Psych · Specialty psychiatry — sexual medicine interface
Erectile and ejaculatory disorders
Also known as Erectile dysfunction · Erectile disorder · Impotence · Premature ejaculation · Early ejaculation · Delayed ejaculation · Anejaculation · PDE5 inhibitors · Sildenafil · Dapoxetine · SSRI sexual side-effects
Exam-exhaustive fellowship leaf on erectile disorder, premature (early) ejaculation, and delayed ejaculation — DSM-5-TR/ISSM nosology, organic vs psychogenic discrimination, IIEF assessment, PDE5 inhibitor efficacy and nitrate safety, PE behavioural and SSRI/dapoxetine strategies, and antidepressant/antipsychotic iatrogenic pathways. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Erectile and ejaculatory presentations are high-yield for FRANZCP MEQs, MRCPsych theory/CASC, and ABPN items because they sit at the psychiatry–urology–cardiology interface. Examiners test phase mapping, IIEF literacy, PDE5 safety, PE latency definitions, and antidepressant sexual side-effects. A candidate who reads only this leaf should manage these presentations at consultant depth without relying solely on the broader sexual-dysfunction hub page.[2][4][14]
Overview and definition
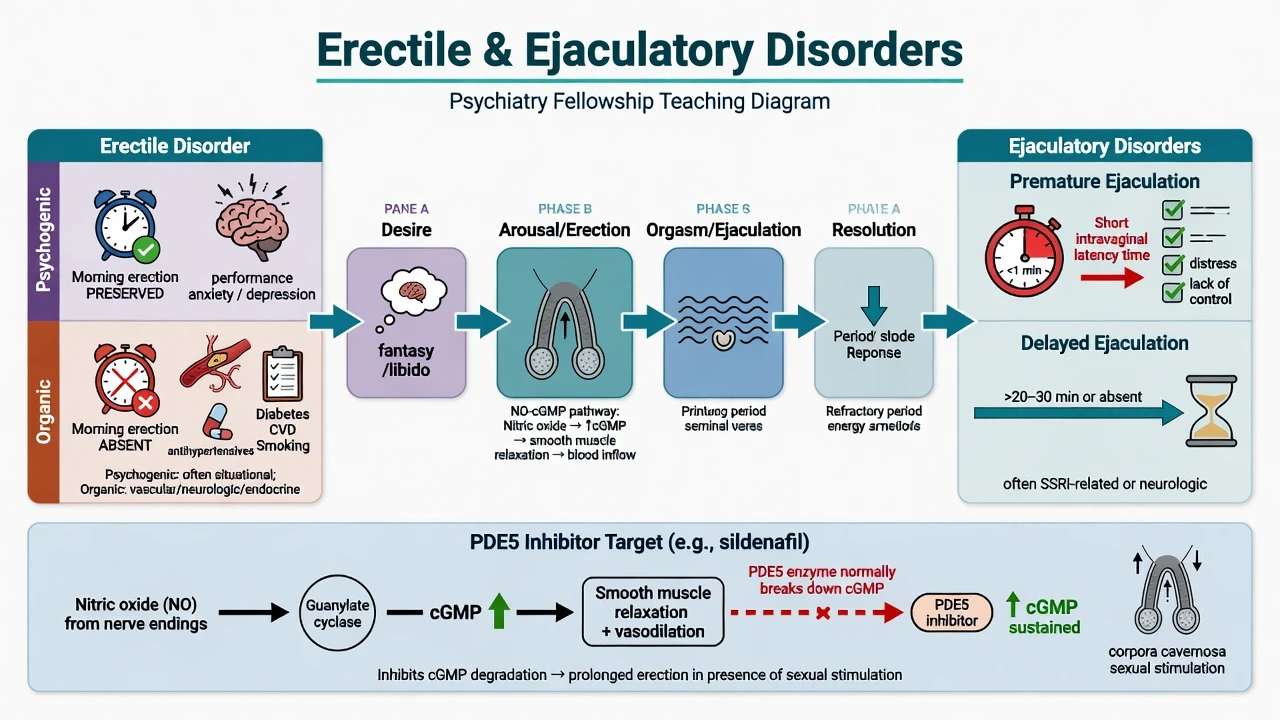
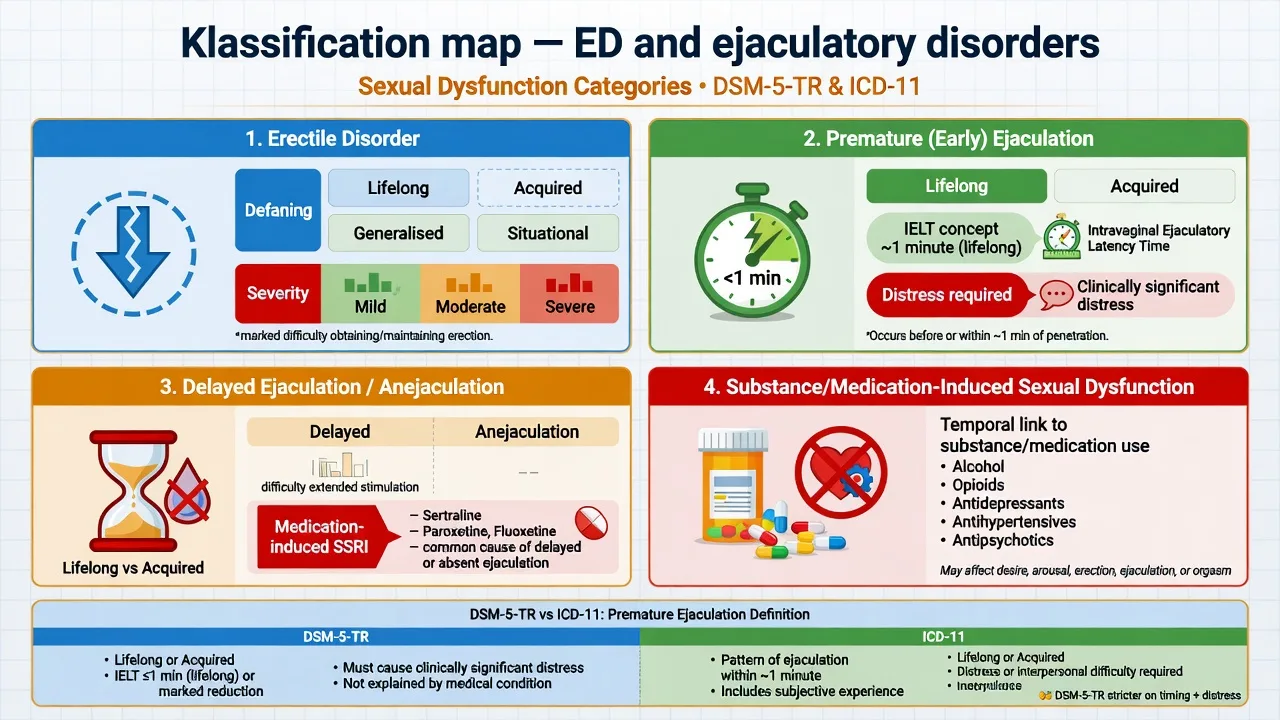
Erectile disorder (DSM-5-TR language; still often called erectile dysfunction clinically) is a marked difficulty obtaining an erection during sexual activity, maintaining an erection until completion, and/or marked decrease in erectile rigidity, with clinically significant distress, typically present for about 6 months, and not better accounted for solely by a nonsexual mental disorder, severe relationship distress alone, substances, or another medical condition when coding a primary sexual dysfunction. Specifiers that examiners expect: lifelong vs acquired, generalised vs situational, and severity (mild/moderate/severe).[2][6]
Premature (early) ejaculation is a persistent pattern of ejaculation occurring during partnered sexual activity within approximately 1 minute following vaginal penetration (lifelong PE teaching cut-point in ISSM-style frameworks) and before the individual wishes it, with inability to delay ejaculation and negative personal consequences (distress, frustration, avoidance). Acquired PE may allow a broader latency frame; always state which manual and which PE subtype you are using because DSM-5 and ICD-11 wording are not identical.[7][8]
Delayed ejaculation is a marked delay in, infrequency of, or absence of ejaculation despite adequate sexual stimulation and the wish to ejaculate, with distress. In psychiatric clinics this phenotype is often medication-induced (especially SSRIs) rather than lifelong primary.[10][14]
Clinical essence. These are not moral problems and not automatic relationship verdicts. They are phase-specific syndromes with vascular, endocrine, neurological, psychological, relational, and iatrogenic drivers — often several at once in midlife men.[3][13]
Classification and nosology
Erectile disorder
- Arousal-phase rigidity problem
- Obtain / maintain / rigidity criteria
- Organic and psychogenic pathways
- IIEF tracks severity and response
Premature (early) ejaculation
- Orgasm/ejaculation timing too early
- IELT + inability to delay + distress
- Lifelong vs acquired PE
- Behavioural ± SSRI/dapoxetine
Delayed ejaculation
- Markedly prolonged or absent ejaculation
- Often SSRI/SNRI iatrogenic
- Fertility and relationship impact
- Switch/reduce serotonergic load
Medication-induced
- Temporal link to drug start/titration
- SSRIs, antipsychotics, alcohol, opioids
- Code as substance/medication-induced when primary
- Adherence risk if ignored
Exam pearl on PE manuals. ISSM guidance emphasises short ejaculatory latency (classically about 1 minute from vaginal penetration for lifelong PE teaching), inability to delay, and negative personal consequences. DSM-5 and ICD-11 definitions diverge enough that Waldinger-type critiques appear in higher-level viva — name the framework and avoid inventing cut-points not in the stem.[7][8]
Epidemiology and risk
Headline epidemiology (exam anchors)
Population surveys show sexual problems are common; rates depend on age, health, and whether distress is required for caseness.[1][2] ICSM consensus statements summarise incidence/prevalence patterns and risk factors: vascular disease, diabetes, smoking, depression, relationship conflict, and medications dominate male ED risk framing.[2][3]
Antidepressant-associated sexual dysfunction is not rare noise — prospective multicentre data (Montejo) and meta-analytic ranking (Serretti) are the exam anchors for agent differences and for treating sexual side-effects as an adherence emergency.[10][11]
Pathophysiology and mechanisms
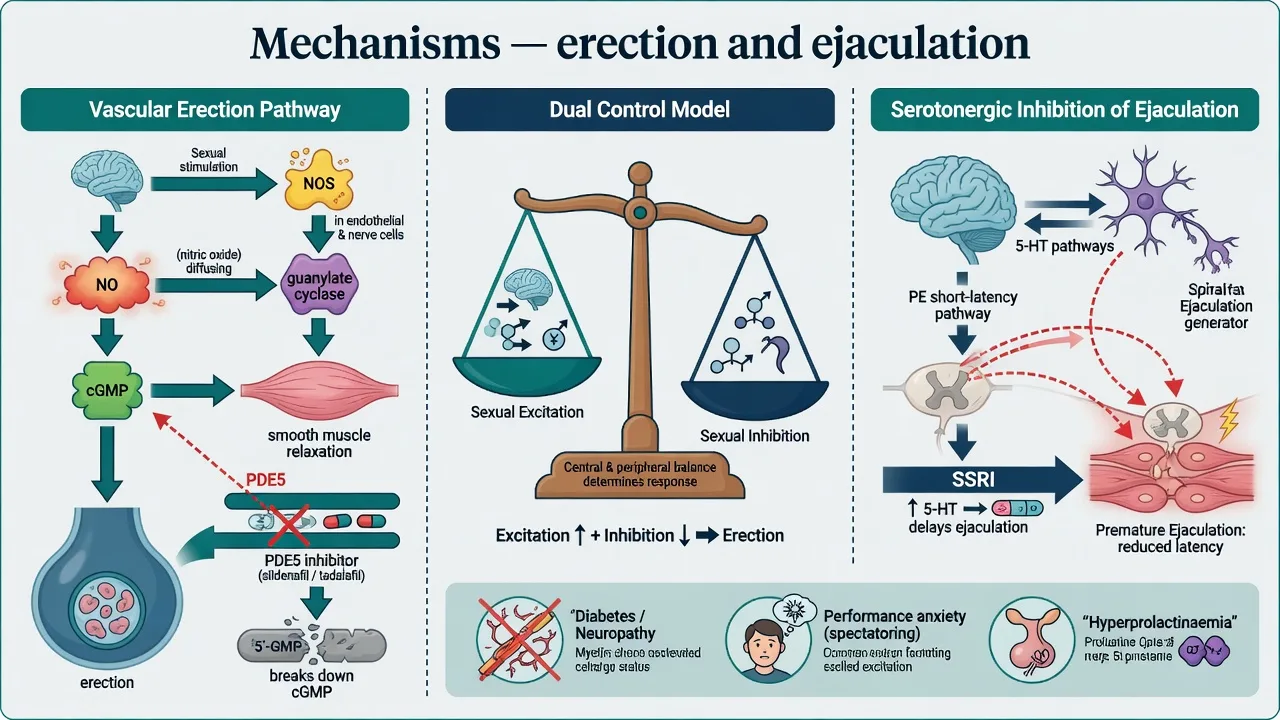
Erection physiology (viva sequence). Sexual stimulation → nitric oxide (NO) release → guanylate cyclase activation → cyclic GMP (cGMP) increase → cavernosal smooth-muscle relaxation → arterial inflow and veno-occlusion. Phosphodiesterase type 5 (PDE5) degrades cGMP; oral PDE5 inhibitors (sildenafil, tadalafil, and related agents) block this step and improve erectile response when sexual stimulation is present.[5][6]
Dual control model. Bancroft and Janssen frame sexual response as a balance of sexual excitation and sexual inhibition systems. High inhibition under performance threat produces psychogenic ED and can maintain PE anxiety loops; treatment often reduces inhibition (safety, sensate focus) while medical therapy improves end-organ response.[13]
Psychogenic vs organic ED discriminators (not absolute rules).
- Favours psychogenic/situational: sudden onset, partner-specific failure, preserved morning/masturbatory erections, strong performance anxiety, recent relationship stress.
- Favours organic: gradual progressive course, absent nocturnal/morning erections, diabetes/CVD/smoking cluster, pelvic surgery, neurological disease, hypogonadism signs.[3][6]
PE mechanisms. Teaching frameworks emphasise serotonergic tone influencing ejaculatory threshold, penile sensory factors, genetic contributions to lifelong PE, and acquired PE secondary to ED, prostatitis, or thyroid disease. Do not claim a single gene or receptor as the sole cause in exams.[7]
Iatrogenic monoamine effects. SSRIs/SNRIs commonly reduce desire and delay orgasm/ejaculation via serotonergic inhibition — useful when treating PE, harmful when treating depression without discussing sexual SE.[10][11][14] Antipsychotic D2 blockade and hyperprolactinaemia contribute to hypogonadism, low desire, and ED; prolactin-sparing strategies matter when psychosis control allows.[12]
Clinical presentation
Erectile disorder history language. Can he obtain an erection adequate for the sexual activity he wants? Does it collapse before completion? Is rigidity reduced? Lifelong or after a clear date (surgery, new SSRI, new partner, MI)? Situational (only with partner) or generalised (including masturbation)? Morning erections? Partner response and meaning-making (rejection, infidelity fears)?[4][6]
PE history language. Estimated IELT (intravaginal ejaculatory latency time), ability to delay, frequency of the pattern, lifelong vs acquired, avoidance of sex, anticipatory anxiety, and whether coexisting ED leads him to “finish early before losing erection.”[7]
Delayed ejaculation language. Time to ejaculation, need for extreme stimulation, anejaculation, fertility goals, and exact antidepressant/antipsychotic timeline.[10][14]
MSE. Shame, guilt, catastrophising (“I am not a man”), low mood, anxiety, substance use, and suicide risk when sexual failure collides with relationship threat. Non-judgemental permission-giving language is a CASC skill, not optional soft skill.[14]
Differential diagnosis
| Presentation | Favours | Discriminator |
|---|---|---|
| Situational ED, normal morning erections | Psychogenic / performance anxiety | Partner-specific; anxiety MSE |
| Progressive generalised ED, vascular risk | Organic / endothelial | Screen diabetes, lipids, CVD |
| Short latency from first sexual experiences | Lifelong PE | ISSM-style criteria |
| New short latency with new ED | Acquired PE secondary to ED | Treat ED first |
| Delayed ejaculation after SSRI titration | Medication-induced | Temporal drug link; remitted mood |
| ED + galactorrhoea / low desire on risperidone | Hyperprolactinaemic pathway | Prolactin, consider switch |
| Anejaculation after prostate surgery | Retrograde / surgical | Urology, not pure psychogenic |
Always include substances (alcohol, opioids, tobacco), antihypertensives, thiazides, spironolactone, finasteride, and untreated depression as competing or additive causes.[3][10][12]
Gender incongruence and sexual orientation are not erectile or ejaculatory disorders; adapt PE latency teaching beyond exclusive penile–vaginal intercourse when practices differ, using distress and control rather than a single anatomical stopwatch.[7][8]
Assessment
Structure the sexual history. Permission → open questions → phase map (desire, erection, ejaculation, satisfaction) → lifelong/acquired → situational/generalised → distress → partner factors → trauma → orientation/identity → medication/substance timeline.[4][14]
Scales.
- IIEF (International Index of Erectile Function; Rosen) — multidimensional ED assessment; shortened IIEF-5 often used clinically for severity and response tracking.[4]
- PE: self-estimated IELT, structured ISSM criteria, and PE-specific screening tools where available.[7]
- Mood/anxiety screens when depression or panic coexists; sexual dysfunction is bidirectional with MDD and antidepressant treatment.[14]
Medical review. BP, BMI, diabetes symptoms, CVD history, pelvic/neurological history, and genital examination by an appropriate clinician when indicated (not every pure situational psychogenic case needs immediate invasive work-up, but midlife generalised ED does need medical risk work-up).[6]
Investigations
- ED baseline risk labs: glucose/HbA1c, lipids; morning total testosterone if hypogonadism signs, low desire, or unexplained ED; free testosterone/SHBG as indicated.[6]
- Prolactin when antipsychotic-related hypogonadism, galactorrhoea, or unexplained low desire/ED cluster is present.[12]
- TFTs and other endocrine tests as clinically directed — not shotgun panels for clear situational psychogenic ED with preserved morning erections.[3][6]
- Specialist vascular testing / penile Doppler when results will change management (urology/sexual medicine), not as default psychiatry clinic kit.[6]
- Cardiac suitability before PDE5i in men with significant CV disease — AUA-aligned shared decision and safety framing; never combine with nitrates.[5][6]
Acute and emergency management
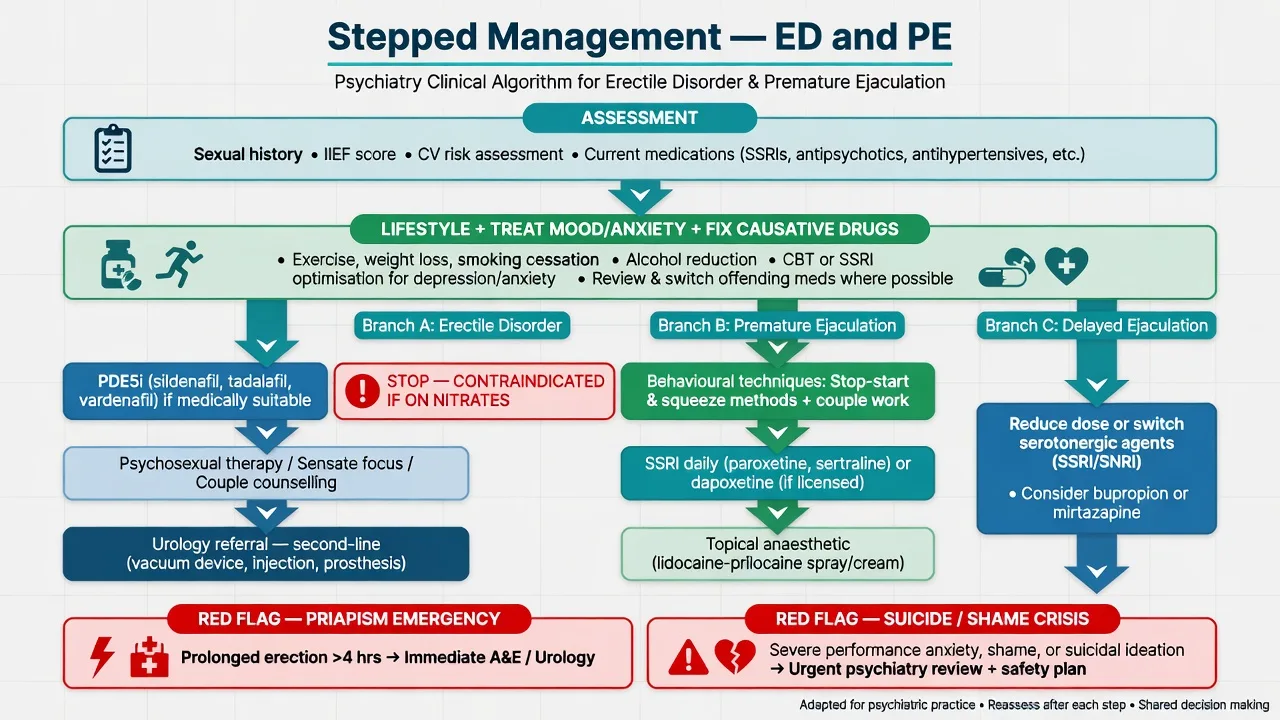
- Priapism (prolonged painful erection, especially after intracavernosal agents; rare with oral PDE5i alone) is a urological emergency — do not “wait and see” beyond local emergency time thresholds.[6]
- Suicidal crisis after sexual humiliation, relationship collapse, or infertility despair — standard suicide risk pathway and safety planning.[14]
- Acute coronary syndrome during sexual activity — medical emergency first; later sexual counselling and cardiac rehabilitation pathways.
Definitive management
Shared foundations
Education, smoking cessation, alcohol reduction, exercise, weight management, sleep optimisation, and treatment of depression/anxiety are not “optional lifestyle leaflets” — they are first-line disease modifiers for sexual function.[3][6] Psychosexual therapy (sensate focus, performance-anxiety CBT, couple work) addresses spectatoring and relationship meaning even when a PDE5i is also used.[7][13]
Erectile disorder — medical therapy
Oral PDE5 inhibitors are first-line pharmacotherapy for many men with ED after medical suitability assessment (AUA guideline framing).[6] Pivotal randomised evidence for oral sildenafil established efficacy and tolerability for ED and launched the modern PDE5i era.[5]
Practical fellowship dosing concepts (always check current product information, age, hepatic impairment, and interactions; local formulary/PBS rules apply):
- Sildenafil: commonly 25–100 mg oral as needed, typically taken about 1 hour before sexual activity; high-fat meals may delay onset; shorter duration window than tadalafil.
- Tadalafil: as-needed dosing (commonly 10–20 mg oral in many labels) or low-dose daily regimens where licensed for ED; longer duration window useful for spontaneity.
- Monitoring: efficacy, headache, flushing, dyspepsia, visual changes, hearing changes; stop and urgent review for chest pain or priapism.
- Absolute safety: no concurrent nitrates; caution with alpha-blockers (hypotension); assess CV risk before prescribing.[5][6]
Second-line / specialist: vacuum erection devices, intraurethral or intracavernosal alprostadil, and penile prosthesis for refractory organic ED — psychiatry’s role is psychosexual readiness, mood, couple adjustment, and realistic expectation setting alongside urology.[6]
Premature ejaculation
ISSM-aligned care combines behavioural techniques (stop-start, squeeze, sensate focus, couple therapy) with pharmacotherapy when distress is significant.[7]
Pharmacotherapy options (region-dependent licensing):
- Daily SSRIs used for PE (classic exam agents: paroxetine, sertraline, fluoxetine) — exploit serotonergic delay of ejaculation; counsel on other sexual SE, mood effects, and discontinuation.
- On-demand strategies where used (including dapoxetine where licensed).
- Dapoxetine: short-acting SSRI developed for on-demand PE; integrated analysis of double-blind RCTs showed efficacy and tolerability versus placebo (Pryor et al., Lancet). Availability and PBS/formulary status vary by jurisdiction — state regional access honestly.[9][7]
- Topical local anaesthetics for selected men; treat coexisting ED first when both are present (ISSM pearl).[7]
Delayed ejaculation and iatrogenic sexual dysfunction
For SSRI-related delayed ejaculation/anorgasmia: validate impact on adherence; options include watchful waiting if mild and depression unstable, dose reduction if safe, switch to a relatively lower sexual-side-effect antidepressant (e.g. bupropion, mirtazapine, or vortioxetine where clinically appropriate and available), or PDE5i adjunct when the phenotype is primarily erectile.[10][11][14]
For antipsychotic-related ED/low desire: assess prolactin, consider prolactin-sparing switch when psychosis allows, and address metabolic health; PDE5i may help residual ED after optimisation.[12]
AUA ED Guideline (2018): shared decision-making, thorough evaluation including CV risk, PDE5i as primary oral therapy for many suitable men, and structured pathways to specialist options.[6] ISSM PE guidelines: diagnostic latency/control/distress triad, lifelong vs acquired, behavioural plus pharmacological algorithms, treat concurrent ED first.[7] ANZ practice: no single RANZCP sexual-dysfunction CPG replaces AUA/ISSM evidence; use local PBS/formulary constraints for PDE5i and dapoxetine, cardiology liaison for nitrate users, and GP shared care for stable responders. NICE/APA interface: psychotropic sexual side-effect literacy and depression treatment decisions often dominate psychiatric clinic presentations even when the end-organ treatment is urological.[10][14]
Special populations and scenarios
- Older adults: organic ED prevalence rises; still offer PDE5i if medically suitable; scrutinise polypharmacy and CV disease; avoid ageist nihilism.[2][6]
- Young adults: PE and situational ED common; exclude substances and performance-anxiety loops; careful SSRI risk–benefit if depression and PE coexist.[7][14]
- Diabetes / post-prostatectomy: high organic burden — early medical/urological collaboration and couple psychosexual support.[3][6]
- Intellectual disability: adapted communication, capacity for sexual health decisions, exclude pain and medication causes.
- LGBTQ+ men: same physiology; adapt PE latency definitions to the sexual practices described; do not force vaginal-penetration-only criteria.
- Cultural/religious contexts: shame and help-seeking barriers; permission-giving history is therapeutic.
Complications and pitfalls
- Prescribing PDE5i with nitrates or unstable cardiac disease.[5][6]
- Treating ED as a lifestyle joke while missing diabetes and CVD.
- Ignoring SSRI causation because “mood is better.”[10][11]
- Using antiandrogens for PE/ED — wrong pathway (not sexual-dysfunction treatment).
- Pathologising normal latency variation without distress.
- Individual-only framing that ignores partner meaning and couple dynamics.
- Treating PE with PDE5i alone when there is no ED (limited role unless coexisting ED).[7]
Prognosis and disposition
Psychogenic ED often improves with integrated psychosexual care and optional PDE5i to break the failure cycle. Organic ED may need long-term medical/urological management with psychiatric support for mood and couple adjustment.[6][13] Lifelong PE tends to persist without behavioural or pharmacological treatment but responds to combined approaches in many men.[7][9] Iatrogenic delayed ejaculation is frequently reversible after antidepressant optimisation.[10][14]
Disposition. GP shared care for stable PDE5i responders; sexual medicine/urology for refractory or second-line device/surgical pathways; crisis services for suicidality; closer psychiatric follow-up while changing antidepressants or antipsychotics for sexual SE.[6][10][12][14]
Exam pearls
ERECTION PLAN (ED and PE clinic)
References
- [1]Laumann EO, Paik A, Rosen RC Sexual dysfunction in the United States: prevalence and predictors JAMA, 1999.PMID 10022110
- [2]McCabe MP, Sharlip ID, Lewis R, et al. Incidence and Prevalence of Sexual Dysfunction in Women and Men: A Consensus Statement from the Fourth International Consultation on Sexual Medicine 2015 J Sex Med, 2016.PMID 26953829
- [3]McCabe MP, Sharlip ID, Lewis R, et al. Risk Factors for Sexual Dysfunction Among Women and Men: A Consensus Statement From the Fourth International Consultation on Sexual Medicine 2015 J Sex Med, 2016.PMID 26953830
- [4]Rosen RC, Riley A, Wagner G, et al. The international index of erectile function (IIEF): a multidimensional scale for assessment of erectile dysfunction Urology, 1997.PMID 9187685
- [5]Goldstein I, Lue TF, Padma-Nathan H, et al. Oral sildenafil in the treatment of erectile dysfunction. Sildenafil Study Group N Engl J Med, 1998.PMID 9580646
- [6]Burnett AL, Nehra A, Breau RH, et al. Erectile Dysfunction: AUA Guideline J Urol, 2018.PMID 29746858
- [7]Althof SE, McMahon CG, Waldinger MD, et al. An update of the International Society of Sexual Medicine's guidelines for the diagnosis and treatment of premature ejaculation (PE) J Sex Med, 2014.PMID 24848686
- [8]Waldinger MD, Schweitzer DH Differences between ICD-11 MMS and DSM-5 definition of premature ejaculation: a continuation of historical inadequacies and a source of serious misinterpretations by some scientists Int J Impot Res, 2019.PMID 30659291
- [9]Pryor JL, Althof SE, Steidle C, et al. Efficacy and tolerability of dapoxetine in treatment of premature ejaculation: an integrated analysis of two double-blind, randomised controlled trials Lancet, 2006.PMID 16962882
- [10]Montejo AL, Llorca G, Izquierdo JA, Rico-Villademoros F Incidence of sexual dysfunction associated with antidepressant agents: a prospective multicenter study of 1022 outpatients J Clin Psychiatry, 2001.PMID 11229449
- [11]Serretti A, Chiesa A Treatment-emergent sexual dysfunction related to antidepressants: a meta-analysis J Clin Psychopharmacol, 2009.PMID 19440080
- [12]Montejo AL, de Alarcón R, Prieto N, et al. Management Strategies for Antipsychotic-Related Sexual Dysfunction: A Clinical Approach J Clin Med, 2021.PMID 33467621
- [13]Bancroft J, Graham CA, Janssen E, Sanders SA The dual control model: current status and future directions J Sex Res, 2009.PMID 19308839
- [14]Clayton AH, El Haddad S, Iluonakhamhe JP, et al. Sexual dysfunction associated with major depressive disorder and antidepressant treatment Expert Opin Drug Saf, 2014.PMID 25148932