]
Stepped care versus full CBT for BN. Mitchell and colleagues showed that a stepped-care approach (starting with less intensive treatment and stepping up) can be effective and efficient compared with immediate full CBT for bulimia nervosa in a randomised trial — use this as the exam narrative for resource-aware pathways, not as an excuse to withhold specialist care when severity is high.[7]
Interpersonal psychotherapy (IPT). Group CBT and group IPT both reduced binge eating in overweight individuals with BED in a landmark randomised comparison; CBT may show faster binge reduction, but IPT is a legitimate evidence-based alternative when interpersonal maintaining factors dominate or CBT is unavailable/unacceptable.[12][9]
Systematic review and meta-analysis of adult BED treatments supports psychological interventions (especially CBT) and selected medications as effective options with different trade-offs.[13]
Pharmacotherapy
| Indication | Agent | Typical adult oral approach (exam teaching) | Key monitoring / cautions |
|---|---|---|---|
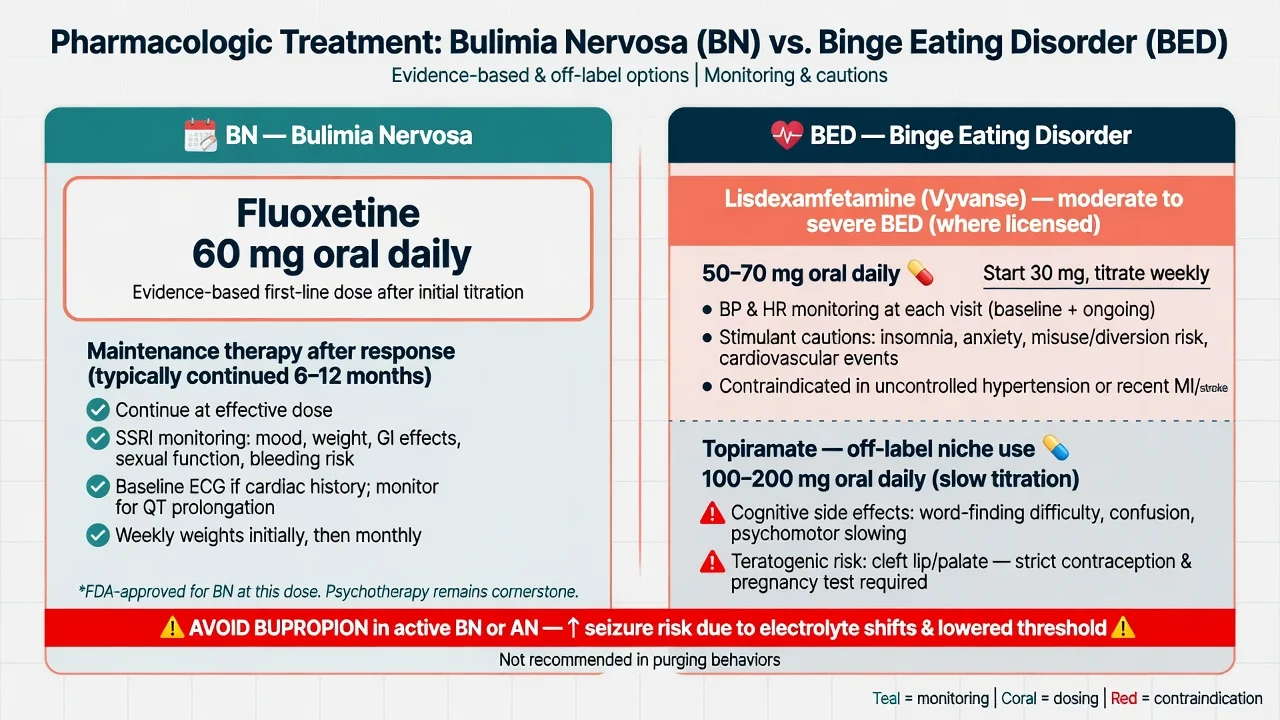
| BN | Fluoxetine | Target 60 mg daily (often start 20 mg, titrate) | Sexual/GI effects; mood/suicidality; interactions |
| BN maintenance | Fluoxetine | Continue effective dose after response | Relapse risk if stopped early after response |
| BED (where licensed) | Lisdexamfetamine | Specialist pathway; commonly titrate toward 50–70 mg daily from lower start | BP/HR; insomnia; misuse risk; CV contraindications |
| BED off-label niche | Topiramate | Slow titration; individualise | Cognition; teratogenicity; glaucoma/metabolic acidosis risk |
| BN or AN | Bupropion | Do not use | Seizure risk elevated |
| Doses individualise for age, hepatic function, interactions, pregnancy; check local product information and licensing.[2][3][10][11][18] |
Fluoxetine for BN — the dose examiners want. The Fluoxetine Bulimia Nervosa Collaborative Study Group multicentre, placebo-controlled trial established that fluoxetine 60 mg daily reduces binge eating and vomiting more effectively than placebo (with 20 mg intermediate/less consistent), embedding 60 mg as the classic exam dose — not the 20 mg depression start left unchanged.[2] Romano and colleagues showed that continued fluoxetine after successful acute treatment reduces relapse compared with switching to placebo, supporting maintenance rather than automatic early cessation.[3]
Lisdexamfetamine for BED. McElroy and colleagues demonstrated efficacy and acceptable short-term safety of lisdexamfetamine versus placebo for adults with moderate to severe BED in a randomised trial, reducing binge-eating days. Licensing and availability differ by region (stronger US pathway historically than many ANZ/UK contexts) — state local formulary and specialist governance explicitly rather than assuming global access.[10][13][18]
Topiramate. Randomised placebo-controlled evidence supports topiramate for BED associated with obesity, but cognitive adverse effects and teratogenicity limit first-line use; reserve as specialist off-label consideration after psychological care and safer options are addressed.[11][13]
Other agents. Other SSRIs are sometimes used clinically for BN when fluoxetine is not tolerated, but the exam anchor remains fluoxetine 60 mg. Do not present antidepressants as a substitute for CBT-E when therapy is accessible. Antipsychotics are not first-line BN/BED treatments.[2][9][18]
Multidisciplinary care and levels of intensity
Dietetics for structured regular eating; dental review for enamel damage; GP for medical monitoring; endocrinology/diabetes teams when insulin omission or metabolic disease is present; specialist eating-disorder services for non-response, high medical risk, or complex comorbidity. Day programmes and inpatient medical/psychiatric settings are for instability, failed outpatient care, or high suicide risk — not default for every BN diagnosis.[14][15][18]
Specific subtypes and scenarios
BN purging versus non-purging compensation. Vomiting and laxative/diuretic misuse drive the classic electrolyte–dental–parotid phenotype; non-purging compensation (extreme exercise, fasting) still maintains the binge cycle and needs the same CBT-E targets with tailored behavioural experiments.[14][15]
BED with obesity and metabolic syndrome. Treat the eating disorder and cardiometabolic risk in parallel; weight-loss-only programmes that intensify restriction without addressing loss of control often worsen bingeing. Integrate CBT principles with medically supervised weight management when needed.[12][13]
Transition from AN to BN. After weight restoration, residual binge–purge with shape overvaluation may meet BN criteria. Continue eating-disorder expertise; do not declare “cured” at a BMI threshold alone.[18][19]
Diabetes and insulin omission. Intentional under-dosing of insulin to influence weight is a medical emergency risk (ketoacidosis, microvascular harm). Coordinate psychiatry, diabetes, and acute medicine; do not manage as “simple BN” in isolation.[15][18]
Treatment-refractory pathway. Confirm diagnosis (especially AN-BP missed), therapy fidelity (true CBT-E vs supportive chat), medication adequacy (fluoxetine actually reached 60 mg for an adequate duration), substances, and trauma/comorbidity. Step up intensity (specialist CBT-E, day programme), consider IPT alternative, review BED medication options if BED, and avoid stacking unproven polypharmacy.[6][7][20]
Complications and pitfalls
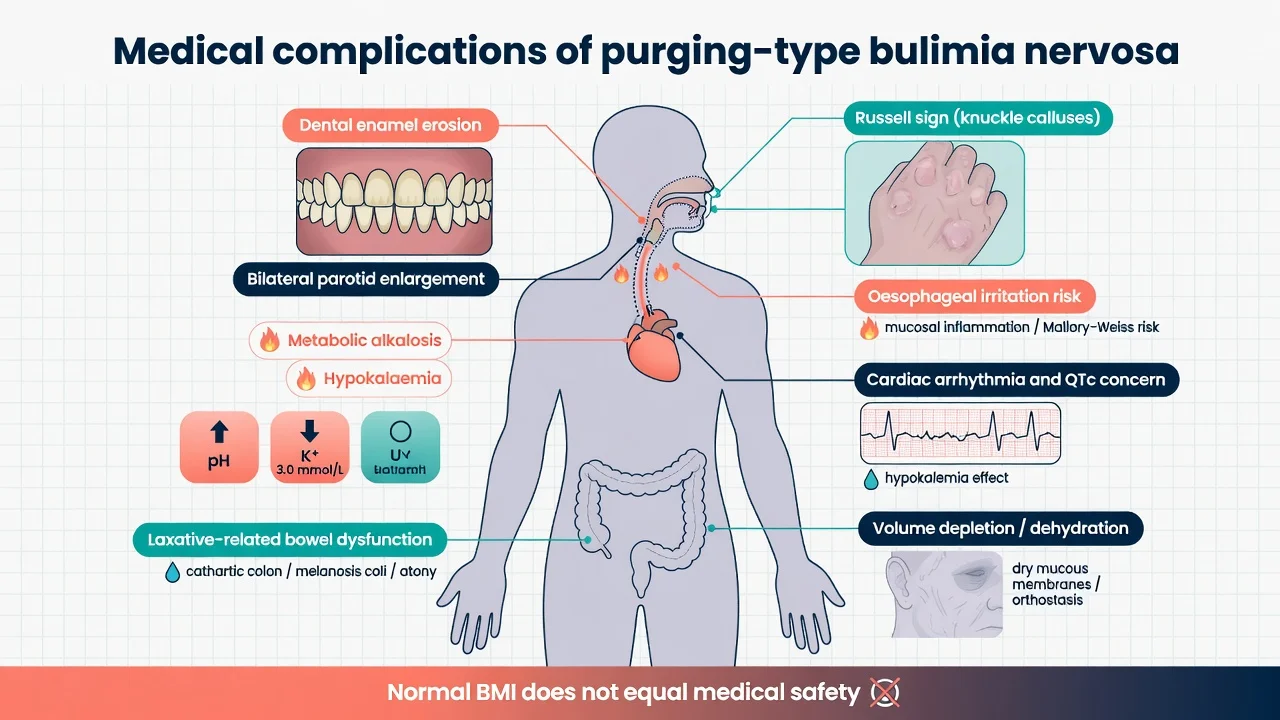
Medical complications of BN (high-yield list). Dental enamel erosion; caries; parotid hypertrophy; Russell sign; oesophagitis and Mallory–Weiss risk; aspiration risk; metabolic alkalosis; hypokalaemia; hypomagnesaemia; dehydration; arrhythmia and QTc concern; constipation or cathartic colon from laxative misuse; oedema after purgative cessation; rare cardiomyopathy reports in severe chronic disease.[14][15]
Classic pitfalls.
- Labelling AN-BP as BN and missing underweight medical risk.[18]
- Declaring “SSRI failure” after fluoxetine 20 mg for two weeks.[2]
- Using bupropion for comorbid depression in active BN/AN.[18]
- Prescribing lisdexamfetamine as first-line for BN without psychological care or outside BED indication/licensing.[10]
- Ignoring suicide risk because the patient is not underweight.[16][17]
- Calling unstructured supportive counselling “CBT-E.”[6][9]
Prognosis and disposition
BN and BED often run a chronic-waxing course without treatment, but many patients achieve substantial reduction in binge/purge frequency with CBT-based care and, where appropriate, medication.[6][9][19] Multisite CBT data for BN identify poorer outcome predictors such as greater symptom severity and related clinical features — use early change and engagement as clinical signals to intensify care.[20]
Disposition map. Mild–moderate, medically stable, engaged → outpatient guided self-help or CBT-E ± fluoxetine (BN) with GP monitoring. Moderate–severe or partial response → specialist ED service, full CBT-E, medication optimisation. Medical instability → medical admission. High suicide risk or failed intensive community care → psychiatric admission with medical monitoring as needed. Always safety-net for electrolyte red flags and suicidal crises.[7][15][18]
Special populations
Adolescents. Developmental body image, family meal patterns, school function, and parent involvement matter; adapt CBT and family work; screen for emerging AN trajectory.[18][19]
Pregnancy and lactation. Active purging threatens maternal–fetal physiology; prioritise medical stability and psychological care. Fluoxetine risk–benefit is individualised with perinatal psychiatry input. Avoid topiramate in pregnancy because of teratogenicity; ensure contraception when topiramate is used in people who can become pregnant.[11][18]
Males and athletes. Under-recognised; performance pressure and muscularity ideals may replace classic thin-ideal language — still map binge, compensation, and medical risk.[19]
Older adults. Lower physiological reserve for electrolyte disturbance and drug interactions; late-onset presentations need medical exclusion of organic drivers of weight and appetite change.[15]
Cultural context. Body ideals and food practices vary; assess overvaluation and distress without imposing a single cultural template. In ANZ practice, culturally safe care for Aboriginal and Torres Strait Islander and Māori patients is part of competent assessment, not an optional add-on.[18]
Evidence, guidelines, and regional differences
Landmark evidence anchors for viva: Fluoxetine Bulimia Nervosa Collaborative Study Group (60 mg); Romano maintenance fluoxetine; Fairburn CBT-E/transdiagnostic CBT trial; Mitchell stepped-care BN trial; Beintner self-help meta-regression; Wilfley CBT vs IPT for BED; McElroy lisdexamfetamine BED RCT; McElroy topiramate BED RCT; Brownley BED systematic review; Hudson NCS-R and Kessler WMH epidemiology; Arcelus and Crow mortality data; Mehler medical complications reviews; Treasure Lancet overview; RANZCP Hay guidelines.[2][3][6][7][10][16][18][19]
Exam pearls
BN vs BED vs AN-BP (weight first)
Classic stem clues: Russell sign, enamel erosion, parotidomegaly, hypokalaemic alkalosis, normal BMI with secretive purging, fluoxetine dose questions, and “is this BN or AN-BP?” weight discriminators.[14][15][18]
References
- [1]Russell G Bulimia nervosa: an ominous variant of anorexia nervosa Psychol Med, 1979.PMID 482466
- [2]Fluoxetine Bulimia Nervosa Collaborative Study Group Fluoxetine in the treatment of bulimia nervosa. A multicenter, placebo-controlled, double-blind trial Arch Gen Psychiatry, 1992.PMID 1550466
- [3]Romano SJ, Halmi KA, Sarkar NP, Koke SC, Lee JS A placebo-controlled study of fluoxetine in continued treatment of bulimia nervosa after successful acute fluoxetine treatment Am J Psychiatry, 2002.PMID 11772696
- [4]Hudson JI, Hiripi E, Pope HG Jr, Kessler RC The prevalence and correlates of eating disorders in the National Comorbidity Survey Replication Biol Psychiatry, 2007.PMID 16815322
- [5]Kessler RC, Berglund PA, Chiu WT, Deitz AC, et al. The prevalence and correlates of binge eating disorder in the World Health Organization World Mental Health Surveys Biol Psychiatry, 2013.PMID 23290497
- [6]Fairburn CG, Cooper Z, Doll HA, O'Connor ME, et al. Transdiagnostic cognitive-behavioral therapy for patients with eating disorders: a two-site trial with 60-week follow-up Am J Psychiatry, 2009.PMID 19074978
- [7]Mitchell JE, Agras S, Crow S, Halmi K, et al. Stepped care and cognitive-behavioural therapy for bulimia nervosa: randomised trial Br J Psychiatry, 2011.PMID 21415046
- [8]Beintner I, Jacobi C, Schmidt UH Participation and outcome in manualized self-help for bulimia nervosa and binge eating disorder - a systematic review and metaregression analysis Clin Psychol Rev, 2014.PMID 24508686
- [9]Wilson GT, Grilo CM, Vitousek KM Psychological treatment of eating disorders Am Psychol, 2007.PMID 17469898
- [10]McElroy SL, Hudson JI, Mitchell JE, Wilfley D, et al. Efficacy and safety of lisdexamfetamine for treatment of adults with moderate to severe binge-eating disorder: a randomized clinical trial JAMA Psychiatry, 2015.PMID 25587645
- [11]McElroy SL, Arnold LM, Shapira NA, Keck PE Jr, et al. Topiramate in the treatment of binge eating disorder associated with obesity: a randomized, placebo-controlled trial Am J Psychiatry, 2003.PMID 12562571
- [12]Wilfley DE, Welch RR, Stein RI, Spurrell EB, et al. A randomized comparison of group cognitive-behavioral therapy and group interpersonal psychotherapy for the treatment of overweight individuals with binge-eating disorder Arch Gen Psychiatry, 2002.PMID 12150647
- [13]Brownley KA, Berkman ND, Peat CM, Lohr KN, et al. Binge-Eating Disorder in Adults: A Systematic Review and Meta-analysis Ann Intern Med, 2016.PMID 27367316
- [14]Mehler PS Medical complications of bulimia nervosa and their treatments Int J Eat Disord, 2011.PMID 21312201
- [15]Nitsch A, Dlugosz H, Gibson D, Mehler PS Medical complications of bulimia nervosa Cleve Clin J Med, 2021.PMID 34078617
- [16]Arcelus J, Mitchell AJ, Wales J, Nielsen S Mortality rates in patients with anorexia nervosa and other eating disorders. A meta-analysis of 36 studies Arch Gen Psychiatry, 2011.PMID 21727255
- [17]Crow SJ, Peterson CB, Swanson SA, Raymond NC, et al. Increased mortality in bulimia nervosa and other eating disorders Am J Psychiatry, 2009.PMID 19833789
- [18]Hay P, Chinn D, Forbes D, Madden S, et al. Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for the treatment of eating disorders Aust N Z J Psychiatry, 2014.PMID 25351912
- [19]Treasure J, Duarte TA, Schmidt U Eating disorders Lancet, 2020.PMID 32171414
- [20]Agras WS, Crow SJ, Halmi KA, Mitchell JE, et al. Outcome predictors for the cognitive behavior treatment of bulimia nervosa: data from a multisite study Am J Psychiatry, 2000.PMID 10910795