Psych · Specialty psychiatry — gender diversity ethics and systems
Gender diversity: broader clinical and ethical issues
Also known as Gender diversity · Transgender mental health · Gender minority stress · Structural stigma · Conversion therapy ethics · Non-binary care · Trans-affirming psychiatry · Healthcare discrimination transgender · Gender affirmation · LGBTQ+ psychiatry ethics
Exam-exhaustive fellowship reference on gender diversity beyond the narrow gender-dysphoria diagnostic pathway — minority stress and structural stigma, healthcare discrimination and avoidance, conversion-effort ethics, inclusive assessment and privacy, non-binary and intersectional care, resilience factors, and professional duties. Affirming, evidence-aware, non-fabricating. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
9 MCQs with explanations
Target exams
Red flags
This leaf complements gender dysphoria and affirming care (criteria, GAHT, surgery readiness). Here the examiner tests systems, ethics, stigma, and population mental health for gender-diverse people who may never meet dysphoria criteria, may want only social/legal affirmation, or present primarily with trauma, discrimination, or healthcare avoidance.[4][5][11]
Definition and classification
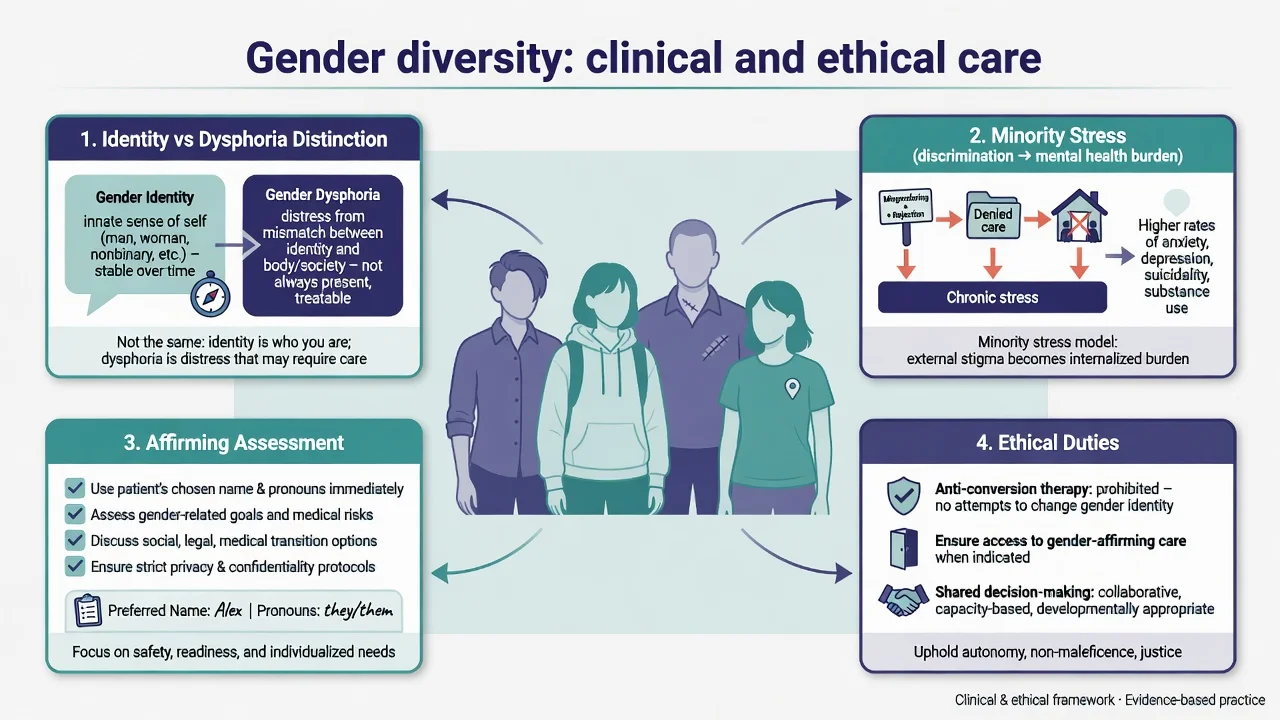
Gender diversity describes the range of gender identities and expressions that differ from cultural expectations based on sex assigned at birth (transgender, non-binary, genderqueer, and culturally specific identities). Diversity itself is not a psychiatric diagnosis.[5][11]
DSM-5-TR gender dysphoria is a distress/impairment construct: marked incongruence of sufficient duration plus clinically significant distress or functional impairment. People may be transgender or gender-diverse without meeting dysphoria criteria and still need respectful mental health care for other problems.[6][11]
ICD-11 gender incongruence is framed for clinical utility and is not classified among mental disorders — a classic exam contrast with DSM placement language.[16]
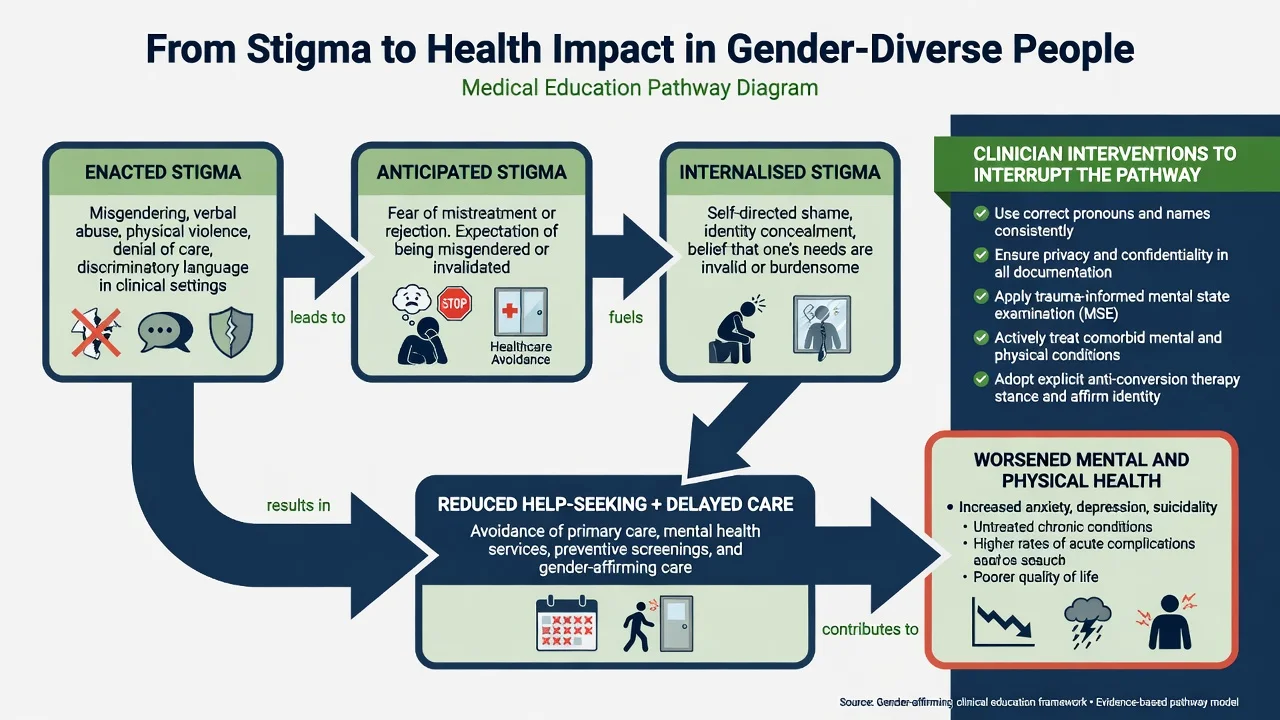
Stigma vocabulary (examinable). Enacted stigma (events of discrimination/abuse); anticipated stigma (expectation of rejection); internalised stigma (negative self-appraisals absorbed from society); structural stigma (laws, policies, service design that systematically disadvantage a group).[3][1]
Gender-diverse identity
- Lived gender identity/expression
- Not a mental disorder
- May need social/legal affirmation only
- Full human rights framing
Gender dysphoria (DSM)
- Incongruence + distress/impairment
- Clinical diagnosis when criteria met
- May prompt medical pathway liaison
- Comorbidity common
ICD-11 incongruence
- Outside mental disorders chapter
- Clinical utility coding
- Reduces pathologisation of identity
- Still needs careful assessment
Exam traps
- Equating identity with illness
- Offering conversion as therapy
- Ignoring stigma drivers
- Rubber-stamping without capacity
Epidemiology and risk
Global reviews document disproportionate burdens of violence, discrimination, HIV (especially among transgender women in many settings), barriers to care, and mental health disparities among transgender and gender-diverse populations.[4][5]
Mental health signals. Reviews of transgender youth and adults report elevated depression, anxiety, self-harm, and suicidality relative to general population comparisons. Interpret as population risk under stigma, not proof that gender diversity is inherently a mental illness.[6][7][8]
Healthcare discrimination. Discrimination in clinical settings is associated with delayed care; anticipated discrimination drives healthcare avoidance — both are clinical risk amplifiers for physical and mental health outcomes.[14][15]
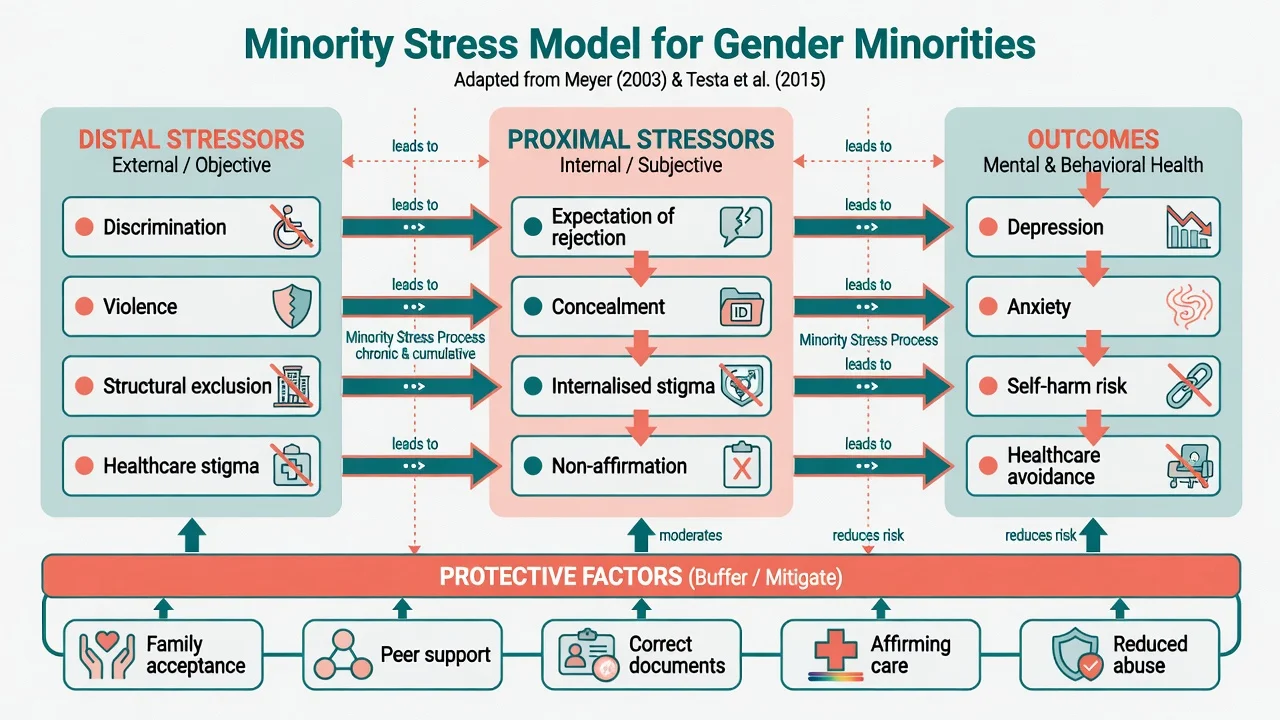
Protective factors are intervenable. Ontario respondent-driven sampling work links lower suicide risk to factors such as social support, reduced transphobia, having identity documents matching lived gender, and access to medical transition when indicated — framing prevention as social and clinical action, not fatalism.[12]
High-yield population anchors
Mechanisms — minority stress and stigma
Meyer's minority stress model (developed in LGB populations) remains the conceptual parent: chronic stress from stigma adds to general stress and elevates mental health risk via distal and proximal pathways.[1]
Gender-minority research extends this. Online US transgender samples link enacted and felt stigma with psychological distress, while peer support and identity pride show resilience associations.[2] Prospective work in transgender women links gender abuse to major depression risk, with resilience modifiers.[13] Critical reviews map stigma determinants, mechanisms, and multi-level interventions (individual coping, interpersonal affirmation, structural policy change).[3]
Gender affirmation (social, psychological, medical congruence supports) is a useful health framework, especially when discussing HIV risk environments and engagement in care among transgender women of colour — affirmation is health-protective scaffolding, not a slogan that replaces assessment.[4][5]
Clinical presentation (beyond the dysphoria clinic)
Common psychiatry interfaces that are not "start hormones tomorrow" include crisis after rejection, stigma-driven mood disorders, healthcare avoidance, and non-medical affirmation needs.[5][8][10]
- Crisis after family rejection, workplace misgendering, or hate-based violence.[5][8]
- Depression/anxiety driven by concealment and anticipated rejection.[1][2]
- Avoidance of primary care, sexual health, or psychiatric follow-up after prior discrimination.[14][15]
- Non-binary adults seeking mental health care with no desire for hormones or surgery.[10][11]
- Documentation, school, or forensic settings where safety and pronouns are the primary need.[10]
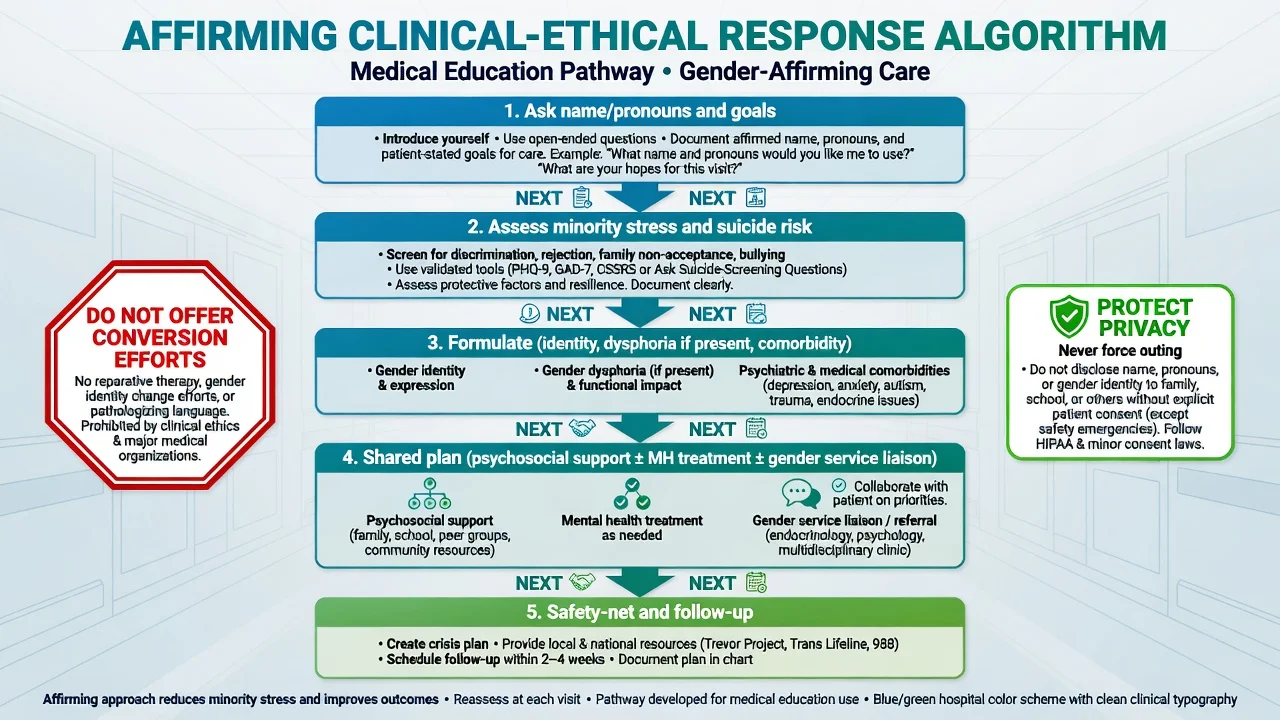
MSE language. Use affirmed name and pronouns; note trauma markers; mood/anxiety/psychosis screen; substance use; insight; suicide and self-harm risk with means; capacity elements if major decisions loom; social determinants (housing, income, community). Document function without voyeuristic genital history unless clinically necessary for a specific medical pathway.[10][11]
Differential and formulation boundaries
Formulate both minority stress and any independent mental disorder. Do not collapse one into the other.[1][2][6]
- Dysphoria pathway indicated: persistent incongruence with distress/impairment and medical goals — see sibling topic; liaison to specialist services.[6][10]
- No dysphoria diagnosis: still treat depression/PTSD/SUD; still affirm identity; do not invent a diagnosis to justify respect.[5][11]
- BDD / psychosis / trauma disruption: careful differential without automatic permanent invalidation of gender experience.[6]
- Orientation vs identity: sexual orientation is not gender identity; avoid conflation in history-taking.[11]
Assessment
- Ask preferred name, pronouns, identity labels, and what would make the encounter safe.[10][11]
- Map minority stress (abuse, discrimination, concealment, family/school/work climate).[2][13]
- Full risk assessment (suicide, self-harm, violence, vulnerability, housing).[7][12]
- Clarify goals — social affirmation, mental health care, medical transition liaison, letters/documents, or combination.[10]
- Privacy: do not out the patient to family/employer without consent except lawful safeguarding duties.[10]
- Collateral with consent; for youth, balance parental involvement with safety if home is hostile.[8]
Investigations
There is no biomarker of gender diversity or of stigma. Order investigations for concurrent illness, psychotropic safety, sexual health when indicated by risk and consent, or specialist endocrine work-up only when a medical gender pathway is active.[11][4]
Acute and emergency management
If psychosis or mania impairs decision-making capacity regarding irreversible medical steps, stabilise first while continuing respectful communication about identity.[10][11]
Definitive management — clinical and ethical pillars
1. Affirmative clinical stance
Respect identity and language; reduce enacted stigma in the clinical micro-environment; provide thorough assessment without voyeurism or pathologising curiosity.[10][11][3]
2. Treat mental illness with standard evidence-based care
Depression, anxiety, PTSD, and substance use disorders receive guideline-concordant therapies and pharmacotherapy as for any patient. Affirmation is not a substitute for treating major depression; treating depression is not a licence for conversion.[6][8]
3. Target intervenable protective factors
Social support, reduced exposure to gender-based abuse, peer connection, correct identity documents, and affirming environments are associated with lower suicide risk signals and are legitimate clinical targets (family work, advocacy letters when appropriate, school liaison, housing support).[12][2]
4. Reduce healthcare avoidance
Train teams, correct records, privacy-conscious letter writing, and trauma-informed sexual health offer reduce anticipated discrimination and delayed care.[14][15][3]
5. Conversion efforts — professional prohibition
Recalled exposure to gender identity conversion efforts is associated with psychological distress and suicide attempts in adult survey data. Conversion or reparative efforts aimed at changing gender identity are not recommended clinical practice.[9]
6. Specialist medical pathways when indicated
When gender dysphoria/incongruence and medical goals exist, liaison with gender services under frameworks such as WPATH SOC8 and endocrine guidance is appropriate; psychiatrists contribute formulation, comorbidity care, capacity assessment, and risk management — not unsupervised initiation of hormones outside competence and protocol.[10][11]
7. Ethical reasoning under uncertainty
Youth medical care, long-term outcome data quality, and regional policy are actively debated. Fellowship standard: affirm the person, state evidence limits honestly, apply decision-specific capacity, follow local law, avoid both moral panic and uncritical certainty.[10][8][16]
Special populations and intersectionality
Youth. Elevated mental health burden and family/school climate effects are well described; family acceptance is protective. Ethical care integrates developmental capacity, parental responsibility frameworks (jurisdiction-specific), school safety, and careful approach to irreversible steps.[8][10]
Transgender women and HIV risk environments. Global epidemiology supports integrated sexual health, PrEP awareness where available, violence prevention, and affirmation-informed engagement — psychiatry interfaces with trauma, depression, and substance use without reducing people to HIV risk categories.[4][5]
Non-binary people. Goals may include partial social transition or no medicalisation; do not force binary pathways.[10]
Indigenous and cultural gender systems. Culturally safe practice recognises diverse gender roles and compounds of racism plus cissexism; use local community knowledge and avoid imposing only Western binary frames.[5]
Detention, homelessness, sex work. High violence and discrimination risk; continuity of established hormones, safety planning, and non-judgemental engagement are priorities where lawful and clinically indicated.[4][5]
ANZ. Practice is shaped by professional college expectations of non-discrimination and affirmative care, public multidisciplinary gender services, anti-conversion legislative movements in some jurisdictions, and evolving youth service criteria. State principles rather than inventing statute numbers under exam pressure.[10][11]
UK/Europe. Specialist gender services and policy reviews influence youth pathways; minority stress and anti-discrimination duties remain core psychiatric competencies across systems.[10][16]
US. WPATH SOC8 and endocrine frameworks influence care while state law varies widely for adolescent medical interventions — always verify local legality; conversion-effort harm data and stigma science remain relevant nationally.[10][9][11]
Prognosis and disposition
Population mental health improves when stigma falls and support rises; individual prognosis depends on comorbidity severity, abuse exposure, housing, and access to affirming care. Residual elevated risk can persist in long-term clinic cohorts after medical transition in the sibling evidence base — so ongoing mental health care is part of good practice, not a failure of affirmation.[6][12][7]
Disposition. Community psychiatry/psychology + primary care + peer support ± gender clinic liaison; crisis services for acute risk; social work for housing/benefits; sexual health when indicated.[10][11][12]
Exam pearls
- Identity is not diagnosis; DSM dysphoria needs distress/impairment. [6][16]
- Minority stress is the mechanism answer for excess MH burden. [1][2][3]
- Conversion efforts: do not offer; harm associations exist. [9]
- Healthcare discrimination → delay/avoidance → worse outcomes. [14][15]
- Protective factors are clinical targets (Bauer-order). [12]
- CASC openers: name, pronouns, agenda, privacy, safety-net. [10][11]
- Do not invent another country's youth statutes. [10]
References
- [1]Meyer IH Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: conceptual issues and research evidence Psychol Bull, 2003.PMID 12956539
- [2]Bockting WO, Miner MH, Swinburne Romine RE, et al. Stigma, mental health, and resilience in an online sample of the US transgender population Am J Public Health, 2013.PMID 23488522
- [3]White Hughto JM, Reisner SL, Pachankis JE Transgender stigma and health: A critical review of stigma determinants, mechanisms, and interventions Soc Sci Med, 2015.PMID 26599625
- [4]Reisner SL, Poteat T, Keatley J, et al. Global health burden and needs of transgender populations: a review Lancet, 2016.PMID 27323919
- [5]Winter S, Diamond M, Green J, et al. Transgender people: health at the margins of society Lancet, 2016.PMID 27323925
- [6]Dhejne C, Van Vlerken R, Heylens G, Arcelus J Mental health and gender dysphoria: A review of the literature Int Rev Psychiatry, 2016.PMID 26835611
- [7]Marshall E, Claes L, Bouman WP, et al. Non-suicidal self-injury and suicidality in trans people: A systematic review of the literature Int Rev Psychiatry, 2016.PMID 26329283
- [8]Connolly MD, Zervos MJ, Barone CJ 2nd, et al. The Mental Health of Transgender Youth: Advances in Understanding J Adolesc Health, 2016.PMID 27544457
- [9]Turban JL, Beckwith N, Reisner SL, Keuroghlian AS Association Between Recalled Exposure to Gender Identity Conversion Efforts and Psychological Distress and Suicide Attempts Among Transgender Adults JAMA Psychiatry, 2020.PMID 31509158
- [10]Coleman E, Radix AE, Bouman WP, et al. Standards of Care for the Health of Transgender and Gender Diverse People, Version 8 Int J Transgend Health, 2022.PMID 36238954
- [11]Safer JD, Tangpricha V Care of Transgender Persons N Engl J Med, 2019.PMID 31851801
- [12]Bauer GR, Scheim AI, Pyne J, et al. Intervenable factors associated with suicide risk in transgender persons: a respondent driven sampling study in Ontario, Canada BMC Public Health, 2015.PMID 26032733
- [13]Nuttbrock L, Bockting W, Rosenblum A, et al. Gender abuse and major depression among transgender women: a prospective study of vulnerability and resilience Am J Public Health, 2014.PMID 24328655
- [14]Jaffee KD, Shires DA, Stroumsa D Discrimination and Delayed Health Care Among Transgender Women and Men: Implications for Improving Medical Education and Health Care Delivery Med Care, 2016.PMID 27314263
- [15]Kcomt L, Gorey KM, Barrett BJ, McCabe SE Healthcare avoidance due to anticipated discrimination among transgender people: A call to create trans-affirmative environments Soc Work Health Care, 2020.PMID 32529022
- [16]Drescher J, Cohen-Kettenis PT, Reed GM Gender incongruence of childhood in the ICD-11: controversies, proposal, and rationale Lancet Psychiatry, 2016.PMID 26946394