Psych · Specialty psychiatry — sexual medicine interface
Female sexual interest, arousal and pain disorders
Also known as Female sexual interest/arousal disorder · FSIAD · Hypoactive sexual desire disorder · HSDD · Female sexual arousal disorder · Genito-pelvic pain/penetration disorder · GPPPD · Vaginismus · Dyspareunia · Vulvodynia · Genitourinary syndrome of menopause · GSM · Flibanserin · Bremelanotide
Exam-exhaustive fellowship atlas on female sexual interest/arousal disorder and genito-pelvic pain/penetration disorder — DSM-5-TR vs ICD-11 nosology, Basson responsive desire and dual-control models, epidemiology with distress thresholds, SSRI and medical differentials, FSFI-informed assessment, stepped psychosexual care, flibanserin/bremelanotide/testosterone pathways, GSM local therapies, and exposure/physio for pain. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Female sexual function is a high-yield specialty interface for FRANZCP MEQs, MRCPsych theory/CASC, and ABPN-style items because examiners test nosology precision, medication literacy, non-stigmatising history skills, and stepped care rather than moral commentary. A candidate who reads only this topic should defend classification deltas, mechanisms, differentials (especially SSRI-related), assessment, and evidence-based management of interest/arousal and genito-pelvic pain presentations at consultant depth.[3][7][14]
Definition and classification
Sexual dysfunction in modern manuals is a clinically significant disturbance in sexual response or pleasure with distress or interpersonal difficulty, organised by phase and by lifelong versus acquired and generalised versus situational course. Frequency alone is never enough.[5][14]
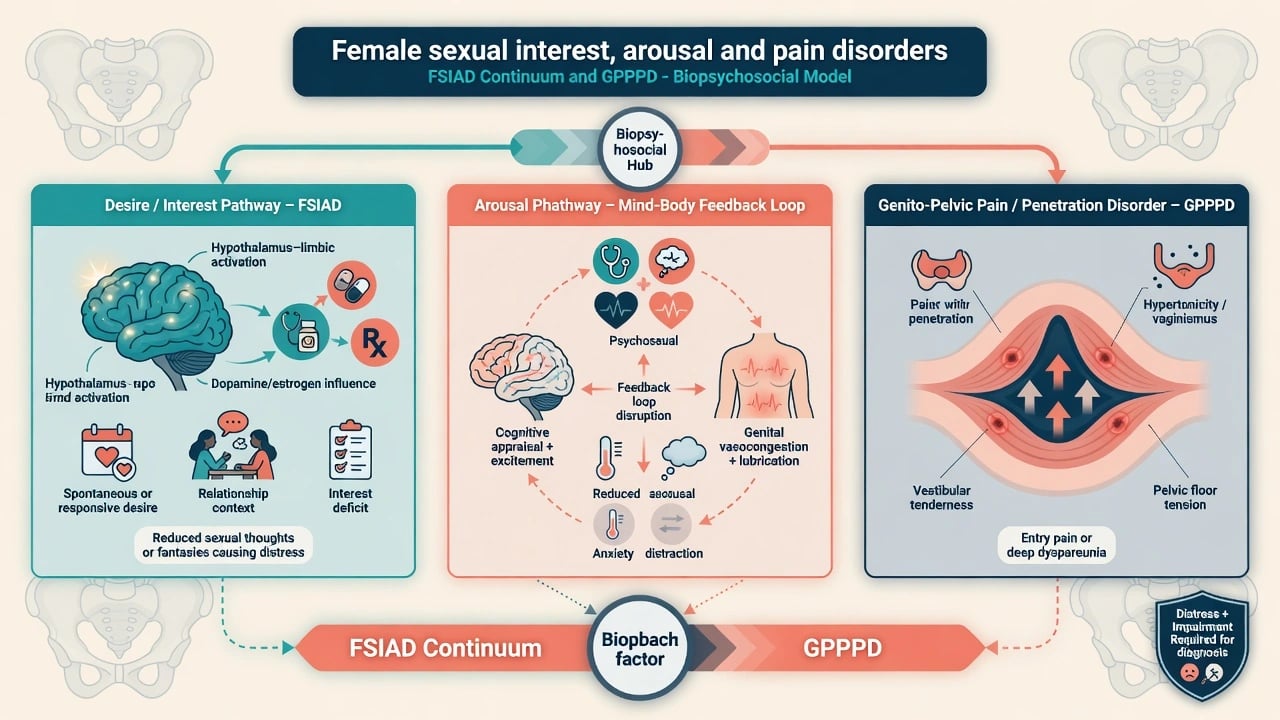
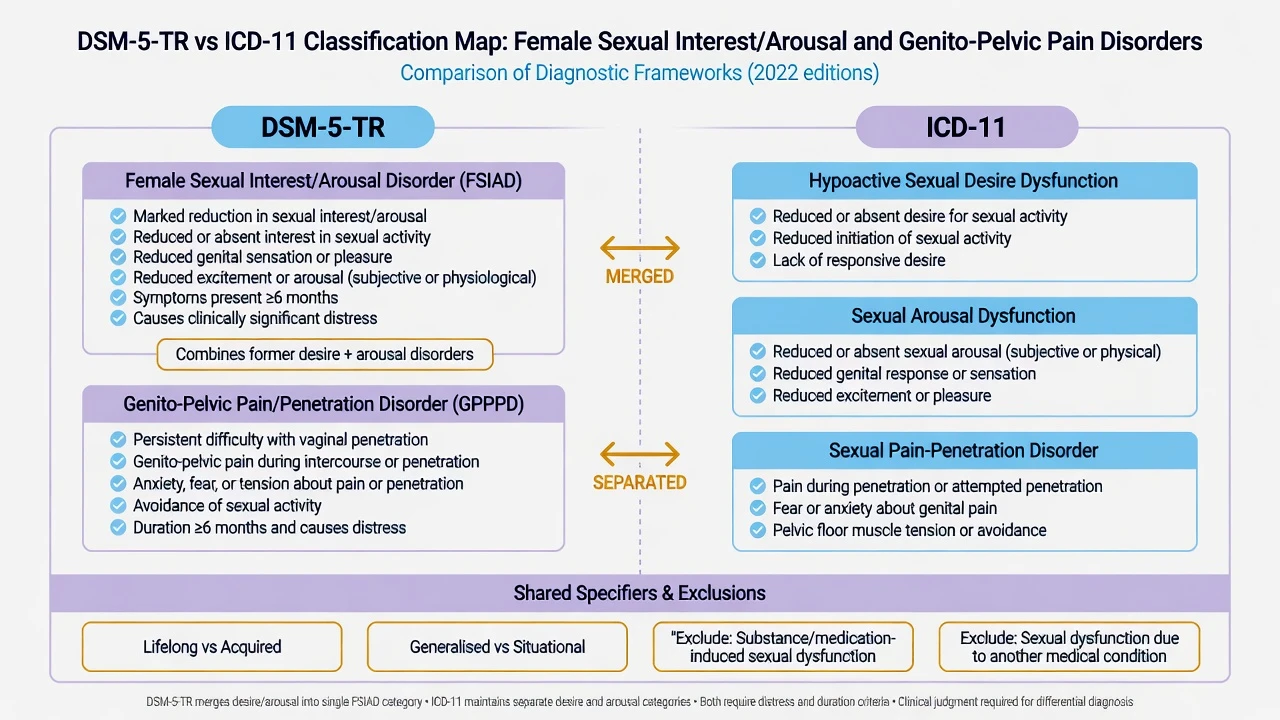
DSM-5-TR Female Sexual Interest/Arousal Disorder (FSIAD) requires a reduced interest and/or arousal pattern (absent or reduced interest, erotic thoughts, initiation or receptivity, excitement/pleasure, genital or nongenital sensations, and/or interest in response to cues — multiple features across contexts) for at least 6 months, with clinically significant distress, not better explained by severe relationship violence, another mental disorder alone, substances/medications, or another medical condition as the exclusive cause. Specifiers: lifelong/acquired; generalised/situational; mild/moderate/severe.[14]
DSM-5-TR Genito-Pelvic Pain/Penetration Disorder (GPPPD) covers one or more of: difficulty with vaginal penetration during intercourse; marked vulvovaginal or pelvic pain during penetration attempts; marked fear or anxiety about pain in anticipation of, during, or as a result of penetration; and marked tensing or tightening of the pelvic floor muscles during attempted penetration — again with duration and distress thresholds and standard exclusions.[5]
ICD-11 typically separates hypoactive sexual desire dysfunction, sexual arousal dysfunction, and sexual pain-penetration disorder, reflecting a major examinable divergence from the DSM-5-TR merger of desire and arousal into FSIAD. In viva, state both systems and code to local practice.[5][14]
FSIAD (DSM-5-TR)
- Desire + arousal features combined
- ≥6 months + distress
- Lifelong/acquired; generalised/situational
- Exclude pure medication/medical cause
ICD-11 desire/arousal
- Often coded separately
- Hypoactive desire dysfunction
- Sexual arousal dysfunction
- Useful when one phase dominates
GPPPD / pain-penetration
- Pain, fear, tension, penetration difficulty
- Vaginismus/dyspareunia continuum
- Tissue + pelvic floor + fear loops
- Needs gynaecology/physio interface
Not a disorder
- Low desire without distress
- Asexual identity without impairment
- Temporary life-stress change
- Partner demand without patient criteria
Epidemiology and risk
Population surveys show high rates of any sexual problem in women, but distress-qualified rates are substantially lower — PRESIDE-type data are examinable for that gap, and ICSM consensus statements emphasise method-dependent prevalence.[3][4][5] Laumann and colleagues classically documented substantial female sexual dysfunction prevalence with strong associations to age, health, and relationship factors.[3]
Key risk correlates: depression and anxiety, relationship dissatisfaction, history of sexual trauma, chronic pain, diabetes and cardiovascular disease, cancer therapies, menopause/GSM, and psychotropic medications (SSRIs/SNRIs; prolactin-elevating antipsychotics).[4][5][7] Partner dysfunction and coercive dynamics can maintain symptoms and must be assessed without blaming the presenting patient.
Mechanisms
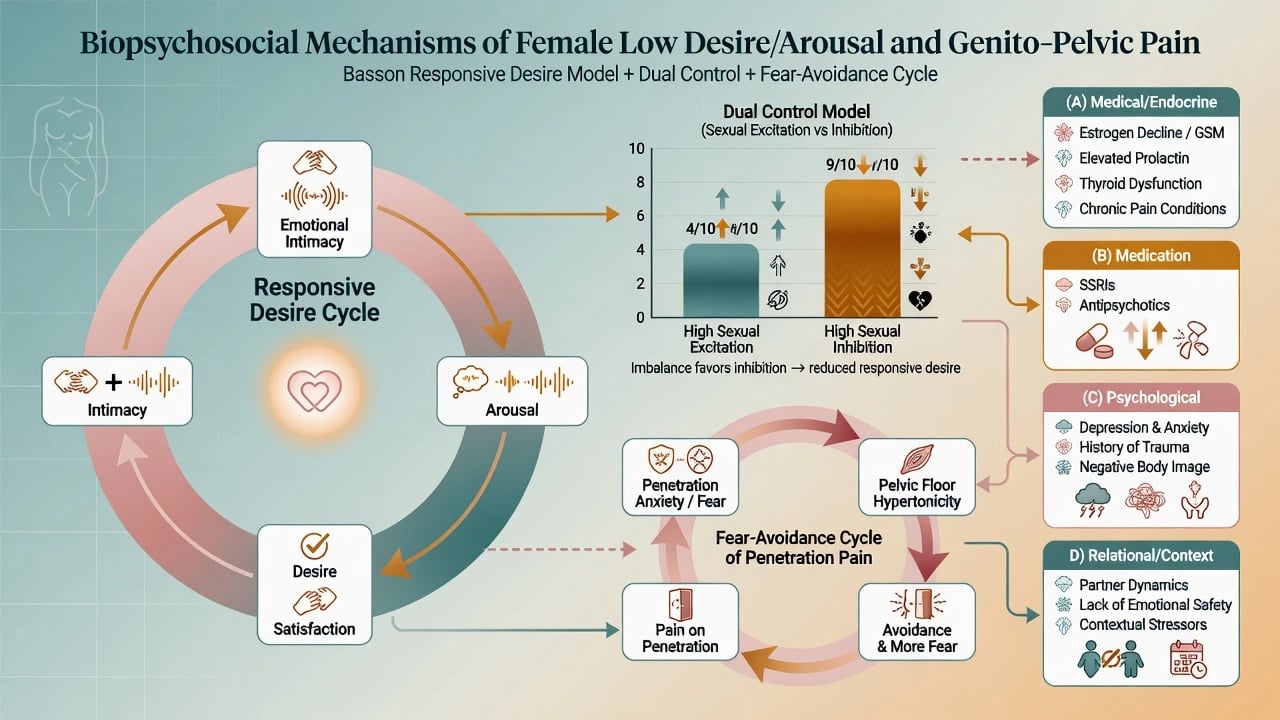
Basson responsive desire model. Many women experience desire after sexual stimuli and emerging arousal within a context of emotional intimacy and incentives, rather than only spontaneous linear desire-first sequencing. This reframes “I never feel desire first” as potentially normal physiology, not automatic pathology.[1]
Dual control model. Sexual response reflects balance between sexual excitation and sexual inhibition systems; high inhibition (performance anxiety, threat, distraction, medication) and low excitation predispose to low desire/arousal problems.[6]
Neurochemistry teaching. Dopaminergic and noradrenergic pathways generally facilitate desire; serotonergic tone (especially SSRI effects) often inhibits. This underpins medication-induced dysfunction and the pharmacology of agents such as flibanserin (multifunctional serotonergic modulator teaching) and bupropion (dopaminergic/noradrenergic).[7][8][9][10]
Pain mechanisms. GPPPD sits on tissue (infection, dermatoses, endometriosis, GSM/atrophy), pelvic floor hypertonicity, central sensitisation, and fear-avoidance loops in which anticipated pain increases tension and avoidance, further impairing penetration tolerance.[5][13]
Clinical presentation
Interest/desire: reduced sexual thoughts, avoidance of initiation, desire discrepancy with a partner, or loss of prior interest with distress. Clarify whether pleasure is still possible when engaged (helps separate global anhedonia from phase-specific desire problems).[5][14]
Arousal: reduced subjective excitement, impaired sense of genital responsiveness/lubrication, need for prolonged stimulation, body-not-responding narratives.[2][5]
Pain/penetration: entry pain, deep pain, inability to tolerate tampons/speculum/penetration, anticipatory anxiety, avoidance of intimacy and of gynaecological care — lifelong “vaginismus” patterns versus acquired dyspareunia after infection, birth trauma, or menopause.[5][13]
Interview skill. Use plain, respectful language; ask permission; avoid heteronormative assumptions; screen for violence and coercion. Include mood, trauma, body image, substances, fertility goals, and full medication list.[7][14]
Differential diagnosis
Differential discriminators for female sexual interest, arousal, and pain presentations are summarised below.[5][7][8][13][14]
| Presentation | Favours | Discriminator |
|---|---|---|
| Low desire + low mood, anhedonia, poor energy | MDD secondary effect | Treat depression; reassess residual sexual symptoms |
| New dysfunction after SSRI/SNRI start or dose rise | Medication-induced | Timeline; Montejo/Serretti-order risk literacy |
| Amenorrhoea/galactorrhoea + low desire | Hyperprolactinaemia | Antipsychotic review; prolactin if indicated |
| Dryness, dyspareunia after menopause | GSM/atrophy | Local estrogen pathway more relevant than “just therapy” |
| Lifelong inability to penetrate, high fear | Primary vaginismus pattern | Exposure + physio, not forced intercourse |
| Desire mismatch, patient not distressed | Not a disorder | Couple work; do not medicalise |
| Arousal only with trauma triggers/flashbacks | PTSD interface | Trauma-focused care + safety |
| Sudden neuro deficit / bleeding / mass | Organic red flag | Urgent medical/gynae pathway |
Always separate individual disorder criteria from relationship problems and from identity (asexual spectrum without distress is not pathology).[5][7][8]
Assessment
- Confidential sexual history — onset, course, phases (desire, arousal, orgasm, pain), contexts, distress, partner factors, consent/safety.[14]
- Psychiatric comorbidity — depression, anxiety, PTSD, OCD/body image, substance use, suicide risk.[4][5]
- Medication and medical review — antidepressants, antipsychotics, opioids, anti-androgens; menopause, diabetes, pelvic disease, cancer treatment.[7][8]
- Measurement — FSFI domains (desire, arousal, lubrication, orgasm, satisfaction, pain) support baseline and response tracking; diagnosis remains clinical.[2]
- Examination/referral threshold — gynaecology for pain, bleeding, discharge, masses, GSM; endocrinology for clear hormonal syndromes; pelvic floor physiotherapy for hypertonicity; do not force exam when trauma-related avoidance is severe without preparation.[5][14]
- Labs — targeted (TSH, prolactin when indicated, metabolic panel, pregnancy test, STI risk-based) — not indiscriminate hormone fishing for every desire complaint.[14]
Acute and safety priorities
Definitive management
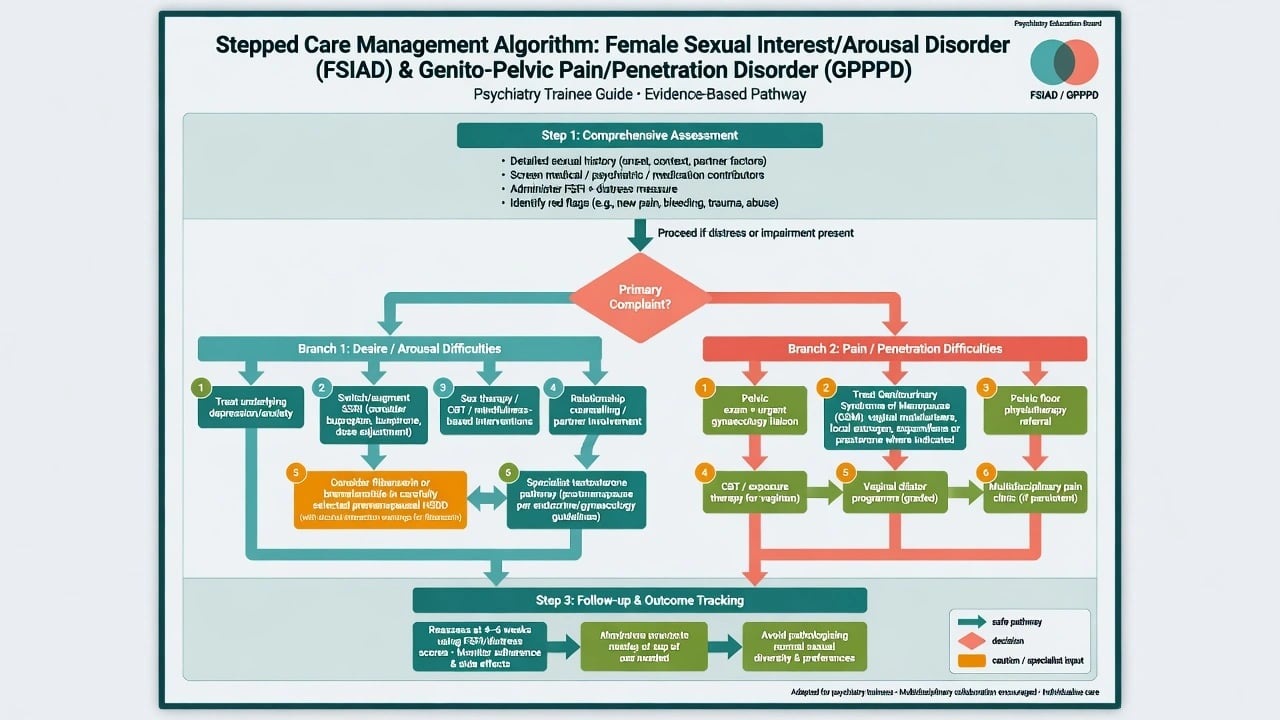
Stepped psychosexual care (first-line foundation)
Education using Basson/dual-control language; optimise sleep, substances, and relationship safety; individual and/or couple sex therapy; CBT for performance anxiety and catastrophic pain expectations; mindfulness-based approaches for desire/arousal (Brotto-order teaching lineage); graded sensual focus exercises when appropriate; treat comorbid depression/anxiety/PTSD concurrently rather than waiting for perfect mood remittance alone.[1][6][14]
ISSWSH-style process-of-care emphasises identification of modifiable biopsychosocial factors before escalating to specialised pharmacotherapy for HSDD.[14]
Medication-induced dysfunction
SSRIs/SNRIs carry high rates of treatment-emergent sexual dysfunction in prospective and meta-analytic data.[7][8] Strategies (individualise to mood stability and suicide risk):
- Wait for adaptation if early and mild; dose reduction if safe.[8]
- Switch to agents with lower sexual burden (teaching hierarchy often includes bupropion, mirtazapine, vortioxetine — choice depends on residual depression, anxiety, seizure risk, and sleep).[8][9]
- Adjunctive bupropion when mood is stable on an SSRI and sexual side-effects dominate (monitor activation, BP, seizure risk).[9]
- Avoid unsupervised “drug holidays” that risk relapse or discontinuation symptoms.[7][8]
Pharmacological options for HSDD / FSIAD (selected cases)
Bupropion sustained-release has randomised evidence in premenopausal HSDD populations; typical clinical teaching uses bupropion SR 150 mg orally once daily, titrating toward 150 mg orally twice daily if tolerated (max per product info; avoid in seizure disorder, abrupt alcohol/benzo withdrawal, bulimia/anorexia history).[9]
Flibanserin 100 mg orally once daily at bedtime for premenopausal HSDD: modest average benefits in trials such as BEGONIA; no alcohol co-use (severe hypotension/syncope); CYP3A4 interaction caution; somnolence; availability and regulatory status vary by region.[10]
Bremelanotide 1.75 mg subcutaneous as needed (teaching: inject at least about 45 minutes before anticipated sexual activity; maximum 8 doses per month): RECONNECT phase 3 programme showed benefit for HSDD; nausea is common; transient BP increases and focal hyperpigmentation are safety teaching points.[11]
Testosterone therapy in postmenopausal women with HSDD: global consensus supports consideration after biopsychosocial optimisation, with specialist dosing/monitoring; often off-label in ANZ practice — document informed consent and avoid supraphysiological levels.[12]
PDE5 inhibitors have limited, inconsistent roles for primary female desire disorders and are not first-line psychiatry answers for FSIAD.[14]
Genito-pelvic pain / penetration
- Identify tissue contributors — infection, dermatoses, endometriosis, postpartum trauma, GSM.[5]
- GSM care — regular vaginal moisturisers and lubricants; low-dose vaginal estrogen when not contraindicated; oral ospemifene or vaginal prasterone (DHEA) pathways in selected postmenopausal dyspareunia (product info, VTE/estrogen-sensitive cancer history, specialist alignment).[5][14]
- Pelvic floor physiotherapy for hypertonicity.[13]
- Psychological treatment — CBT and therapist-aided exposure / dilator programmes for lifelong vaginismus-type GPPPD improve penetration ability versus wait-list in randomised data; never recommend forced intercourse.[13]
- Multidisciplinary pain pathways for vestibulodynia/vulvodynia when local measures fail.[5][13]
ANZ / RANZCP-facing practice: prioritise holistic psychosexual formulation, medication review, gynaecology/physio liaison, and relationship safety. Flibanserin and bremelanotide access may be limited or non-PBS; testosterone for female HSDD is often specialist and off-label. NICE/APA-aligned teaching similarly emphasises psychosocial care and medical optimisation over drug-first algorithms for most patients. State regional availability honestly in exams.[12][14]
Subtypes and scenarios
- SSRI-emergent FSIAD with partial MDD response — optimise antidepressant first.[7][8]
- Perimenopausal GSM + desire loss — treat tissue and mood/relationship layers together.[5][14]
- Lifelong vaginismus / unconsummated relationship — exposure + physio; CASC communication gold.[13]
- Cancer survivorship — body image, estrogen deprivation, pain; oncology liaison.[5]
- Desire discrepancy without individual distress criteria — couple therapy framing.[5][14]
- Trauma-related avoidance — PTSD treatment, pacing, consent-centred sex therapy.[5][14]
Complications and pitfalls
Missing medication causes; medicalising low desire without distress; ignoring GSM in pain; alcohol with flibanserin; colluding with coercive partners; promising large pharmacologic effect sizes when trial benefits are modest; pathologising asexual identity; skipping safeguarding in adolescents.[10][11][14]
Prognosis and disposition
Medication-induced cases often improve with regimen change. Psychosexual therapy and exposure-based pain programmes can produce meaningful gains, though residual symptoms are common. Disposition is typically outpatient psychiatry or sexual medicine with sex therapy ± gynaecology ± pelvic floor physio; step up for risk, severe depression, or refractory complex pain.[13][14]
Special populations
Adolescents: developmental assessment, consent, safeguarding; avoid adult labelled drugs. Perinatal: desire change is common; screen depression, obstetric trauma, pain. Older adults: GSM, polypharmacy, partner health. Intellectual disability: capacity, exploitation risk, accessible education. LGBTQ+ and culturally diverse patients: inclusive goals beyond penile-vaginal intercourse; interpreter and cultural humility.[5][14]
Evidence and guidelines pearls
Name Basson, dual control, FSFI, PRESIDE/Laumann prevalence with distress framing, Montejo/Serretti antidepressant sexual dysfunction, Segraves bupropion, BEGONIA flibanserin, RECONNECT bremelanotide, global testosterone consensus, ter Kuile exposure, and ISSWSH HSDD process of care.[1][2][4][10][11][12][13][14]
Exam pearls
The DESIRE-PAIN checklist packages the high-yield safety and process-of-care points examiners expect in MEQ and CASC answers.[1][13][14]
References
- [1]Basson R The female sexual response: a different model J Sex Marital Ther, 2000.PMID 10693116
- [2]Rosen R, Brown C, Heiman J, et al. The Female Sexual Function Index (FSFI): a multidimensional self-report instrument for the assessment of female sexual function J Sex Marital Ther, 2000.PMID 10782451
- [3]Laumann EO, Paik A, Rosen RC Sexual dysfunction in the United States: prevalence and predictors JAMA, 1999.PMID 10022110
- [4]Shifren JL, Monz BU, Russo PA, et al. Sexual problems and distress in United States women: prevalence and correlates Obstet Gynecol, 2008.PMID 18978095
- [5]McCabe MP, Sharlip ID, Lewis R, et al. Incidence and Prevalence of Sexual Dysfunction in Women and Men: A Consensus Statement from the Fourth International Consultation on Sexual Medicine 2015 J Sex Med, 2016.PMID 26953829
- [6]Bancroft J, Graham CA, Janssen E, Sanders SA The dual control model: current status and future directions J Sex Res, 2009.PMID 19308839
- [7]Montejo AL, Llorca G, Izquierdo JA, Rico-Villademoros F Incidence of sexual dysfunction associated with antidepressant agents: a prospective multicenter study of 1022 outpatients J Clin Psychiatry, 2001.PMID 11229449
- [8]Serretti A, Chiesa A Treatment-emergent sexual dysfunction related to antidepressants: a meta-analysis J Clin Psychopharmacol, 2009.PMID 19440080
- [9]Segraves RT, Clayton A, Croft H, et al. Bupropion sustained release for the treatment of hypoactive sexual desire disorder in premenopausal women J Clin Psychopharmacol, 2004.PMID 15118489
- [10]Katz M, DeRogatis LR, Ackerman R, et al. Efficacy of flibanserin in women with hypoactive sexual desire disorder: results from the BEGONIA trial J Sex Med, 2013.PMID 23672269
- [11]Kingsberg SA, Clayton AH, Portman D, et al. Bremelanotide for the Treatment of Hypoactive Sexual Desire Disorder: Two Randomized Phase 3 Trials Obstet Gynecol, 2019.PMID 31599840
- [12]Davis SR, Baber R, Panay N, et al. Global Consensus Position Statement on the Use of Testosterone Therapy for Women J Clin Endocrinol Metab, 2019.PMID 31498871
- [13]ter Kuile MM, Melles R, de Groot HE, et al. Therapist-aided exposure for women with lifelong vaginismus: a randomized waiting-list control trial of efficacy J Consult Clin Psychol, 2013.PMID 24060195
- [14]Clayton AH, Goldstein I, Kim NN, et al. The International Society for the Study of Women's Sexual Health Process of Care for Management of Hypoactive Sexual Desire Disorder in Women Mayo Clin Proc, 2018.PMID 29545008