Psych · Specialty psychiatry — sleep medicine interface
Restless legs syndrome
Also known as RLS · Willis-Ekbom disease · Willis–Ekbom disease · Ekbom syndrome · Periodic limb movements of sleep · PLMS · Periodic limb movement disorder · PLMD · Dopamine agonist augmentation
Exam-exhaustive fellowship atlas on restless legs syndrome (Willis–Ekbom disease) for psychiatry — IRLSSG five criteria, primary vs secondary RLS, brain-iron and A11 dopaminergic mechanisms, PLMS/PLMD, akathisia differential, ferritin-led iron therapy, α2δ ligands versus dopamine agonists and augmentation, psychotropic aggravation, pregnancy/CKD/older adult pathways, and AASM/AAN/IRLSSG guideline deltas. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
RLS is a high-yield psychiatry–sleep interface leaf. FRANZCP MEQs test ferritin thresholds, augmentation, and antidepressant aggravation. MRCPsych CASCs test plain-language explanation and collaborative deprescribing of dopamine agonists. ABPN items test IRLSSG criteria, PLMS/PLMD, and first-line pharmacologic strategy. A candidate who reads only this page should defend diagnosis, organic work-up, and stepped care at consultant depth without relying on the broader sleep hub alone.[2][8][12]
Overview and definition
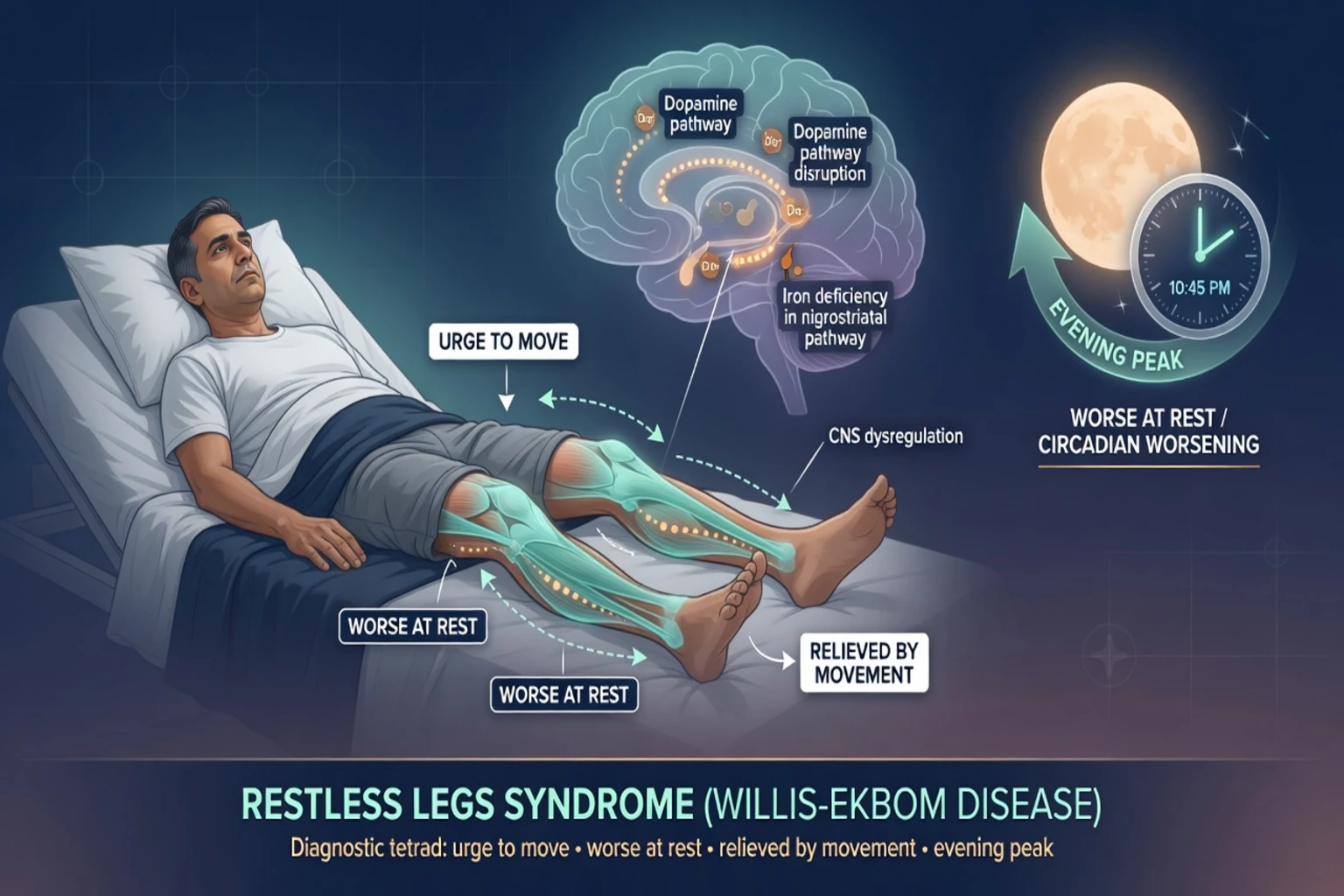
Restless legs syndrome (RLS), also called Willis–Ekbom disease, is defined by an urge to move the legs, usually with uncomfortable sensations, that begins or worsens at rest, is partially or totally relieved by movement while activity continues, is worse in the evening or night (or occurs only then), and is not solely accounted for by another medical or behavioural condition (cramps, positional discomfort, neuropathy, venous stasis, arthritis, myalgia, or akathisia-type mimics). All five elements are required in contemporary IRLSSG consensus criteria.[1]
Psychiatry essence. RLS is a common cause of sleep-onset insomnia and nocturnal agitation that is mislabelled as anxiety, “just insomnia,” or antipsychotic akathisia. Untreated RLS fragments sleep, amplifies depressive and anxiety symptoms, and invites chronic hypnotic or dopamine-agonist traps. Treating the mood disorder while ignoring iron deficiency and sensorimotor criteria is a classic fellowship fail.[2][9]
ICSD-3 placement. RLS sits among sleep-related movement disorders, alongside periodic limb movement disorder (PLMD), sleep-related leg cramps, bruxism, and rhythmic movement disorder. Psychiatrists must navigate this map even when the electronic record only codes the comorbid mental disorder.[12]
Classification and nosology
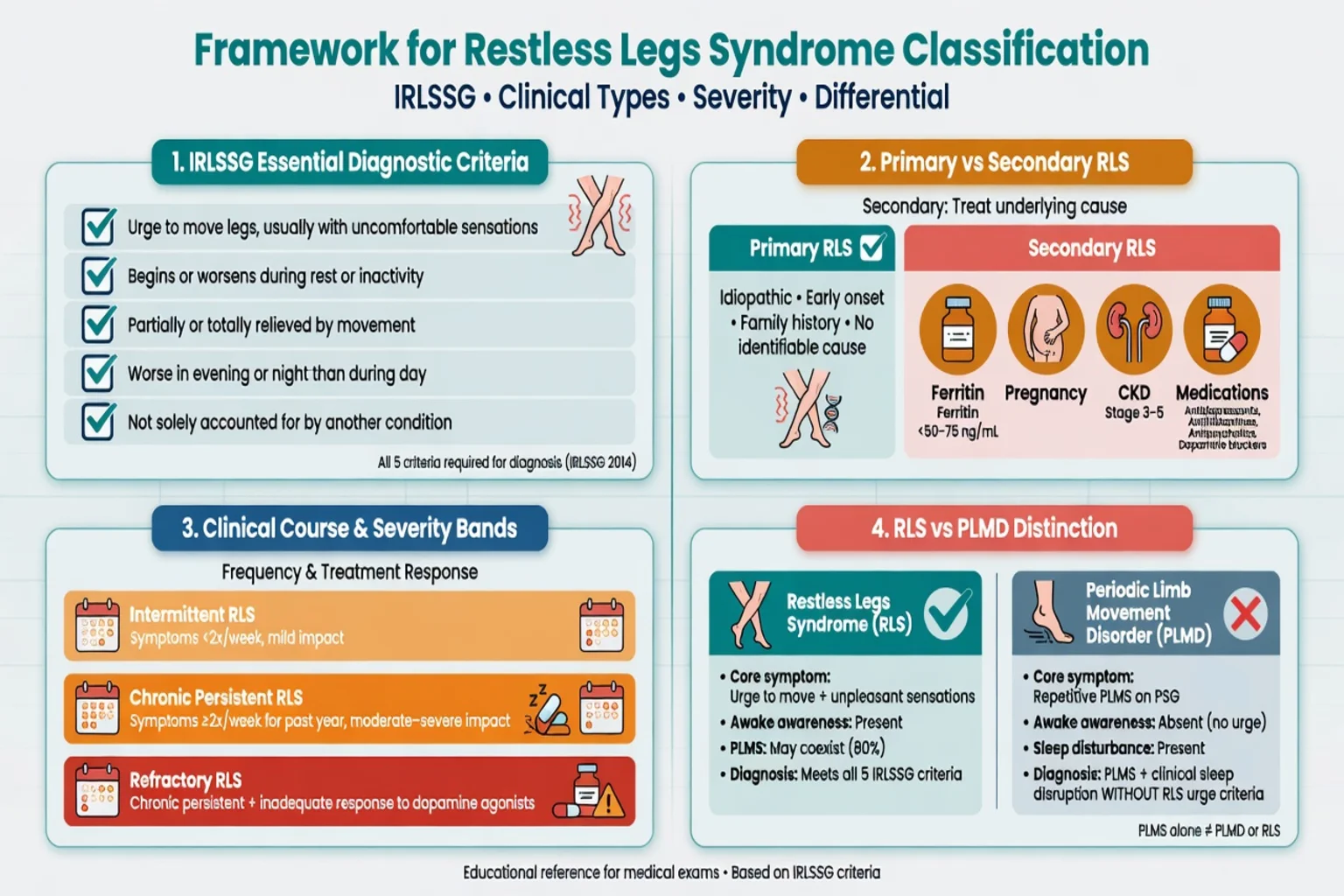
Primary (idiopathic) RLS
- Often early-onset, familial
- No single reversible driver
- Chronic fluctuating course
- Iron still relevant even if Hb normal
Secondary RLS
- Iron deficiency, pregnancy, CKD
- Medication-induced/aggravated
- Neuropathy, inflammatory disease
- Treat driver + RLS pathway
Severity bands
- Intermittent: occasional nights
- Chronic persistent: frequent distress
- Refractory: fails standard therapy
- Guides intensity of drug therapy
PLMS / PLMD
- PLMS: PSG movement index finding
- Common in RLS but not required
- PLMD: PLMS + sleep disturbance without RLS
- Do not equate PLMS with RLS diagnosis
Management algorithms often separate intermittent, chronic persistent, and refractory RLS because drug exposure risk (especially dopaminergic augmentation) scales with chronicity.[5][8]
Epidemiology and risk
Epidemiology anchors for exams
Population work shows RLS and PLMD are common and associate with physical and mental disorders; clinically significant disease (symptoms several nights weekly with distress) is less prevalent than casual “restless legs” self-report.[14][2] Women are over-represented in adult samples; prevalence generally rises across middle and older adulthood, with important secondary peaks in pregnancy and uraemia.[2][12]
Psychiatric interface. RLS and mood disorders are frequently comorbid; recognition matters because many insomnia and antidepressant pathways can worsen sensory symptoms if RLS is missed.[9][10]
Pathophysiology and mechanisms
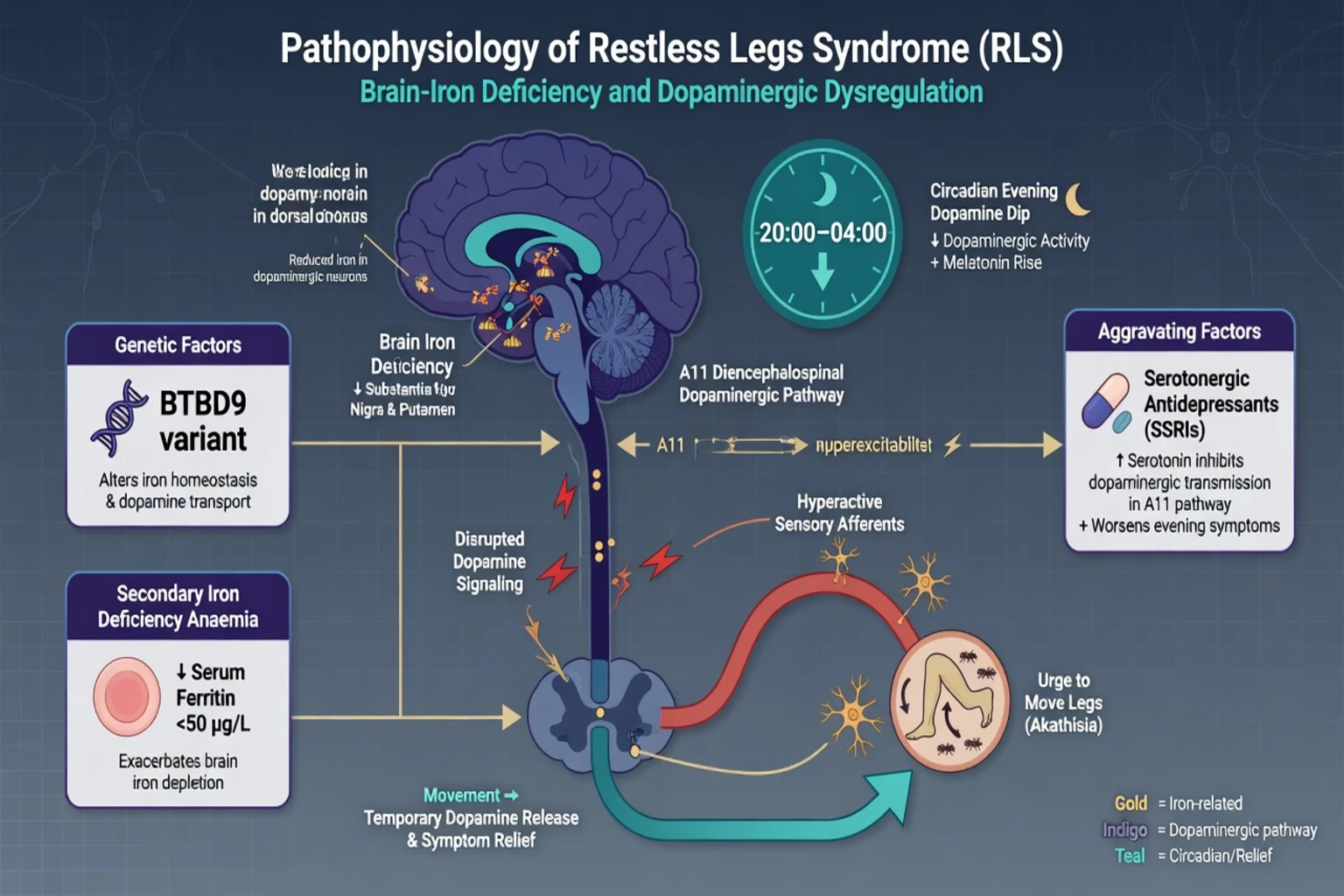
Contemporary synthesis emphasises regional brain-iron deficiency, altered dopaminergic signalling (including descending A11-related pathways), and strong circadian modulation with evening worsening. Genetics contribute in early-onset families; secondary iron deficiency, pregnancy, and uraemia provide reverse-translational clinical models.[2][12]
Why psychiatrists care about mechanisms. Serotonergic antidepressants can increase periodic limb movements and may unmask RLS symptoms; dopamine-blocking antipsychotics and antiemetics can worsen the phenotype or create akathisia that mimics it. Iron repletion can improve symptoms and is a disease-biology intervention, not a placebo gesture.[10][6][2]
Clinical presentation
History language examiners want. “Crawling,” “electric,” “pulling,” “ants under the skin,” irresistible urge to move, partial relief while walking or stretching that returns when still, and clear evening predominance. Sleep-onset latency rises; bed partners may report kicking (PLMS).[1][12]
Daytime phenotype. Fatigue, irritability, and cognitive fog from fragmentation are common; true hypersomnolence should still prompt OSA screening when risk factors coexist. Mood symptoms track sleep loss and the sensory distress itself.[9][2]
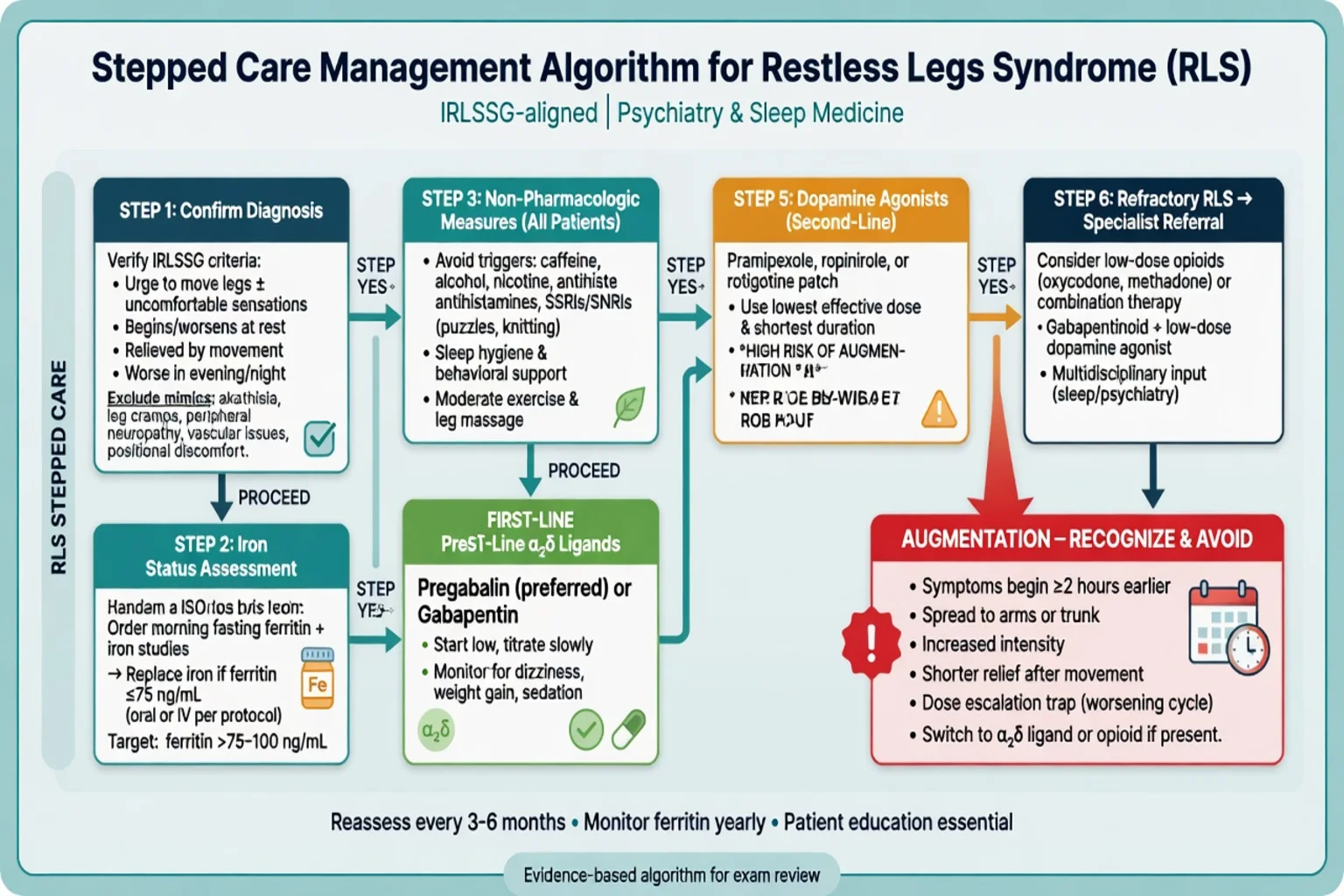
Augmentation (must recognise). After dopaminergic therapy, symptoms start earlier in the day, intensify, spread to arms or trunk, and show shorter rest latency — Max Planck/IRLSSG diagnostic standards formalise this construct. Escalating the dopamine agonist deepens the trap.[13][5]
Differential diagnosis
Discriminators beat lists — map the rest–relief circadian pattern against akathisia, cramps, neuropathy, and positional mimics before labelling pure psychiatric restlessness.[1][12]
| Presentation | Favours | Against pure RLS alone |
|---|---|---|
| Whole-day inner restlessness after antipsychotic, not relieved by walking, no evening peak | Akathisia | Classic circadian rest–relief pattern |
| Painful sustained calf contraction relieved by stretch | Nocturnal leg cramps | Continuous urge without true cramp |
| Stocking numbness/burning, not movement-relieved | Neuropathy | Clear rest-worsening and movement relief |
| Discomfort only in one position, resolves with repositioning | Positional discomfort | Persistent urge across positions at rest |
| Claudication with walking, relief at rest | Vascular disease | Opposite activity relationship to RLS |
| Night-time worry without urge-to-move phenomenology | Anxiety/insomnia | Meets all five IRLSSG criteria |
Always review substances and medications: antihistamines, dopamine antagonists, SSRIs/SNRIs, lithium, alcohol, and caffeine near bedtime.[8][10]
Assessment
Structure. Walk through all five criteria; explicitly exclude mimics; map circadian pattern, sleep schedule, substances, mood/anxiety/psychosis, suicide risk, occupational risk, and full medication list including OTC sedating antihistamines.[1][8]
Tools.
- IRLS (International RLS Study Group rating scale) for severity and response tracking.[11]
- Sleep diary for onset latency and night awakenings.
- Partner report for PLMS and snoring/apnoeas (OSA co-screen).
- MSE for akathisia signs, mood, and medication side effects.
Medication audit (exam gold). SSRIs and venlafaxine associate with increased PLMS in laboratory data; antipsychotic-related akathisia is the top differential when neuroleptics were recently started or increased.[10][9]
Investigations
- Morning fasting iron studies in essentially every clinically significant RLS case: ferritin, serum iron, TIBC/transferrin saturation. Do not wait for anaemia. AASM guidance emphasises regular iron study testing to guide oral versus IV iron decisions.[4][6]
- Ferritin teaching threshold. Consensus and guideline-linked practice commonly consider iron repletion when ferritin is approximately ≤75 ng/mL (or transferrin saturation under ~20%), with IV iron pathways considered at somewhat higher ferritin bands when oral iron is unsuitable — exact product selection is specialist/local formulary-guided.[4][6][7]
- Renal function (uraemic secondary RLS), glucose, and B12/folate when neuropathy or deficiency risk is present; pregnancy test when indicated.[2][12]
- PSG is not required for typical clinical RLS. Consider sleep testing for suspected OSA, unexplained hypersomnia, or PLMD without clear RLS phenotype.[12][8]
Acute and emergency management
- Impulse-control behaviours on dopamine agonists: stop or switch urgently; document collateral gambling/sexual/spending changes.[5][8]
- New post-antipsychotic restlessness: rate for akathisia first; do not automatically add another dopamine agonist for “RLS.”
- Pregnancy: non-drug and iron first; specialist liaison before off-label chronic dopaminergic therapy.[8][12]
Definitive management
Non-drug and trigger control
Mental alerting activities during sedentary evening periods, avoidance of alcohol and sedating antihistamines, caffeine moderation, and protection of sleep opportunity are foundational. Treat reversible drivers (iron deficiency, OSA if present, uraemia optimisation).[8][12]
Iron therapy
IRLSSG iron guidelines support oral and IV iron strategies based on iron studies and clinical severity; ferric carboxymaltose has RCT support in selected ferritin bands, and AASM 2025 elevates iron evaluation and selected IV iron recommendations for adults with appropriate iron status.[6][4] AAN guidance similarly supports considering ferrous sulfate with vitamin C when ferritin is approximately ≤75 μg/L.[7]
Illustrative adult oral iron framing (check current product information, GI tolerance, and interaction with other meds): ferrous sulfate oral commonly in standard deficiency doses (for example 65 mg elemental iron ranges depending on salt/formulation) with vitamin C to enhance absorption when used for RLS iron repletion pathways; monitor ferritin and stop if iron overload risk rises. IV iron is sleep/medicine-led when oral fails, absorption is poor, or ferritin band/severity warrants it.[6][7][4]
Pharmacotherapy for chronic persistent RLS
α2δ calcium-channel ligands (pregabalin, gabapentin, gabapentin enacarbil where available) are preferred first-line pharmacologic options for many patients because they are effective and carry little augmentation risk compared with dopamine agonists.[5][8][4]
Allen and colleagues showed that pregabalin 300 mg daily improved IRLS scores versus placebo and had significantly lower augmentation rates than pramipexole 0.5 mg over long follow-up in a large RCT — a landmark exam pearl driving the modern preference shift.[3]
Illustrative adult dosing frames (always individualise for renal function, age, and product information):
- Pregabalin oral often titrated toward the 150–300 mg/day evening-weighted range used in RLS trials; monitor dizziness, sedation, oedema, weight, and mood/SI signals.[3][4]
- Gabapentin oral evening-weighted titration commonly in hundreds of milligrams (for example starting 300 mg oral at night and titrating) with renal dose adjustment — local protocols govern maximums.[8][12]
- Pramipexole oral often starts at 0.125 mg at night and titrates cautiously (many patients remain at ≤0.5 mg); ropinirole oral often starts near 0.25 mg with slow titration; rotigotine transdermal patch offers continuous delivery when oral timing is problematic — all carry augmentation and impulse-control risk and are increasingly second-line for chronic therapy.[5][7][8]
- Avoid chronic levodopa as routine long-term monotherapy because of high augmentation risk.[5][8]
Refractory RLS. Combination therapy, careful opioid pathways (specialist protocols), and re-evaluation of iron, mimics, OSA, and medications — not endless DA dose escalation.[8][5]
Psychiatry-specific prescribing
- Prefer less RLS-provoking antidepressant choices when clinically feasible after risk–benefit discussion; bupropion is often discussed as relatively preferential for PLMS/RLS phenotypes compared with many SSRIs/SNRIs, though depression indication and seizure risk still govern choice.[10][9]
- Do not treat undiagnosed RLS with open-ended benzodiazepines or quetiapine as first-line “sleepers.”
- Document impulse-control screening when any dopamine agonist is used.[5]
AASM 2025: updated adult RLS/PLMD CPG with strong emphasis on iron evaluation and recommendations favouring agents such as pregabalin and selected IV iron formulations in appropriate patients.[4] AAN 2016: practice guideline summary supporting iron when ferritin low and multiple pharmacologic options with evidence grades.[7] IRLSSG: diagnostic criteria (2014), iron task force (2018), and augmentation prevention/treatment guidance (2016) preferring α2δ ligands to reduce long-term dopaminergic harm.[1][5][6] Silber 2021 Mayo algorithm: practical intermittent vs chronic persistent vs refractory pathways widely used in clinics.[8] ANZ practice: use local formulary/PBS constraints, sleep physician referral for refractory/complex cases, and start iron plus non-drug care during rural waitlists.
Subtypes and high-yield scenarios
High-yield stems include SSRI-associated night restlessness after “successful” depression treatment; clozapine/olanzapine clinics where akathisia versus RLS must be split; dialysis units with uraemic RLS; third-trimester pregnancy RLS; and ADHD youth with “growing pains” plus sleep-onset difficulty.[2][9][12]
Complications and pitfalls
Dopamine-agonist augmentation and impulse-control disorders, missing low-normal ferritin, calling akathisia RLS (or the reverse), chronic hypnotic dependence for undiagnosed RLS, and treating only mood while iron deficiency continues are classic examinable failures.[5][6][13][9]
Prognosis and disposition
Primary RLS often runs a chronic fluctuating course; secondary forms may improve when iron is restored, pregnancy ends, or renal disease is optimised (including post-transplant teaching points).[2][12] Shared care: psychiatry for mood, suicide risk, and psychotropic review; sleep medicine for refractory pharmacotherapy, IV iron logistics, and complex PSG phenotypes. Safety-net for SI, ICD behaviours, occupational impairment, and progressive augmentation.
Special populations
- Older adults: start low, go slow on α2δ ligands; fall risk with sedation; avoid high-dose dopamine agonists and polypharmacy sedatives.[8]
- Pregnancy/lactation: iron and non-drug first; specialist obstetric–sleep pathways; reassess post-partum.[8][12]
- Children/adolescents: iron status and behavioural measures; ADHD comorbidity common; avoid adult DA-first thinking.[6][12]
- CKD/dialysis: high secondary burden; coordinate with nephrology on timing, iron, and drug clearance.[2]
- ANZ remote care: check ferritin early; begin non-drug and α2δ pathways while awaiting sleep clinic when criteria are clear.
Exam pearls
REST LEGS (RLS clinic checklist)
Use this checklist whenever evening leg restlessness, sleep-onset insomnia, or new “restlessness” after antidepressants or antipsychotics appears in a stem.[9][10][4]
References
- [1]Allen RP, Picchietti DL, Garcia-Borreguero D, et al. Restless legs syndrome/Willis-Ekbom disease diagnostic criteria: updated International Restless Legs Syndrome Study Group (IRLSSG) consensus criteria--history, rationale, description, and significance Sleep Med, 2014.PMID 25023924
- [2]Trenkwalder C, Allen R, Högl B, et al. Comorbidities, treatment, and pathophysiology in restless legs syndrome Lancet Neurol, 2018.PMID 30244828
- [3]Allen RP, Chen C, Garcia-Borreguero D, et al. Comparison of pregabalin with pramipexole for restless legs syndrome N Engl J Med, 2014.PMID 24521108
- [4]Winkelman JW, Berkowski JA, DelRosso LM, et al. Treatment of restless legs syndrome and periodic limb movement disorder: an American Academy of Sleep Medicine clinical practice guideline J Clin Sleep Med, 2025.PMID 39324694
- [5]Garcia-Borreguero D, Silber MH, Winkelman JW, et al. Guidelines for the first-line treatment of restless legs syndrome/Willis-Ekbom disease, prevention and treatment of dopaminergic augmentation: a combined task force of the IRLSSG, EURLSSG, and the RLS-foundation Sleep Med, 2016.PMID 27448465
- [6]Allen RP, Picchietti DL, Auerbach M, et al. Evidence-based and consensus clinical practice guidelines for the iron treatment of restless legs syndrome/Willis-Ekbom disease in adults and children: an IRLSSG task force report Sleep Med, 2018.PMID 29425576
- [7]Winkelman JW, Armstrong MJ, Allen RP, et al. Practice guideline summary: Treatment of restless legs syndrome in adults: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology Neurology, 2016.PMID 27856776
- [8]Silber MH, Buchfuhrer MJ, Earley CJ, et al. The Management of Restless Legs Syndrome: An Updated Algorithm Mayo Clin Proc, 2021.PMID 34218864
- [9]Becker PM, Sharon D Mood disorders in restless legs syndrome (Willis-Ekbom disease) J Clin Psychiatry, 2014.PMID 25093484
- [10]Yang C, White DP, Winkelman JW Antidepressants and periodic leg movements of sleep Biol Psychiatry, 2005.PMID 16005440
- [11]Walters AS, LeBrocq C, Dhar A, et al. Validation of the International Restless Legs Syndrome Study Group rating scale for restless legs syndrome Sleep Med, 2003.PMID 14592342
- [12]Gossard TR, Trotti LM, Videnovic A, et al. Restless Legs Syndrome: Contemporary Diagnosis and Treatment Neurotherapeutics, 2021.PMID 33880737
- [13]García-Borreguero D, Allen RP, Kohnen R, et al. Diagnostic standards for dopaminergic augmentation of restless legs syndrome: report from a World Association of Sleep Medicine-International Restless Legs Syndrome Study Group consensus conference at the Max Planck Institute Sleep Med, 2007.PMID 17544323
- [14]Ohayon MM, Roth T Prevalence of restless legs syndrome and periodic limb movement disorder in the general population J Psychosom Res, 2002.PMID 12127170