Psych · Specialty psychiatry — sleep medicine interface
Insomnia disorder
Also known as Chronic insomnia · Primary insomnia · Psychophysiological insomnia · CBT-I · Cognitive behavioural therapy for insomnia · Sleep-onset insomnia · Sleep-maintenance insomnia · Hypnotics · Z-drugs
Exam-exhaustive fellowship atlas on insomnia disorder — DSM-5-TR/ICSD-3 nosology, Spielman 3P and hyperarousal models, epidemiology and depression/suicide bidirectionality, differential from OSA/DSPD/mania, assessment and ISI/diary, CBT-I first-line with digital options, short-term hypnotics and deprescribing, elderly harm, and ACP/AASM/ESRS/BAP guideline deltas. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Insomnia is not optional comfort care. FRANZCP MEQs test CBT-I components, hypnotic deprescribing, and the insomnia–depression–suicide link. MRCPsych CASCs test plain-language CBT-I explanation and collaborative taper. ABPN items test DSM/ICSD thresholds, phenotype language, and psychotropic sleep effects. A candidate who reads only this leaf should defend assessment, organic exclusion, and stepped care at consultant depth without relying on the broader sleep hub page alone.[6][12][19]
Overview and definition
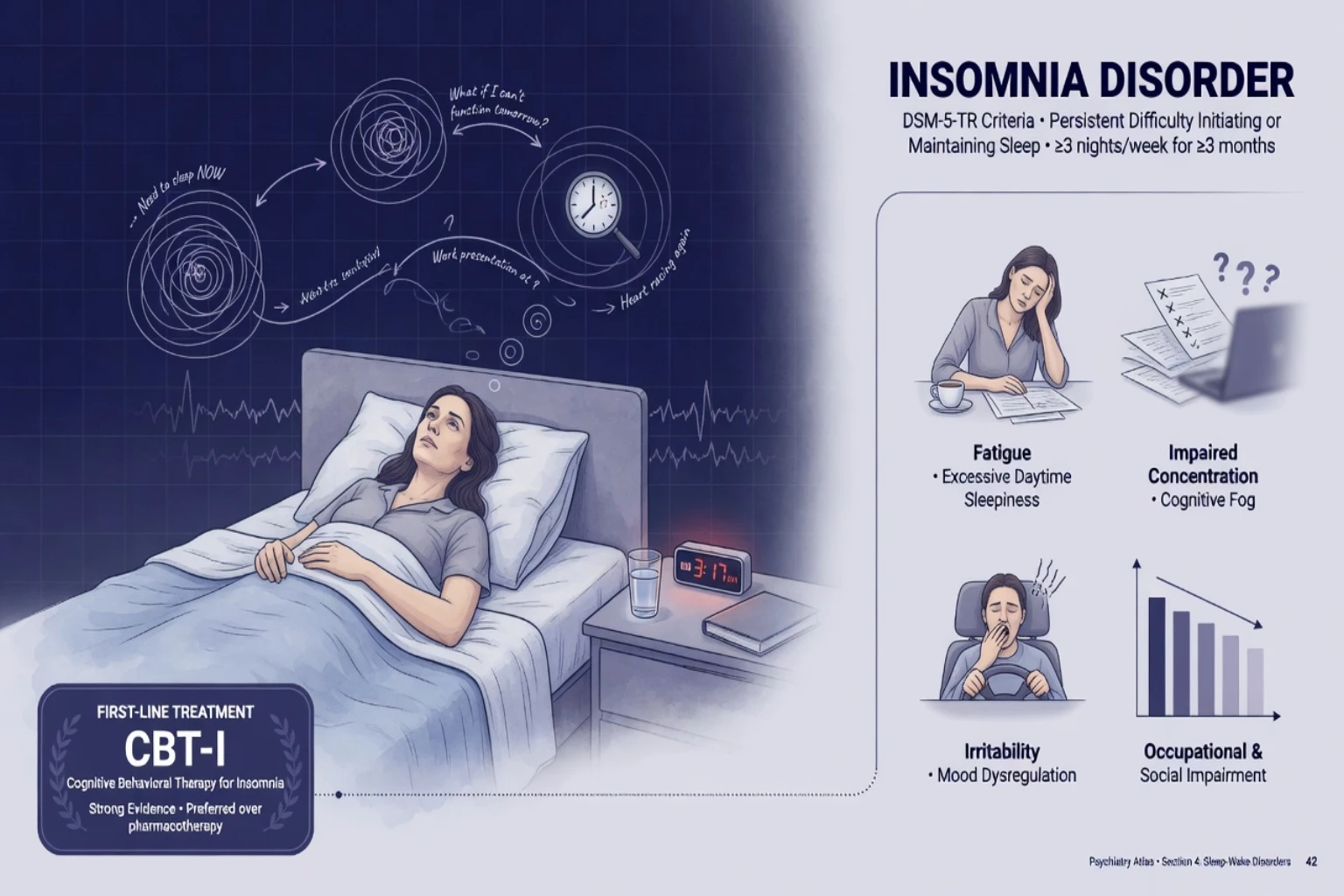
Insomnia disorder (DSM-5-TR) is a predominant complaint of dissatisfaction with sleep quantity or quality associated with difficulty initiating sleep, difficulty maintaining sleep, or early-morning awakening with inability to return to sleep. Daytime distress or impairment is required; opportunity for sleep must be adequate; and another sleep–wake, mental, medical, or substance disorder must not fully explain the presentation when those conditions alone account for the sleep complaint. Chronicity for exam framing is typically at least 3 nights per week for at least 3 months (chronic insomnia disorder in ICSD-3 terms), with short-term/episodic presentations lasting less than 3 months still clinically important.[12][13]
Clinical essence. Insomnia is both a symptom across mood, anxiety, trauma, psychosis, and substance disorders and an independent disorder that maintains residual symptoms, predicts incident depression, and amplifies suicide risk. Waiting for the parent diagnosis to remiss fully before treating sleep is outdated exam-fail care. Nightly open-ended hypnotics without behavioural change are likewise outdated.[8][9][2]
ICSD-3 context. The International Classification of Sleep Disorders, third edition places insomnia disorders among major sleep pathology groups (alongside breathing, hypersomnolence, circadian, parasomnia, and movement disorders). Psychiatrists must navigate this map even when coding DSM-5-TR insomnia disorder in the mental health record.[13]
Classification and nosology
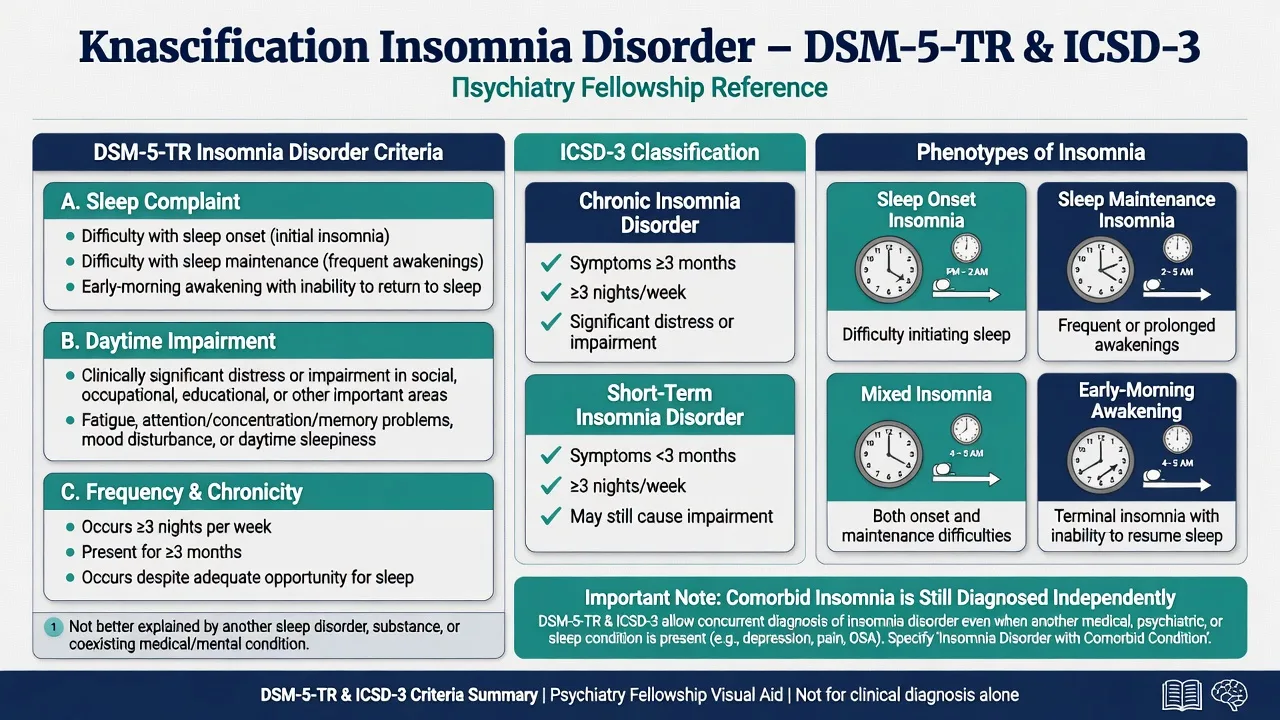
Sleep-onset type
- Long sleep latency
- Rumination and sleep effort common
- Anxiety/OCD interface frequent
- Stimulus control high yield
Sleep-maintenance type
- WASO high; fragmented sleep
- Pain, OSA, alcohol, nocturia clues
- Middle insomnia classic in MDD
- Review apnoeas and substances
Early-morning type
- Terminal awakening
- Mood disorder interface
- Circadian advance in older adults
- Distinguish from planned early rise
Comorbid framing
- Diagnose insomnia even with MDD/GAD/PTSD
- Primary vs secondary dichotomy retired
- Treat sleep and parent illness together
- Residual insomnia predicts relapse
Exam pearl on comorbidity. Modern nosology allows insomnia disorder when criteria are met even with co-occurring depression or anxiety. The old primary versus secondary dichotomy is largely retired — treat both processes rather than waiting for mood remittance alone.[12][5]
Epidemiology and risk
Headline epidemiology (exam anchors)
Community data place insomnia disorder at roughly one in ten adults, with intermittent symptoms far more common; women and older adults are disproportionately affected, and multi-year chronicity is substantial without effective behavioural treatment.[16]
Longitudinal meta-analytic evidence shows insomnia predicts incident depression (order of approximately doubled risk in Baglioni-type analyses) and broader mental disorders in Hertenstein-type syntheses — examiners use this to reject the idea that insomnia is only secondary noise.[8][9]
Sleep disturbance associates with suicidal ideation, attempt, and death across meta-analytic and systematic reviews; severe insomnia and nightmares deserve explicit risk documentation on every assessment that includes sleepless nights.[10][11]
Pathophysiology and mechanisms
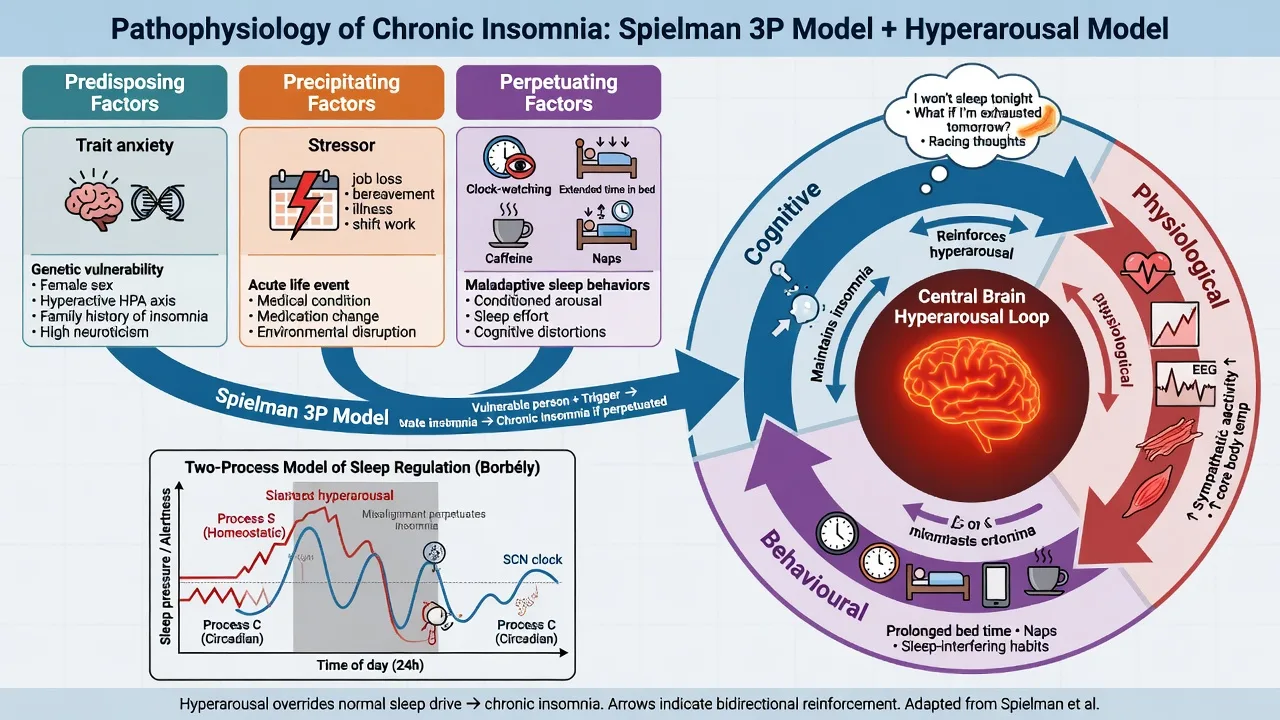
Spielman 3P model (viva gold).
- Predisposing: trait anxiety, family history of poor sleep, high arousal set-point, female sex, older age.
- Precipitating: acute stressor, illness, loss, hospitalisation, psychiatric episode, schedule change.
- Perpetuating: extended time in bed, irregular schedule, daytime naps, clock-watching, caffeine/alcohol as self-treatment, catastrophic sleep beliefs, conditioned arousal to the bedroom. CBT-I works primarily on perpetuating factors after the original stressor has often resolved.[12][5]
Hyperarousal. Cognitive (rumination, threat monitoring of sleep), physiological (HPA tone, high-frequency EEG signatures in research settings), and behavioural loops maintain chronic insomnia independent of the original trigger.[12]
Two-process model interface. Homeostatic sleep pressure (Process S) builds with wakefulness; circadian alerting (Process C) is SCN-driven. Extending time in bed dilutes sleep efficiency and weakens the bed–sleep association. Sleep restriction temporarily matches time in bed to average total sleep time to rebuild Process S — which is why it works and why it must be planned carefully in bipolar, seizure, and safety-critical occupations.[4][19]
Clinical presentation
History language examiners want. Sleep onset latency (SOL), wake after sleep onset (WASO), early terminal awakening, total sleep time (TST), time in bed (TIB), sleep efficiency (TST/TIB), naps, weekday–weekend discrepancy, sleep effort, and catastrophic beliefs (“if I do not sleep 8 hours I will crack tomorrow”).[12]
Daytime phenotype. Fatigue is not the same as sleepiness. Classic insomnia often shows fatigue, irritability, and cognitive fog with relatively preserved ability to stay awake; marked sleepiness raises OSA, circadian misalignment, or sedating drug effects.[12][19]
Psychiatric pattern language.
- MDD: middle and late insomnia classic; hypersomnia in atypical features.
- Bipolar: reduced need for sleep without fatigue is a mania/hypomania clue — distinct from inability to sleep.
- PTSD: nightmares, hyperarousal, avoidance of bed.
- Anxiety/OCD: sleep-onset rumination and checking rituals.
- Psychosis: reversed sleep phase, environmental threat, medication sedation. These patterns are discriminators, not pathognomonic rules — integrate full MSE and collateral.[12][19]
Differential diagnosis
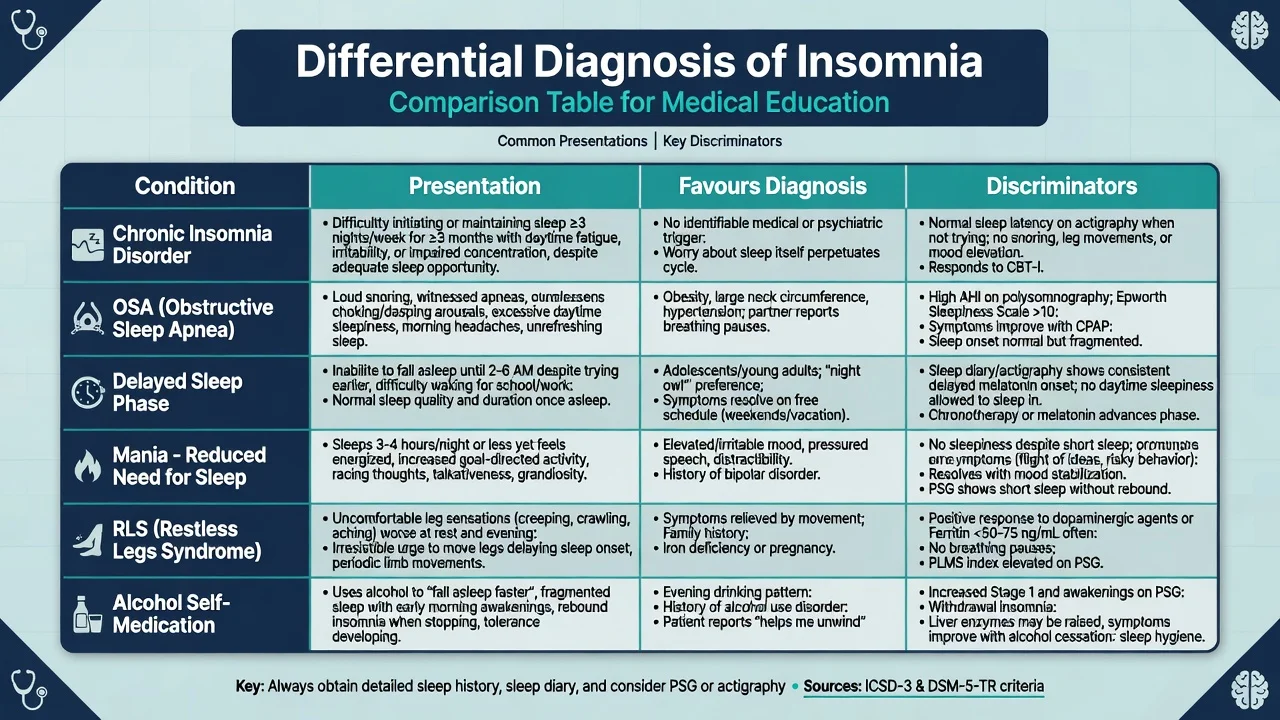
| Presentation | Favours | Against pure insomnia alone |
|---|---|---|
| Loud snoring + witnessed apnoea + high BMI | OSA | Partner denial does not fully exclude |
| Delayed sleep, can sleep long if free schedule | DSPD | Fixed early wake with long latency only |
| Reduced need for sleep + elevated mood/energy | Mania/hypomania | Classic insomnia with dysphoria and tiredness |
| Urge to move legs evening, relief with movement | RLS | Whole-body restlessness on antipsychotics (akathisia) |
| Nightcap alcohol “helps me drop off” | Substance-maintained fragmenting | True restorative sleep architecture |
| Starts after activating antidepressant | Medication-induced component | Pre-existing chronic pattern unchanged |
Always include substances (alcohol shortens latency but fragments architecture and worsens OSA; caffeine/stimulants; cannabis withdrawal), medical pain, nocturia, heart failure, thyroid disease, and medication timing.[12][20][19]
Assessment
Core structure. Chronotype, work pattern, substances, bed partner report, mood/anxiety/trauma/psychosis screen, suicide risk, driving/occupational risk, medication list including OTC antihistamines and alcohol “nightcaps.” A complete sleep history is standard psychiatric assessment, not an optional add-on.[12][19]
Tools.
- Sleep diary for 1–2 weeks is high-yield for SOL, WASO, TST, TIB, and naps.
- Actigraphy when schedules are chaotic or report reliability is low.
- Insomnia Severity Index (ISI) for severity and treatment response tracking.
- Epworth Sleepiness Scale (ESS) when sleepiness or driving risk is the question — ESS is not an insomnia severity scale.[12][5]
OSA screen. STOP-BANG / Berlin-type concepts (snoring, tiredness, observed apnoea, hypertension, BMI, age, neck, gender) triage who needs sleep study referral while CBT-I can still start for clear insomnia features.[19]
Risk domains. Document SI/NSSI linked to sleepless nights; fitness to drive with sleepiness; fall risk if prescribing sedatives to older adults.[10][14]
Investigations
- Not everyone needs PSG. Typical chronic insomnia without atypical features is a clinical diagnosis; start CBT-I without waiting for a sleep laboratory appointment.[2][4]
- Refer for sleep study when moderate–high OSA probability, unexplained hypersomnia, treatment-resistant insomnia with red flags, suspected parasomnia/RBD with injury risk, or preoperative risk.
- Labs as indicated: TFT, FBC, glucose/HbA1c, ferritin if RLS clues, toxicology when substance contribution is plausible.
- Baseline before sedating drugs: ECG/QTc when using antipsychotics or TCAs for sleep; falls and cognitive baseline in older adults.[14][3]
Acute and emergency management
- Acute mania: prioritise mood stabilisation and sleep protection; do not default to outpatient hypnotic-only care.
- Hypnotic overdose / delirium / falls: ABC, stop agent, medical liaison; plan deprescribing after stabilisation.
- Occupational near-miss: temporary work safety planning and fitness-to-drive principles by jurisdiction.
- Alcohol withdrawal insomnia: treat withdrawal properly; do not mislabel as primary chronic insomnia during detox.[19]
Definitive management — CBT-I first
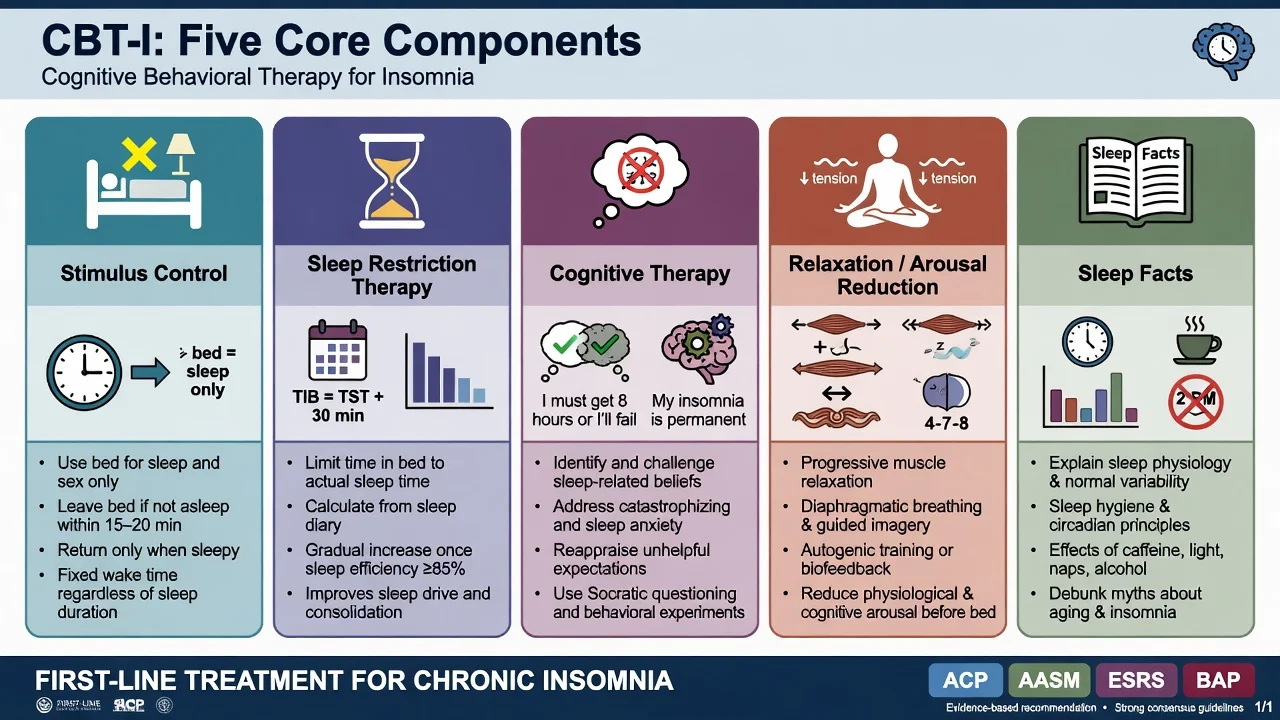
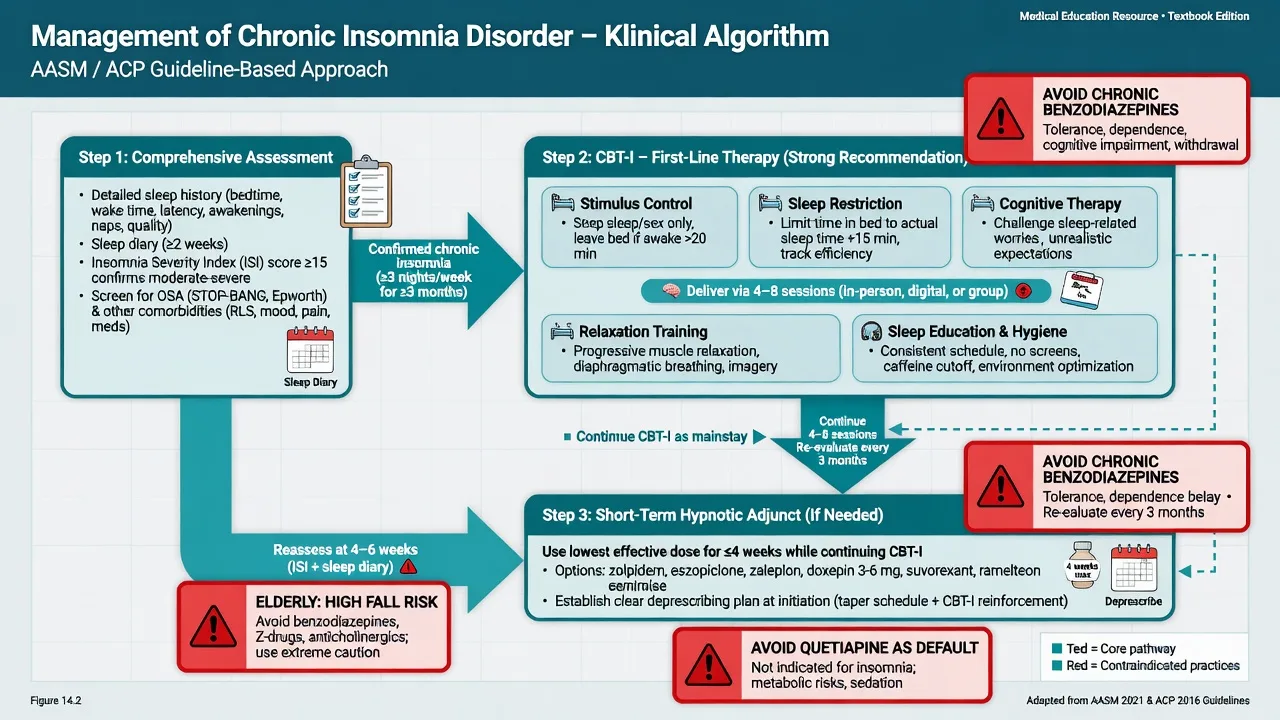
Multicomponent cognitive behavioural therapy for insomnia (CBT-I) is first-line for chronic insomnia in adults across ACP, AASM behavioural, and European guidelines, reaffirmed in the 2023 European update.[2][4][5][6]
Core components (must list in viva):
- Stimulus control — bed for sleep/sex only; leave bed if unable to sleep after a short period of wakefulness; fixed wake time; no clock-watching.
- Sleep restriction therapy — match time in bed to average total sleep time; expand when efficiency improves (plan carefully if bipolar, seizure disorder, or safety-critical work).
- Cognitive therapy — challenge unhelpful sleep beliefs and safety behaviours.
- Relaxation / arousal reduction.
- Sleep education (hygiene is necessary but not sufficient alone as therapy).[4][1]
Meta-analysis shows CBT-I produces clinically meaningful improvements in sleep outcomes for chronic insomnia.[1] Digital CBT-I improves functional health and psychological well-being at scale (Espie-order RCT).[15] Improving sleep can mediate reductions in paranoia and hallucinations in student samples (Freeman OASIS), supporting sleep as a modifiable mental health target, not a cosmetic outcome.[17]
Morin’s combination trial logic remains an exam pearl: medication may help short-term, but CBT-I drives more durable gains for long-term planning.[7]
Pharmacotherapy (second-line / adjunct)
Guidelines do not support open-ended nightly benzodiazepines as standard care. AASM pharmacologic guidance offers mostly weak recommendations for specific agents over no treatment for short-term use; long-term hypnotic monotherapy is discouraged relative to CBT-I.[3][2]
Practical fellowship framing (local product information and formulary govern exact licensed doses):
- Prefer shortest effective duration (often days to a few weeks) with a written taper plan from day one.
- Classes with guideline discussion: non-benzodiazepine receptor agonists (Z-drugs such as zolpidem, zopiclone/eszopiclone, zaleplon where available), short/intermediate benzodiazepines (e.g. temazepam), low-dose doxepin for sleep-maintenance phenotypes, melatonin receptor agonists, and dual orexin receptor antagonists where marketed.
- Illustrative adult short-term examples (always check current product info, age, hepatic impairment, and interactions): zolpidem often 5–10 mg oral at bedtime (use 5 mg in older adults where licensed); zopiclone often 3.75–7.5 mg oral at bedtime; low-dose doxepin for insomnia typically in the 3–6 mg oral range where the low-dose product is available; avoid dose stacking with alcohol.[3][18][19]
- Sedating antidepressants (trazodone, mirtazapine, low-dose doxepin/amitriptyline) are widely used when depression/anxiety coexists — understand receptor effects, hangover, weight gain, and OSA risk; they are not automatic CBT-I substitutes.[20][19]
- Avoid defaulting to quetiapine for primary insomnia without psychotic/mood indication — metabolic and QTc costs are disproportionate for a sleep complaint alone.[20]
- Older adults: meta-analytic risk–benefit of sedative-hypnotics is unfavourable (cognitive events, falls) — non-drug first, lowest dose, shortest time if any drug is used.[14]
ACP (US): CBT-I first for all adults with chronic insomnia; discuss medication only after or with CBT-I when needed.[2] AASM: strong support for multicomponent CBT-I; pharmacologic options weak and agent-specific for short-term use.[3][4] ESRS Europe: CBT-I first-line; 2023 update reaffirms behavioural priority and modern diagnostic framing.[5][6] BAP (UK): consensus on insomnia, parasomnias, and circadian disorders — behavioural first, rational short-term drugs, specialist pathways.[18][19] ANZ practice: align with CBT-I first, sleep physician referral for OSA red flags, and local PBS/formulary constraints on hypnotics; rural access delays should not block behavioural care start.
Special populations and scenarios
- Older adults: falls, delirium, cognitive blunting with BZD/Z-drugs — prefer CBT-I/adapted behavioural care; review polypharmacy; avoid automatic dose escalation.[14]
- Pregnancy/lactation: prioritise non-drug; individualise any medication with obstetric liaison (agent-specific data; avoid fabricating absolute safety claims).
- Youth: DSPD and insomnia common; family-supported behavioural schedules first; do not force early lights-out without phase work when delay is the driver.[19]
- MDD comorbidity: treat residual insomnia actively; it predicts poorer course and is not automatically fixed by SSRI alone.[8][20]
- Bipolar: protect sleep continuity; caution with sleep restriction; avoid antidepressant activation that fragments nights.
- Psychosis inpatient: environmental control, schedule regularity, and adapted CBT-I principles support recovery; sedating antipsychotics treat psychosis — they are not a licence for chronic primary-insomnia quetiapine culture.
- ANZ contexts: FIFO/shift work and rural sleep-lab delays — start behavioural care while awaiting PSG when OSA probability is moderate.
Complications and pitfalls
- Long-term benzodiazepine/Z-drug dependence, tolerance, rebound insomnia, falls, and cognitive fog — especially in older adults.[14]
- Missing OSA and labelling only “treatment-resistant depression.”
- Quetiapine as routine hypnotic in non-psychotic insomnia.
- Starting sleep restriction without bipolar, seizure, or occupational safety planning.
- Alcohol as self-medication — shortens latency, fragments architecture, worsens OSA.
- Calling “sleep hygiene leaflet” CBT-I.
Prognosis and disposition
Without CBT-I, insomnia often chronicles for years. With CBT-I, gains are more durable than medication alone; plan booster sessions and hypnotic deprescribing from the outset.[7][1] Safety-net for escalating SI, driving near-misses, falls, and witnessed apnoeas. Step up to sleep medicine, liaison medicine, or crisis services when red flags appear.
Exam pearls
INSOMNIA CARE (assessment and plan)
References
- [1]Trauer JM, Qian MY, Doyle JS, et al. Cognitive Behavioral Therapy for Chronic Insomnia: A Systematic Review and Meta-analysis Ann Intern Med, 2015.PMID 26054060
- [2]Qaseem A, Kansagara D, Forciea MA, et al. Management of Chronic Insomnia Disorder in Adults: A Clinical Practice Guideline From the American College of Physicians Ann Intern Med, 2016.PMID 27136449
- [3]Sateia MJ, Buysse DJ, Krystal AD, et al. Clinical Practice Guideline for the Pharmacologic Treatment of Chronic Insomnia in Adults: An American Academy of Sleep Medicine Clinical Practice Guideline J Clin Sleep Med, 2017.PMID 27998379
- [4]Edinger JD, Arnedt JT, Bertisch SM, et al. Behavioral and psychological treatments for chronic insomnia disorder in adults: an American Academy of Sleep Medicine clinical practice guideline J Clin Sleep Med, 2021.PMID 33164742
- [5]Riemann D, Baglioni C, Bassetti C, et al. European guideline for the diagnosis and treatment of insomnia J Sleep Res, 2017.PMID 28875581
- [6]Riemann D, Espie CA, Altena E, et al. The European Insomnia Guideline: An update on the diagnosis and treatment of insomnia 2023 J Sleep Res, 2023.PMID 38016484
- [7]Morin CM, Vallieres A, Guay B, et al. Cognitive behavioral therapy, singly and combined with medication, for persistent insomnia: a randomized controlled trial JAMA, 2009.PMID 19454639
- [8]Baglioni C, Battagliese G, Feige B, et al. Insomnia as a predictor of depression: a meta-analytic evaluation of longitudinal epidemiological studies J Affect Disord, 2011.PMID 21300408
- [9]Hertenstein E, Feige B, Gmeiner T, et al. Insomnia as a predictor of mental disorders: A systematic review and meta-analysis Sleep Med Rev, 2019.PMID 30537570
- [10]Pigeon WR, Pinquart M, Conner K Meta-analysis of sleep disturbance and suicidal thoughts and behaviors J Clin Psychiatry, 2012.PMID 23059158
- [11]Bernert RA, Kim JS, Iwata NG, et al. Sleep disturbances as an evidence-based suicide risk factor Curr Psychiatry Rep, 2015.PMID 25698339
- [12]Buysse DJ Insomnia JAMA, 2013.PMID 23423416
- [13]Sateia MJ International classification of sleep disorders-third edition: highlights and modifications Chest, 2014.PMID 25367475
- [14]Glass J, Lanctot KL, Herrmann N, et al. Sedative hypnotics in older people with insomnia: meta-analysis of risks and benefits BMJ, 2005.PMID 16284208
- [15]Espie CA, Emsley R, Kyle SD, et al. Effect of Digital Cognitive Behavioral Therapy for Insomnia on Health, Psychological Well-being, and Sleep-Related Quality of Life: A Randomized Clinical Trial JAMA Psychiatry, 2019.PMID 30264137
- [16]Morin CM, Jarrin DC Epidemiology of Insomnia: Prevalence, Course, Risk Factors, and Public Health Burden Sleep Med Clin, 2022.PMID 35659072
- [17]Freeman D, Sheaves B, Goodwin GM, et al. The effects of improving sleep on mental health (OASIS): a randomised controlled trial with mediation analysis Lancet Psychiatry, 2017.PMID 28888927
- [18]Wilson SJ, Nutt DJ, Alford C, et al. British Association for Psychopharmacology consensus statement on evidence-based treatment of insomnia, parasomnias and circadian rhythm disorders J Psychopharmacol, 2010.PMID 20813762
- [19]Wilson S, Anderson K, Baldwin D, et al. British Association for Psychopharmacology consensus statement on evidence-based treatment of insomnia, parasomnias and circadian rhythm disorders: An update J Psychopharmacol, 2019.PMID 31271339
- [20]Wichniak A, Wierzbicka A, Walecka M, et al. Effects of Antidepressants on Sleep Curr Psychiatry Rep, 2017.PMID 28791566