Psych · Specialty psychiatry — sleep medicine interface
Sleep disorders in psychiatry
Also known as Insomnia disorder · CBT-I · Cognitive behavioural therapy for insomnia · Obstructive sleep apnoea · OSA · Hypersomnia · Narcolepsy · Circadian rhythm sleep-wake disorder · Restless legs syndrome · Hypnotics · Z-drugs · Parasomnia
Exam-exhaustive fellowship reference on sleep disorders at the psychiatry interface — DSM-5-TR/ICSD-3 insomnia and hypersomnia nosology, OSA screening and CPAP framing, circadian and parasomnia boundaries, CBT-I first-line evidence, hypnotic risk/benefit and deprescribing, psychotropic effects on sleep, and suicide-risk implications. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
12 MCQs with explanations
Target exams
Red flags
Sleep is a core vital sign of mental health. FRANZCP MEQs test CBT-I components, hypnotic deprescribing, and the insomnia–suicide link. MRCPsych CASCs test explanation of CBT-I and CPAP negotiation. ABPN items test DSM/ICSD nosology, OSA clues, and psychotropic sleep effects. A candidate who reads only this topic should defend assessment, organic exclusion, and stepped care at consultant depth.[6][16][19]
Overview and definition
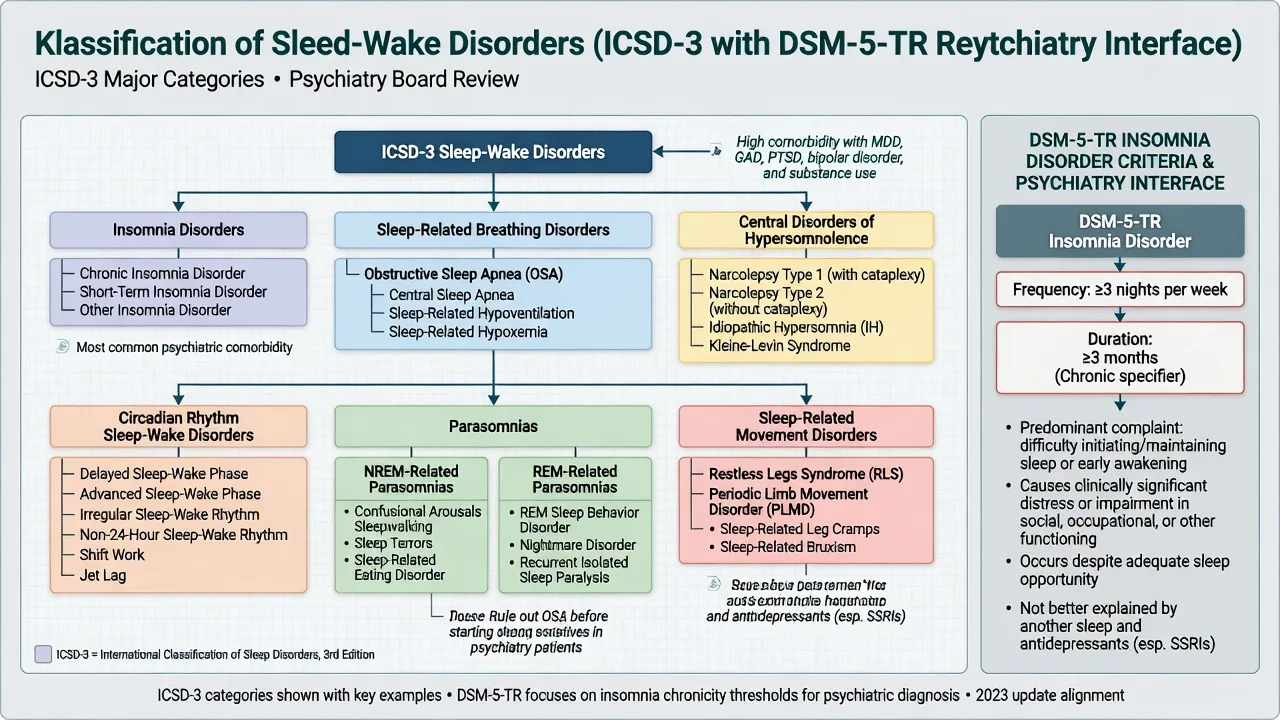
Insomnia disorder (DSM-5-TR) is a predominant complaint of dissatisfaction with sleep quantity or quality, with difficulty initiating sleep, maintaining sleep, or early-morning awakening with inability to return to sleep, plus daytime distress or impairment, occurring despite adequate opportunity for sleep, and not better explained by another sleep–wake, mental, medical, or substance disorder when those fully account for the presentation. Chronic course is typically framed as symptoms on at least 3 nights per week for at least 3 months.[19][20]
Clinical essence for viva. Insomnia is both a symptom of mood, anxiety, trauma, psychosis, and substance disorders and an independent disorder that maintains and predicts psychopathology. Treating only the parent diagnosis and ignoring sleep perpetuates residual symptoms and suicide risk. Treating only with nightly hypnotics without behavioural change is outdated exam-fail care.[8][9][2]
ICSD-3 map. The International Classification of Sleep Disorders, third edition organises pathology into major groups including insomnia disorders, sleep-related breathing disorders, central disorders of hypersomnolence, circadian rhythm sleep–wake disorders, parasomnias, and sleep-related movement disorders — the skeleton every fellowship candidate must navigate.[20]
Classification and nosology
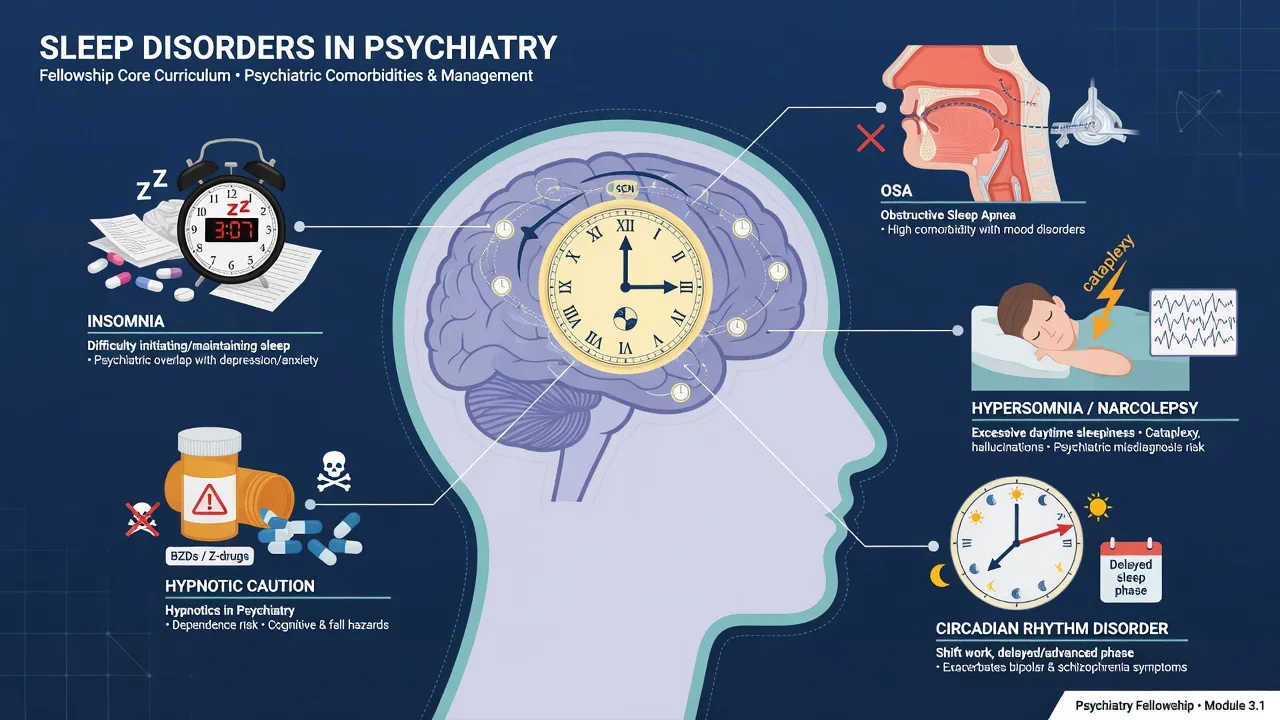
Insomnia disorders
- Chronic vs short-term (ICSD-3)
- Onset / maintenance / early awakening phenotypes
- Comorbid with MDD, GAD, PTSD common
- Not equivalent to short sleep without distress
Breathing (OSA focus)
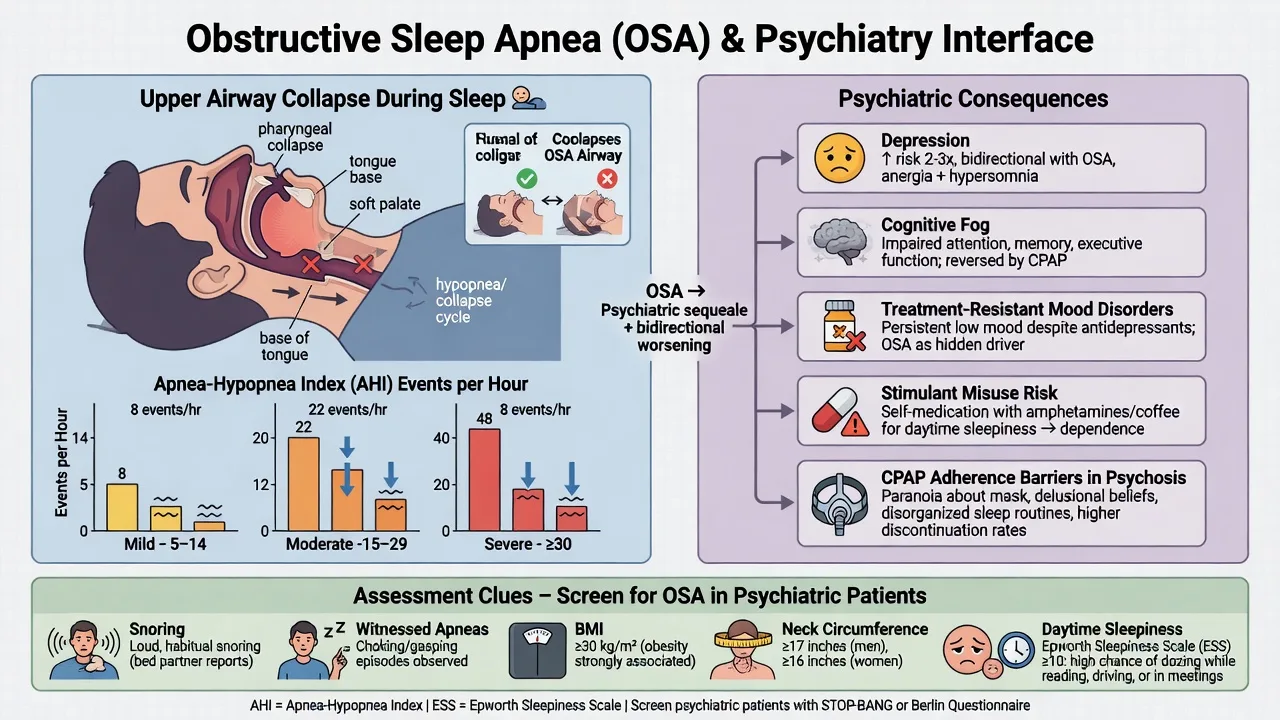
- AHI mild 5–14; moderate 15–29; severe ≥30
- Obesity, male sex, age, craniofacial risk
- Mimics and worsens depression/cognition
- CPAP is disease-modifying for symptoms/AHI
Hypersomnolence
- Narcolepsy type 1: cataplexy ± low CSF orexin
- Type 2: without cataplexy
- Idiopathic hypersomnia
- Distinguish from fatigue and atypical depression
Circadian / movement / parasomnia
- DSPD common in youth and ADHD
- RLS: urge to move, rest, evening, relief with movement
- NREM parasomnias vs REM sleep behaviour disorder
- RBD → neurodegeneration pathway
DSM-5-TR vs ICSD-3 exam pearl. Psychiatrists code insomnia disorder when criteria are met even with comorbidity (the old “primary vs secondary” dichotomy is largely retired). Sleep physicians still use ICSD-3 granularity for OSA, narcolepsy, and parasomnias — collaborate rather than compete.[19][20]
Epidemiology and risk
Headline epidemiology (exam anchors)
Community data place insomnia disorder at roughly one in ten adults, with intermittent symptoms far more common; women and older adults are disproportionately affected, and chronicity is substantial over multi-year follow-up.[25]
Meta-analytic longitudinal evidence shows insomnia predicts incident depression (order of approximately doubled risk in Baglioni-type analyses) and broader psychopathology in Hertenstein-type syntheses — examiners use this to reject the idea that insomnia is only secondary noise.[8][9]
Sleep disturbance associates with suicidal ideation, attempt, and death across meta-analytic and systematic reviews; nightmares and severe insomnia deserve explicit risk documentation.[17][18]
OSA prevalence rose with obesity epidemics; population studies (Peppard-order; HypnoLaus-order; global burden estimates) show sleep-disordered breathing is common enough that psychiatric services will miss it weekly if they do not screen.[10][27]
Pathophysiology and mechanisms
Insomnia hyperarousal. Cognitive (rumination, threat monitoring of sleep), physiological (HPA tone, high-frequency EEG), and behavioural (clock-watching, extending time in bed) loops maintain chronic insomnia independent of the original stressor.[19][5]
Two-process model. Sleep is regulated by homeostatic sleep pressure (Process S) and circadian alerting (Process C, SCN-driven). Delayed sleep–wake phase disorder is a timing mismatch, not “laziness.” Night-shift work repeatedly misaligns both processes and worsens bipolar and psychotic vulnerability.[16]
OSA mechanism. Pharyngeal collapsibility produces recurrent apnoeas/hypopnoeas, intermittent hypoxia, arousals, and fragmented sleep architecture → daytime sleepiness, mood and cognitive change, hypertension, and metabolic risk. Severity is conventionally summarised by the apnoea–hypopnoea index (AHI).[10][11]
Narcolepsy type 1. Selective loss or dysfunction of orexin/hypocretin neurons of the lateral hypothalamus explains sleep–wake instability and cataplexy; type 2 lacks clear cataplexy and typically has normal CSF orexin pathways.[22][23]
Psychotropics. Antidepressants vary: activating SSRIs/SNRIs can fragment sleep early; sedating agents (mirtazapine, trazodone, low-dose doxepin, some TCAs) improve subjective sleep but may oversedate or increase weight/OSA risk; serotonergic agents can worsen RLS. Antipsychotics (olanzapine, quetiapine) sedate via H1 and other receptors but carry metabolic cost.[12][28]
Clinical presentation
Insomnia history language. Sleep onset latency, wake after sleep onset (WASO), early terminal awakening, total sleep time, time in bed, naps, and weekday–weekend discrepancy. Ask about sleep effort, clock-watching, and catastrophic beliefs (“if I do not sleep 8 hours I will crack”).[19]
Psychiatric patterns.
- MDD: middle/late insomnia classic; hypersomnia in atypical features.
- Bipolar: reduced need for sleep without fatigue is a mania/hypomania clue — distinct from inability to sleep.
- PTSD: nightmares, hyperarousal, avoidance of bed.
- Psychosis: reversed sleep phase, paranoia about environment, medication sedation.
- Anxiety/OCD: sleep onset rumination and checking rituals. These patterns are exam discriminators rather than pathognomonic rules — always integrate full MSE and collateral.[16][19]
OSA red-flag history. Loud snoring, witnessed apnoeas, gasping, unrefreshing sleep, morning headache, resistant hypertension, large neck, obesity, and treatment-resistant “depression” with anergia.[10]
Hypersomnia clues. Irresistible sleep attacks, automatic behaviour, cataplexy (emotion-triggered weakness), sleep paralysis, hypnagogic/hypnopompic hallucinations — misdiagnosis as psychosis is an examinable trap.[22][23]
Differential diagnosis
Discriminators beat lists. Use organic and primary sleep diagnoses before labelling pure psychiatric insomnia.[16][20]
| Presentation | Favours | Against pure psychiatric insomnia |
|---|---|---|
| Loud snoring + witnessed apnoea + high BMI | OSA | Normal ESS and partner deny apnoea do not fully exclude |
| Delayed sleep, can sleep long if free schedule | DSPD | Fixed early wake with long latency only |
| Urge to move legs evening, relief with movement | RLS | Akathisia is more whole-body restlessness on antipsychotics |
| Dream enactment with injury | RBD | NREM parasomnia often first third of night, incomplete awakening |
| Cataplexy + sleep attacks | Narcolepsy type 1 | Pure fatigue without sleep propensity |
| Reduced need for sleep + elevated mood | Mania | Classic insomnia with dysphoria |
Always include substances (alcohol fragments sleep and worsens OSA; caffeine/stimulants; cannabis withdrawal), medical pain, nocturia, heart failure, thyroid disease, and medication timing.[16][12][10]
Assessment
Core structure. Chronotype, work pattern, substances, bed partner report, mood/anxiety/trauma/psychosis screen, suicide risk, driving/occupational risk, medication list (including OTC antihistamines and alcohol “nightcaps”). A complete sleep history is part of standard psychiatric assessment, not an optional add-on.[19][16]
Tools. Sleep diary (1–2 weeks) is high-yield. Actigraphy when schedule is chaotic. Insomnia Severity Index and Epworth Sleepiness Scale are commonly used validated instruments — state that local cut-offs should be interpreted with clinical context rather than inventing numbers under stress.[19][5]
OSA screens. STOP-BANG / Berlin concepts (snoring, tiredness, observed apnoea, pressure/hypertension, BMI, age, neck, gender) triage who needs sleep study referral.[10]
Risk domains. Document SI/NSSI linked to sleepless nights; fitness to drive with hypersomnolence; fall risk if prescribing sedatives to older adults.[17][21]
Investigations
- Not everyone needs PSG. Typical chronic insomnia without atypical features is a clinical diagnosis; start CBT-I without waiting for a sleep lab.[2][4]
- Refer for sleep study when moderate–high OSA probability, unexplained hypersomnia, treatment-resistant insomnia with red flags, suspected parasomnia/RBD with injury, or preoperative risk.
- MSLT (after adequate sleep opportunity and often after PSG) supports narcolepsy diagnosis pathways; CSF orexin when type 1 is strongly suspected and available.[22]
- RLS labs: ferritin/iron studies (replete iron when indices low-normal per specialist guidance); review antidepressants/antipsychotics that worsen RLS.[26]
- Baseline before sedating drugs: ECG/QTc when using antipsychotics or TCAs; falls/cognitive baseline in older adults.[21]
Acute and emergency management
- Unstable OSA / hypercapnia: medical admission pathway.
- Hypnotic overdose / delirium: ABC, stop agent, toxicology liaison; plan deprescribing after stabilisation.
- Acute mania: prioritise mood stabilisation and sleep protection (often antipsychotic/mood stabiliser), not outpatient CBT-I.
- Cataplexy falls / RBD injury: environmental safety, urgent specialist referral.[22][16]
Definitive management — insomnia
CBT-I (first-line)
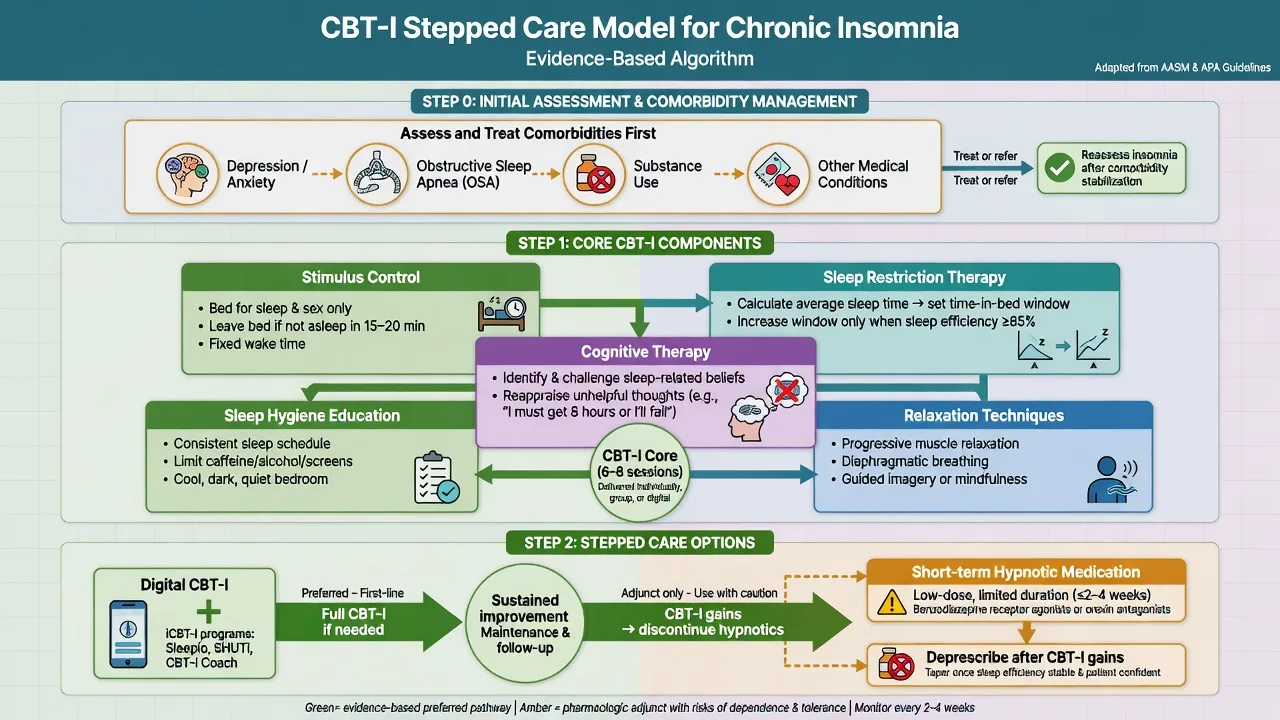
Multicomponent cognitive behavioural therapy for insomnia is first-line for chronic insomnia in adults across ACP, AASM behavioural, and European guidelines.[2][4][5][6]
Core components (viva list):
- Stimulus control — bed for sleep/sex only; leave bed if unable to sleep; fixed wake time.
- Sleep restriction therapy — match time in bed to average total sleep time; expand when efficiency improves (plan carefully if bipolar, seizure disorder, or safety-critical work).
- Cognitive therapy — challenge unhelpful sleep beliefs and safety behaviours.
- Relaxation / arousal reduction.
- Sleep education (hygiene is necessary but not sufficient alone).[4][1]
Meta-analysis shows CBT-I produces clinically meaningful improvements in sleep outcomes for chronic insomnia.[1] Digital CBT-I improves functional health and psychological well-being at scale (Espie-order RCT) and can reduce paranoia/hallucination severity via sleep mediation in student samples (Freeman OASIS).[24][13] CBT for sleep also shows pilot benefit in persistent psychotic symptoms (BEST).[14]
Morin’s combination trial logic: medication may help short-term, but CBT-I drives more durable gains — exam pearl for long-term planning.[7]
Pharmacotherapy for insomnia (second-line / adjunct)
Guidelines do not support open-ended nightly benzodiazepines as standard care. AASM pharmacologic guidance offers mostly weak recommendations for specific agents over no treatment for short-term use; long-term hypnotic monotherapy is discouraged relative to CBT-I.[3][2]
Practical fellowship framing (jurisdiction product information governs exact doses):
- Prefer shortest effective duration (often days to a few weeks) with planned taper.
- Classes: non-benzodiazepine receptor agonists (Z-drugs), short/intermediate benzodiazepines, low-dose doxepin, melatonin receptor agonists, dual orexin receptor antagonists where marketed.
- Sedating antidepressants (trazodone, mirtazapine, low-dose doxepin/amitriptyline) are widely used off-label for sleep in depression — understand receptor effects and residual hangover; they are not automatic CBT-I substitutes.[12][15][16]
- Avoid defaulting to quetiapine for primary insomnia without psychotic/mood indication — metabolic and QTc costs are real.[28]
- Older adults: meta-analytic risk–benefit of sedative-hypnotics is unfavourable (falls, cognitive adverse effects) — non-drug first.[21]
ACP (US): CBT-I first for all adults with chronic insomnia; discuss medication only after or with CBT-I when needed.[2] AASM: strong support for multicomponent CBT-I; pharmacologic options weak and agent-specific.[3][4] ESRS Europe: CBT-I first-line; 2023 update reaffirms behavioural priority.[5][6] BAP (UK): consensus on insomnia, parasomnias, circadian disorders — behavioural first, rational short-term drugs, specialist pathways.[15][16] ANZ practice: align with CBT-I first, sleep physician referral for OSA/narcolepsy, and local PBS/formulary constraints on hypnotics and wake-promoting agents.
OSA — psychiatry interface
Management principles. Weight loss, positional strategies, alcohol avoidance, CPAP for moderate–severe OSA, mandibular advancement devices in selected mild–moderate cases, surgery in anatomical subsets via ENT. Psychiatry’s job: recognise, refer, support adherence (mask paranoia in psychosis, depression reducing motivation), and avoid pure “antidepressant escalation” when hypoxia is the driver.[10][27]
SAVE trial pearl. In adults with moderate–severe OSA and established cardiovascular disease, CPAP plus usual care did not reduce hard cardiovascular composite endpoints versus usual care alone in the primary analysis — yet symptom and quality-of-life benefits and blood pressure effects remain clinically important. Do not oversell CPAP as proven secondary CV prevention in that cohort design.[11]
Hypersomnia, circadian, RLS, parasomnias
Narcolepsy. Scheduled naps, wake-promoting agents (modafinil and related agents per local licence), sodium oxybate-class therapy for cataplexy where available, psychosocial and driving advice. Specialist sleep/neurology co-management is standard.[22][23]
Circadian disorders. Timed light, melatonin timing (not “any time nightcap”), schedule regularity; DSPD is common in adolescents and delayed chronotypes — do not force 22:00 lights-out without phase work.[16]
RLS. Non-drug measures, iron repletion when ferritin low-normal, review exacerbating meds (many antidepressants, antipsychotics); alpha-2-delta ligands and dopamine agonists have evidence with augmentation risk on dopamine agonists — specialist-informed choice.[26]
Parasomnias. NREM disorders of arousal: safety, trigger reduction (sleep deprivation, alcohol), rarely clonazepam. RBD: secure environment, melatonin/clonazepam pathways, neurodegeneration counselling — not a primary “psychosis” diagnosis.[16]
Psychotropics and sleep
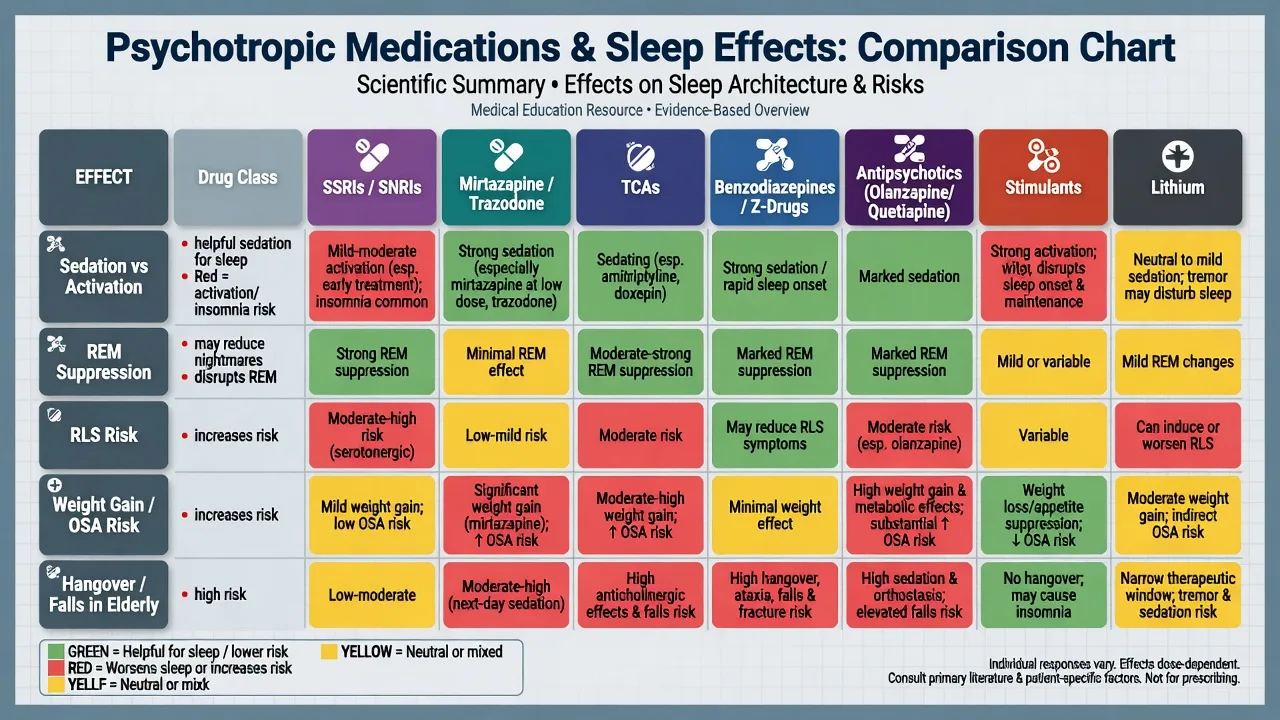
Antidepressant effects on sleep depend on agent, dose, timing, and duration; sleep-promoting effects of low-dose sedating antidepressants should be embedded in a CBT-I framework when insomnia is the target.[12] Second-generation antipsychotics alter sleep continuity with variable architecture effects; metabolic weight gain can secondarily worsen OSA.[28]
Special populations
- Older adults: falls, delirium, cognitive blunting with BZD/Z-drugs — prefer CBT-I/adapted behavioural care; review polypharmacy.[21]
- Pregnancy/lactation: prioritise non-drug; individualise any medication with obstetric liaison (agent-specific data; avoid fabricating absolute safety claims).
- Youth: DSPD and insomnia common; family-supported behavioural schedules first; specialist for narcolepsy.
- Psychosis inpatient: sleep stabilisation is part of acute care; CBT-I adaptations and environmental control matter.[14]
- ANZ contexts: FIFO/shift work, rural sleep-lab access delays — start behavioural care while awaiting PSG when OSA probability is moderate.
Prognosis and disposition
Without CBT-I, insomnia often chronicles for years. With CBT-I, gains are more durable than medication alone; plan booster sessions and hypnotic deprescribing.[7][1] OSA is a chronic disease model — adherence determines benefit. Safety-net for escalating SI, driving near-misses, and witnessed apnoeas. Step up to sleep medicine, liaison medicine, or crisis services when red flags appear.
Exam pearls
SLEEP CARE (assessment checklist)
Use this checklist on every complex sleep–psychiatry case to avoid missing OSA, substances, risk, and first-line CBT-I.[2][10][17]
References
- [1]Trauer JM, Qian MY, Doyle JS, et al. Cognitive Behavioral Therapy for Chronic Insomnia: A Systematic Review and Meta-analysis Ann Intern Med, 2015.PMID 26054060
- [2]Qaseem A, Kansagara D, Forciea MA, et al. Management of Chronic Insomnia Disorder in Adults: A Clinical Practice Guideline From the American College of Physicians Ann Intern Med, 2016.PMID 27136449
- [3]Sateia MJ, Buysse DJ, Krystal AD, et al. Clinical Practice Guideline for the Pharmacologic Treatment of Chronic Insomnia in Adults: An American Academy of Sleep Medicine Clinical Practice Guideline J Clin Sleep Med, 2017.PMID 27998379
- [4]Edinger JD, Arnedt JT, Bertisch SM, et al. Behavioral and psychological treatments for chronic insomnia disorder in adults: an American Academy of Sleep Medicine clinical practice guideline J Clin Sleep Med, 2021.PMID 33164742
- [5]Riemann D, Baglioni C, Bassetti C, et al. European guideline for the diagnosis and treatment of insomnia J Sleep Res, 2017.PMID 28875581
- [6]Riemann D, Espie CA, Altena E, et al. The European Insomnia Guideline: An update on the diagnosis and treatment of insomnia 2023 J Sleep Res, 2023.PMID 38016484
- [7]Morin CM, Vallieres A, Guay B, et al. Cognitive behavioral therapy, singly and combined with medication, for persistent insomnia: a randomized controlled trial JAMA, 2009.PMID 19454639
- [8]Baglioni C, Battagliese G, Feige B, et al. Insomnia as a predictor of depression: a meta-analytic evaluation of longitudinal epidemiological studies J Affect Disord, 2011.PMID 21300408
- [9]Hertenstein E, Feige B, Gmeiner T, et al. Insomnia as a predictor of mental disorders: A systematic review and meta-analysis Sleep Med Rev, 2019.PMID 30537570
- [10]Peppard PE, Young T, Barnet JH, et al. Increased prevalence of sleep-disordered breathing in adults Am J Epidemiol, 2013.PMID 23589584
- [11]McEvoy RD, Antic NA, Heeley E, et al. CPAP for Prevention of Cardiovascular Events in Obstructive Sleep Apnea N Engl J Med, 2016.PMID 27571048
- [12]Wichniak A, Wierzbicka A, Walecka M, et al. Effects of Antidepressants on Sleep Curr Psychiatry Rep, 2017.PMID 28791566
- [13]Freeman D, Sheaves B, Goodwin GM, et al. The effects of improving sleep on mental health (OASIS): a randomised controlled trial with mediation analysis Lancet Psychiatry, 2017.PMID 28888927
- [14]Freeman D, Waite F, Startup H, et al. Efficacy of cognitive behavioural therapy for sleep improvement in patients with persistent delusions and hallucinations (BEST): a prospective, assessor-blind, randomised controlled pilot trial Lancet Psychiatry, 2015.PMID 26363701
- [15]Wilson SJ, Nutt DJ, Alford C, et al. British Association for Psychopharmacology consensus statement on evidence-based treatment of insomnia, parasomnias and circadian rhythm disorders J Psychopharmacol, 2010.PMID 20813762
- [16]Wilson S, Anderson K, Baldwin D, et al. British Association for Psychopharmacology consensus statement on evidence-based treatment of insomnia, parasomnias and circadian rhythm disorders: An update J Psychopharmacol, 2019.PMID 31271339
- [17]Pigeon WR, Pinquart M, Conner K Meta-analysis of sleep disturbance and suicidal thoughts and behaviors J Clin Psychiatry, 2012.PMID 23059158
- [18]Bernert RA, Kim JS, Iwata NG, et al. Sleep disturbances as an evidence-based suicide risk factor Curr Psychiatry Rep, 2015.PMID 25698339
- [19]Buysse DJ Insomnia JAMA, 2013.PMID 23423416
- [20]Sateia MJ International classification of sleep disorders-third edition: highlights and modifications Chest, 2014.PMID 25367475
- [21]Glass J, Lanctot KL, Herrmann N, et al. Sedative hypnotics in older people with insomnia: meta-analysis of risks and benefits BMJ, 2005.PMID 16284208
- [22]Bassetti CLA, Adamantidis A, Burdakov D, et al. Narcolepsy - clinical spectrum, aetiopathophysiology, diagnosis and treatment Nat Rev Neurol, 2019.PMID 31324898
- [23]Scammell TE Narcolepsy N Engl J Med, 2015.PMID 26716917
- [24]Espie CA, Emsley R, Kyle SD, et al. Effect of Digital Cognitive Behavioral Therapy for Insomnia on Health, Psychological Well-being, and Sleep-Related Quality of Life: A Randomized Clinical Trial JAMA Psychiatry, 2019.PMID 30264137
- [25]Morin CM, Jarrin DC Epidemiology of Insomnia: Prevalence, Course, Risk Factors, and Public Health Burden Sleep Med Clin, 2022.PMID 35659072
- [26]Winkelmann J, Allen RP, Hogl B, et al. Treatment of restless legs syndrome: Evidence-based review and implications for clinical practice (Revised 2017) Mov Disord, 2018.PMID 29756335
- [27]Benjafield AV, Ayas NT, Eastwood PR, et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis Lancet Respir Med, 2019.PMID 31300334
- [28]Monti JM, Torterolo P, Pandi Perumal SR The effect of second-generation antipsychotic drugs on sleep parameters in patients with unipolar or bipolar disorder Sleep Med, 2016.PMID 27692282