Psych · Specialty psychiatry — clinical paraphilic disorders
Paraphilic disorders (clinical)
Also known as Paraphilias · Pedophilic disorder · Exhibitionistic disorder · Voyeuristic disorder · Fetishistic disorder · Sexual sadism disorder · Sexual masochism disorder · Compulsive sexual behaviour disorder · Antiandrogen therapy · WFSBP paraphilia guidelines
Exam-exhaustive fellowship atlas on clinical paraphilic disorders — DSM-5-TR/ICD-11 interest-versus-disorder threshold, epidemiology of interests, mechanisms (dual control and motivation–facilitation), voluntary help-seeking assessment, differential from CSBD/OCD/gender incongruence, child-protection and suicide red flags, CBT and WFSBP-aligned stepped pharmacotherapy, subtype scenarios, and regional ethics. Clinical primary; forensic interface secondary. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Exam framing
Fellowship examiners test nosological precision without moralising. This leaf is clinical first: voluntary help-seeking, ego-dystonic distress, differential from CSBD and OCD sexual obsessions, confidentiality limits, and specialist drive-reduction algorithms. Forensic sexual-offending pathways, actuarial tools, and MAPPA-type systems are a secondary interface (see related forensic topics), not the primary lens.[1][8][11]
Definition and classification
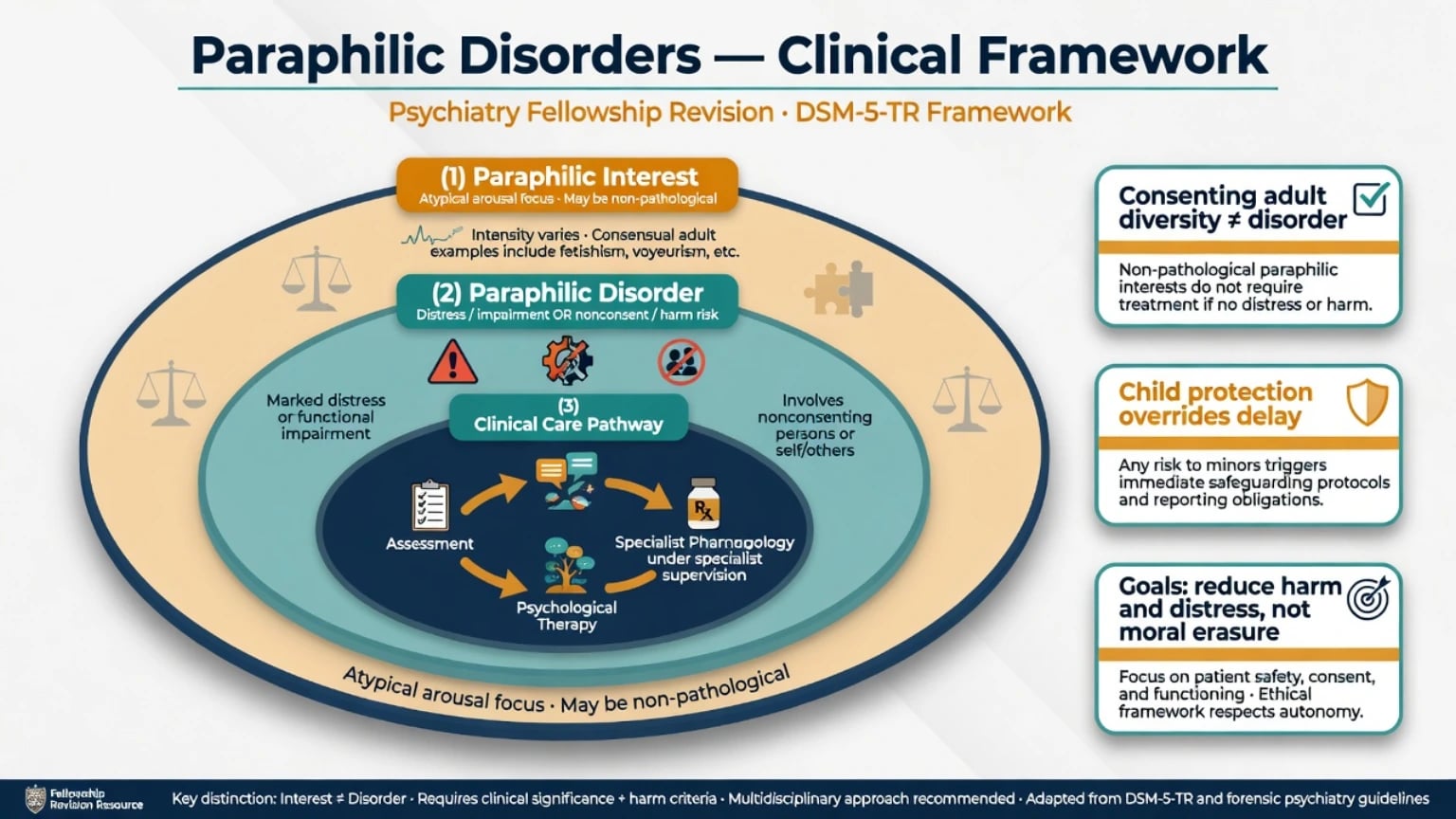
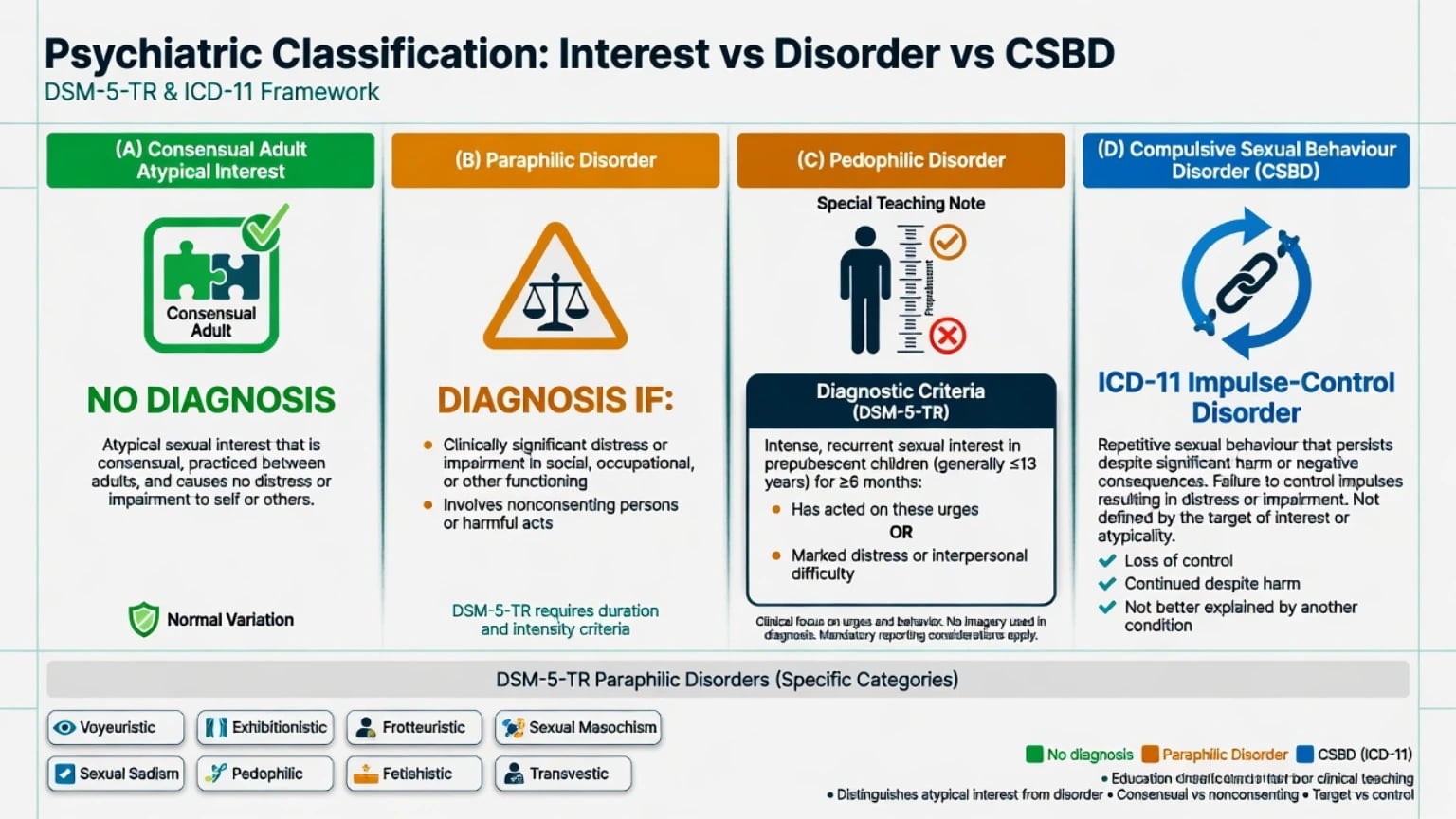
Paraphilia denotes an intense and persistent atypical sexual interest (fantasy, urge, or behaviour). Paraphilic disorder requires the interest plus clinically significant distress or impairment in the person, or involvement of nonconsenting persons / personal harm or risk of harm to others. This threshold is the single highest-yield teaching point across DSM-5-TR and ICD-11 reform work.[1][2]
DSM-5-TR categories commonly examined
| Disorder | Core focus of arousal (exam shorthand) |
|---|---|
| Voyeuristic | Observing unsuspecting persons who are naked, undressing, or engaging in sexual activity |
| Exhibitionistic | Exposing genitals to unsuspecting persons |
| Frotteuristic | Touching or rubbing against a nonconsenting person |
| Sexual masochism | Being humiliated, beaten, bound, or otherwise made to suffer |
| Sexual sadism | Physical or psychological suffering of another person |
| Pedophilic | Preferential sexual interest in prepubescent children |
| Fetishistic | Nonliving objects or highly specific nongenital body parts |
| Transvestic | Cross-dressing (distinct from gender incongruence pathways) |
| Other specified / unspecified | Residual clinical presentations |
| These eight named categories plus residual codes are the core DSM-5-TR teaching map for paraphilic disorders; duration, intensity, and clinical significance criteria apply per manual — name the manual you are using in stems.[1] |
Pedophilic disorder — precise teaching
Preferential sexual interest in prepubescent children is a sexual interest pattern; pedophilic disorder is diagnosed when the person has acted on the urges or the urges cause marked distress or interpersonal difficulty (standard DSM teaching). Specify exclusive vs nonexclusive; sex of interest; limited to incest when applicable. Pedophilia is neither necessary nor sufficient for every child sexual offence, and not every person with pedophilic interest offends.[8][11]
ICD-11 and CSBD
ICD-11 proposals centre consent, harm, and distress, deliberately depathologising many consensual adult atypical practices that were historically over-pathologised.[1][2] Compulsive sexual behaviour disorder (CSBD) in ICD-11 is framed as an impulse-control problem: persistent failure to control intense sexual impulses resulting in repetitive behaviour with marked distress or impairment — not defined by an atypical target, and not automatically a paraphilia.[2][14] Kafka’s proposed hypersexual disorder for DSM-5 was not adopted as an official DSM-5 category; state the nosological debate rather than treating “sex addiction” as a free-standing DSM diagnosis.[7][14]
Paraphilic interest
- Atypical focus of arousal
- May be lifelong and ego-syntonic
- Consensual adult practice ≠ disorder
- No diagnosis solely for diversity
Paraphilic disorder
- Interest + distress/impairment
- OR nonconsent/harm risk
- Risk assessment is core
- Therapy ± specialist pharmacology
CSBD (ICD-11)
- Impulse-control framing
- Repetitive behaviour despite harm
- Not defined by atypical target
- Heavy comorbidity formulation
OCD sexual obsessions
- Ego-dystonic intrusive thoughts
- Anxiety-driven, not preferred arousal
- Compulsions reduce anxiety
- Treat as OCD, not paraphilia
Epidemiology and risk
Community surveys show paraphilia-associated arousal patterns and interests are not rare; clinic disorders and forensic samples are highly selected and must not be confused with community base rates.[9][10] Ahlers and colleagues documented paraphilia-associated sexual arousal patterns in a community male sample, underscoring that atypical content alone does not equal disorder.[10] Joyal and Carpentier reported provincial survey prevalence of paraphilic interests and behaviours, supporting teaching that interest ≫ diagnosed disorder.[9]
Exam-order epidemiology (order-of-magnitude teaching)
Pathophysiology and mechanisms
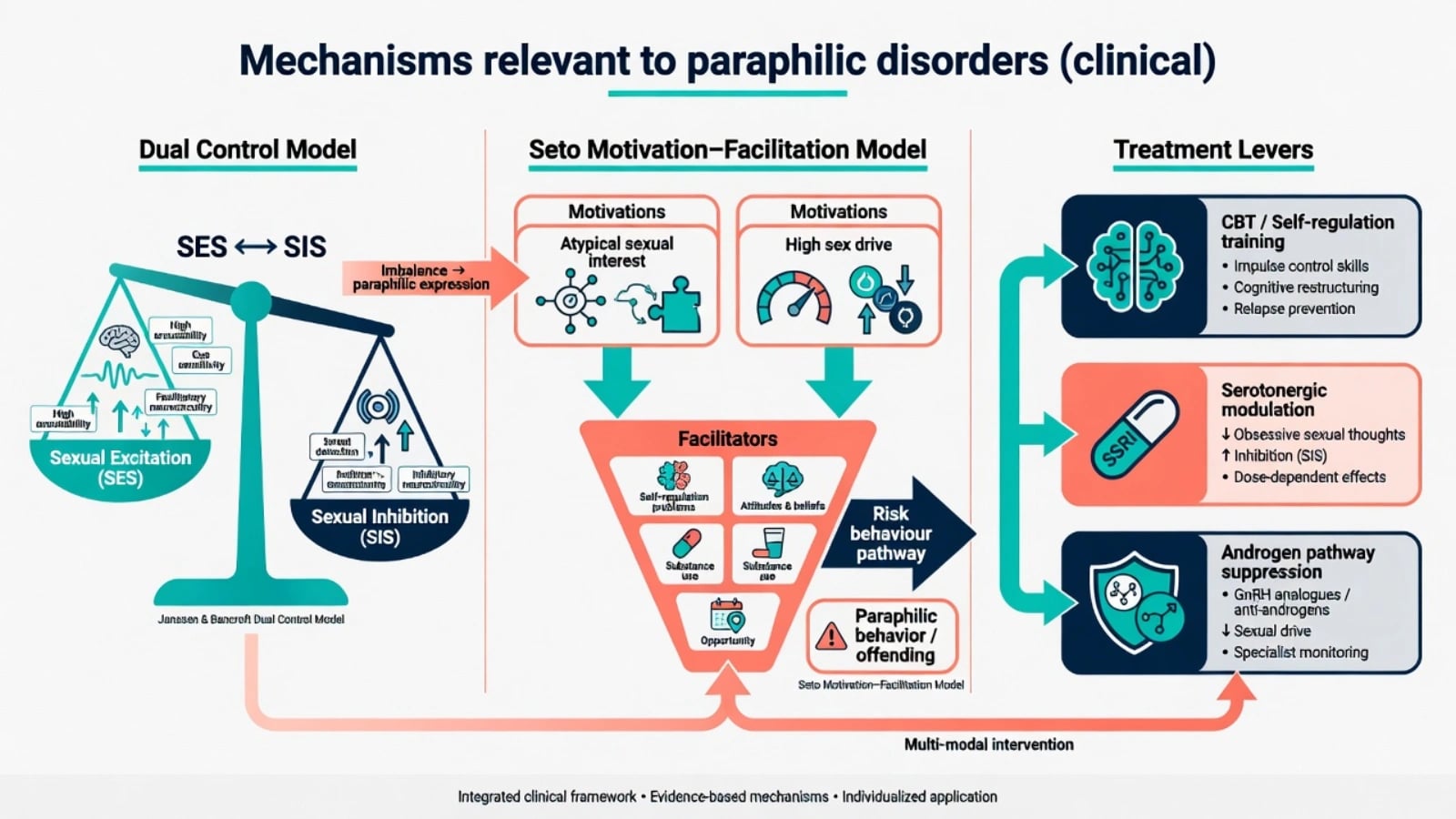
Mechanisms are multifactorial: developmental and learning pathways, high sexual drive and compulsivity dimensions, and dual-control imbalance between sexual excitation and inhibition systems. Do not invent a single gene or lesion as the exam answer.[8]
Motivation–facilitation model (Seto). Motivations (e.g. atypical sexual interest, high sex drive) interact with facilitators (self-regulation problems, attitudes supportive of offending, substance use, opportunity). This model prevents two fatal exam errors: equating interest with offence, and ignoring facilitators when interest is present.[11]
Pedophilia research signals. Neurodevelopmental and white-matter research findings exist in selected samples; they do not justify routine diagnostic neuroimaging in general adult clinics.[8]
Pharmacological rationale. Serotonergic tone modulates sexual drive and compulsivity — the rationale for SSRI strategies in selected patients. Androgen-dependent components of sexual drive underpin antiandrogen and GnRH pathways in severe high-risk specialist care.[3][4][5]
Clinical presentation
Voluntary clinic. Ego-dystonic fantasies, fear of acting, relationship rupture after disclosure, escalating online pornography focused on atypical themes, or prevention-oriented help-seeking without known offences.[8]
MSE language (examples). “Expresses exclusive pedophilic fantasies with marked shame; denies contact offences; works in a school — access risk high.” “Exhibitionistic urges on public transport with partial insight and alcohol use before episodes.” Document insight, planning, access, substance use, minimisation, and suicidality without humiliation.[8][11]
Atypical presentations. Female clinic cases are less frequent but real; late midlife disclosure; cultural stigma delaying care; intellectual disability with capacity and vulnerability complexity — still apply the same interest-versus-disorder and risk thresholds.[8][9]
Differential diagnosis
| Presentation | Prefer | Discriminators |
|---|---|---|
| Consensual adult kink, no distress | Not a disorder | Consent + no impairment |
| Preferred atypical arousal + distress/nonconsent | Paraphilic disorder | Preference pattern + threshold |
| High porn use, loss of control, typical targets | CSBD / habit / anxiety | Control failure, not atypical target |
| Intrusive unwanted sexual thoughts with anxiety rituals | OCD | Ego-dystonic, not preferred fantasy |
| Sexual disinhibition in mania | Mood episode | Elevated mood, reduced need for sleep |
| Cross-dressing for gender affirmation | Gender incongruence path | Identity motives, not fetish arousal |
| Child sexual offence without pedophilic preference | Offence + other risk factors | Situational, antisocial, substance |
| Use the table as a discriminator map: non-pathological diversity, true disorder threshold, CSBD, OCD, mania, gender pathways, and offence without pedophilic preference.[1][2][7][14] |
Gender incongruence is not a paraphilia; ICD-11 relocation of gender incongruence reflects scientific and human-rights shifts while care pathways remain clinically important.[2]
Assessment
Permission-based sexual history. Normalise the topic; move from open to specific questions: interests, age of onset, exclusivity, fantasy versus behaviour, consent, online behaviour, frequency, distress, and goals of care (stop risk, reduce shame, preserve relationship, legal requirements).[1][3]
Risk domain (always when nonconsent or children possible). Current access to children or vulnerable persons; prior acts; escalation; grooming; substance use; antisocial attitudes; treatability and engagement. Confidentiality has limits — mandatory reporting and public protection duties are jurisdiction-specific; state the principle and local statutes rather than inventing foreign section numbers.[4][8]
Suicide risk. Shame, blackmail, arrest, and relationship collapse commonly precipitate acute suicidality — screen every high-stigma presentation in parallel with victim-protection work.[4][8]
Collateral and records. When risk is live, multiagency information is not optional. Maintain a therapeutic stance without colluding with minimisation.[4][11]
Investigations
No laboratory or imaging test diagnoses a paraphilia. Tests guide medical fitness for drive-reduction pharmacology and exclude rare organic mimics of late-onset disinhibition.[3][4]
Before antiandrogen or GnRH pathways: baseline bloods (FBC, U&E, LFT), metabolic panel, lipids, glucose, morning testosterone as indicated, cardiovascular risk assessment, and bone health planning for prolonged androgen suppression. Toxicology when substances facilitate risk. Specialist phallometry or viewing-time measures belong in expert forensic settings, not routine general adult clinics.[4][5][12]
Acute and emergency management
Acute tasks: safety of potential victims; medical stabilisation if intoxicated; explain confidentiality limits; crisis plan for the patient; document decisions; escalate to forensic/public protection pathways when indicated.[4][8]
Definitive management
Principles
- Do not diagnose consensual adult atypical interests without distress or nonconsent.
- Risk first when children or nonconsenting adults are involved.
- Psychological treatments are foundational for most help-seeking presentations.
- Pharmacological drive reduction is for selected high-drive, highly distressing, or high-risk disorders within specialist frameworks — not first-line for low-risk ego-dystonic fetishistic disorder without risk.[3][4][5]
Psychological treatments
CBT adapted to sexual behaviour problems, self-management and relapse-prevention skills, addressing dynamic risk factors (substance use, emotional dysregulation, opportunity control), motivational work, and couple therapy when appropriate. For pedophilic help-seekers without known offences, prevention-oriented programmes and structured self-management are clinically important — always within local reporting law.[3][8]
Pharmacotherapy (WFSBP-aligned)
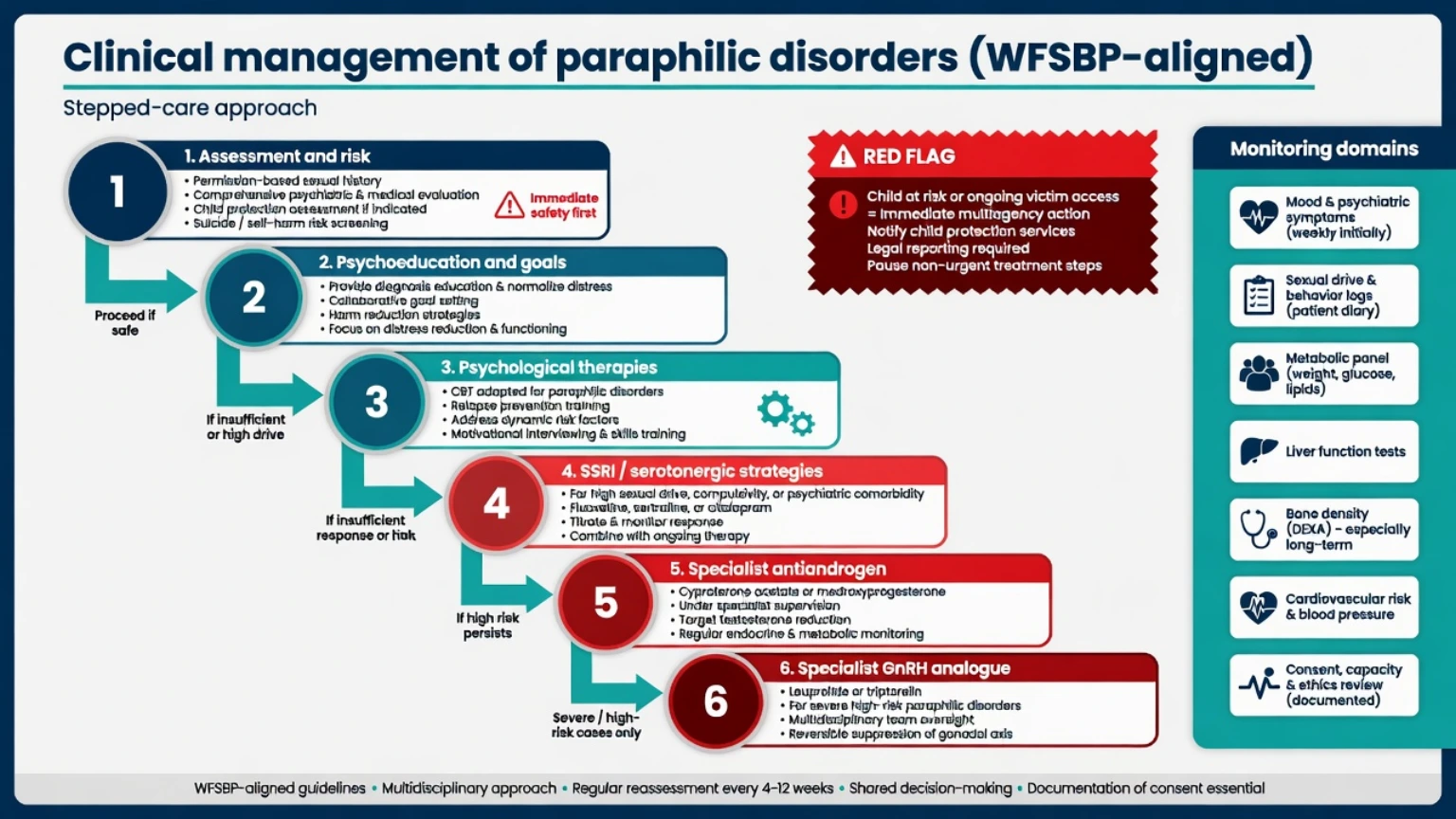
WFSBP guidelines for biological treatment of paraphilias (2010) and the 2020 pharmacological update outline stepped intensity with informed consent, medical monitoring, and legal–ethical clarity.[3][4]
| Step | Strategy | Exam-level notes |
|---|---|---|
| 1 | Psychological therapy ± risk management | Foundation for nearly all |
| 2 | SSRIs / serotonergic strategies | High drive, compulsivity, comorbid depression/OCD |
| 3 | Steroidal antiandrogens | Specialist; e.g. cyproterone or medroxyprogesterone pathways where available |
| 4 | GnRH analogues (LHRH agonists) | Severe high-risk; systematic review supports specialist use |
| WFSBP-aligned teaching escalates intensity with risk and drive rather than starting at androgen suppression for every distressed patient.[3][4][5][12] |
SSRIs. Used at antidepressant-class dosing ranges (e.g. sertraline typically titrated within usual adult depression ranges such as 50–200 mg oral daily, or fluoxetine 20–60 mg oral daily, individualised) to reduce drive/compulsivity and treat comorbid mood/OCD. Counsel on delayed onset, sexual side-effects, and early suicide-risk monitoring after initiation in depressed patients. Exact agent choice is comorbidity- and formulary-dependent.[3][4][5]
Antiandrogens and GnRH analogues. Reserved for severe, high-risk, or treatment-resistant presentations under specialist supervision. Turner and Briken’s systematic review supports LHRH agonist use in sexual offenders or men at risk of sexual offending with paraphilic disorders, with careful selection and monitoring.[12] Monitoring domains to name at viva: sexual drive and behaviour logs, mood and suicidality, metabolic status, liver function where relevant, bone mineral density with prolonged suppression, cardiovascular risk, and thromboembolic considerations depending on agent.[4][5][6][12]
Subtypes and clinical scenarios
- Pedophilic disorder, help-seeking, no known offence: prevention-oriented psychological care; assess access (work/family); mandatory-reporting principles; consider SSRI if high drive/distress; escalate pharmacology only with risk and specialist input.[8][4]
- Exhibitionistic / voyeuristic / frotteuristic disorders: behavioural control plans, substance work, legal realities, therapy ± SSRI.
- Sexual sadism with nonconsent risk versus consensual BDSM (not a disorder when consenting adults, no distress threshold met).[1]
- Fetishistic / transvestic disorders with ego-dystonic distress: therapy first; avoid over-medicalisation.
- CSBD overlap: treat control failure, comorbidities, and digital behaviour; do not force a paraphilia label without atypical target criteria.[14]
Complications and pitfalls
- Pathologising consensual diversity; missing child-protection duties; colluding with minimisation.
- Antiandrogens without monitoring or consent; “chemical castration” as populist framing.
- Confusing OCD sexual obsessions with preferred paraphilic fantasy.
- Assuming all people who sexually offend against children have pedophilic disorder (false), and that all people with pedophilic interest offend (false).[8][11][13]
- Iatrogenic harms of androgen suppression and SSRI sexual side-effects.
Hanson and Morton-Bourgon’s meta-analysis of sexual recidivism predictors supports structured attention to antisocial orientation and sexual deviance as risk-relevant domains in offender populations — useful for forensic interface teaching, not for diagnosing community help-seekers.[13]
Prognosis and disposition
Atypical interests often persist. Clinical goals are usually risk reduction, prevention of harm, reduced distress, improved self-control, and psychosocial function — not guaranteed eradication of all atypical arousal.[3][4][8]
Most voluntary presentations are managed in outpatient specialist psychosexual or forensic-community interfaces. Step up intensity with escalating risk, non-engagement, high victim access, or need for androgen-suppression monitoring. Safety-net for new child access, offline escalation, and post-legal suicidality.[3][4]
Special populations
Adolescents. Developmental caution before lifelong adult paraphilic labels; online contexts matter; child-protection duties still apply when harm is present.[4]
Intellectual disability. Capacity, vulnerability to exploitation, and behavioural support frameworks; do not over-label normative developmental sexuality while still protecting others from nonconsent harm.[3][4]
Older adults. New-onset sexual disinhibition with cognitive change → exclude neurocognitive/frontal pathology before attributing a primary lifelong paraphilia.[8]
Women. Under-represented in clinic samples; do not assume absence of paraphilic disorders or of victimisation risk pathways.[9][10]
Cultural / Indigenous ANZ contexts. Stigma and help-seeking barriers require cultural safety; harm to children is never relativised under cultural framing.[4]
Evidence and regional guidelines
ANZ: RANZCP ethics and jurisdiction-specific mandatory reporting (state/territory child-protection law; public-interest disclosures). Specialist sexual-offender and prevention services vary by jurisdiction. WFSBP algorithms provide the international pharmacological framing used in fellowship answers.[3][4] UK: MRCPsych expects interest-versus-disorder precision, CSBD/ICD-11 literacy, and confidentiality limits. MAPPA multiagency public protection for relevant offenders; GMC public-interest disclosure principles. US: ABPN blueprint items cover paraphilic disorders; APA ethics require protection of identifiable potential victims; mandatory reporting varies by state. India (MD/DNB / NEET-SS): Theory/viva emphasise DSM/ICD criteria, risk, and ethics; local statutes and limited specialist access shape disposition while WFSBP principles still organise answers.[1][2]
Exam pearls
- Interest ≠ disorder; consenting adult kink ≠ pathology.[1]
- Pedophilia ≠ every child sex offence; every pedophilic interest ≠ offence.[8][11]
- CSBD is ICD-11 impulse-control, not automatic paraphilia; Kafka hypersexual is not an official DSM-5 category.[7][14]
- WFSBP ladder: psychology ± SSRI → antiandrogen → GnRH for severe high-risk.[3][4]
- Confidentiality has limits when identifiable children/others are at risk — name local duties, not foreign statute numbers.[4][8]
- Goals: harm and distress reduction, not moral erasure of preference.[3][4]
Related topics
Sexual dysfunction and paraphilias (hub overview) · Sexual offending (forensic primary) · OCD · Antisocial personality disorder · Gender dysphoria and affirming care · Suicide risk assessment · Violence risk assessment · Professional ethics and boundaries. Use the hub topic for phase-based sexual dysfunction detail and the forensic leaf for offence-focused risk instruments.[1][8]
References
- [1]Krueger RB, Reed GM, First MB, et al. Proposals for Paraphilic Disorders in the International Classification of Diseases and Related Health Problems, Eleventh Revision (ICD-11) Arch Sex Behav, 2017.PMID 28210933
- [2]Reed GM, Drescher J, Krueger RB, et al. Disorders related to sexuality and gender identity in the ICD-11: revising the ICD-10 classification based on current scientific evidence, best clinical practices, and human rights considerations World Psychiatry, 2016.PMID 27717275
- [3]Thibaut F, De La Barra F, Gordon H, et al. The World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for the biological treatment of paraphilias World J Biol Psychiatry, 2010.PMID 20459370
- [4]Thibaut F, Cosyns P, Fedoroff JP, et al. The World Federation of Societies of Biological Psychiatry (WFSBP) 2020 guidelines for the pharmacological treatment of paraphilic disorders World J Biol Psychiatry, 2020.PMID 32452729
- [5]Assumpção AA, Garcia FD, Garcia HD, et al. Pharmacologic treatment of paraphilias Psychiatr Clin North Am, 2014.PMID 24877704
- [6]Garcia FD, Thibaut F Pharmacologic treatment of sex offenders with paraphilic disorder Curr Psychiatry Rep, 2013.PMID 23572328
- [7]Kafka MP Hypersexual disorder: a proposed diagnosis for DSM-V Arch Sex Behav, 2010.PMID 19937105
- [8]Seto MC Pedophilia Annu Rev Clin Psychol, 2009.PMID 19327034
- [9]Joyal CC, Carpentier J The Prevalence of Paraphilic Interests and Behaviors in the General Population: A Provincial Survey J Sex Res, 2017.PMID 26941021
- [10]Ahlers CJ, Schaefer GA, Mundt IA, et al. How unusual are the contents of paraphilias? Paraphilia-associated sexual arousal patterns in a community-based sample of men J Sex Med, 2011.PMID 19929918
- [11]Seto MC The Motivation-Facilitation Model of Sexual Offending Sex Abuse, 2019.PMID 28715948
- [12]Turner D, Briken P Treatment of Paraphilic Disorders in Sexual Offenders or Men With a Risk of Sexual Offending With Luteinizing Hormone-Releasing Hormone Agonists: An Updated Systematic Review J Sex Med, 2018.PMID 29289377
- [13]Hanson RK, Morton-Bourgon KE The characteristics of persistent sexual offenders: a meta-analysis of recidivism studies J Consult Clin Psychol, 2005.PMID 16392988
- [14]Krueger RB Diagnosis of hypersexual or compulsive sexual behavior can be made using ICD-10 and DSM-5 despite rejection of this diagnosis by the American Psychiatric Association Addiction, 2016.PMID 27086656