Psych · Specialty psychiatry — sleep medicine interface
Parasomnias
Also known as Disorders of arousal · NREM parasomnia · Sleepwalking · Somnambulism · Sleep terrors · Night terrors · Confusional arousals · Nightmare disorder · REM sleep behaviour disorder · REM sleep behavior disorder · RBD · Sleep-related eating disorder · Sexsomnia
Exam-exhaustive fellowship atlas on parasomnias — NREM disorders of arousal versus REM parasomnias (nightmare disorder, RBD), ICSD-3/DSM-5-TR nosology, epidemiology, state-dissociation and RSWA mechanisms, RBD–synucleinopathy risk, differential from seizures/OSA/drug behaviours, video-PSG, bedroom safety, melatonin/clonazepam for RBD, IRT and prazosin nuance for nightmares, and BAP/AASM guideline deltas. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Parasomnias are not comic “sleepwalking stories.” FRANZCP MEQs test NREM versus REM discriminators, RBD as a neurodegenerative prodrome, and safety-first plans. MRCPsych CASCs test plain-language explanation to partners after nocturnal injury. ABPN items test ICSD maps, drug-induced complex behaviours, and nightmare treatment hierarchy. A candidate who reads only this leaf should defend assessment, organic exclusion, and stepped care at consultant depth without relying solely on the broader sleep hub page.[3][6][8]
Overview and definition
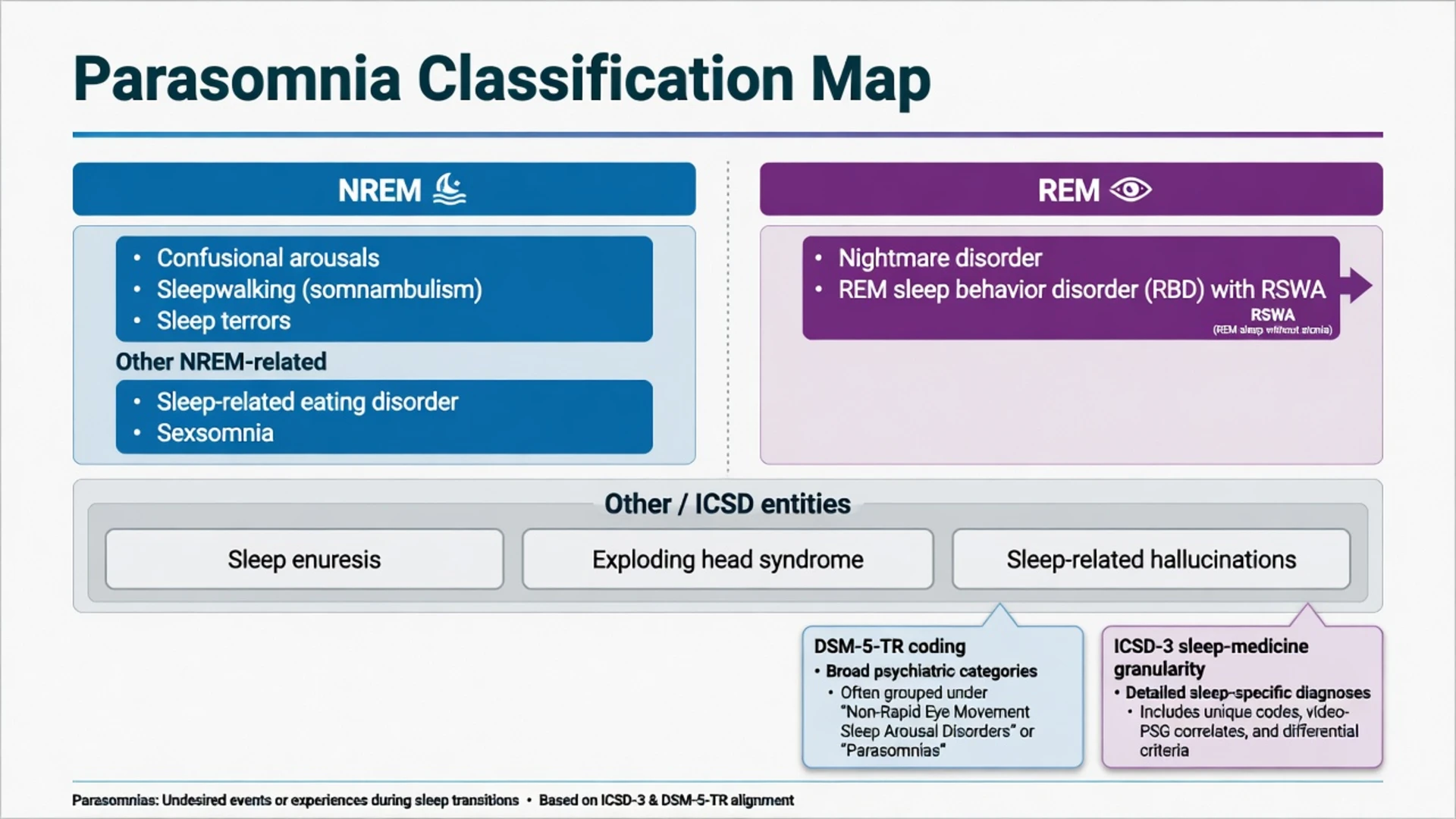
Parasomnias are undesirable physical events or experiences that occur during entry into sleep, within sleep, or during arousals from sleep. ICSD-3 groups them among major sleep pathology categories alongside insomnia, breathing, hypersomnolence, circadian, and movement disorders; psychiatrists must navigate this map even when the mental health record codes a narrower DSM-5-TR construct such as nightmare disorder or non-REM sleep arousal disorder.[3]
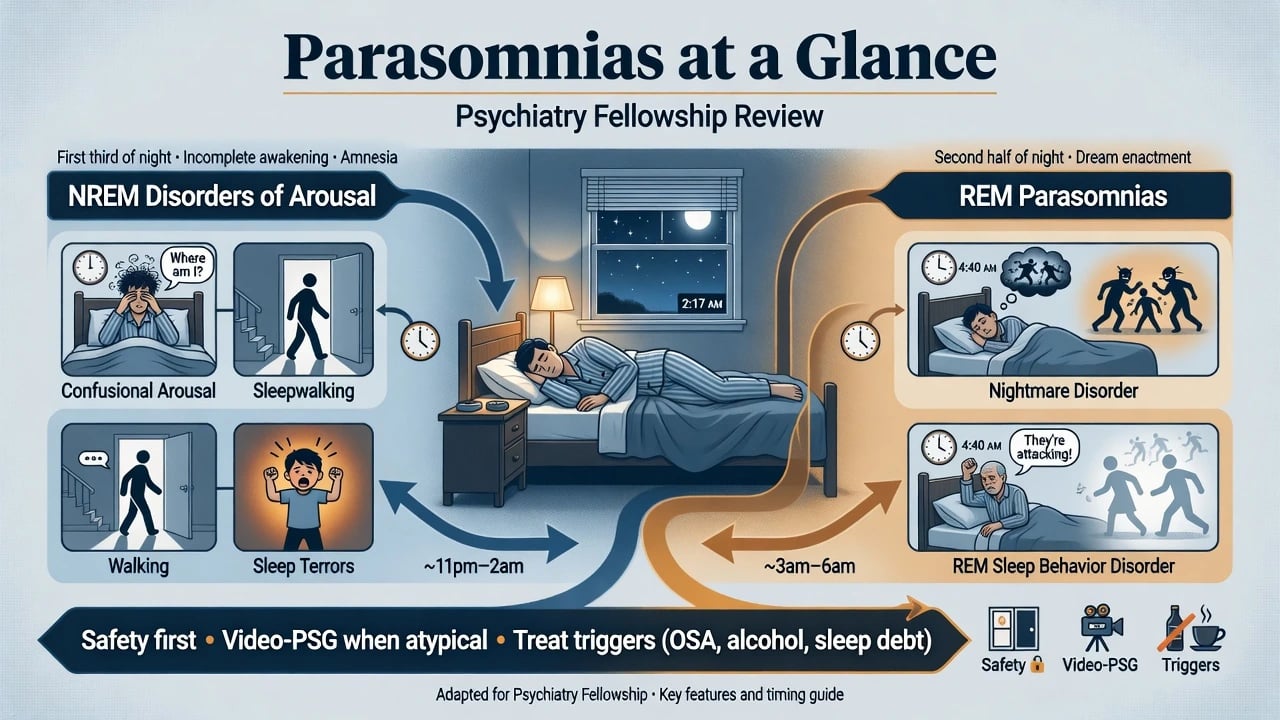
Clinical essence. Two systems dominate exam stems:
- NREM disorders of arousal (DOA) — confusional arousals, sleepwalking, sleep terrors — incomplete transitions out of deep NREM sleep with relative unresponsiveness and often limited recall.[8][16]
- REM parasomnias — nightmare disorder (vivid dysphoric dreams with full awakening and orientation) and REM sleep behaviour disorder (RBD) (dream enactment with loss of normal REM atonia).[7][4]
Other entities examiners use as traps: sleep-related eating disorder (SRED), sexsomnia, sleep enuresis, exploding head syndrome, and medication- or alcohol-facilitated complex sleep behaviours.[2][3]
Classification and nosology
Confusional arousals
- Sit/speak confused in bed
- First third of night typical
- Poor responsiveness
- Partial/no dream narrative
Sleepwalking
- Ambulation/complex acts
- Injury and exit risk
- Amnesia common
- Genetic/family history frequent
Sleep terrors
- Autonomic storm, scream
- Hard to console
- Amnesia on settling
- Not the same as nightmare
RBD
- Later-night dream acts
- Matches dream content
- Alert on waking
- Synucleinopathy prodrome
DSM-5-TR language. Non-REM sleep arousal disorders cover sleepwalking and sleep terror types; nightmare disorder is coded separately; RBD appears as rapid eye movement sleep behaviour disorder. ICSD-3 remains the sleep laboratory’s finer map for DOA spectrum, RBD diagnostic criteria including RSWA, and related entities.[3]
Epidemiology and risk
Headline epidemiology (exam anchors)
In a large adult general-population interview study, confusional arousals, night terrors, and sleepwalking were each reported in the low single-digit percentages and declined with age, with associations to other sleep and mental disorders — useful order-of-magnitude anchors rather than precise global constants.[13]
Childhood NREM parasomnias are common and often self-limited. Adult-onset or newly injurious DOA should trigger a search for secondary drivers: OSA, sleep deprivation, alcohol, sedative-hypnotics, stress, medical illness, and seizure mimics.[8][2]
RBD risk framing. Classic clinic series described dream-enacting behaviours with injury potential; idiopathic RBD is now recognised as a powerful long-term marker of neurodegenerative synucleinopathy (Parkinson disease, dementia with Lewy bodies, multiple system atrophy). Multicentre longitudinal work and meta-analytic syntheses show substantial cumulative conversion risk over multi-year follow-up — examiners expect counselling and surveillance language, not false reassurance that “it is only dreams.”[7][6][15]
Pathophysiology and mechanisms
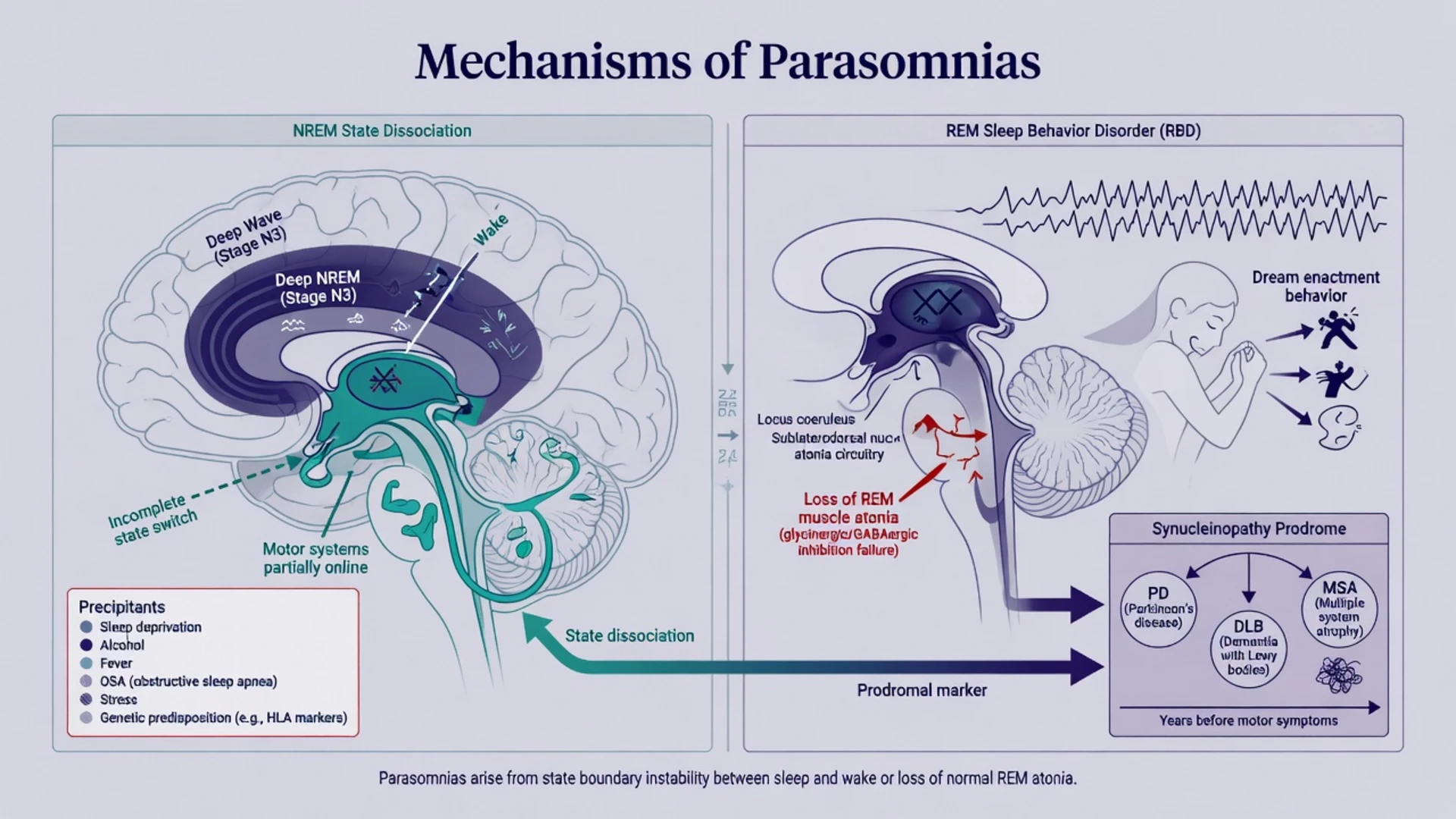
NREM DOA as state dissociation. Sleepwalking and related DOA reflect partial arousals in which motor and affective systems activate while full cortical wakefulness and episodic memory encoding remain incomplete. Genetic predisposition interacts with precipitants: sleep debt, irregular schedules, fever, stress, alcohol, and sleep-disordered breathing.[8][16]
RBD. Normal REM sleep includes skeletal muscle atonia. In RBD, REM sleep without atonia (RSWA) permits dream enactment — punching, kicking, leaping, vocalisation — classically in the second half of the night, with patients often alert and able to report a matching dream on awakening.[7][4]
Nightmares. Dysphoric REM mentation culminates in awakening with orientation and detailed recall. PTSD nightmares add trauma memory reconsolidation and noradrenergic hyperarousal — the mechanistic rationale historically used for alpha-1 blockade with prazosin, tempered by later mixed trial data.[10][11][12]
Drug mechanisms examiners love.
- Alcohol and sleep deprivation fragment sleep and facilitate NREM events.
- Z-drugs and other sedative-hypnotics can produce complex sleep-related behaviours.
- Some antidepressants are associated with dream enactment or RBD-like phenomena and require dechallenge reasoning.
- Cholinesterase inhibitors and other agents may intensify nightmares in vulnerable patients (history-driven review).[2][1]
Clinical presentation
History language examiners want. Time of night (first third versus second half), degree of arousal and orientation, dream recall content matching behaviour, amnesia, consolability, vocalisation, ambulation, injury, bed-partner report, family history of childhood sleepwalking/terrors, OSA clues, substances, and medication list.[8][2]
NREM DOA phenotype. Episodes often arise from deep NREM in the first sleep cycles. The person may sit, talk nonsense, look through the examiner, scream with marked autonomic surge (terrors), or leave the bed. Forcible restraint can escalate thrashing. Morning amnesia is common. Sleep terrors are not nightmares: the person is hard to wake and typically cannot narrate a long dream story.[8][13]
RBD phenotype. Later-night dream enactment, eyes usually closed, behaviour congruent with dream plot, rapid alertness on awakening, and partner injuries are classic. Ask explicitly about anosmia, constipation, dream content of being attacked, and subtle motor slowness — prodromal synucleinopathy clues.[7][6]
Nightmare disorder. Repeated extended, extremely dysphoric, well-remembered dreams that cause awakening with full alertness and clinically significant distress or impairment. PTSD nightmares often recreate trauma themes; idiopathic nightmare disorder lacks that obligatory trauma content.[9][10]
SRED and sexsomnia. Involuntary nocturnal eating with partial/no recall (SRED) and sleep-related sexual behaviour (sexsomnia) sit at the forensic and safety interface — medication review (including sedative-hypnotics), partner safety, and specialist assessment outweigh moralising formulations.[2]
Differential diagnosis
| Presentation | Favours | Against pure primary parasomnia alone |
|---|---|---|
| First-third night, amnesia, hard to console, family history | NREM DOA | Late-night vivid dream report matching acts |
| Second-half night, dream enactment, alert on waking | RBD | Childhood-only calm sleepwalking history without RSWA work-up |
| Stereotyped hypermotor spells, clustering, daytime seizures | Nocturnal epilepsy | Variable incomplete arousals with deep-sleep context |
| Loud snoring, obesity, apnoeas, morning headache | OSA-triggered arousals/“pseudo-RBD” | Pure psychiatric nightmare without breathing clues |
| Onset after zolpidem/alcohol binge | Drug/alcohol complex behaviour | Lifelong untreated childhood pattern unchanged |
| Trauma replay dreams, daytime PTSD | PTSD nightmares | Blank terror with amnesia and inconsolability |
Always include nocturnal panic, dissociative behaviours when forensic issues dominate, delirium in older inpatients, and medication-induced phenomena.[2][8][4]
Assessment
Core structure. Chronotype and sleep opportunity, episode phenomenology with bed-partner or smartphone video collateral, substances (alcohol near bedtime), prescription and OTC sedatives, antidepressants, OSA screen, trauma/mood/psychosis screen, injury history, weapons in bedroom, cognitive and motor soft signs in older adults, driving/occupational impact of sleep disruption, and capacity/forensic context when sexsomnia or violence is alleged.[2][5]
Risk domains. Self and partner injury; falls in older adults if clonazepam is considered; suicidal ideation linked to relentless nightmares; child safety if a parent has violent RBD or sleepwalking exits; forensic risk in sexsomnia.[4][14]
Investigations
- Classic childhood DOA without atypical features is often clinical — education and safety can start without delaying for a laboratory appointment.[2][8]
- Video-PSG when adult-onset atypical events, injury, suspected RBD, seizure differential, treatment resistance, or medicolegal weight require objective capture; score RSWA and correlate video with stage.[4][5]
- EEG strategy expands when nocturnal frontal lobe epilepsy remains plausible.
- OSA testing when pretest probability is moderate–high — treating OSA can reduce NREM events driven by respiratory arousals.[2]
- Neurodegeneration pathway for iRBD: neurological examination, cognitive screen, olfactory history, and neurology/sleep-medicine referral for longitudinal care — not a one-off hypnotic script.[6][15]
Acute and emergency management
- Do not forcibly shake or argue with a person mid-sleep-terror; guide gently to safety and allow the episode to settle.
- Stop alcohol near bedtime and stop or reduce Z-drugs when complex behaviours appear.
- Temporary separate rooms protect partners during violent RBD until treatment takes effect.[4][1]
Definitive management
NREM disorders of arousal
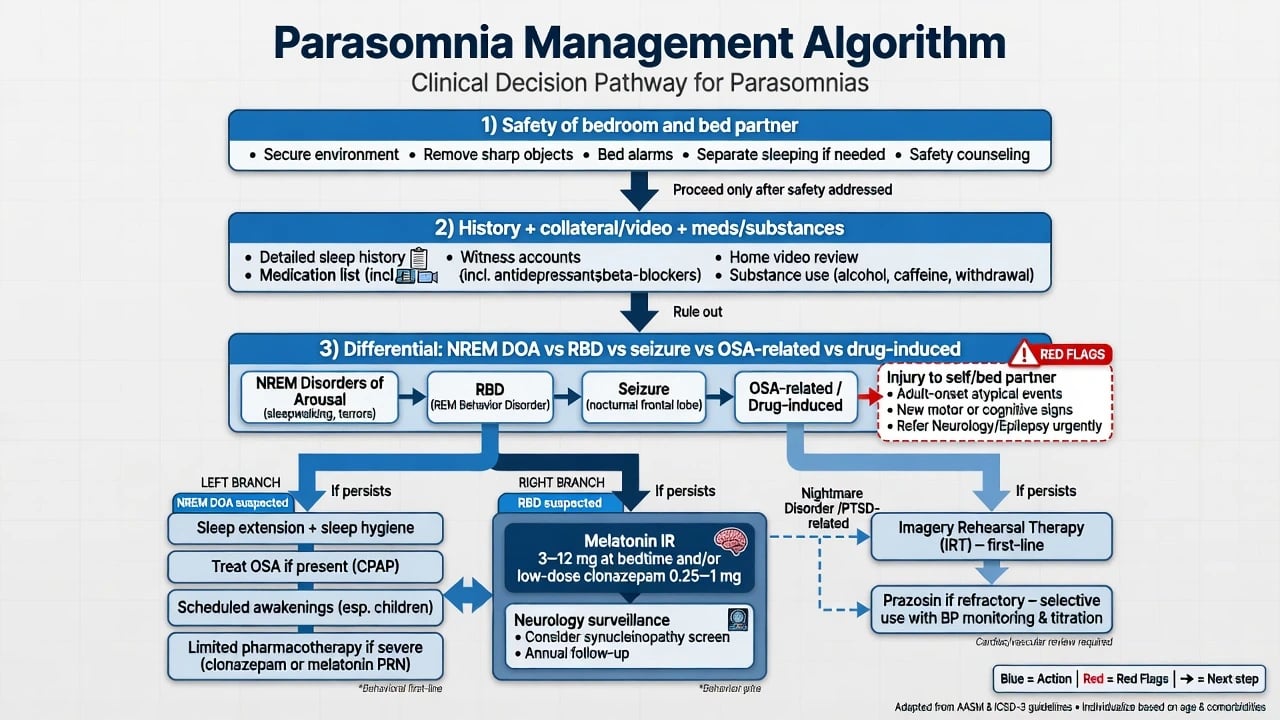
- Safety engineering of the sleep environment (ground-floor preference if exits are risky, window locks, clear floors, door alarms as needed).
- Protect sleep opportunity — reverse chronic sleep debt; regular schedule.
- Remove precipitants — alcohol, unnecessary sedative-hypnotics, untreated OSA, fever/illness when possible.
- Scheduled awakenings (especially children) timed before habitual episode windows.
- Pharmacotherapy only for frequent, injurious, or treatment-resistant adult cases after behavioural/safety measures — BAP consensus discusses specialist use of agents such as clonazepam in selected severe parasomnias, informed by long-term case-series experience with injurious events rather than large modern RCTs for every DOA subtype.[2][14][1]
REM sleep behaviour disorder
AASM guidance emphasises modifying the sleep environment as foundational care, with pharmacologic options including immediate-release melatonin and clonazepam in appropriate patients; the 2023 AASM clinical practice guideline updates management recommendations for adult RBD beyond the 2010 best-practice guide.[4][5]
Practical fellowship framing (check current product information, age, falls risk, respiratory disease, and interactions):
- Melatonin (immediate-release): commonly started in the low milligram range at bedtime and titrated against dream enactment and morning hangover; attractive when benzodiazepine risk is high (older adults, fall risk, cognitive vulnerability).[5][4]
- Clonazepam: often 0.25–0.5 mg oral at bedtime, titrated cautiously (many respond below 1–2 mg; higher historical ceilings appear in specialist series). Monitor falls, residual sedation, confusion, respiratory depression risk, and dependence; review need periodically.[4][14][5]
- Treat comorbid OSA; review antidepressants that may worsen dream enactment.
- Counsel that idiopathic RBD carries substantial long-term neurodegenerative risk and arrange serial neurological surveillance without catastrophic single-visit framing.[6][15]
Nightmare disorder and PTSD nightmares
AASM best-practice and position papers support image rehearsal therapy (IRT) and related cognitive approaches as preferred psychological treatments for nightmare disorder; progressive muscle relaxation and systematic desensitization have historical support for idiopathic nightmares.[10][9]
Prazosin (alpha-1 antagonist) improved trauma nightmares in earlier veteran RCTs, typically starting low (for example 1 mg oral at bedtime) and titrating against nightmare response and orthostatic blood pressure — but a large 2018 multicentre veteran trial did not show benefit over placebo for distressing dreams, so examiners expect nuanced, not automatic, prescribing and continued priority for trauma-focused and nightmare-specific psychotherapies.[11][12][9]
BAP (UK) 2010/2019: consensus spanning insomnia, parasomnias, and circadian disorders — safety, behavioural measures, selective pharmacology, specialist pathways.[1][2] AASM RBD: 2010 best-practice guide plus 2023 clinical practice guideline — environmental modification, melatonin, clonazepam, comorbidity management.[4][5] AASM nightmares: 2010 best practice and 2018 position paper — psychological therapies (IRT) central; prazosin discussed with evolving evidence.[10][9] ANZ practice: align with safety-first care, sleep physician referral for video-PSG/RBD, neurology for iRBD surveillance, and local formulary constraints on clonazepam; rural PSG delays should not block same-night bedroom safety.
Special populations and scenarios
- Children: parental education, safety, sleep extension, scheduled awakenings; avoid reflexive long-term benzodiazepines for developmental DOA that often remits.[2][8]
- Older adults: new dream enactment = RBD pathway until proven otherwise; falls risk dominates clonazepam decisions; prefer environmental safety and melatonin-first strategies when appropriate.[5][6]
- PTSD: combine trauma-focused care with IRT-type nightmare work; prazosin only with BP monitoring and explicit uncertainty after the large negative trial.[9][12]
- Antidepressant-associated enactment: review timing of onset, consider switch/dechallenge with mood risk balanced, and evaluate true RBD if behaviours persist.
- Intellectual disability / residential care: caregiver video, OSA under-detection, environmental hazards, and staff plans for nocturnal exits.
- Pregnancy: prioritise non-drug safety; specialist advice before any sedative.
Complications and pitfalls
- Labelling injurious RBD as “bad nightmares” without partner safety or neurodegeneration counselling.[6][7]
- Missing nocturnal seizures.
- Escalating Z-drugs into complex sleep behaviours.
- Ignoring OSA as a DOA precipitant.
- Forcing arousal mid-sleep-terror and escalating violence.
- Overconfident lifelong prazosin after mixed large-trial evidence without offering IRT.[12][9]
- Starting clonazepam without falls plan in an older adult.
Prognosis and disposition
Childhood NREM DOA often improves with age; adult DOA prognosis tracks trigger control and safety adherence.[8][13] Idiopathic RBD carries high cumulative conversion risk to synucleinopathy over long follow-up — disposition includes sleep-medicine/neurology shared care, not discharge after one script.[6][15] Safety-net for escalating violence, new motor/cognitive signs, OSA red flags, and treatment-related sedation.
Exam pearls
PARASOMNIA SAFE (assessment and plan)
References
- [1]Wilson SJ, Nutt DJ, Alford C, et al. British Association for Psychopharmacology consensus statement on evidence-based treatment of insomnia, parasomnias and circadian rhythm disorders J Psychopharmacol, 2010.PMID 20813762
- [2]Wilson S, Anderson K, Baldwin D, et al. British Association for Psychopharmacology consensus statement on evidence-based treatment of insomnia, parasomnias and circadian rhythm disorders: An update J Psychopharmacol, 2019.PMID 31271339
- [3]Sateia MJ International classification of sleep disorders-third edition: highlights and modifications Chest, 2014.PMID 25367475
- [4]Aurora RN, Zak RS, Maganti RK, et al. Best practice guide for the treatment of REM sleep behavior disorder (RBD) J Clin Sleep Med, 2010.PMID 20191945
- [5]Howell M, Avidan AY, Foldvary-Schaefer N, et al. Management of REM sleep behavior disorder: an American Academy of Sleep Medicine clinical practice guideline J Clin Sleep Med, 2023.PMID 36515157
- [6]Postuma RB, Iranzo A, Hu M, et al. Risk and predictors of dementia and parkinsonism in idiopathic REM sleep behaviour disorder: a multicentre study Brain, 2019.PMID 30789229
- [7]Schenck CH, Bundlie SR, Ettinger MG, et al. Chronic behavioral disorders of human REM sleep: a new category of parasomnia Sleep, 1986.PMID 3505730
- [8]Zadra A, Desautels A, Petit D, et al. Somnambulism: clinical aspects and pathophysiological hypotheses Lancet Neurol, 2013.PMID 23415568
- [9]Morgenthaler TI, Auerbach S, Casey KR, et al. Position paper for the treatment of nightmare disorder in adults: an American Academy of Sleep Medicine position paper J Clin Sleep Med, 2018.PMID 29852917
- [10]Aurora RN, Zak RS, Auerbach SH, et al. Best practice guide for the treatment of nightmare disorder in adults J Clin Sleep Med, 2010.PMID 20726290
- [11]Raskind MA, Peskind ER, Hoff DJ, et al. A parallel group placebo controlled study of prazosin for trauma nightmares and sleep disturbance in combat veterans with post-traumatic stress disorder Biol Psychiatry, 2007.PMID 17069768
- [12]Raskind MA, Peskind ER, Chow B, et al. Trial of Prazosin for Post-Traumatic Stress Disorder in Military Veterans N Engl J Med, 2018.PMID 29414272
- [13]Ohayon MM, Guilleminault C, Priest RG Night terrors, sleepwalking, and confusional arousals in the general population: their frequency and relationship to other sleep and mental disorders J Clin Psychiatry, 1999.PMID 10221293
- [14]Schenck CH, Mahowald MW Long-term, nightly benzodiazepine treatment of injurious parasomnias and other disorders of disrupted nocturnal sleep in 170 adults Am J Med, 1996.PMID 8629680
- [15]Galbiati A, Verga L, Giora E, et al. The risk of neurodegeneration in REM sleep behavior disorder: A systematic review and meta-analysis of longitudinal studies Sleep Med Rev, 2019.PMID 30503716
- [16]Castelnovo A, Lopez R, Proserpio P, et al. NREM sleep parasomnias as disorders of sleep-state dissociation Nat Rev Neurol, 2018.PMID 29959394