Psych · Specialty psychiatry — gender and sexuality
Gender dysphoria and affirming care
Also known as Gender dysphoria · Gender incongruence · Transgender mental health · Gender-affirming care · Gender-affirming hormone therapy · GAHT · WPATH · Gender identity · Non-binary gender · Puberty suppression
Exam-exhaustive fellowship reference on gender dysphoria (DSM-5-TR) and ICD-11 gender incongruence — comprehensive assessment, minority stress and mental health comorbidity, affirmative care principles, endocrine and surgical pathway liaison, capacity and consent with developmental nuance, and evidence-aware synthesis without stigma. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Gender dysphoria is a high-stakes fellowship topic at the interface of psychiatry, endocrinology, ethics, and law. FRANZCP MEQs test differential diagnosis, risk, capacity, and liaison. MRCPsych CASCs test respectful communication and explanation of pathways. ABPN items test DSM criteria, comorbidity, and affirmative care principles. Write without pathologising identity and without abandoning clinical rigour.[1][7][18]
Definition and classification
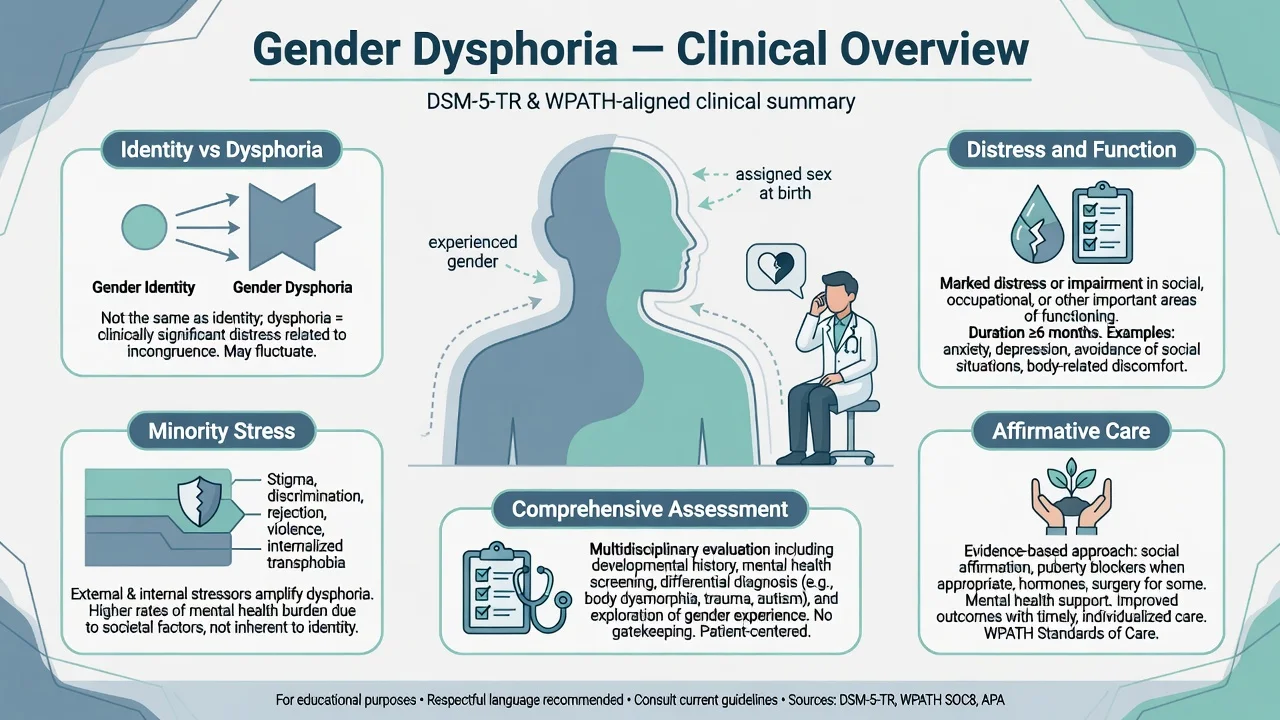
DSM-5-TR gender dysphoria requires a marked incongruence between one's experienced/expressed gender and assigned gender, of at least 6 months, associated with clinically significant distress or impairment. Being transgender or gender-diverse without that distress/impairment package is not the same construct as the DSM diagnosis.[1][22]
Adult/adolescent Criterion A features (teaching list). Strong desire to be of another gender (or alternative gender different from assigned); strong desire to be treated as another gender; marked incongruence between experienced gender and primary and/or secondary sex characteristics; strong desire for the sex characteristics of the experienced gender; strong desire to be rid of one's sex characteristics (or, in adolescents, prevent development of secondary characteristics); conviction that one has the typical feelings and reactions of another gender. A specified number of features plus distress/impairment complete the diagnosis — quote the manual under exam pressure rather than inventing a count if unsure.[1]
Childhood criteria emphasise cross-gender preferences, roles, and toys; rejection of anatomic sex characteristics; and insistence on being another gender, with duration and intensity thresholds distinct from adult criteria. Qualitative and quantitative follow-up work shows some children desist and some persist into adolescence — individual prediction is imperfect.[10][11]
ICD-11 gender incongruence of adolescence/adulthood (and a separate childhood category) is framed for clinical utility and is not classified among mental disorders — an examinable divergence from DSM placement language. The clinical task remains careful assessment of incongruence, distress, function, comorbidity, and goals of care.[2]
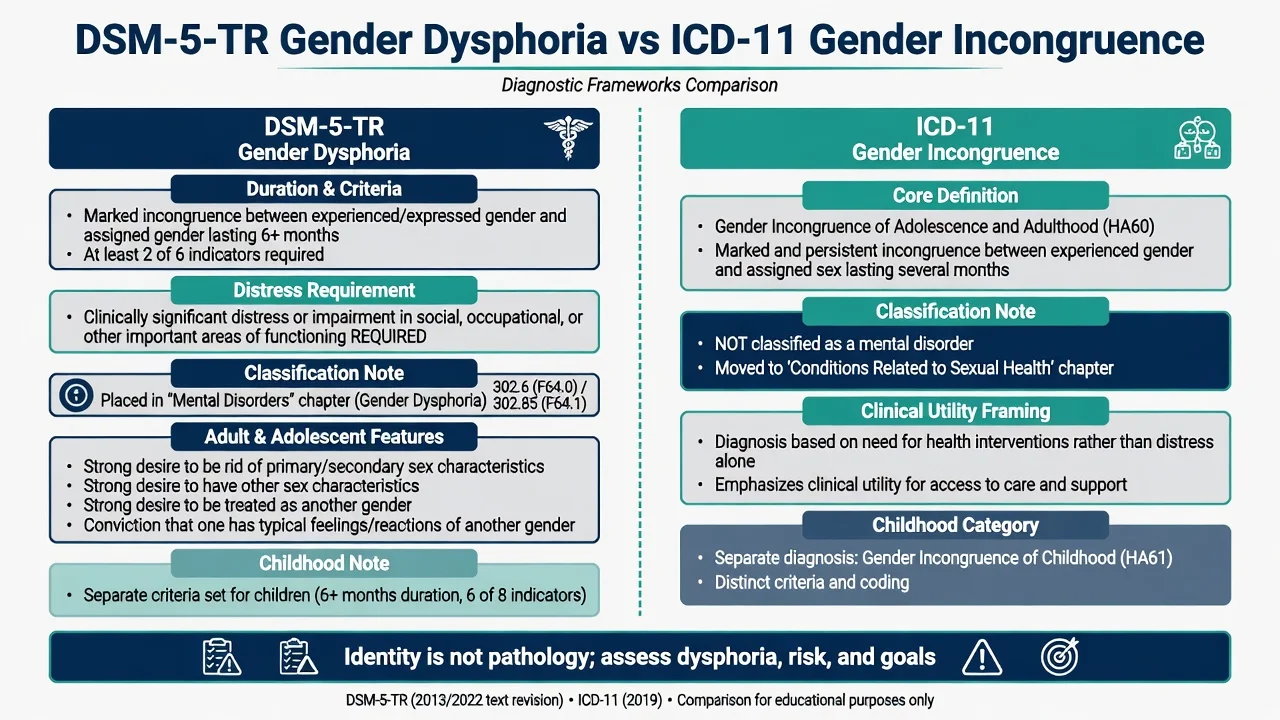
DSM-5-TR gender dysphoria
- Incongruence ≥6 months
- Distress or impairment required
- Adult/adolescent and childhood criteria sets
- Placed among mental disorders for coding utility
ICD-11 gender incongruence
- Marked and persistent incongruence
- Sexual health chapter framing
- Not classified as a mental disorder
- Separate childhood category
Related but distinct
- Transgender identity without clinical dysphoria
- Non-binary goals of partial medicalisation
- Post-transition status with residual needs
- DSD/intersex medical context when present
Exam traps
- Equating identity with diagnosis
- Assuming all GD is childhood-onset
- Missing BDD or psychosis differentials
- Treating conversion as legitimate therapy
Epidemiology and risk
Meta-analytic prevalence estimates for transsexualism/clinic-defined samples are low in absolute terms but methodologically heterogeneous; clinic referral volumes have risen markedly in many countries, with changing age and sex-ratio patterns that examiners discuss as epidemiology under evolution rather than a single fixed rate.[3][1]
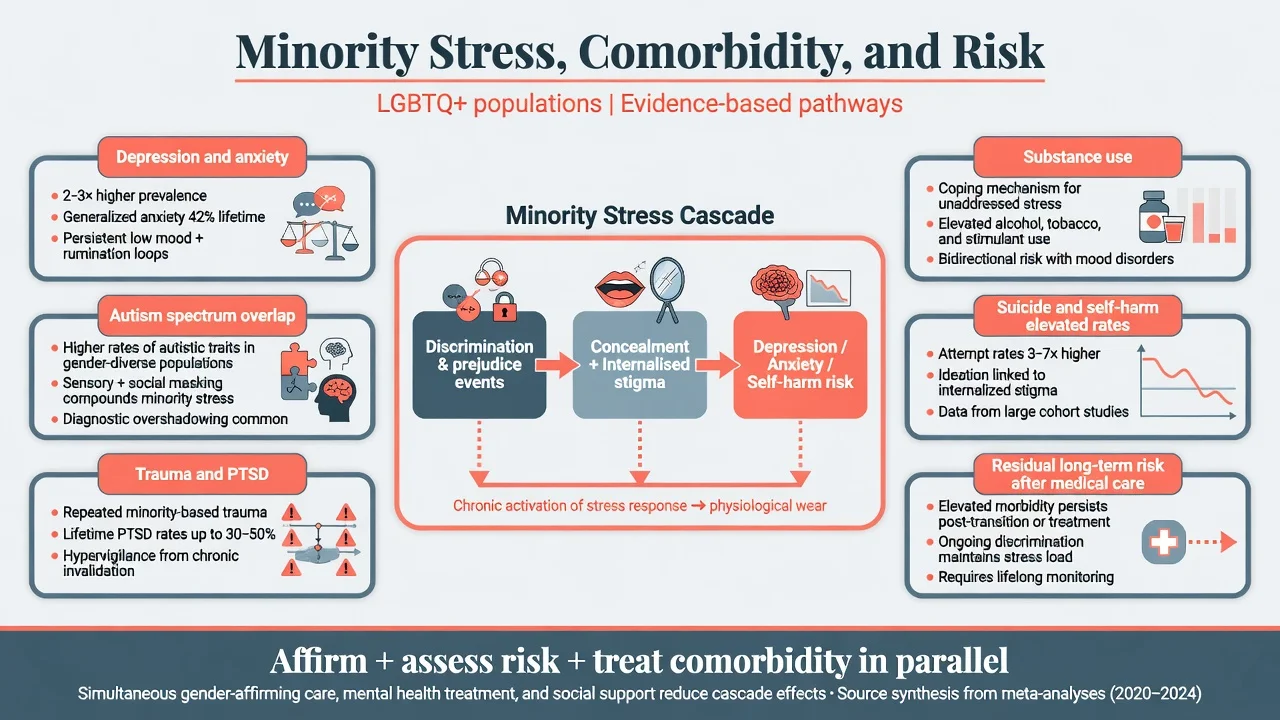
Mental health burden. Reviews consistently find elevated depression, anxiety, self-harm, and suicidality among transgender and gender-diverse people relative to general population comparisons, especially in youth samples. Mechanisms include minority stress, discrimination, family rejection, and barriers to care — not a claim that gender diversity is inherently a mental illness.[4][5][6][7]
Autism spectrum. Systematic reviews and clinic studies report higher rates of autistic traits/ASD diagnoses among gender-dysphoric populations than base rates — requiring adapted communication and extended assessment, not automatic dismissal of gender experience.[8][9]
Long-term mortality/suicide. Swedish long-term cohort data after surgical transition showed elevated overall mortality and suicide versus population controls, indicating residual vulnerability and need for ongoing mental health care. Amsterdam Cohort analyses of suicide death risk similarly support continued vigilance after gender-affirming medical care rather than assuming risk is abolished by transition alone.[19][20]
Exam anchors (order-of-magnitude teaching)
Mechanisms and formulation
Use a biopsychosocial formulation. Gender identity development is multifactorial; no laboratory test diagnoses gender dysphoria. Sex characteristics can be a focus of profound dysphoria and a target of medical interventions. Concurrent psychiatric disorders can amplify distress without "explaining away" authentic incongruence.[1][4]
Minority stress links distal stressors (discrimination, violence, structural exclusion) and proximal stressors (concealment, expectation of rejection, internalised stigma) to depression, anxiety, and self-harm risk. Affirmative environments and social support are clinical interventions, not optional niceties.[6][7]
Developmental pathways. Early-onset childhood gender dysphoria may desist or persist; adolescent-onset presentations have increased in many services and require careful, non-ideological assessment of comorbidity, social context, and persistence. Steensma-order qualitative/quantitative work remains the classic citation for childhood course nuance.[10][11][1]
Clinical presentation
Adults and adolescents may describe longstanding or more recent incongruence; chest, genital, voice, hair, or menstrual distress; desire for social and/or medical transition; and variable binary or non-binary goals. Children show intense cross-gender preferences and identity statements with functional impact at home and school.[1][6]
MSE language (fellowship). Respectful use of affirmed name/pronouns; coherent identity narrative over time; mood and anxiety; psychotic symptoms; cognitive rigidity/ASD traits; trauma markers; substance use; insight into medical risks/benefits; suicide and self-harm risk with means and intent. Document function (school, work, relationships) and family response.[4][5]
Differential diagnosis
Body dysmorphic disorder
- Perceived defect focus
- Checking/camouflage rituals
- Not primary gender identity incongruence
- Can co-occur — formulate both
Psychosis
- Delusional gender change as one of many delusions
- Thought disorder/hallucinations
- Stabilise psychosis first
- Do not permanently invalidate all gender experience
Transvestic disorder
- Cross-dressing for sexual arousal primary
- Not equivalent to gender dysphoria
- History clarifies motivation
- Avoid moralising language
Trauma / ASD / identity exploration
- Trauma can disrupt self-concept
- ASD: rigid categories, sensory body issues
- Extended assessment helps
- Not automatic exclusion criteria
Also distinguish questions of sexual orientation from gender identity, and consider DSD/intersex conditions when history or examination suggests them.[1][22]
Assessment
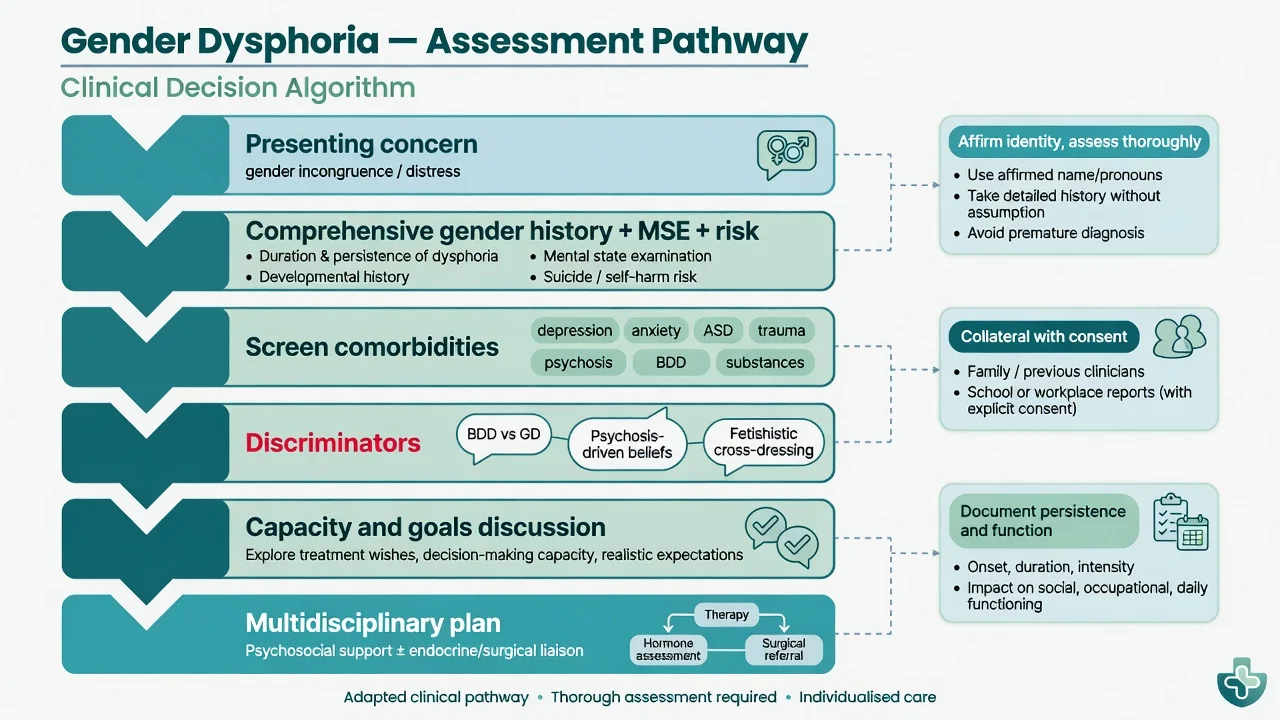
Structure. Gender developmental history (onset, persistence, insistence, consistency); social transition steps; prior treatments; body goals; fertility and sexual function goals; full psychiatric history; medical history (thrombosis, smoking, migraine with aura, polycythaemia risk factors); family/school context; cultural factors.[1][17][18]
Risk assessment is mandatory: ideation, intent, plan, means, prior attempts, NSSI, protective factors, housing, rejection, bullying. Safety planning is concurrent with gender care, not postponed until after transition.[5][6]
Collateral with consent improves accuracy in youth and complex adult presentations. Structured scales may assist communication but do not replace clinical diagnosis.[1][17]
Investigations
There is no diagnostic biomarker for gender dysphoria. Investigations support safe medical care and exclusion of organic differentials when indicated.[16][18]
Before gender-affirming hormones (specialist pathway). Baseline assessment typically includes cardiovascular risk factors, smoking status, FBC (especially if testosterone planned), lipids, LFTs, glucose/HbA1c as indicated, sex steroid levels as relevant to the regimen, pregnancy test when applicable, and VTE risk discussion. Bone density is considered in selected patients (e.g. prolonged hypogonadism risk). Psychotropics require their own baseline ECG/metabolic monitoring when used.[16][18]
Acute and emergency management
Stabilise mania/psychosis before irreversible decisions. Safeguard against conversion pressure and violence. Hormone complications (VTE, severe erythrocytosis) need medical admission pathways with endocrine input.[16][18]
Definitive management — affirmative care
Principles
- Respect identity, name, and pronouns; reduce stigma in the clinical encounter.[7][17]
- Assess thoroughly — affirmative care is not the absence of differential diagnosis.[1][22]
- Treat comorbidity in parallel (depression, anxiety, PTSD, ASD supports, SUD).[4][6]
- Shared decision-making with realistic expectations about what medical transition can and cannot do for mental health.[17][18]
- Oppose conversion efforts aimed at changing gender identity; recalled exposure is associated with psychological distress and suicide attempts in adult survey data.[15]
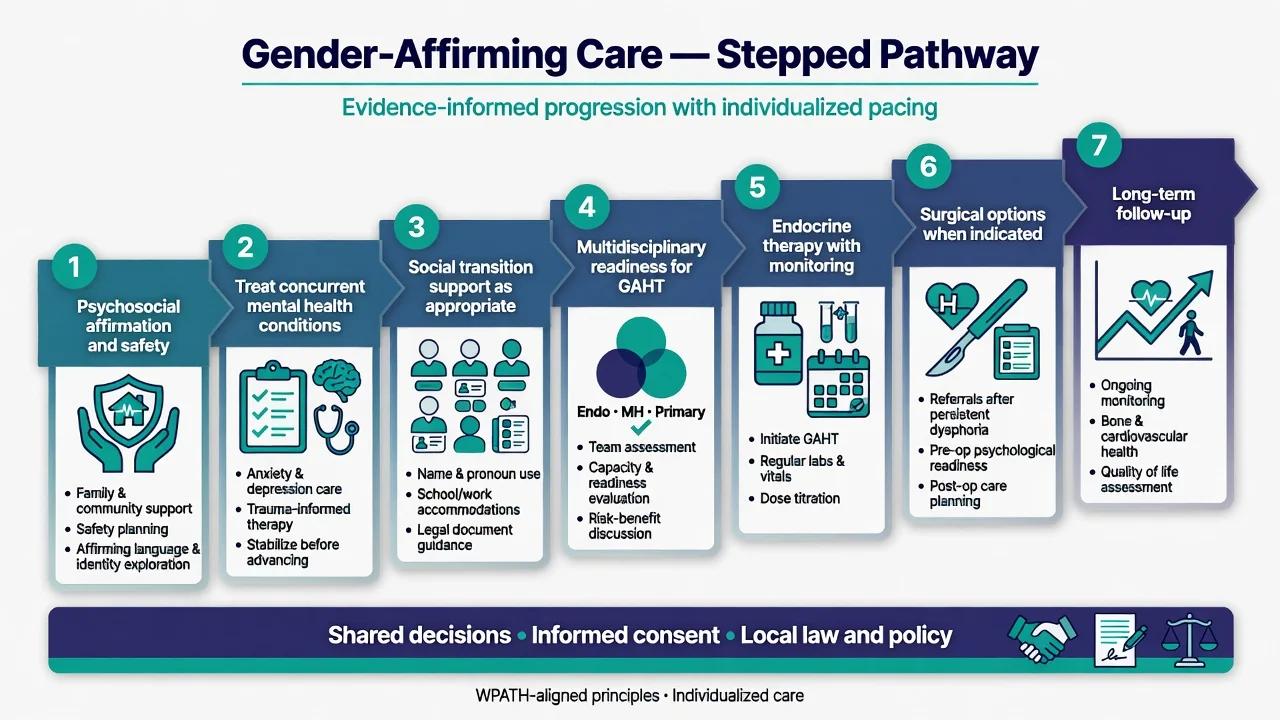
Psychosocial care
Supportive psychotherapy, family work, school advocacy, peer support, and trauma-informed care. Evidence-based treatments for depression/anxiety/PTSD apply as in other populations. Social transition (name, pronouns, clothing, documents) is a psychosocial intervention with benefits and social risks that should be discussed, especially for minors.[6][17][22]
Gender-affirming hormone therapy (GAHT)
Psychiatrists typically assess, formulate, treat comorbidity, and liaison — initiation and titration are specialist endocrine/gender-service roles under guidelines. Endocrine Society guidance and WPATH SOC8 outline eligibility frameworks, monitoring, and informed consent including fertility counselling.[16][17][18]
Teaching overview (not a prescribing recipe for unsupervised start). Feminising pathways commonly involve oestradiol with or without anti-androgen strategies; masculinising pathways use testosterone preparations. Monitoring addresses haematocrit (testosterone), thromboembolism risk (oestrogen), blood pressure, lipids, and clinical response. Exact agents, doses, and targets are protocol- and jurisdiction-specific — state that in viva and cite guideline frameworks rather than inventing a fixed dose table from memory.[16][18]
Puberty suppression
GnRH analogues may be considered in carefully selected adolescents after multidisciplinary assessment to pause puberty while gender identity and mental health are clarified — evidence quality is limited and policy is evolving regionally. Fertility implications, bone health, and capacity require explicit counselling. Follow local law, institutional criteria, and specialist pathways.[12][16][17]
Surgery
Chest, genital, and facial surgeries may be appropriate after readiness assessment for adults (and, where lawful, selected older adolescents). Systematic reviews of psychosocial outcomes after hormonal/surgical treatment report improvements for many people, with important methodological limits. Regret is uncommon but not zero; residual psychiatric morbidity can persist — ongoing MH follow-up is part of good care.[21][19][17]
Selected outcome signals (evidence-aware)
- Dutch clinic young-adult outcomes after puberty suppression and gender reassignment reported psychological improvement in a carefully selected historical cohort.[12]
- Observational youth cohorts (e.g. Tordoff) report associations between gender-affirming medical care and lower odds of depression/suicidality over short follow-up — confounded designs warrant cautious interpretation.[14]
- Chen et al. (NEJM) reported two-year psychosocial functioning trajectories among transgender youth on hormones — cite as contemporary outcome data with residual questions about durability and selection.[13]
- Population and cohort studies (Dhejne; Wiepjes) remind examiners that long-term suicide risk and mortality can remain elevated relative to general population, supporting continuous mental health care.[19][20]
Comorbidity, minority stress, and risk framing
Screen and treat: major depression, anxiety disorders, PTSD, substance use, eating disorders, OCD/BDD, ADHD/ASD, personality vulnerability, and psychosis when present. Self-harm and suicide risk assessment is longitudinal, not a single checkbox.[4][5][8]
Capacity, consent, and developmental nuance
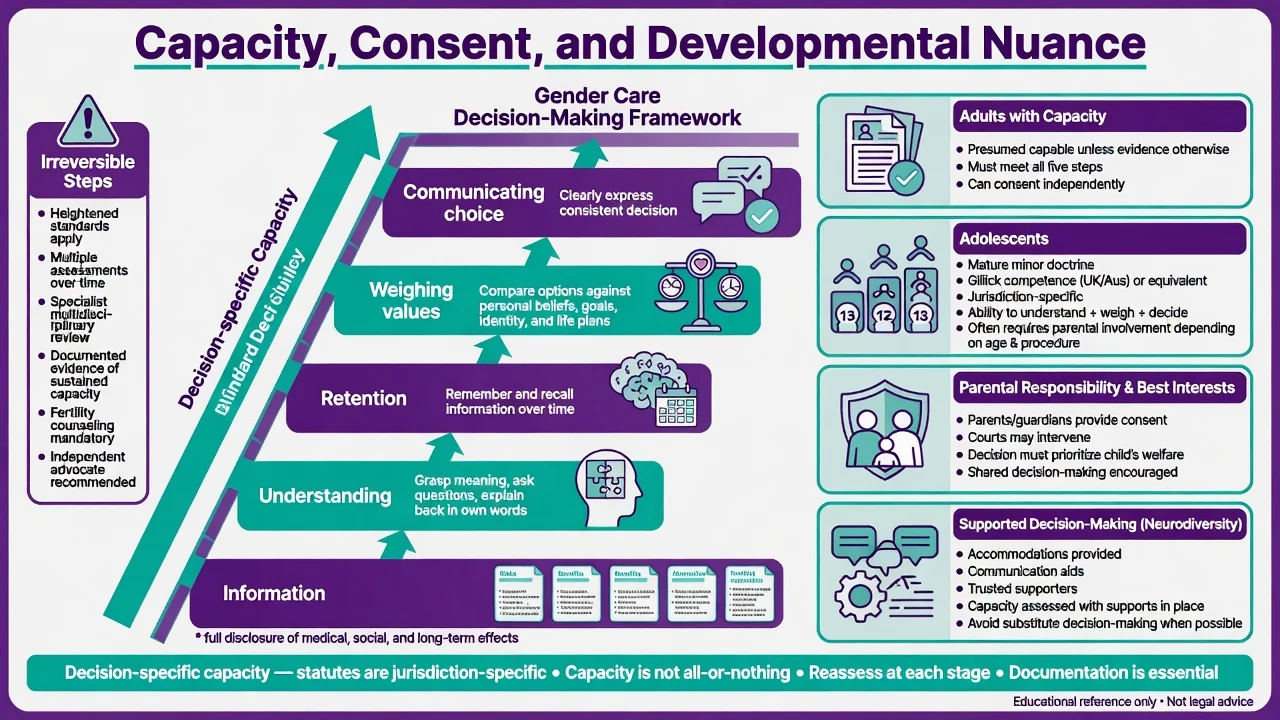
Capacity is decision-specific: understand information (including fertility, sexual function, medical risks, unknowns), retain, weigh in light of values, and communicate a choice. Adults are presumed capable unless evidence shows otherwise. Adolescents may meet mature-minor/Gillick-type thresholds in some jurisdictions; parental responsibility and best-interests frameworks apply differently by statute — name that laws are local and do not invent section numbers for another country.[17][18]
For irreversible steps, document sustained congruence, realistic expectations, comorbidity management, and multidisciplinary agreement. Neurodivergent patients may need supported decision-making and longer assessment windows without default denial of care.[8][17]
Special populations and regional practice
Children and adolescents. Extended assessment; family work; school safety; cautious approach to irreversible interventions; evolving service criteria. Historical childhood follow-up informs humility about prediction.[10][11][6]
Autistic gender-diverse people. Higher co-occurrence; use concrete communication, sensory accommodations, and avoid diagnostic overshadowing in either direction.[8][9]
Cultural and Indigenous contexts. Culturally safe practice; recognise diverse gender systems; address racism and minority stress intersectionally.[7]
ANZ. Care is shaped by RANZCP-aligned professional positions, public gender services with multidisciplinary models, and jurisdiction-specific consent/capacity and youth service rules that have been under active policy review. State principles of affirmative assessment, anti-conversion stance, and lawful consent rather than memorising another country's statutes.[17]
UK/Europe. Specialist gender services and evolving youth pathway guidance (including major service reviews in some systems) — cite local operational criteria in clinical practice.[17][16]
US. Endocrine Society and WPATH SOC8 heavily influence practice; state law variation is extreme — always check local legality for adolescent medical care.[16][17][18]
Prognosis and disposition
Childhood course is heterogeneous. Many adults report improved quality of life and reduced dysphoria with affirmative psychosocial and medical care, while some have complicated courses with ongoing psychiatric need. Disposition spans community mental health, specialist gender clinics, endocrine and surgical tertiary services, and crisis pathways. Long-term follow-up includes mental health, hormone safety, and anatomy-based preventive care.[1][12][19][21]
Exam pearls
AFFIRM framework (clinical checklist)
Pitfalls
Pitfalls include pathologising identity or rubber-stamping irreversible care without assessment; missing BDD, psychosis, trauma, or ASD; assuming medical transition abolishes all suicide risk; conversion practices or forced outing; ignoring fertility, VTE, smoking, and long-term monitoring; and replacing evidence literacy with politicised certainty.[1][15][19]
Good fellowship practice is affirmative, thorough, collaborative, and humble about evidence limits.[1][15][17][19]
References
- [1]Zucker KJ, Lawrence AA, Kreukels BP Gender Dysphoria in Adults Annu Rev Clin Psychol, 2016.PMID 26788901
- [2]Drescher J, Cohen-Kettenis PT, Reed GM Gender incongruence of childhood in the ICD-11: controversies, proposal, and rationale Lancet Psychiatry, 2016.PMID 26946394
- [3]Arcelus J, Bouman WP, Van Den Noortgate W, et al. Systematic review and meta-analysis of prevalence studies in transsexualism Eur Psychiatry, 2015.PMID 26021270
- [4]Dhejne C, Van Vlerken R, Heylens G, Arcelus J Mental health and gender dysphoria: A review of the literature Int Rev Psychiatry, 2016.PMID 26835611
- [5]Marshall E, Claes L, Bouman WP, et al. Non-suicidal self-injury and suicidality in trans people: A systematic review of the literature Int Rev Psychiatry, 2016.PMID 26329283
- [6]Connolly MD, Zervos MJ, Barone CJ 2nd, et al. The Mental Health of Transgender Youth: Advances in Understanding J Adolesc Health, 2016.PMID 27544457
- [7]Winter S, Diamond M, Green J, et al. Transgender people: health at the margins of society Lancet, 2016.PMID 27323925
- [8]Glidden D, Bouman WP, Jones BA, Arcelus J Gender Dysphoria and Autism Spectrum Disorder: A Systematic Review of the Literature Sex Med Rev, 2016.PMID 27872002
- [9]van der Miesen AIR, de Vries ALC, Steensma TD, Hartman CA Autistic Symptoms in Children and Adolescents with Gender Dysphoria J Autism Dev Disord, 2018.PMID 29189919
- [10]Steensma TD, McGuire JK, Kreukels BP, et al. Factors associated with desistence and persistence of childhood gender dysphoria: a quantitative follow-up study J Am Acad Child Adolesc Psychiatry, 2013.PMID 23702447
- [11]Steensma TD, Biemond R, de Boer F, Cohen-Kettenis PT Desisting and persisting gender dysphoria after childhood: a qualitative follow-up study Clin Child Psychol Psychiatry, 2011.PMID 21216800
- [12]de Vries AL, McGuire JK, Steensma TD, et al. Young adult psychological outcome after puberty suppression and gender reassignment Pediatrics, 2014.PMID 25201798
- [13]Chen D, Berona J, Chan YM, et al. Psychosocial Functioning in Transgender Youth after 2 Years of Hormones N Engl J Med, 2023.PMID 36652355
- [14]Tordoff DM, Wanta JW, Collin A, et al. Mental Health Outcomes in Transgender and Nonbinary Youths Receiving Gender-Affirming Care JAMA Netw Open, 2022.PMID 35212746
- [15]Turban JL, Beckwith N, Reisner SL, Keuroghlian AS Association Between Recalled Exposure to Gender Identity Conversion Efforts and Psychological Distress and Suicide Attempts Among Transgender Adults JAMA Psychiatry, 2020.PMID 31509158
- [16]Hembree WC, Cohen-Kettenis PT, Gooren L, et al. Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Society Clinical Practice Guideline Endocr Pract, 2017.PMID 29320642
- [17]Coleman E, Radix AE, Bouman WP, et al. Standards of Care for the Health of Transgender and Gender Diverse People, Version 8 Int J Transgend Health, 2022.PMID 36238954
- [18]Safer JD, Tangpricha V Care of Transgender Persons N Engl J Med, 2019.PMID 31851801
- [19]Dhejne C, Lichtenstein P, Boman M, et al. Long-term follow-up of transsexual persons undergoing sex reassignment surgery: cohort study in Sweden PLoS One, 2011.PMID 21364939
- [20]Wiepjes CM, den Heijer M, Bremmer MA, et al. Trends in suicide death risk in transgender people: results from the Amsterdam Cohort of Gender Dysphoria study (1972-2017) Acta Psychiatr Scand, 2020.PMID 32072611
- [21]Murad MH, Elamin MB, Garcia MZ, et al. Hormonal therapy and sex reassignment: a systematic review and meta-analysis of quality of life and psychosocial outcomes Clin Endocrinol (Oxf), 2010.PMID 19473181
- [22]Byne W, Bradley SJ, Coleman E, et al. Report of the American Psychiatric Association Task Force on Treatment of Gender Identity Disorder Arch Sex Behav, 2012.PMID 22736225