Psych · Specialty psychiatry — sleep medicine interface
Narcolepsy and hypersomnolence disorders
Also known as Narcolepsy type 1 · Narcolepsy type 2 · Cataplexy · Idiopathic hypersomnia · Hypocretin · Orexin · MSLT · Excessive daytime sleepiness · Central disorders of hypersomnolence · Sodium oxybate · Modafinil
Exam-exhaustive fellowship atlas on narcolepsy and central hypersomnolence — ICSD-3/DSM-5-TR nosology, orexin loss, tetrad presentation, MSLT and CSF hypocretin work-up, differentials (insufficient sleep, OSA, depression), AASM/European wake-promoter and anticataplexy pathways, driving risk, and psychiatry interface. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Psychiatrists meet hypersomnolence as “treatment-resistant depression,” ADHD-like inattention, conversion collapses, or “psychotic” dream-like experiences at sleep onset. FRANZCP MEQs test nosology, organic exclusion, and fitness to drive. MRCPsych CASCs test plain-language explanation of cataplexy and medication plans. ABPN items test MSLT criteria and orexin biology. This leaf must stand alone for central disorders of hypersomnolence without relying only on the broader sleep hub.[1][2][9]
Overview and definition
Central disorders of hypersomnolence (ICSD-3) include narcolepsy type 1 (NT1), narcolepsy type 2 (NT2), idiopathic hypersomnia (IH), and related entities such as Kleine–Levin syndrome. The shared clinical problem is pathological daytime sleepiness or long sleep need that is not explained solely by insufficient sleep opportunity or another primary sleep disruptor such as untreated OSA.[9][1]
Narcolepsy type 1 is defined by chronic excessive daytime sleepiness (EDS) with cataplexy and/or CSF hypocretin-1 (orexin-A) deficiency, supported by nocturnal PSG plus daytime MSLT findings. Narcolepsy type 2 shows EDS with MSLT criteria for narcolepsy without cataplexy and without documented low CSF hypocretin. Idiopathic hypersomnia features EDS with long sleep and/or short MSLT latencies without the SOREMP pattern that defines narcolepsy, often with severe sleep inertia.[1][2][9][16]
DSM-5-TR hypersomnolence disorder is a broader psychiatric coding frame; sleep physicians usually map the same patients onto ICSD-3 labels that drive MSLT interpretation and drug licences. Fellowship answers should move fluently between both languages.[9]
Classification and nosology
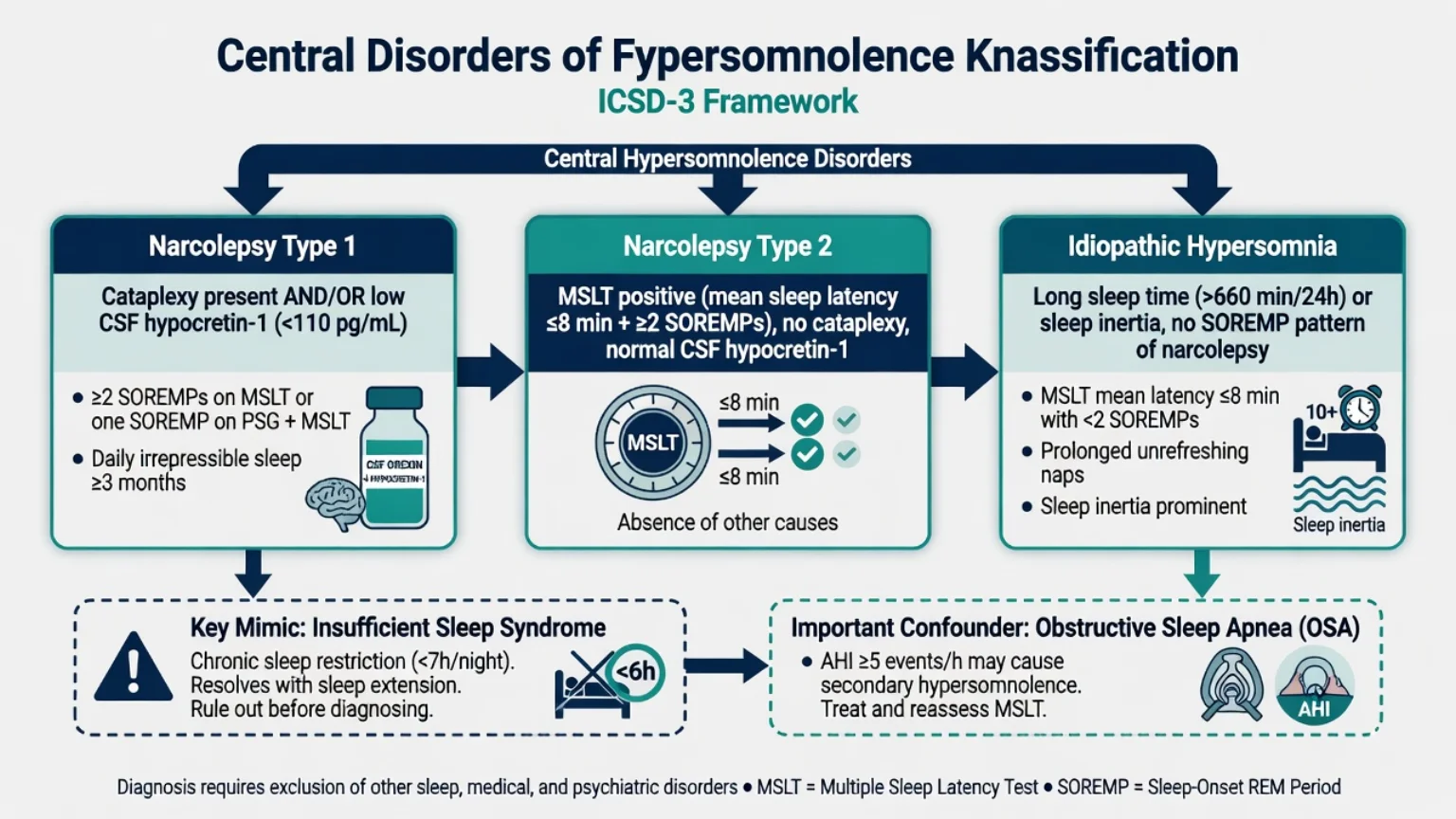
Narcolepsy type 1
- Cataplexy present and/or low CSF hypocretin
- Orexin neuron loss mechanism
- MSLT often short latency + SOREMPs
- Highest exam yield tetrad
Narcolepsy type 2
- No cataplexy
- Normal CSF hypocretin if measured
- MSLT criteria met after exclusions
- May convert phenotype over time rarely
Idiopathic hypersomnia
- Long sleep / unrefreshing naps
- Severe sleep inertia common
- Lacks classic narcolepsy SOREMP pattern
- Heterogeneous biology
Key mimics
- Insufficient sleep syndrome first
- OSA fragmentation
- Sedating drugs/substances
- Atypical depression hypersomnia
Epidemiology and risk
Headline epidemiology (exam anchors)
Population estimates place narcolepsy in the order of roughly 25–50 per 100,000, with substantial under-recognition and diagnostic delay measured in years in many cohorts.[8][2] Peak onset in adolescence and early adulthood is classic; childhood presentations are easy to mislabel as behavioural or learning problems.[1][8]
HLA-DQB1*06:02 is strongly enriched in NT1 but is common enough in the general population that it is supportive, never standalone diagnostic. Post-H1N1 infection and AS03-adjuvanted Pandemrix vaccination associations fuelled the modern autoimmune framing of orexin neuron destruction in susceptible hosts.[15][1]
Pathophysiology and mechanisms
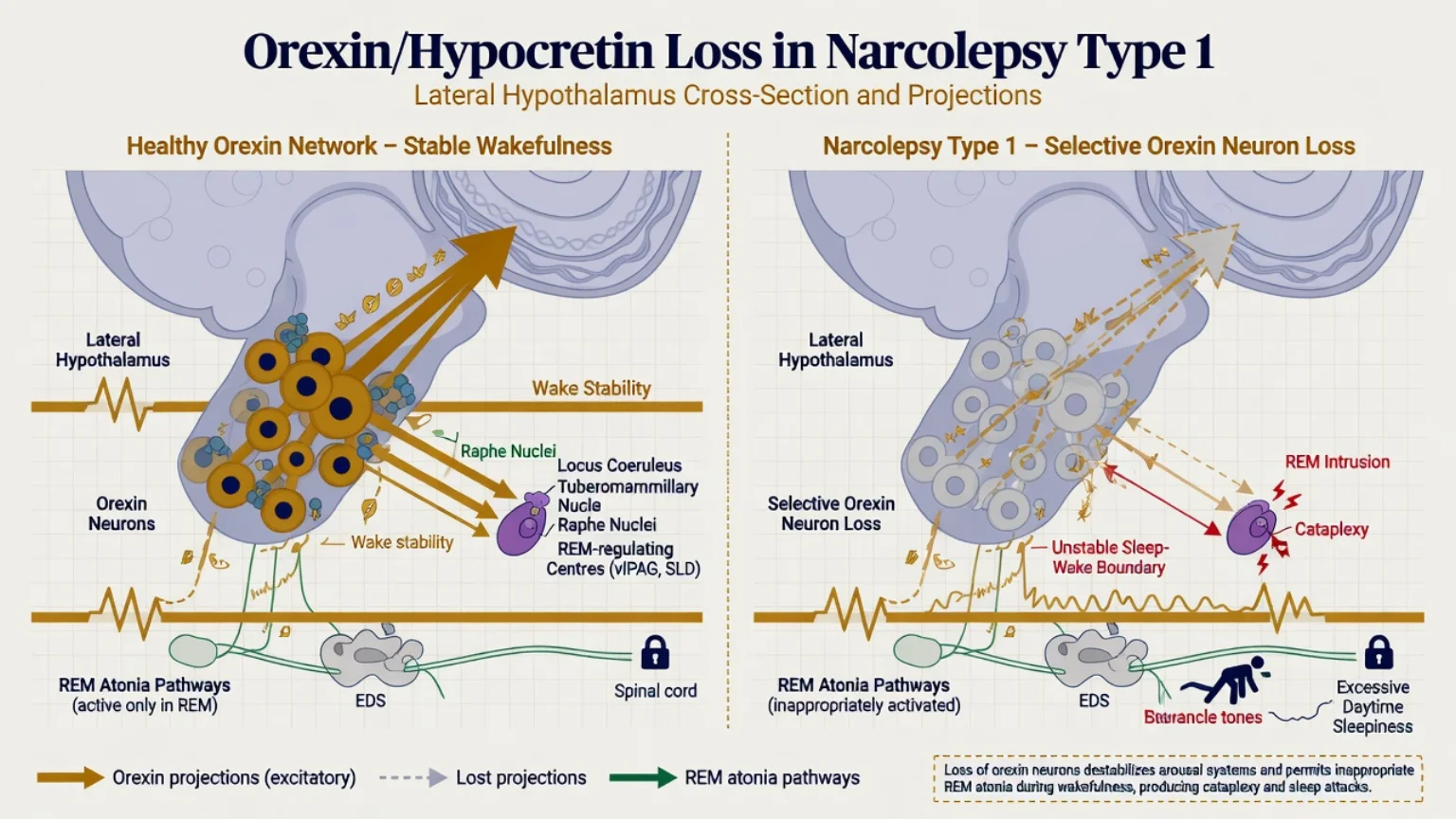
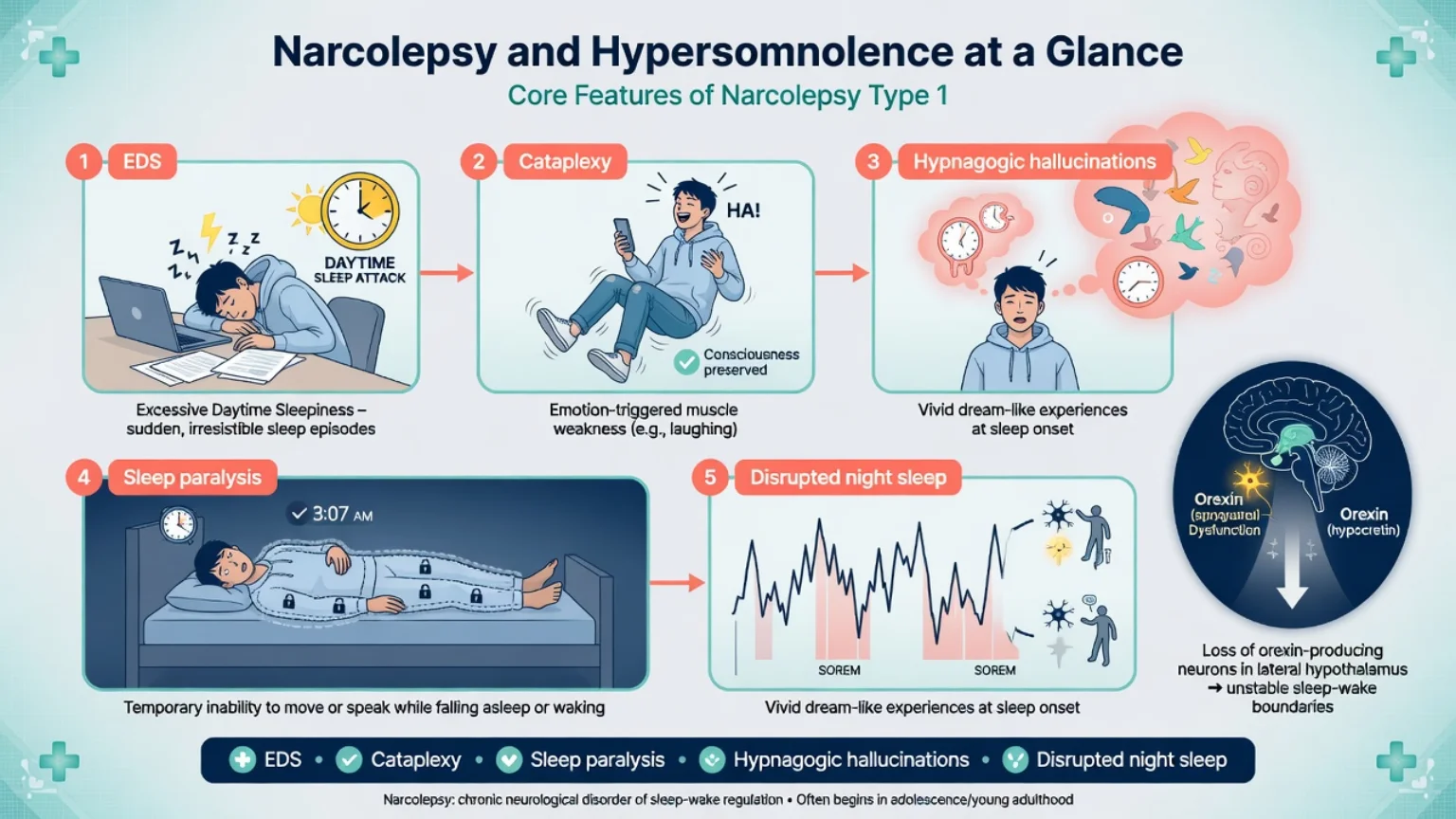
NT1 core lesion. Human pathology and CSF studies show selective loss of hypocretin/orexin neurons in the lateral hypothalamus with low CSF hypocretin-1.[3][4][5] Orexin normally stabilises the wake state and helps suppress inappropriate REM-state phenomena. Loss destabilises the sleep–wake boundary: sleep attacks, hypnagogic hallucinations, sleep paralysis, and cataplexy (REM-sleep atonia invading wakefulness with preserved consciousness).[1][2][3]
Autoimmune hypothesis. Genetic risk (HLA class II), temporal clustering after influenza/vaccine exposures in some regions, and T-cell directed attack on orexin neurons form the dominant pathophysiological narrative for classic NT1 — useful for viva depth without overclaiming universal causation for every case worldwide.[15][1]
NT2 and IH. NT2 lacks documented orexin deficiency by definition; IH is heterogeneous with long sleep and sleep inertia as clinical anchors rather than a single orexin biomarker.[16][9]
Clinical presentation
The classic tetrad (plus fifth pillar).
- Excessive daytime sleepiness / sleep attacks — irresistible, often brief, may include automatic behaviour.
- Cataplexy — bilateral loss of muscle tone with preserved consciousness, classically triggered by laughter, surprise, or anger; ranges from jaw sag and knee buckle to falls.
- Hypnagogic / hypnopompic hallucinations — vivid dream-like experiences at sleep onset/offset.
- Sleep paralysis — transient inability to move at sleep–wake transitions.
- Disrupted nocturnal sleep — fragmented night architecture is common in NT1 and often under-taught.[1][2]
Idiopathic hypersomnia phenotype. Long unrefreshing sleep, difficulty waking (sleep drunkenness/inertia), and daytime sleepiness without the full REM-intrusion tetrad of NT1.[16]
Psychiatry MSE traps. Hypnagogic hallucinations with insight and sleep-bound timing are not first-rank schizophrenia. Cataplexy is not syncope, seizure, or conversion by default — consciousness is retained and emotion triggers are classic. Severe EDS can look like amotivation or ADHD-like inattention until history is taken properly.[1][2]
Differential diagnosis
| Presentation | Favours | Against central hypersomnia alone |
|---|---|---|
| Sleeps 5 hours, weekends catch-up long | Insufficient sleep syndrome | Sleep debt must be corrected first |
| Loud snoring, high BMI, witnessed apnoeas | OSA | Treat/assess before final MSLT read |
| Starts after sedating antipsychotic / BZD | Medication-induced sleepiness | Review drug list before wake promoters |
| Low mood, leaden paralysis, rejection sensitivity | Atypical depression hypersomnia | Still exclude organic sleep disorders |
| Recurrent weeks-long sleep episodes in teen | Kleine–Levin syndrome | Episodic not continuous NT1 pattern |
| Collapse with loss of consciousness | Syncope / seizure | Cataplexy preserves awareness |
Always include substances, thyroid disease, anaemia, head injury, encephalitis, and hypothalamic lesions for secondary/symptomatic narcolepsy pathways.[1][9][16]
Assessment
History structure. Time in bed, total sleep time, naps, sleep attacks, cataplexy triggers and distribution, dream-like experiences at edges of sleep, sleep paralysis, nocturnal fragmentation, shift work, caffeine/alcohol/cannabis, current psychotropics, school/work failures, near-miss driving.[1][2]
Tools. Epworth Sleepiness Scale (ESS) quantifies subjective sleepiness for monitoring but does not diagnose narcolepsy alone. Partner/work collateral is often more honest than self-report. Screen mood, anxiety, ADHD-like symptoms, and suicide risk when function collapses.[1][7]
Risk domains. Fitness to drive and operate machinery; cataplexy injury; caregiving capacity; stimulant diversion risk if prescribed; oxybate safety rules if used.[7][6]
Investigations
- Fix the preconditions. Ensure adequate sleep opportunity; screen and treat clinically important OSA; plan psychotropic effects on REM carefully with sleep medicine before MSLT when feasible.[10][9]
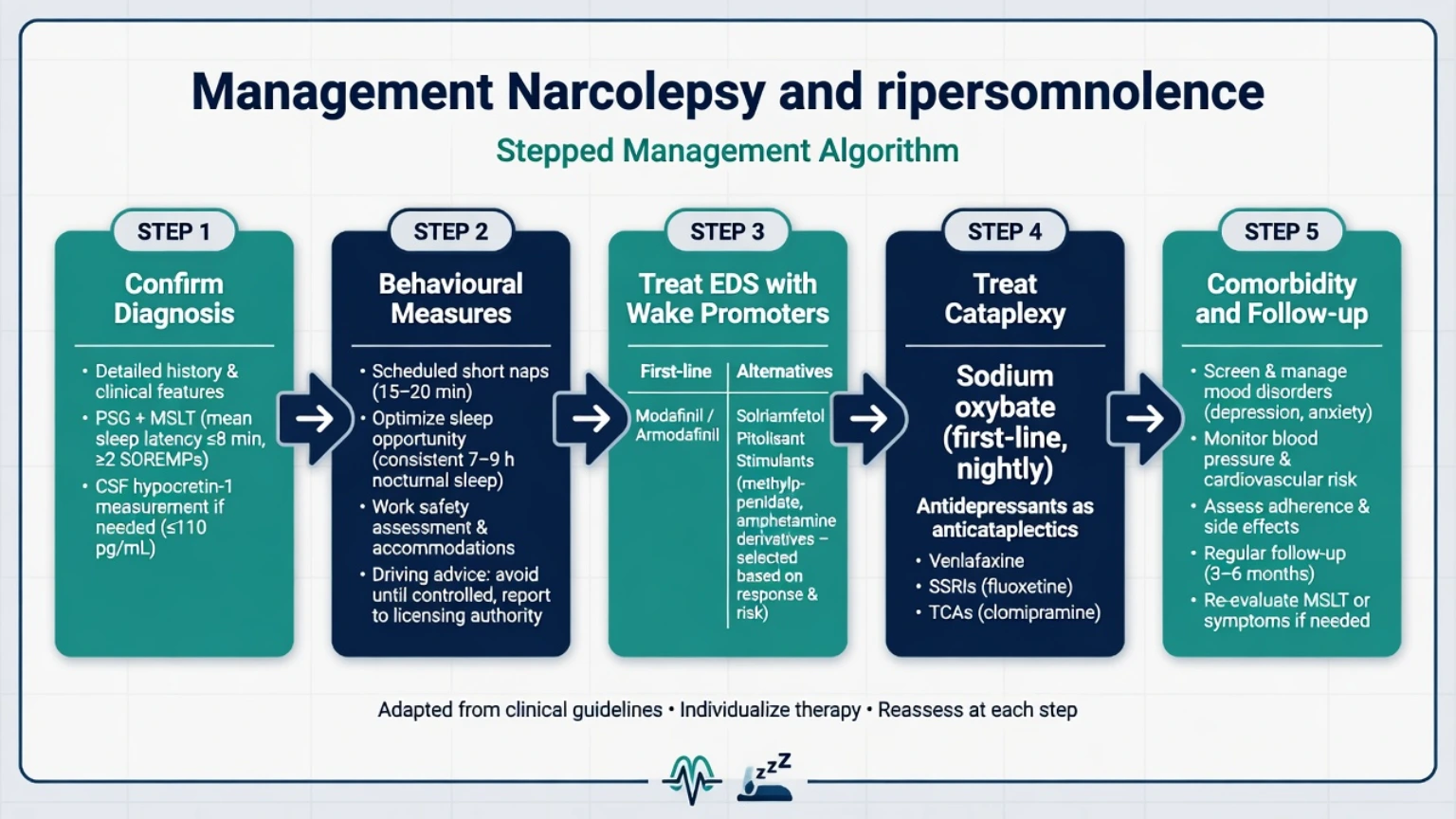
- Nocturnal PSG then MSLT. Classic teaching for narcolepsy support: mean sleep latency 8 minutes or less with 2 or more sleep-onset REM periods (SOREMPs) (with recognised caveats for drugs, sleep debt, and shift schedules). Practice parameters govern clinical use of MSLT and MWT.[10][1]
- CSF hypocretin-1. Low values support NT1 when available and indicated; especially helpful when cataplexy is ambiguous or MSLT confounded.[5][4]
- HLA-DQB1*06:02. Supportive enrichment only — never sole diagnostic criterion.[15][1]
- Labs as indicated. TFT, FBC, metabolic panel, toxicology; neuroimaging when secondary hypothalamic disease is plausible.
Acute and emergency management
- Cataplexy injury risk: falls, cooking burns, swimming — restrict high-risk activities until control improves; start anticataplectic pathway with specialist input.[2][7]
- Oxybate + alcohol/sedatives: treat as high-risk polypharmacy; educate and stop the combination.[12][6]
- Misdiagnosed psychosis: do not default to high-dose antipsychotics for sleep-bound hallucinations with insight — reformulate and treat the sleep disorder.[1]
Definitive management
Non-drug core
- Strategic scheduled naps (often brief, planned).
- Protect nocturnal sleep opportunity; regular schedule.
- Workplace/school accommodations; disability supports.
- Explicit driving and occupational counselling every review.[7][6]
Pharmacotherapy for EDS (wake promotion)
AASM 2021 guidance and European narcolepsy statements support structured pharmacotherapy for central hypersomnolence, with agent choice shaped by phenotype, comorbidity, licence, and controlled-substance rules.[6][7]
Illustrative adult dosing frames (always check current product information, age, hepatic/renal status, pregnancy, and local formulary — these are exam-facing anchors, not personalised prescriptions).[6][7][11]
- Modafinil: commonly 100–200 mg oral in the morning, titrated toward 200–400 mg/day in divided morning/midday doses as tolerated for narcolepsy EDS; monitor blood pressure, anxiety/insomnia, and rare serious rash signals. Multicentre RCT evidence supports efficacy for daytime somnolence.[11][6][7]
- Armodafinil: often 150–250 mg oral once in the morning where licensed.[6][7]
- Solriamfetol: narcolepsy trials commonly used 75–150 mg oral once daily for excessive sleepiness; monitor blood pressure and heart rate.[14][6]
- Pitolisant (H3 receptor inverse agonist): titrated per product info (often stepwise toward adult maximums such as 36 mg/day where labelled); QT and interaction checks matter; RCT data versus placebo/modafinil inform placement.[13][6][7]
- Traditional stimulants (methylphenidate, amphetamine salts): second-line or selected cases when first-line wake promoters fail or are unavailable; abuse liability and cardiovascular monitoring required.[6][7]
Cataplexy and consolidated night treatment
- Sodium oxybate (and related oxybate products where licensed): improves cataplexy and EDS in classic multicentre RCT evidence; typically twice-nightly oral dosing under controlled-substance protocols — never combine with alcohol or other CNS depressants; counsel on respiratory depression, enuresis, and misuse risk.[12][6][7]
- Anticataplectic antidepressants: REM-suppressing agents such as venlafaxine, clomipramine, SSRIs, or atomoxetine are used clinically for cataplexy when oxybate is unsuitable; monitor standard psychiatric adverse effects and withdrawal. Abrupt cessation can rebound cataplexy.[2][7][6]
Idiopathic hypersomnia notes
Modafinil-class agents are commonly first pharmacologic options; selected patients may access oxybate products under expanding licences/guidelines — individualise with sleep medicine rather than psychiatry-alone titration for complex cases.[16][6]
AASM 2021 (Maski et al.): clinical practice recommendations for treating central disorders of hypersomnolence — strong emphasis on evidence-graded wake promoters and oxybate-class options by disorder.[6] Europe 2021 (Bassetti et al.): adult and paediatric narcolepsy statements covering diagnosis, behavioural care, pharmacotherapy ladders, and comorbidities.[7] ANZ practice: sleep physician co-management for PSG/MSLT and controlled oxybate programmes; PBS/formulary access to modafinil and related agents varies — do not assume every trial agent is locally listed. Align fitness-to-drive advice with Australian/NZ licensing medical standards and occupational medicine where relevant.
Special populations and scenarios
- Children/adolescents: school failure, “laziness” stigma, behavioural mislabels; involve paediatric sleep expertise for dosing and educational plans.[7]
- Pregnancy/lactation: individualise; many wake promoters and oxybate lack simple safety green lights — obstetric and sleep liaison, non-drug safety first.[7]
- Older adults: cardiovascular risk of stimulants/solriamfetol; polypharmacy and fall risk from cataplexy.[6]
- Comorbid OSA: treat breathing disorder; residual NT1 still needs wake promotion.[1]
- Secondary narcolepsy: hypothalamic tumours, demyelination, traumatic injury — neurology partnership.[1]
- ANZ rural: delayed sleep-lab access should not delay behavioural safety planning and interim specialist advice.
Complications and pitfalls
- Multi-year misdiagnosis as depression, conversion, malingering, or primary psychosis.[1][2]
- MSLT after sleep restriction or on REM-active drugs without planning.
- HLA typing used as a stand-alone “rule-in.”
- Ignoring driving legislation.
- Oxybate + sedatives; stimulant diversion.
- Stopping anticataplectic antidepressants abruptly with rebound cataplexy.
Prognosis and disposition
NT1 is chronic after irreversible orexin neuron loss with current therapies; function can improve markedly with adherent multimodal treatment, scheduled naps, and workplace adaptation.[1][7] Disposition is shared care: sleep medicine for diagnosis and oxybate programmes; psychiatry for mood, ADHD-like comorbidity, suicide risk, and psychotropic interactions. Safety-net for near-misses, new injuries, severe depression, and medication misuse.
Exam pearls
NARCOLEPSY MAP (viva scaffold)
References
- [1]Scammell TE Narcolepsy N Engl J Med, 2015.PMID 26716917
- [2]Dauvilliers Y, Arnulf I, Mignot E Narcolepsy with cataplexy Lancet, 2007.PMID 17292770
- [3]Thannickal TC, Moore RY, Nienhuis R, et al. Reduced number of hypocretin neurons in human narcolepsy Neuron, 2000.PMID 11055430
- [4]Nishino S, Ripley B, Overeem S, et al. Hypocretin (orexin) deficiency in human narcolepsy Lancet, 2000.PMID 10615891
- [5]Mignot E, Lammers GJ, Ripley B, et al. The role of cerebrospinal fluid hypocretin measurement in the diagnosis of narcolepsy and other hypersomnias Arch Neurol, 2002.PMID 12374492
- [6]Maski K, Trotti LM, Kotagal S, et al. Treatment of central disorders of hypersomnolence: an American Academy of Sleep Medicine clinical practice guideline J Clin Sleep Med, 2021.PMID 34743789
- [7]Bassetti CLA, Kallweit U, Vignatelli L, et al. European guideline and expert statements on the management of narcolepsy in adults and children J Sleep Res, 2021.PMID 34173288
- [8]Longstreth WT Jr, Koepsell TD, Ton TG, et al. The epidemiology of narcolepsy Sleep, 2007.PMID 17310860
- [9]Sateia MJ International classification of sleep disorders-third edition: highlights and modifications Chest, 2014.PMID 25367475
- [10]Littner MR, Kushida C, Wise M, et al. Practice parameters for clinical use of the multiple sleep latency test and the maintenance of wakefulness test Sleep, 2005.PMID 15700727
- [11]US Modafinil in Narcolepsy Multicenter Study Group Randomized trial of modafinil as a treatment for the excessive daytime somnolence of narcolepsy Neurology, 2000.PMID 10720292
- [12]US Xyrem Multicenter Study Group A randomized, double blind, placebo-controlled multicenter trial comparing the effects of three doses of orally administered sodium oxybate with placebo for the treatment of narcolepsy Sleep, 2002.PMID 11833860
- [13]Dauvilliers Y, Bassetti C, Lammers GJ, et al. Pitolisant versus placebo or modafinil in patients with narcolepsy: a double-blind, randomised trial Lancet Neurol, 2013.PMID 24107292
- [14]Thorpy MJ, Shapiro C, Mayer G, et al. A randomized study of solriamfetol for excessive sleepiness in narcolepsy Ann Neurol, 2019.PMID 30694576
- [15]Partinen M, Kornum BR, Plazzi G, et al. Narcolepsy as an autoimmune disease: the role of H1N1 infection and vaccination Lancet Neurol, 2014.PMID 24849861
- [16]Billiard M, Sonka K Idiopathic hypersomnia Sleep Med Rev, 2016.PMID 26599679