Psych · Specialty psychiatry — sleep medicine interface
Obstructive sleep apnoea and psychiatry
Also known as OSA · Obstructive sleep apnea · Sleep-disordered breathing · CPAP psychiatry · STOP-BANG · Apnoea-hypopnoea index · OSA depression
Exam-exhaustive fellowship reference on obstructive sleep apnoea at the psychiatry interface — ICSD-3/AASM severity, epidemiology, mood and cognitive comorbidity, STOP-BANG screening, PSG/HSAT pathways, CPAP first-line care with SAVE caveats, psychotropic airway and weight effects, benzodiazepine risk, driving safety, and special populations. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
OSA is not a "lifestyle footnote" to mood clinics. FRANZCP MEQs test TRD plus obesity/snoring stems. MRCPsych CASCs test CPAP negotiation and driving advice. ABPN items test AHI bands, screening tools, and psychotropic interactions. A candidate who reads only this topic should defend screening, organic exclusion, first-line PAP, and safe prescribing at consultant depth.[13][15][16]
Overview and definition
Obstructive sleep apnoea is characterised by recurrent partial or complete upper-airway collapse during sleep, producing apnoeas and hypopnoeas, intermittent hypoxaemia, arousals, and sleep fragmentation. It sits within ICSD-3 sleep-related breathing disorders and is clinically framed as OSA when respiratory events are predominantly obstructive and accompanied by symptoms, daytime impairment, or relevant comorbidity.[21][15]
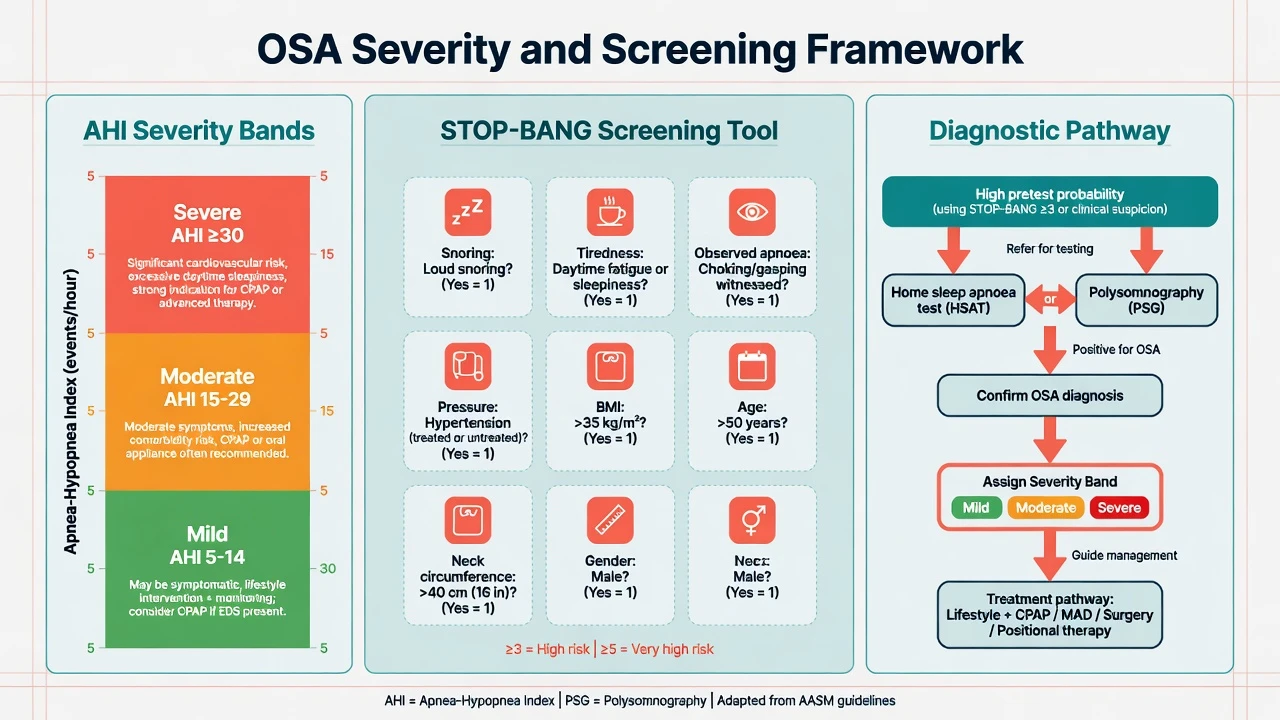
Severity (AHI bands — highest-yield MCQ). Conventional adult teaching uses apnoea–hypopnoea index (events per hour of sleep): mild 5–14, moderate 15–29, and severe ≥30. Clinical decisions integrate AHI with symptoms, desaturation burden, cardiovascular risk, and occupational safety — not AHI alone.[15][13]
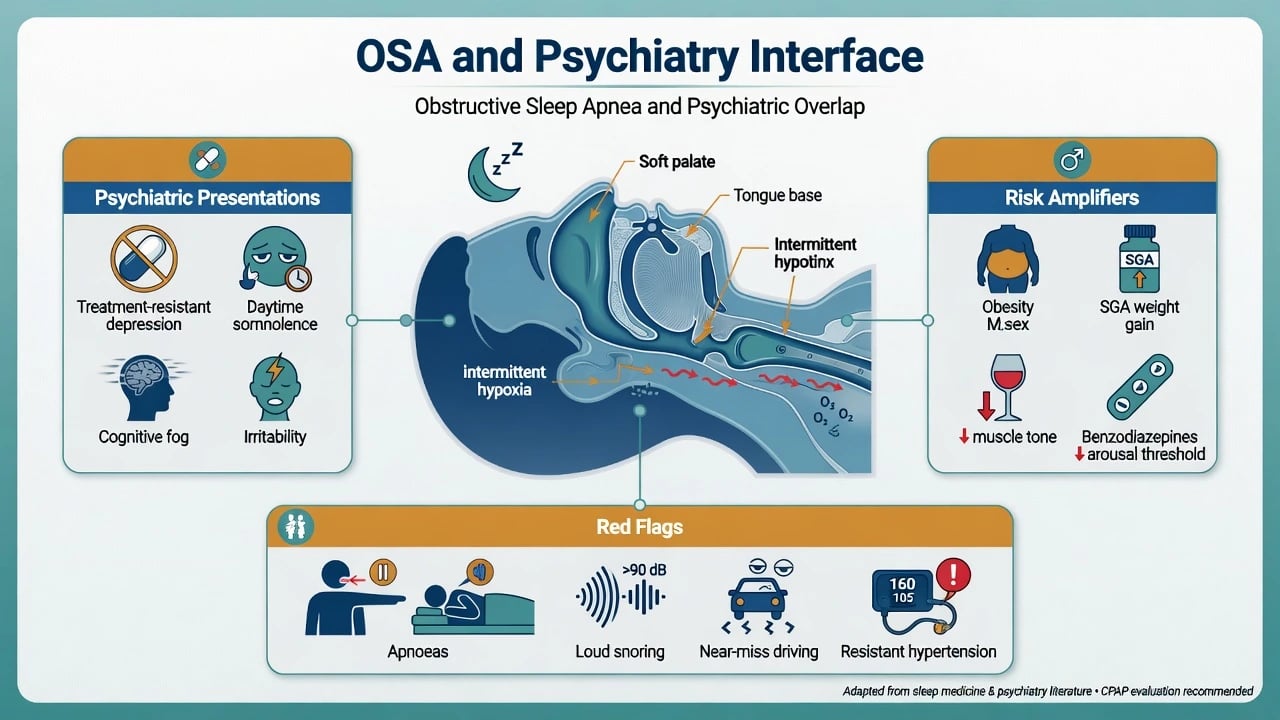
Psychiatry essence. Untreated OSA produces anergia, irritability, cognitive slowing, unrefreshing sleep, and depressive symptoms that look like residual MDD. Treating only the mood disorder while the airway collapses nightly is a classic fellowship fail.[5][6][9]
Classification and nosology
Obstructive events
- Airway collapse with ongoing effort
- Snoring, gasping common
- Obesity/craniofacial risk
- PAP is disease-modifying for AHI
Central events
- Reduced drive; effort absent
- Opioids, heart failure associations
- Different titration logic
- Do not assume pure OSA
Psychiatric mimicry
- TRD with anergia
- Cognitive fog / pseudo-dementia
- Hypersomnia vs fatigue
- SGA weight-amplified OSA
Related syndromes
- Primary snoring without high AHI
- Obesity hypoventilation
- Overlap COPD
- Upper airway resistance concepts
DSM-5-TR does not replace sleep-medicine nosology for OSA. Psychiatrists code the mental disorder and document OSA as a medical contributor requiring concurrent management.[21][6]
Epidemiology and risk
Epidemiology anchors for exams
Landmark population work (Wisconsin Sleep Cohort; Peppard updates; HypnoLaus) established that sleep-disordered breathing is common in middle-aged adults and that prevalence estimates rose as obesity and scoring sensitivity increased.[1][2][3] Global literature-based estimates place hundreds of millions of adults with OSA-range AHI, implying psychiatric services will encounter undiagnosed disease weekly.[4]
Psychiatric populations. Systematic review and meta-analysis show OSA is common across severe mental illness, with higher pooled clinical prevalence estimates in MDD than bipolar disorder or schizophrenia in Stubbs-order data; age and BMI are key moderators.[6][7] Population surveys link sleep-disordered breathing symptoms with probable major depression.[8] Longitudinal Wisconsin analyses show a dose–response association between sleep-related breathing disorder and depression, supporting a causal contribution rather than pure confounding.[5]
Classic risk factors. Male sex, older age, elevated BMI, large neck circumference, craniofacial restriction, nasal obstruction, menopause, alcohol near bedtime, and sedating medications.[1][2][15]
Pathophysiology and mechanisms
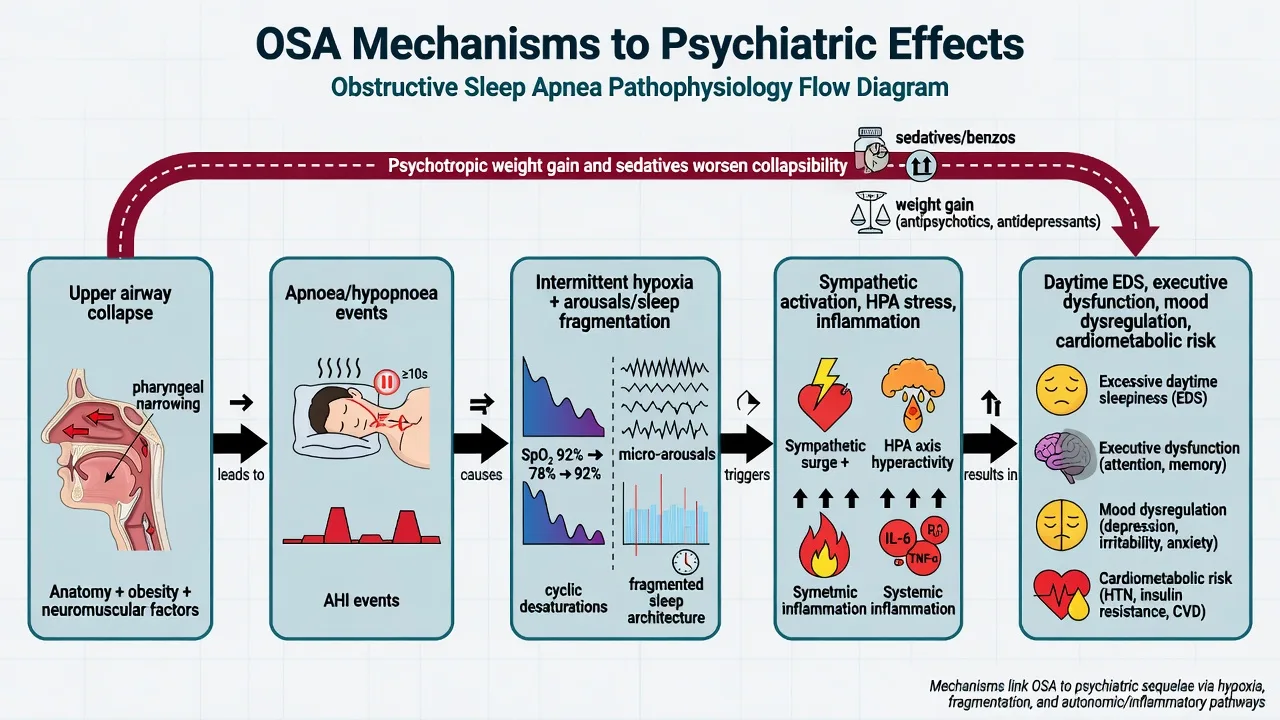
Recurrent pharyngeal collapse produces cyclical hypoxaemia, hypercapnia swings, and cortical arousals. Fragmented sleep architecture destroys restorative slow-wave and REM continuity. Downstream: sympathetic surges, HPA activation, systemic inflammation, endothelial dysfunction, hypertension, atrial fibrillation risk, insulin resistance, and daytime sleep propensity with executive dysfunction.[15][2]
Psychotropic amplification. Second-generation antipsychotics alter sleep continuity and frequently promote weight gain that worsens collapsibility; sedating antidepressants can help subjective sleep while increasing hangover and, via weight, OSA risk.[19][20] Opioids, hypnotics, and benzodiazepines can blunt arousal and upper-airway muscle tone; Cochrane synthesis examines effects of sedating medications on SDB severity, and observational data associate benzodiazepine use with acute respiratory failure risk in OSA cohorts.[17][18]
Clinical presentation
Bedside history. Loud snoring, witnessed apnoeas, gasping/choking awakenings, unrefreshing sleep, morning headache, dry mouth, nocturia, and partner-reported breathing pauses. Daytime: sleepiness (distinct from pure fatigue), microsleeps, irritability, reduced concentration, reduced libido.[15][11]
Psychiatric phenotypes examiners love. TRD phenotype (multiple antidepressant trials, persistent anergia, long unrefreshing sleep, elevated BMI, partner snoring); SGA metabolic phenotype (olanzapine/quetiapine/clozapine weight gain, daytime nodding, new hypertension); older-adult cognitive slowing mislabelled as dementia progression; and psychosis with reversed sleep phase, mask intolerance/paranoia about CPAP, and tobacco/obesity co-factors all warrant OSA screening before pure psychiatric escalation.[6][7][1]
Differential diagnosis
Discriminators beat lists. Loud snoring with witnessed apnoea and high BMI favours OSA (versus primary snoring if AHI is low). Unrefreshing sleep without snoring may be insomnia, depression, or RLS, but silent OSA still belongs on the differential in high-risk body habitus. Hypersomnia with true cataplexy points to narcolepsy type 1 rather than OSA alone. Reduced need for sleep with elevated mood is mania/hypomania until proven otherwise. Opioid-related pauses raise central/complex SDB. Nightly temazepam hangover is sedative effect and can coexist with and worsen OSA.[15][21][17]
Always exclude hypothyroidism, anaemia, heart failure, COPD overlap, substances, and circadian disorders as co-contributors.[15][21][17]
Assessment
Structure. Sleep schedule, substances (alcohol, cannabis, opioids), bed partner report, mood/anxiety/psychosis screen, suicide risk, driving/occupational risk, full medication list, BMI and neck, blood pressure.[15][11]
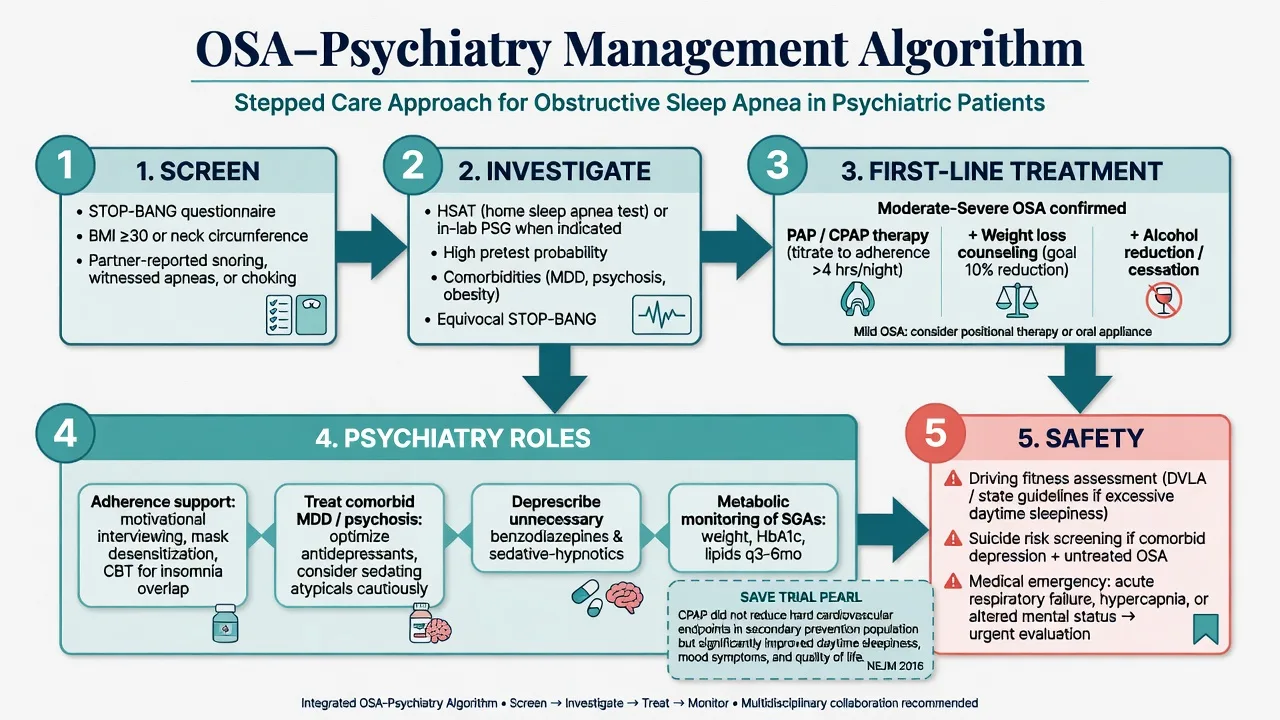
STOP and STOP-BANG. The STOP questionnaire (Snoring, Tiredness, Observed apnoea, blood Pressure) and STOP-BANG (adds BMI, Age, Neck, Gender) are validated screening tools; higher STOP-BANG scores associate with higher OSA probability and triage urgency of testing.[11][12] Do not invent service-specific cut-offs under exam stress — name the domains and state that elevated scores warrant referral.
Scales. Epworth Sleepiness Scale for sleep propensity context; depression scales (PHQ-9) knowing somatic items overlap with OSA; document SI carefully because sleep disturbance elevates suicide-risk domains in broader literature.[8][9]
Investigations
AASM diagnostic guidance supports polysomnography and, in appropriate uncomplicated high-probability adults, home sleep apnoea testing pathways; complex, atypical, or comorbid presentations often need in-lab PSG.[13][22] ACP guidance similarly emphasises sleep study for unexplained daytime sleepiness with clinical suspicion.[22]
Psychiatry practical rules. High pretest OSA probability plus psychiatric illness warrants referral without waiting for perfect mood remission; typical pure insomnia without OSA clues can start behavioural insomnia care without mandating PSG first; and sleep reports should be read for AHI/RDI, oxygen nadir, positional component, and residual events on treatment.[13][15]
Baseline metabolic panel, ECG, and glucose/lipids when SGAs are involved remain standard psychopharmacology practice alongside OSA work-up.[20][15]
Acute and emergency management
- Stop or urgently review benzodiazepines/opioids in untreated severe OSA.[17][18]
- Inpatient psychiatry: minimise unnecessary night sedation, nurse head-of-bed elevation when safe, early liaison with medicine/sleep.
- Treat active suicidal ideation as co-primary with sleep pathology when both are present.[8][9]
Definitive management
Airway and lifestyle (disease-modifying core)
Positive airway pressure (CPAP/APAP/BiPAP as indicated) is first-line therapy for moderate–severe OSA in adults; AASM systematic review and GRADE assessment support PAP for improving disease-oriented and selected patient-oriented outcomes when used.[14][15] Adherence (hours per night, nights per week) determines real-world benefit more than the machine sitting by the bed.
Adjuncts. Weight loss, alcohol reduction especially evening, positional therapy for positional OSA, mandibular advancement devices in selected mild–moderate cases, ENT surgery for anatomical subsets — sleep/ENT-led.[15]
Mood and CPAP evidence
Depressive symptoms are common in OSA and improve substantially with adherent CPAP in clinical cohorts (Edwards-order before–after data).[9] Secondary analyses from the SAVE programme and meta-analysis of trials suggest CPAP can reduce depression and anxiety symptoms versus control, even though hard cardiovascular endpoint benefits were not demonstrated in the primary SAVE analysis.[10][16]
SAVE pearl (exam). In adults with moderate–severe OSA and established cardiovascular disease, CPAP plus usual care did not significantly reduce the primary composite cardiovascular endpoint versus usual care alone — do not oversell CPAP as proven secondary CV event prevention in that design. Symptom, blood pressure, and quality-of-life benefits still matter clinically.[16] Meta-analysis of PAP and cardiovascular events/death similarly cautions against assuming hard outcome reduction across all adult sleep apnoea populations.[23]
Psychiatry-specific prescribing
- Prefer behavioural sleep strategies and treat parent psychiatric illness; do not use open-ended benzodiazepines as default sleepers in high-probability OSA.[17][18]
- If short-term pharmacologic sedation is unavoidable (e.g., acute mania, severe agitation), choose the lowest effective dose with medical monitoring and an exit plan — jurisdiction product information governs exact dosing.
- Sedating antidepressants (mirtazapine, trazodone, low-dose doxepin/TCAs) may help comorbid depression-insomnia phenotypes but watch weight, hangover, and residual OSA.[19]
- SGAs: continue when psychosis/mood stability requires them, but intensify metabolic monitoring (weight, BMI, waist, fasting glucose/lipids per local protocol) and OSA screening when BMI rises.[20]
- Do not escalate quetiapine solely to "knock out" snoring patients with depression.
AASM: diagnostic testing (Kapur) and PAP treatment evidence (Patil); Epstein long-term care pathway remains a classic structured approach to evaluation and chronic management.[13][14][15] ACP: sleep study for unexplained daytime sleepiness with clinical concern.[22] ANZ practice: refer to accredited sleep physicians/labs; CPAP funding and driving standards are jurisdiction-specific (advise per local Austroads/NZTA-type guidance without fabricating cut-offs). Rural/FIFO patients may wait for PSG — start weight, alcohol, sedative deprescribing, and safety advice immediately.
Subtypes and high-yield scenarios
High-yield scenarios include TRD clinic with positive STOP-BANG (sleep study before endless fourth-line agents when airway clues dominate); clozapine clinic metabolic surge with OSA screen and CPAP support for energy/adherence; bipolar sleep protection without high-dose night benzodiazepines; PTSD nightmares coexisting with OSA (treat both); and commercial drivers with EDS who need documented advice and urgent escalation.[2][6][7][15]
Complications and pitfalls
Missing OSA and labelling pure treatment-resistant depression, chronic benzodiazepine scripts that raise respiratory risk signals in OSA cohorts, overselling SAVE-neutral hard CV endpoints as "CPAP does nothing," ignoring CPAP non-adherence (claustrophobia, mask leak, nasal obstruction, psychosis, depression, cost), and ignoring partner history are classic examinable pitfalls.[5][6][16][18]
Prognosis and disposition
OSA is a chronic disease. Effective PAP with adherence can improve sleepiness, mood symptoms, and quality of life; residual psychiatric illness still needs standard care.[9][14] Shared care: sleep clinic for device titration/adherence data; psychiatry for mood, psychosis, substance, and suicide risk. Safety-net for escalating EDS, SI, witnessed cyanosis, and occupational near-misses.
Special populations
- Older adults: cognitive mimicry; avoid sedative-hypnotics; fall risk.[17]
- Pregnancy: OSA risk rises with BMI; specialist obstetric–sleep pathways; avoid unnecessary benzos.
- Youth: adenotonsillar disease dominant; ADHD/behavioural interface — paediatric sleep referral.
- Intellectual disability / Down syndrome: high OSA prevalence; caregiver-reported snoring and restless sleep are essential.
- Indigenous and remote ANZ: access barriers to labs — start risk reduction and prioritise referral urgency by EDS/occupational risk.
Exam pearls
AIRWAY PSY (OSA–psychiatry checklist)
Use this checklist every time obesity, snoring, TRD, SGA weight gain, or daytime sleepiness appears in a stem.[7][12][14]
References
- [1]Young T, Palta M, Dempsey J, et al. The occurrence of sleep-disordered breathing among middle-aged adults N Engl J Med, 1993.PMID 8464434
- [2]Peppard PE, Young T, Barnet JH, et al. Increased prevalence of sleep-disordered breathing in adults Am J Epidemiol, 2013.PMID 23589584
- [3]Heinzer R, Vat S, Marques-Vidal P, et al. Prevalence of sleep-disordered breathing in the general population: the HypnoLaus study Lancet Respir Med, 2015.PMID 25682233
- [4]Benjafield AV, Ayas NT, Eastwood PR, et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis Lancet Respir Med, 2019.PMID 31300334
- [5]Peppard PE, Szklo-Coxe M, Hla KM, et al. Longitudinal association of sleep-related breathing disorder and depression Arch Intern Med, 2006.PMID 16983048
- [6]Gupta MA, Simpson FC Obstructive sleep apnea and psychiatric disorders: a systematic review J Clin Sleep Med, 2015.PMID 25406268
- [7]Stubbs B, Vancampfort D, Veronese N, et al. The prevalence and predictors of obstructive sleep apnea in major depressive disorder, bipolar disorder and schizophrenia: A systematic review and meta-analysis J Affect Disord, 2016.PMID 26999550
- [8]Wheaton AG, Perry GS, Chapman DP, et al. Sleep disordered breathing and depression among U.S. adults: National Health and Nutrition Examination Survey, 2005-2008 Sleep, 2012.PMID 22467983
- [9]Edwards C, Mukherjee S, Simpson L, et al. Depressive Symptoms before and after Treatment of Obstructive Sleep Apnea in Men and Women J Clin Sleep Med, 2015.PMID 25902824
- [10]Zheng D, Xu Y, You S, et al. Effects of continuous positive airway pressure on depression and anxiety symptoms in patients with obstructive sleep apnoea: results from the sleep apnoea cardiovascular Endpoint randomised trial and meta-analysis EClinicalMedicine, 2019.PMID 31312807
- [11]Chung F, Yegneswaran B, Liao P, et al. STOP questionnaire: a tool to screen patients for obstructive sleep apnea Anesthesiology, 2008.PMID 18431116
- [12]Chung F, Subramanyam R, Liao P, et al. High STOP-Bang score indicates a high probability of obstructive sleep apnoea Br J Anaesth, 2012.PMID 22401881
- [13]Kapur VK, Auckley DH, Chowdhuri S, et al. Clinical Practice Guideline for Diagnostic Testing for Adult Obstructive Sleep Apnea: An American Academy of Sleep Medicine Clinical Practice Guideline J Clin Sleep Med, 2017.PMID 28162150
- [14]Patil SP, Ayappa IA, Caples SM, et al. Treatment of Adult Obstructive Sleep Apnea With Positive Airway Pressure: An American Academy of Sleep Medicine Systematic Review, Meta-Analysis, and GRADE Assessment J Clin Sleep Med, 2019.PMID 30736888
- [15]Epstein LJ, Kristo D, Strollo PJ Jr, et al. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults J Clin Sleep Med, 2009.PMID 19960649
- [16]McEvoy RD, Antic NA, Heeley E, et al. CPAP for Prevention of Cardiovascular Events in Obstructive Sleep Apnea N Engl J Med, 2016.PMID 27571048
- [17]Mason M, Cates CJ, Smith I Effects of opioid, hypnotic and sedating medications on sleep-disordered breathing in adults with obstructive sleep apnoea Cochrane Database Syst Rev, 2015.PMID 26171909
- [18]Wang SH, Chen WS, Tang SE, et al. Benzodiazepines Associated With Acute Respiratory Failure in Patients With Obstructive Sleep Apnea Front Pharmacol, 2018.PMID 30666205
- [19]Wichniak A, Wierzbicka A, Walecka M, et al. Effects of Antidepressants on Sleep Curr Psychiatry Rep, 2017.PMID 28791566
- [20]Monti JM, Torterolo P, Pandi Perumal SR The effect of second-generation antipsychotic drugs on sleep parameters in patients with unipolar or bipolar disorder Sleep Med, 2016.PMID 27692282
- [21]Sateia MJ International classification of sleep disorders-third edition: highlights and modifications Chest, 2014.PMID 25367475
- [22]Qaseem A, Dallas P, Owens DK, et al. Diagnosis of obstructive sleep apnea in adults: a clinical practice guideline from the American College of Physicians Ann Intern Med, 2014.PMID 25089864
- [23]Yu J, Zhou Z, McEvoy RD, et al. Association of Positive Airway Pressure With Cardiovascular Events and Death in Adults With Sleep Apnea: A Systematic Review and Meta-analysis JAMA, 2017.PMID 28697252