Psych · Specialty psychiatry — sexual dysfunction and paraphilias
Sexual dysfunction and paraphilias
Also known as Erectile dysfunction · Premature ejaculation · Hypoactive sexual desire · Female sexual interest/arousal disorder · Genito-pelvic pain/penetration disorder · Paraphilic disorders · Pedophilic disorder · Exhibitionism · SSRI sexual side-effects · Compulsive sexual behaviour disorder
Exam-exhaustive fellowship reference on sexual dysfunction across desire, arousal, orgasm and pain phases; medication-induced sexual side-effects; assessment and stepped management; and paraphilic disorders carefully distinguished from non-pathological sexual diversity, with risk, child protection, and WFSBP-aligned pharmacological framing. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
6 MCQs with explanations
Target exams
Red flags
Sexual function and paraphilic presentations are high-yield specialty topics where examiners test clinical precision without moralising. FRANZCP MEQs and MRCPsych theory/CASC stations expect phase-based diagnosis, medication side-effect literacy, non-stigmatising sexual history skills, and a clean separation between atypical interest and disorder/risk. A candidate who reads only this topic should defend classification, assessment, medical–psychiatric differentials, stepped management, and forensic-risk framing at consultant depth.[15][16]
Overview and definition
Sexual dysfunction means a clinically significant disturbance in a person’s ability to respond sexually or to experience sexual pleasure, organised in modern manuals primarily by phase (desire, arousal, orgasm, pain) and by whether symptoms are lifelong or acquired, generalised or situational, and accompanied by marked distress. Frequency alone is not a diagnosis; distress or interpersonal difficulty is required in DSM-5-TR-style criteria for most categories.[2][15]
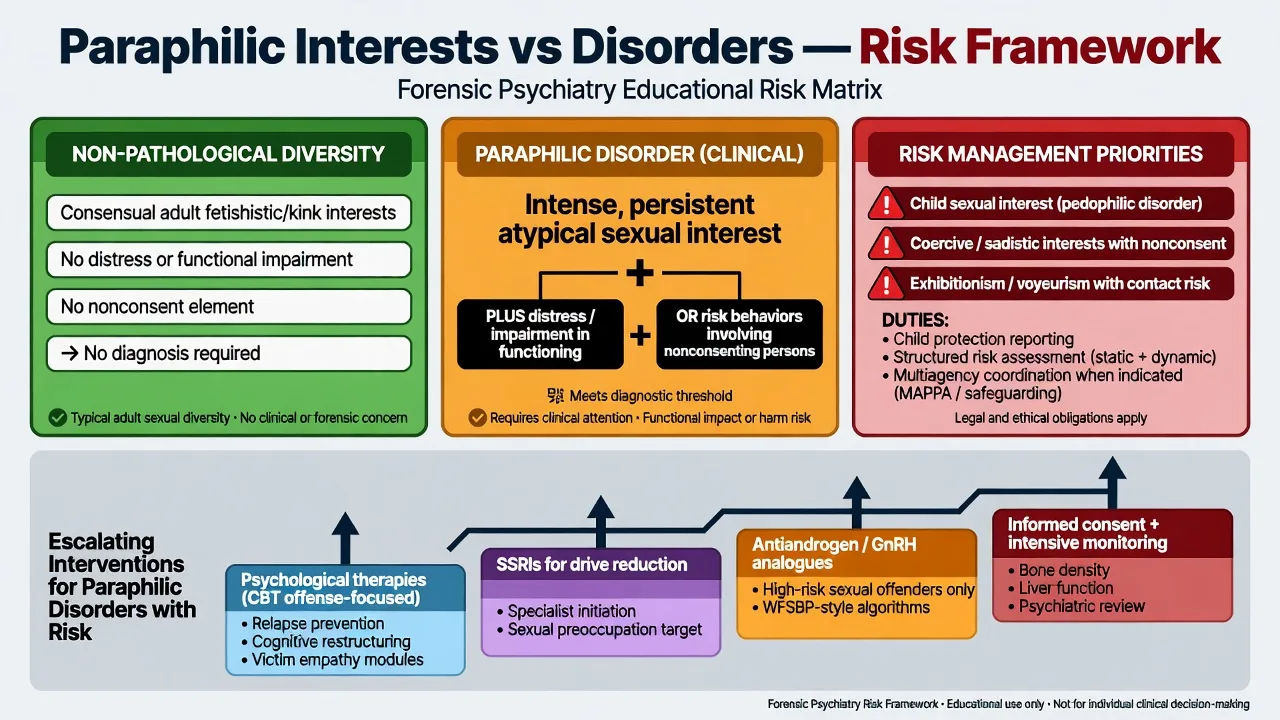
Paraphilia denotes an intense and persistent atypical sexual interest. A paraphilic disorder is diagnosed only when the interest causes marked distress or impairment in the person, or when satisfaction of the interest has entailed personal harm or risk of harm to others (classically nonconsenting persons). Consensual adult fetishistic or kink practices without distress or nonconsent are not disorders and must not be pathologised in exams or clinics.[15][16]
Classification
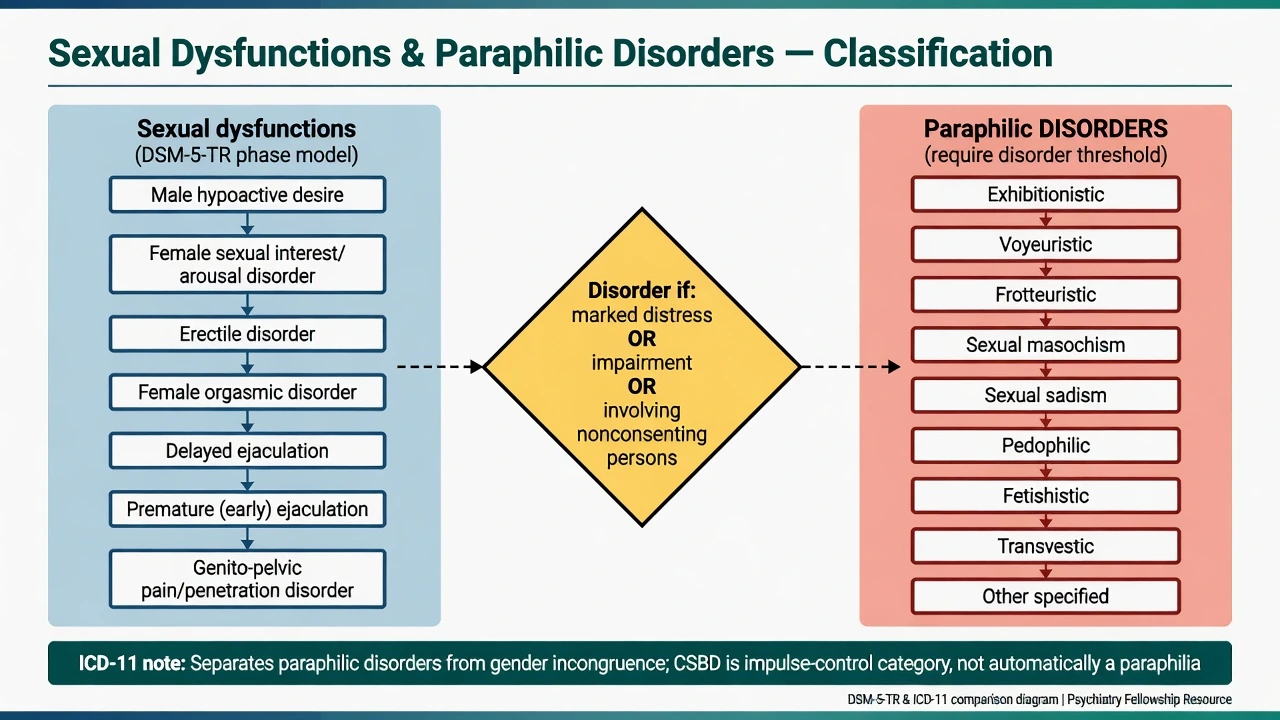
Sexual dysfunctions (DSM-5-TR structure to teach)
| Domain | Core exam entities |
|---|---|
| Desire | Male hypoactive sexual desire disorder; female sexual interest/arousal disorder (merged interest + arousal in DSM-5-TR) |
| Arousal / erectile | Erectile disorder |
| Orgasm / ejaculation | Female orgasmic disorder; delayed ejaculation; premature (early) ejaculation |
| Pain | Genito-pelvic pain/penetration disorder |
| Secondary | Substance/medication-induced sexual dysfunction; other specified / unspecified |
| Phase-based DSM-5-TR teaching groups desire, arousal/erectile, orgasm/ejaculation, pain, and substance/medication-induced sexual dysfunction as the core exam map.[2][15] |
Many DSM-5-TR sexual dysfunction criteria require symptoms for about 6 months and clinically significant distress; always state lifelong vs acquired and generalised vs situational when answering stems.[2][11]
Premature (early) ejaculation. ISSM guidance emphasises short ejaculatory latency (classically about 1 minute from vaginal penetration for lifelong PE teaching, with broader framing for acquired PE), inability to delay ejaculation, and negative personal consequences. DSM-5 and ICD-11 wording are not identical — name the manual and avoid inventing exact cut-points from memory when the stem does not require them.[10][11]
Paraphilic disorders
Commonly examined DSM-5-TR categories: voyeuristic, exhibitionistic, frotteuristic, sexual masochism, sexual sadism, pedophilic, fetishistic, transvestic, plus other specified/unspecified. ICD-11 retains a harm/consent/distress-informed approach to paraphilic disorders and deliberately separates gender incongruence from sexual dysfunction and paraphilia nosology.[15][16]
ICD-11 compulsive sexual behaviour disorder (CSBD) sits with impulse-control disorders: a persistent failure to control intense sexual impulses/urges resulting in repetitive behaviour with marked distress or impairment — not automatically a paraphilia. DSM-5 did not adopt Kafka’s proposed hypersexual disorder as an official category; do not treat “sex addiction” as a free-standing DSM diagnosis in exam answers without stating the nosological debate.[15][16]
Sexual dysfunction
- Phase problem (desire/arousal/orgasm/pain)
- Distress or impairment required
- Often medical, relational, or iatrogenic
- Treatment aims restore function/satisfaction
Paraphilic interest
- Atypical focus of arousal
- May be lifelong and ego-syntonic
- Consensual adult practice ≠ disorder
- No diagnosis solely for diversity
Paraphilic disorder
- Interest + distress/impairment
- OR acts/risk involving nonconsent
- Risk assessment is core
- Therapy ± specialist pharmacology
CSBD (ICD-11)
- Impulse-control framing
- Repetitive sexual behaviour despite harm
- Not defined by atypical target
- Comorbidity-heavy formulation
Epidemiology and risk factors
Exam-order epidemiology (order-of-magnitude teaching)
Laumann and colleagues documented substantial prevalence of sexual dysfunction symptoms in a US national sample with strong associations with health and emotional problems.[1] International consultation consensus statements summarise incidence/prevalence patterns and risk factors across women and men, emphasising age, cardiovascular and metabolic disease, psychiatric comorbidity, relationship factors, and medications.[2][3]
Iatrogenic burden. Prospective clinic data show high incidence of sexual dysfunction across antidepressant classes, with meaningful differences among agents; meta-analytic work ranks treatment-emergent sexual dysfunction rates and supports agent selection as a clinical lever.[6][7][8]
Pathophysiology
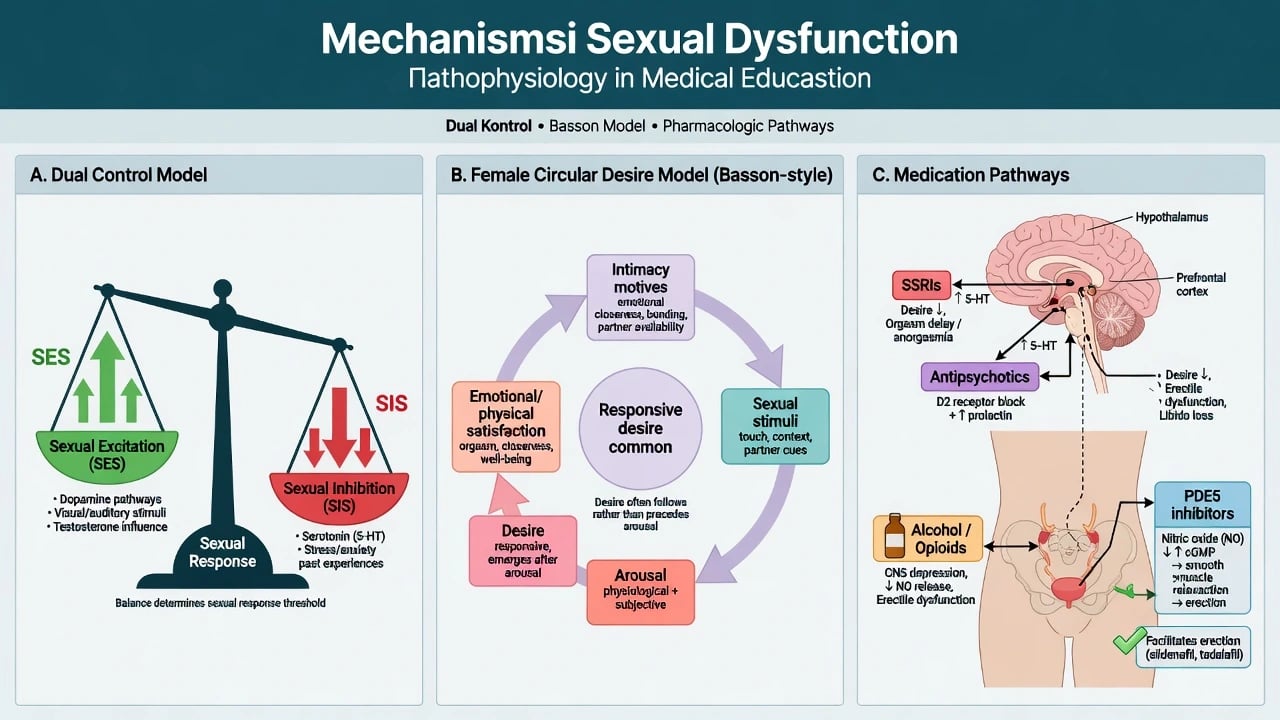
Dual control model. Sexual response reflects a balance between sexual excitation and sexual inhibition systems; high inhibition or low excitation (from mood, threat, medication, relationship context) predicts dysfunction without requiring a single “hormone defect.”[5]
Basson circular model. Many women (and some men) experience responsive desire emerging after intimacy motives and arousal rather than spontaneous desire initiating every encounter — a key antidote to pathologising non-linear desire patterns when distress is absent.[4]
Erectile physiology and PDE5 inhibitors. Nitric oxide–cGMP signalling mediates penile smooth-muscle relaxation; PDE5 inhibitors potentiate this pathway and transformed ED care after landmark randomised evidence for oral sildenafil.[9]
Psychopharmacology of sexual side-effects. Enhanced serotonergic tone (SSRIs/SNRIs) commonly reduces desire and delays or blocks orgasm; dopaminergic tone and normalised prolactin support desire/arousal; D2-blocking, prolactin-elevating antipsychotics are frequent culprits for reduced desire, erectile problems, and menstrual disturbance.[6][8][14]
Sexual offending framework (viva). Seto’s motivation–facilitation model separates motivations (e.g. atypical sexual interest, high sex drive, excessive mating effort) from facilitators (e.g. self-regulation problems, hostile attitudes, situational opportunity, substance use). Pedophilic interest is neither necessary nor sufficient for every child sexual offence — and not every person with pedophilic interest offends.[19]
Clinical presentation
Desire. Reduced sexual thoughts/fantasies and unreceptive response to partners, with distress. Always map secondary causes: depression, relationship rupture, trauma triggers, menopausal change, opioids, SSRIs.[3][8]
Arousal / erectile. Difficulty obtaining or maintaining erection sufficient for satisfactory sexual activity; morning erections and masturbation function help discriminate situational psychogenic patterns from more global organic disease (not absolute rules).[2][9]
Orgasm / ejaculation. Delayed/absent orgasm (especially SSRI-related); PE with short latency, inability to delay, and avoidance/distress.[10][11]
Pain. Fear of penetration, pelvic floor hypertonicity, dyspareunia, post-trauma avoidance — often needs gynaecology/physiotherapy interface plus psychosexual care.[2][3]
Paraphilic presentations. Ego-dystonic interests sought voluntarily; partner conflict; forensic referral after exhibitionism, voyeurism, frotteurism, possession of child exploitation material, or contact offences. MSE documents insight, shame, minimisation, planning, access to victims, and comorbid personality/substance pathology without humiliation.[16][19]
Differential diagnosis
| Presentation | Prefer | Discriminators |
|---|---|---|
| Low desire + melancholia | Depression-related | Anhedonia global; improves with mood |
| Low desire after SSRI start | Medication-induced | Timeline; other serotonergic SE |
| ED + diabetes/CVD | Organic ± mixed | Risk factors; nocturnal erections reduced |
| Lifelong short IELT | Lifelong PE | Consistent pattern from early encounters |
| High porn use + distress | CSBD vs habit vs anxiety | Loss of control, impairment, not atypical target alone |
| Kink, consenting adults | Not a disorder | No distress/nonconsent |
| Gender incongruence | Not paraphilia/SD | Identity/gender path, not phase dysfunction |
| Sexual contact with child | Offence + risk path | May or may not meet pedophilic disorder |
| Use the table as a discriminator map: secondary psychiatric and medication causes, organic ED risk, PE latency patterns, CSBD vs high desire, non-pathological kink, gender incongruence, and offence pathways that may or may not equal pedophilic disorder.[3][8][15][16] |
Gender incongruence is not a sexual dysfunction and not a paraphilia; ICD-11 relocation away from mental-disorder chapters reflects this human-rights and scientific shift while care pathways remain clinically important.[15]
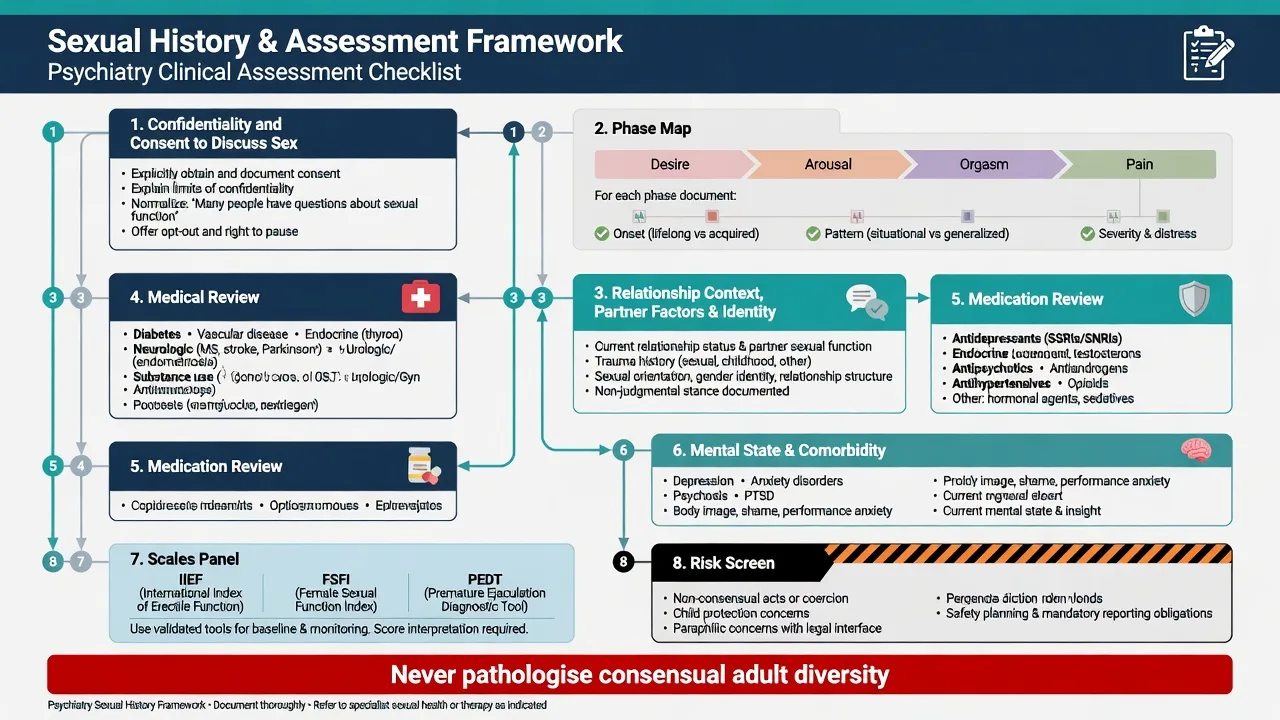
Clinical and bedside assessment
Permission and structure. Normalise the topic; ask open then specific questions; map phase, onset, context, distress, partner factors, trauma, orientation/identity without imposing values. Document language carefully for notes that may later appear in legal settings.[2][3]
Medication timeline. Antidepressants, antipsychotics, mood stabilisers, antiandrogens, antihypertensives, 5-alpha-reductase inhibitors, opioids, and recreational substances — onset relative to symptoms is the highest-yield diagnostic clue for iatrogenic dysfunction.[6][8][14]
Scales (conceptual). International Index of Erectile Function (IIEF) for ED severity/response tracking; female sexual function indices in specialist settings; PE tools and stopwatch/IELT concepts per ISSM teaching. Use depression/anxiety screens routinely because mood disorders both cause and result from sexual problems.[8][10]
Risk and confidentiality. When paraphilic or offence-related material emerges: clarify current access to children or potential victims, prior behaviours, escalation, substance use, antisocial attitudes, and treatability. Confidentiality has limits — mandatory reporting and public protection duties are jurisdiction-specific; state the principle and name local statutes rather than inventing foreign section numbers.[18][19]
Investigations
Sexual dysfunction. Cardiovascular risk assessment for ED; glucose/HbA1c, lipids; morning testosterone if hypogonadal signs/symptoms; prolactin when antipsychotic-related sexual dysfunction, galactorrhoea, or menstrual disruption is present; TFTs and other tests as indicated. Avoid shotgun panels for clearly situational, recent-onset psychogenic presentations, but do not miss diabetes/CVD windows.[3][9][14]
Paraphilic/forensic. Laboratory tests guide medical fitness for antiandrogen/GnRH pathways (baseline bloods, metabolic and bone health planning) rather than “diagnosing” paraphilia. Specialised phallometric or viewing-time measures belong in expert forensic settings, not routine general adult clinics.[17][18]
Management — acute risk
Medical emergencies. Priapism after ED treatments needs urgent urology. Cardiovascular red flags before PDE5 therapy (and absolute avoidance with nitrates) are safety-critical teaching points.[9]
Management — definitive sexual dysfunction
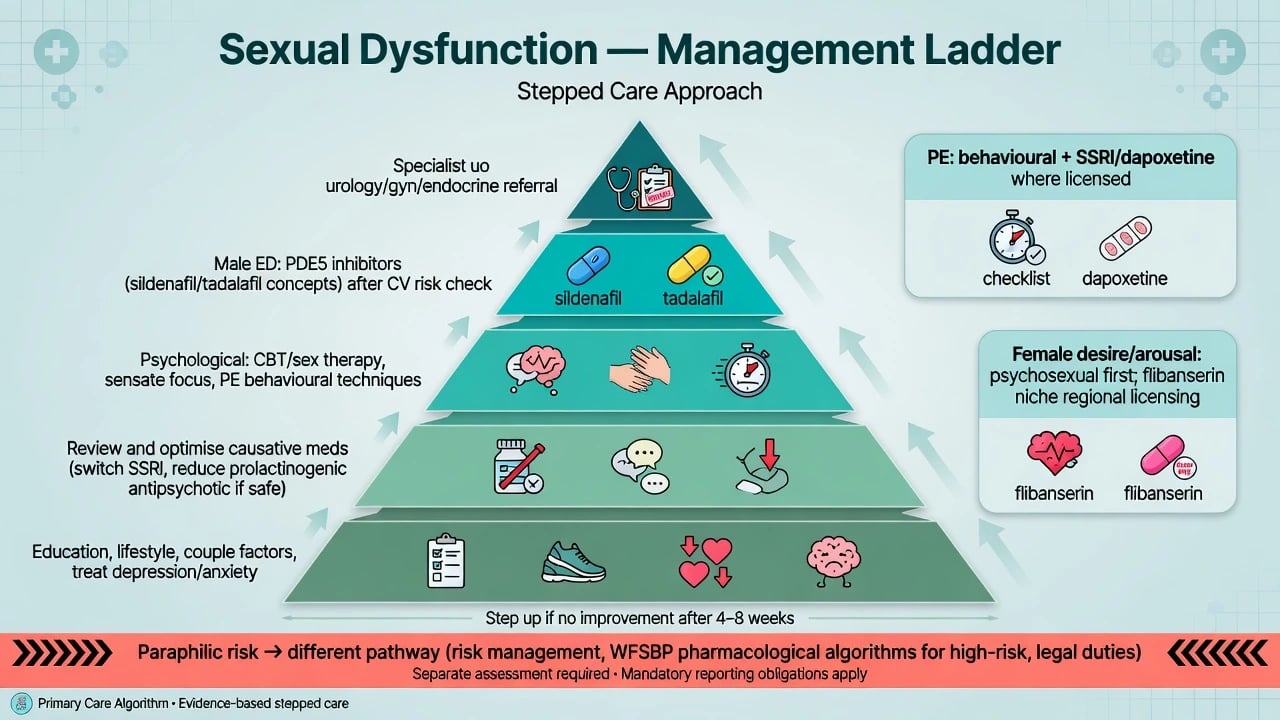
Stepped psychological and lifestyle care
- Psychoeducation (normal variation, responsive desire, dual control).
- Lifestyle: alcohol reduction, smoking cessation, exercise, sleep, weight management where relevant.
- Treat depression, anxiety, PTSD, psychosis — sexual recovery often follows psychiatric improvement if medications are not the ongoing cause.
- Psychosexual therapy / CBT / couple therapy; sensate focus; PE behavioural methods (stop–start, squeeze) with partner collaboration when appropriate.[4][5][10]
Optimising causative psychotropics
Antidepressant-induced sexual dysfunction. Strategies: assess adherence impact; allow adaptation if mild and depression still settling; dose adjustment; switch to relatively lower-risk agents (commonly discussed options include bupropion, mirtazapine, and some multimodal agents — formulary and indication-dependent); adjunctive approaches in specialist hands. Bupropion has trial signals for desire problems in selected populations and is relatively sexually sparing versus SSRIs, with seizure-risk cautions in eating disorders and other contraindications.[6][7][8][12]
Antipsychotic-related sexual dysfunction. Clinical approach: confirm prolactin contribution when relevant; consider switch to more prolactin-sparing antipsychotic if psychosis control allows; address metabolic health; avoid abandoning antipsychotic efficacy for cosmetic sexual goals without shared decision and relapse planning.[14]
Targeted pharmacotherapy
Erectile disorder. Oral PDE5 inhibitors (sildenafil, tadalafil, and related agents) after cardiovascular suitability assessment. Landmark RCT evidence established oral sildenafil efficacy versus placebo. Absolute exam trap: concurrent nitrate therapy is contraindicated. Counsel on timing, food/alcohol effects, and priapism rarity but urgency.[9]
Premature ejaculation. ISSM-aligned care combines behavioural methods with pharmacotherapy options (daily SSRI strategies, on-demand agents where licensed such as dapoxetine in some regions). Regional licensing and PBS/formulary access vary — state principles and local availability.[10][11]
Female desire. First-line remains psychosexual and contextual (relationship, mood, pain, medications). Flibanserin (multifunctional serotonin modulator) is a niche, regionally licensed option for premenopausal HSDD with important alcohol interaction and hypotension warnings — not a universal first-line outside licensed pathways.[12][13]
Management — paraphilic disorders and risk
Principles
- Do not diagnose for consensual adult atypical interests without distress/impairment.
- Risk first when children or nonconsenting adults are involved.
- Psychological treatments (offence-focused CBT, relapse prevention, addressing dynamic risk factors) are foundational.
- Pharmacological drive reduction is for selected high-risk or highly distressing disorders within specialist frameworks — not a moral punishment and not first-line for low-risk ego-dystonic fetishistic disorder.[16][17][18]
Pharmacological options (WFSBP-aligned teaching)
WFSBP guidelines for biological treatment of paraphilias and the 2020 pharmacological update outline stepped intensity: SSRIs (and related serotonergic strategies) for some patients with high sexual drive, compulsivity, or comorbid OCD/depression; steroidal antiandrogens; and GnRH analogues for severe, high-risk presentations, always with informed consent, medical monitoring, and legal–ethical clarity. Exact agent choice, dosing, and monitoring schedules belong to specialist protocols — exams test indications, hierarchy, monitoring domains, and ethics, not cookbook prescribing outside supervision.[17][18][20]
Monitoring domains to name at viva: sexual drive and behaviour logs, mood/suicidality, metabolic status, liver function where relevant, bone mineral density with prolonged androgen suppression, cardiovascular risk, and thromboembolic considerations depending on agent. Adolescents require separate caution and distinct guidance pathways.[17][18]
Forensic risk tools (concept level)
Actuarial tools such as Static-99R (with age weighting refinements) inform sexual recidivism risk estimation in convicted adult male sexual offenders in forensic services. They do not diagnose paraphilia and are not a substitute for structured clinical judgement, dynamic risk management, or child-protection action in acute community psychiatry.[19]
Special populations
Adolescents. Developmental sexual behaviour, online contexts, and caution before lifelong adult paraphilic labels; child protection remains paramount when peer or age-discordant harm is present.[18]
Older adults. Vascular ED, polypharmacy, bereavement, and ageist assumptions that older adults are “not sexual” — prevalence and medical risk rise with age and comorbidity.[1][2][3]
Intellectual disability. Capacity for sexual consent is decision-specific; protect from abuse; avoid pathologising all sexual expression while maintaining safeguarding.[15][18]
Cultural and religious contexts. Elicit values; do not impose clinician sexual norms; still apply universal child-protection duties.[15]
Regional notes
Mandatory reporting and public protection frameworks are jurisdiction-specific (Australian state/territory legislation; NZ counterparts). PDE5 inhibitors are widely used; dapoxetine and flibanserin availability/licensing differ from US pathways — check local formulary. Forensic sexual-offender treatment is specialised; general adult psychiatrists manage sexual side-effects, basic risk triage, and referral.[18]
Classic PE/ED pharmacotherapy and SSRI sexual side-effects remain high-yield. Forensic questions on paraphilias and risk emphasise principles over foreign statute numbers. WFSBP pharmacological algorithms provide international specialist framing.[17][18]
Prognosis and disposition
Many sexual dysfunctions improve substantially when medical contributors, mood disorders, relationships, and iatrogenic drugs are addressed, with or without PDE5/PE-specific therapy.[2][9][10] Paraphilic interests may persist; clinical goals are often risk reduction, prevention of harm, reduced distress, and improved psychosocial function rather than eradication of all atypical arousal. Disposition ranges from outpatient psychosexual care to forensic community teams and, rarely, secure settings based on risk — not on moral disapproval of interests alone.[18][19]
Exam pearls
SEX-SAFE assessment prompt
Fellowship stems reward calm, precise language: treat sexual problems as clinical phenomena, protect the vulnerable without pathologising diversity, and prescribe only within evidence and legal–ethical bounds.[15][16][18]
References
- [1]Laumann EO, Paik A, Rosen RC Sexual dysfunction in the United States: prevalence and predictors JAMA, 1999.PMID 10022110
- [2]McCabe MP, Sharlip ID, Lewis R, et al. Incidence and Prevalence of Sexual Dysfunction in Women and Men: A Consensus Statement from the Fourth International Consultation on Sexual Medicine 2015 J Sex Med, 2016.PMID 26953829
- [3]McCabe MP, Sharlip ID, Lewis R, et al. Risk Factors for Sexual Dysfunction Among Women and Men: A Consensus Statement From the Fourth International Consultation on Sexual Medicine 2015 J Sex Med, 2016.PMID 26953830
- [4]Basson R The female sexual response: a different model J Sex Marital Ther, 2000.PMID 10693116
- [5]Bancroft J, Graham CA, Janssen E, Sanders SA The dual control model: current status and future directions J Sex Res, 2009.PMID 19308839
- [6]Montejo AL, Llorca G, Izquierdo JA, Rico-Villademoros F Incidence of sexual dysfunction associated with antidepressant agents: a prospective multicenter study of 1022 outpatients J Clin Psychiatry, 2001.PMID 11229449
- [7]Serretti A, Chiesa A Treatment-emergent sexual dysfunction related to antidepressants: a meta-analysis J Clin Psychopharmacol, 2009.PMID 19440080
- [8]Clayton AH, El Haddad S, Iluonakhamhe JP, et al. Sexual dysfunction associated with major depressive disorder and antidepressant treatment Expert Opin Drug Saf, 2014.PMID 25148932
- [9]Goldstein I, Lue TF, Padma-Nathan H, et al. Oral sildenafil in the treatment of erectile dysfunction. Sildenafil Study Group N Engl J Med, 1998.PMID 9580646
- [10]Althof SE, McMahon CG, Waldinger MD, et al. An update of the International Society of Sexual Medicine's guidelines for the diagnosis and treatment of premature ejaculation (PE) J Sex Med, 2014.PMID 24848686
- [11]Waldinger MD, Schweitzer DH Differences between ICD-11 MMS and DSM-5 definition of premature ejaculation: a continuation of historical inadequacies and a source of serious misinterpretations by some scientists Int J Impot Res, 2019.PMID 30659291
- [12]Segraves RT, Clayton A, Croft H, et al. Bupropion sustained release for the treatment of hypoactive sexual desire disorder in premenopausal women J Clin Psychopharmacol, 2004.PMID 15118489
- [13]Stahl SM Mechanism of action of flibanserin, a multifunctional serotonin agonist and antagonist (MSAA), in hypoactive sexual desire disorder CNS Spectr, 2015.PMID 25659981
- [14]Montejo AL, de Alarcón R, Prieto N, et al. Management Strategies for Antipsychotic-Related Sexual Dysfunction: A Clinical Approach J Clin Med, 2021.PMID 33467621
- [15]Reed GM, Drescher J, Krueger RB, et al. Disorders related to sexuality and gender identity in the ICD-11: revising the ICD-10 classification based on current scientific evidence, best clinical practices, and human rights considerations World Psychiatry, 2016.PMID 27717275
- [16]Krueger RB, Reed GM, First MB, et al. Proposals for Paraphilic Disorders in the International Classification of Diseases and Related Health Problems, Eleventh Revision (ICD-11) Arch Sex Behav, 2017.PMID 28210933
- [17]Thibaut F, De La Barra F, Gordon H, et al. The World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for the biological treatment of paraphilias World J Biol Psychiatry, 2010.PMID 20459370
- [18]Thibaut F, Cosyns P, Fedoroff JP, et al. The World Federation of Societies of Biological Psychiatry (WFSBP) 2020 guidelines for the pharmacological treatment of paraphilic disorders World J Biol Psychiatry, 2020.PMID 32452729
- [19]Seto MC The Motivation-Facilitation Model of Sexual Offending Sex Abuse, 2019.PMID 28715948
- [20]Assumpção AA, Garcia FD, Garcia HD, et al. Pharmacologic treatment of paraphilias Psychiatr Clin North Am, 2014.PMID 24877704