Cardiology · Cardiology
Aortic Regurgitation
Also known as Aortic regurgitation · Aortic insufficiency · AR · Aortic incompetence
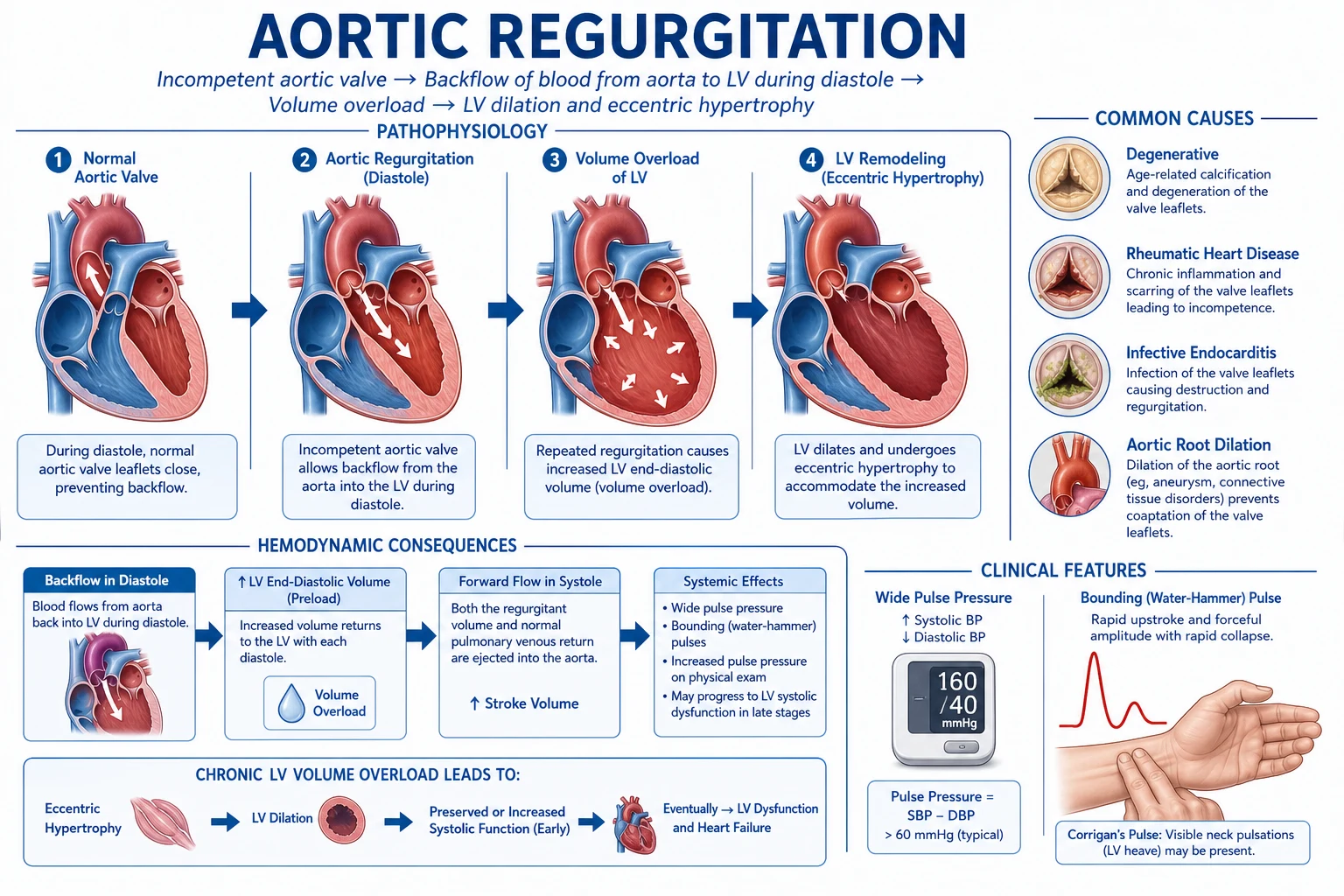
Aortic regurgitation (AR) is diastolic incompetence of the aortic-valve complex permitting backflow from the aorta into the left ventricle. In chronic AR the LV remodels by eccentric hypertrophy, giving the classic signs — early-diastolic decrescendo murmur at Erb point, wide pulse pressure, water-hammer (Corrigan) pulse and a constellation of peripheral signs (de Musset, Quincke, Traube, Duroziez, Hill). Causes are leaflet disease (rheumatic, bicuspid, endocarditis) or aortic-root dilation (Marfan, hypertension, ankylosing spondylitis, syphilis). Acute severe AR (endocarditis, type A dissection, trauma) presents as sudden pulmonary oedema without the classic signs. Diagnosis is by echocardiography, which grades severity (regurgitant volume, fraction, EROA, vena contracta). Definitive treatment is aortic valve surgery (AVR) when symptomatic, when EF is 50 percent or below, or when LV end-systolic diameter exceeds 50 mm. Never use an intra-aortic balloon pump in significant AR.
On this page & tools
Your progress
Saved locally on this device.
Exam tags
Red flags
Overview & Definition
Aortic regurgitation (AR), also called aortic insufficiency or aortic incompetence, is diastolic incompetence of the aortic-valve complex — the three leaflets (right, left and non-coronary cusps), the annulus, the sinuses of Valsalva and the proximal ascending aorta — that permits blood to flow back from the aorta into the left ventricle during diastole.[1]
The normal aortic valve is a passive, pressure-driven structure: it opens in systole when LV pressure exceeds aortic pressure, and snaps shut at the onset of diastole as aortic pressure climbs above the falling LV pressure. Three features keep a competent valve: thin, supple, well-opposed leaflets; a structurally normal annulus of the correct diameter; and an ascending aorta that does not dilate and pull the commissures apart. Disease of any one of these three elements can produce AR — which is why the differential runs from a single perforated cusp in endocarditis to a normal valve leaflet stranded in a Marfan aortic root that has dilated to 6 cm. This anatomic fact is the basis of the leaflet-versus-root dichotomy that decides the operation.[3]
The clinical skill in AR is not naming the murmur (a well-taken early-diastolic decrescendo murmur at the left sternal edge is unmistakable) but distinguishing chronic from acute disease and timing surgery — operating before the LV has suffered irreversible systolic dysfunction, yet not so early that the patient takes on lifelong prosthetic-valve risk unnecessarily. Chronic AR allows years of compensation by eccentric hypertrophy; acute AR is a surgical emergency in which the classic peripheral signs are absent and the murmur may be soft and short because aortic and LV diastolic pressures equalise almost instantly.[1][2]
Classification
AR is classified along three axes — timing (acute vs chronic), mechanism (leaflet vs root), and severity — because each drives management differently.[1]
Chronic AR
- Gradual onset over years; LV remodels by eccentric hypertrophy (sarcomeres in series)
- Classic signs present: wide pulse pressure, water-hammer pulse, hyperdynamic displaced apex, florid peripheral signs
- Murmur long, high-pitched, blowing decrescendo; tolerated for years to decades
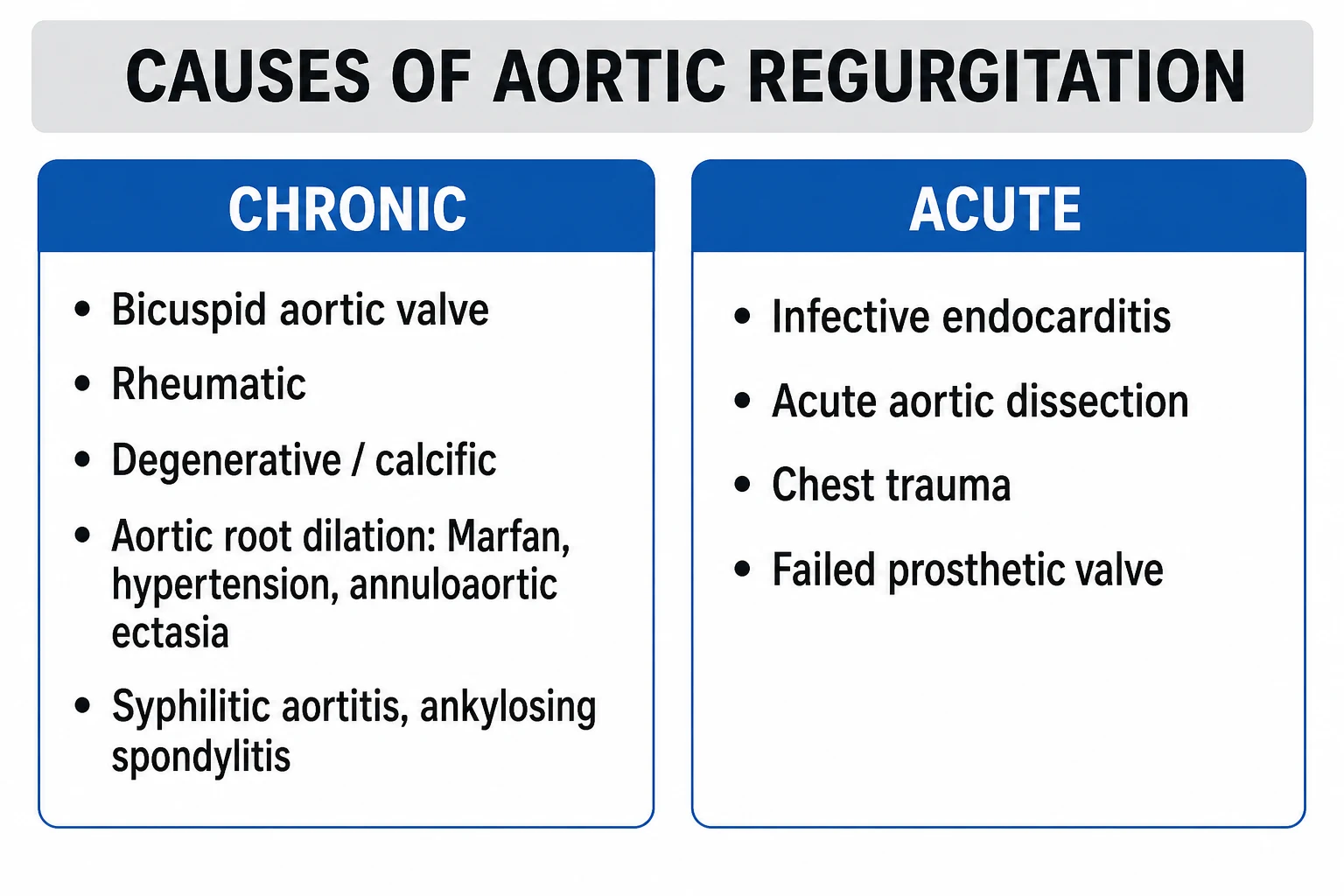
- Causes: bicuspid valve, degenerative/calcific, rheumatic, aortic-root dilation (Marfan, hypertension, seronegative arthropathy, syphilis)
Acute AR
- Sudden incompetence over hours; LV cannot remodel
- Sudden rise in LVEDP, acute LV failure, pulmonary oedema, cardiogenic shock
- Classic peripheral signs ABSENT; pulse pressure often narrow; murmur short, soft or inaudible
- Causes: infective endocarditis, type A aortic dissection, blunt chest trauma, prosthetic-valve dehiscence; SURGICAL EMERGENCY
By mechanism, AR is either leaflet/cusp disease — rheumatic scarring and retraction, bicuspid cusp prolapse, infective vegetations preventing coaptation, degenerative calcification, myxomatous prolapse, drug-induced (historic fenfluramine-phentermine anorexigens) — or aortic-root and annular disease, in which dilation pulls structurally normal leaflets apart. The root causes include Marfan syndrome, Loeys-Dietz syndrome, vascular (type IV) Ehlers-Danlos, bicuspid aortopathy, long-standing hypertension, senile annuloaortic ectasia, tertiary syphilis, ankylosing spondylitis, rheumatoid arthritis, systemic lupus erythematosus, giant-cell arteritis, Takayasu arteritis, relapsing polychondritis, psoriatic arthropathy and reactive arthritis. This mechanism split is more than academic: a diseased leaflet needs replacement (AVR), whereas a dilated root with normal leaflets may be cured by valve-sparing root replacement (David procedure), sparing the patient lifelong anticoagulation.[3][1]
By severity (echo-derived — see Investigations): mild, moderate, severe, based on jet-to-LVOT-width ratio, vena contracta width, regurgitant volume, regurgitant fraction and effective regurgitant orifice area (EROA), supplemented by the pressure half-time and the presence of holodiastolic flow reversal in the descending aorta.[4]
Epidemiology & Risk Factors
AR is less common than aortic stenosis in elderly populations but is the second commonest single valvular lesion requiring surgery overall. Trace or mild AR is found on transthoracic echo in a high proportion of healthy adults — detectable in up to a third of older adults with structurally normal valves — and is of no clinical consequence. Moderate or severe chronic AR affects roughly 2 to 3 percent of older adults. Bicuspid aortic valve, the commonest congenital cardiac anomaly with a prevalence of about 1 in 100, is the commonest congenital cause of AR and is frequently complicated by aortic coarctation and an associated aortopathy of the root and ascending aorta that progresses independently of the valve lesion.[3]
The aetiology of AR is dominated by geography and age, an examiner favourite that also dictates what a candidate will see in clinical practice: [1]
| Setting | Commonest causes |
|---|---|
| Developed world, any age | Bicuspid aortic valve, degenerative/calcific, aortic-root dilation from long-standing hypertension |
| Developing world (India/South Asia) | Rheumatic heart disease (usually mixed mitral and aortic disease) |
| Young adult, tall habitus | Marfan syndrome, Loeys-Dietz, vascular Ehlers-Danlos (root aneurysm) |
| Seronegative arthropathy | Ankylosing spondylitis, reactive arthritis, psoriatic/enteropathic arthropathy (aortitis) |
| Tertiary syphilis | Luetic aortitis of the ascending aorta (tree-bark intimal appearance, characteristically spares the sinuses unlike other aortitides) |
| Acute severe AR | Infective endocarditis, type A aortic dissection, blunt chest trauma, prosthetic-valve dehiscence |
| Drugs | Historic fenfluramine-phentermine (anorexigens), carcinoid (rare, right-sided usually) |
AR at a glance
Risk factors are essentially the conditions above: congenital bicuspid valve, family history of aortic aneurysm or dissection, long-standing hypertension, rheumatic fever, injection drug use (endocarditis), connective-tissue disorders (Marfan, Loeys-Dietz, vascular Ehlers-Danlos), autoimmune inflammatory disease (ankylosing spondylitis, RA, SLE, vasculitis) and prior mediastinal radiation.[1]
Pathophysiology
Chronic AR — combined volume and pressure overload
In chronic AR the LV receives, each diastole, the normal pulmonary venous inflow from the left atrium PLUS the regurgitant volume returning from the aorta. The total diastolic filling is therefore supernormal, and the response of a slowly overloaded ventricle is eccentric hypertrophy — addition of sarcomeres in series, lengthening individual myocytes and dilating the chamber — so the cavity enlarges while wall thickness remains relatively normal or even thinned. This is the mirror image of the concentric hypertrophy (sarcomeres in parallel) of aortic stenosis, where the chamber is small and the wall thick.[3]
This produces a deceptively well-tolerated compensated state for years: the total stroke volume (forward plus regurgitant) is large, the ejection fraction is preserved or even supernormal, and forward cardiac output is maintained. The cost is a steadily rising wall stress described by Laplace's relationship — wall stress equals (intracavitary pressure times radius) divided by (twice the wall thickness). As the chamber dilates (radius rises) the wall stress climbs, so the afterload on this "volume-overloaded" ventricle is in fact also raised. The compensated phase therefore has an inbuilt timer: eventually systolic function falls, the EF drops, the LV enters a decompensated phase, and the dysfunction may be irreversible even after a technically perfect valve replacement. This irreversible loss is exactly what surgical surveillance is designed to prevent.[1][3]
As decompensation evolves, the myocardium activates the same neurohormonal cascades seen in other forms of heart failure — sympathetic nervous system up-regulation (tachycardia, vasoconstriction), renin-angiotensin-aldosterone system activation (sodium and water retention, further afterload rise), and N-terminal pro-B-type natriuretic peptide (NT-proBNP) release from the stretched ventricle. A rising NT-proBNP is therefore an early biochemical marker of the transition from the compensated to the decompensated phase and is incorporated into modern surveillance. Histologically the chronically volume-overloaded myocardium develops interstitial fibrosis and myocyte apoptosis that contribute to the irreversibility of late dysfunction — which is exactly why the surgical thresholds (EF 50 percent, LVESD 50 mm) are deliberately set before symptoms, so the operating surgeon is working on a ventricle that can still recover.[3][5]
Why the wide pulse pressure and peripheral signs
Two simultaneous mechanisms produce the wide pulse pressure that is the haemodynamic signature of severe chronic AR. First, a high systolic pressure, because the dilated LV ejects a large total stroke volume (forward plus regurgitant) into a fixed aortic reservoir. Second, a low diastolic pressure, because blood runs off rapidly through two parallel exits — the systemic capillaries and the incompetent valve back into the LV — emptying the aorta faster than normal. The lower the diastolic pressure, the larger the pulse pressure and the more florid the peripheral signs (Corrigan pulse, Traube pistol-shot, Duroziez, Hill). A diastolic pressure below 50 mmHg strongly suggests severe AR, and a pulse pressure exceeding 100 mmHg is similarly suggestive.[3]
Coronary perfusion and angina
Coronary blood flow occurs predominantly in diastole and is driven by the aortic-to-myocardial pressure gradient (aortic diastolic pressure minus intramyocardial diastolic pressure). In severe AR the diastolic aortic pressure falls (rapid run-off) while the LV diastolic pressure rises (volume overload), collapsing that gradient and reducing coronary perfusion reserve. Patients therefore experience angina even in the absence of epicardial coronary artery disease — a classic and frequently tested point. The angina is often nocturnal, because sleep bradycardia lengthens diastole, increasing per-beat regurgitant volume and widening the run-off, and because the heart rate falls and the diastolic pressure drops further.[3]
Acute AR — no time to remodel
In acute severe AR (endocarditis destroying or perforating a cusp, type A dissection raising a cusp by detaching the commissure, blunt chest trauma, prosthetic dehiscence) the LV has no time for eccentric remodelling. The sudden regurgitant load is dumped into a normal-sized, non-compliant ventricle, raising LV end-diastolic pressure dramatically; the mitral valve may close prematurely in diastole (functional mitral stenosis protecting the pulmonary circulation); and the patient develops acute left heart failure, pulmonary oedema and cardiogenic shock. Critically, because aortic and LV diastolic pressures equalise rapidly, the murmur is often short, soft and early rather than the long decrescendo of chronic disease, and the wide pulse pressure and peripheral signs are absent — the pulse pressure is often narrow because the patient is in shock. Missing acute AR at the bedside is a classic and fatal error.[1]
Heart rate dependence
Because regurgitation occurs in diastole, anything that lengthens diastole (bradycardia) increases regurgitant volume per beat, and anything that shortens diastole (tachycardia) reduces it. This is why pure beta-blocker monotherapy is avoided in significant acute AR unless required for another indication (e.g., dissection), and why the physiological tachycardia of pregnancy is, within limits, a compensatory response in chronic AR.[1]
Clinical Presentation
Chronic severe AR
Chronic AR is often asymptomatic for years or even decades, discovered on a routine examination (a murmur) or incidentally on echocardiography performed for another reason. This long silent compensated phase is the rationale for serial surveillance imaging. Once symptomatic, three symptom clusters dominate:[3]
- Left heart failure — exertional dyspnoea, orthopnoea, paroxysmal nocturnal dyspnoea and fatigue, reflecting falling forward output as the LV decompensates and LVEDP climbs.
- Angina — atypical, often nocturnal, occurring even with angiographically normal coronaries, because diastolic run-off collapses the coronary perfusion gradient (see Pathophysiology).
- Palpitations — a forceful, pounding heartbeat from the large stroke volume is itself a symptom, distinct from an arrhythmia; atrial fibrillation may develop in advanced disease as the dilated left atrium stretches. [1]
Less common but well-recognised symptoms include exertional syncope or presyncope (inability to raise output on effort), nocturnal angina (bradycardia-driven), and peripheral oedema and ascites once right heart failure supervenes in end-stage disease. [1]
Acute severe AR
Presents as sudden severe dyspnoea, pulmonary oedema, hypotension and cardiogenic shock. There is usually an obvious trigger: fever, a new murmur and embolic phenomena in endocarditis; tearing interscapular chest pain with a pulse or blood-pressure differential in type A dissection; recent blunt deceleration chest trauma; or sudden dysfunction of a known prosthetic valve. The early-diastolic murmur may be soft or inaudible, and the pulse pressure is often narrow rather than wide because the patient is in shock and there has been no time for remodelling.[1]
Atypical and special presentations
- Elderly: present with heart failure, fatigue, or falls rather than classic symptoms; degenerative/calcific and mixed AS-AR lesions are common, and the stiff, non-compliant LV decompensates at smaller regurgitant volumes than in younger patients.
- Pregnancy: chronic stable AR is generally well tolerated because the tachycardia and fall in systemic vascular resistance of pregnancy both reduce regurgitant volume; acute decompensation is rare but possible in severe lesions.
- Athletes: mild physiological LV dilation on echo (the "athlete's heart") must be distinguished from pathological AR by careful assessment of valve morphology, regurgitant fraction and chamber dimensions.
- Asymptomatic with advanced LV dilation: silent progression to irreversible LV dysfunction is exactly the scenario surveillance echocardiography is designed to catch before the EF falls. [1]
Differential Diagnosis
A diastolic murmur plus bounding pulses is not always AR. The high-yield differentials an examiner will probe:[3]
| Mimic | Murmur character | Distinguishing features |
|---|---|---|
| Pulmonary regurgitation (Graham Steell) | Identical early-diastolic decrescendo blowing murmur at the left sternal edge | Secondary to pulmonary hypertension; loud P2, RV heave/parasternal lift, elevated JVP with prominent a wave; signs of the cause (severe MS, Eisenmenger) |
| Mitral stenosis | Mid-diastolic rumble at the apex with presystolic accentuation | Localised to the apex (not left sternal edge); opening snap; no peripheral signs; confused with Austin Flint murmur of AR itself |
| Patent ductus arteriosus | Continuous machinery murmur, maximal under the left clavicle | Bounding pulses present from childhood; not acquired in adult life |
| Mixed AS and AR | Systolic ejection murmur plus an early-diastolic murmur | Carotid radiation and slow-rising pulsus parvus et tardus of AS coexist with the AR signs |
| VSD with aortic cusp prolapse | Systolic and diastolic murmurs | The prolapsing right coronary cusp causes AR; thrill and signs of VSD |
| Functional/trivial AR | Small, clinically silent leak | Detected only on echo; no peripheral signs, normal LV |
The single most useful distinguishing manoeuvre is the site and character of the murmur combined with signs of pulmonary hypertension (loud P2, RV heave) — the presence of pulmonary hypertension excludes simple AR as the cause of the murmur and points to Graham Steell. An Austin Flint murmur is distinguished from organic mitral stenosis by the absence of an opening snap, no loud S1, and no presystolic accentuation in atrial fibrillation.[3]
Clinical & Bedside Assessment
The murmur
The classical murmur of chronic AR is an early-diastolic, high-pitched, blowing, decrescendo murmur heard best at the left third intercostal space (Erb point) — occasionally at the right second intercostal space in root-dilating AR (where the regurgitant jet is directed anteriorly by the dilated root) — using the diaphragm of the stethoscope pressed firmly against the chest, with the patient sitting forward and the breath held in expiration (which brings the aortic area closer to the chest wall and removes lung interposition). The murmur begins immediately after A2 and decrescendos through diastole as the aorto-LV pressure gradient falls.[3]
Two companion findings are examiner staples: [1]
- Austin Flint murmur — a low-pitched mid-diastolic rumble at the apex, produced by the regurgitant jet striking the anterior mitral leaflet and pushing it partly closed, creating a functional mitral stenosis. Heard with the bell of the stethoscope in the left lateral position. Distinguished from true organic MS by the absence of an opening snap, no loud S1, and no presystolic accentuation in atrial fibrillation (because there is no atrial kick to accentuate flow across a stenotic valve).
- Soft or absent A2 (aortic component of S2) in severe chronic AR, because the leaflets cannot snap shut; paradoxical splitting is rare. A third heart sound appears late as the LV fails and compliance falls. [1]
The duration of the murmur is inversely related to severity in acute AR: as regurgitation worsens, aortic and LV pressures equalise sooner and the murmur shortens — a soft short murmur in acute AR is therefore a red flag, not reassurance. In chronic AR a longer murmur generally reflects more severe regurgitation because the gradient persists through more of diastole.[3]
Pulse and peripheral signs
The constellation of peripheral signs of a wide pulse pressure is a high-yield viva topic. Each is a visible or audible manifestation of the same underlying phenomenon — a large stroke volume entering the aorta and then running off rapidly in diastole. Memorise the full set:[3]
Peripheral signs of severe AR
Other named signs less often asked but sometimes examined: Landolfi (alternating pupil constriction and dilation with each beat), Rosenbach (liver pulsation), Gerhardt/Sailer (spleen and liver pulsation respectively), Sherman (femoral systolic expansion), and Mayne (drop in diastolic BP exceeding 15 mmHg on raising the arm). A water-hammer (Corrigan) pulse is a rapidly rising, collapsing pulse best felt by raising the patient's arm above the head and gripping the radial artery with the palm — the collapsing phase is the diastolic run-off.[3]
The apex and the blood pressure
The apex beat is displaced downwards and outwards (often into the sixth or seventh intercostal space, mid-axillary line), diffuse, hyperdynamic and thrusting — the so-called "heaving" apex of volume overload, distinct from the sustained heave of pressure overload seen in aortic stenosis. A systolic thrill may be felt over the aortic area and base from the large stroke volume traversing a normal LV outflow tract (a flow thrill, not necessarily mixed stenosis). A diastolic thrill is occasionally felt in very severe AR.[3]
Blood pressure shows a wide pulse pressure: systolic raised (often 140-180 mmHg from the large stroke volume), diastolic lowered (often 40-60 mmHg from rapid run-off). A diastolic pressure below 50 mmHg or a pulse pressure exceeding 100 mmHg suggests severe AR. Hill's sign — lower-limb systolic BP exceeding upper-limb systolic BP by more than 20 mmHg (and over 60 mmHg in severe AR) — is a quantitative peripheral sign; the gradient reflects the augmented pressure wave travelling down the aorta. [1]
[1]Peripheral signs of AR — SQAD-CQ (or STOP-MT)
SQAD-CQ
femoral systolic expansion
nail-bed capillary pulsation
apical mid-diastolic rumble + hyperdynamic displaced apex
femoral to-and-fro murmur with compression
water-hammer pulse + head nodding
pistol-shot over femorals; plus Hill, Muller, Becker
Investigations
ECG
Non-specific but supportive. In chronic AR the ECG typically shows left ventricular hypertrophy with voltage criteria — Sokolow-Lyon (SV1 plus RV5 or RV6 exceeding 35 mm) or Cornell (SV3 plus RaVL exceeding 28 mm in men, 20 mm in women) — and a left ventricular strain pattern (ST depression and T-wave inversion in lateral leads I, aVL, V5-V6). Left-axis deviation, left atrial enlargement (bifid P in V1, widened notched P in II) and, late in the disease, conduction defects (left bundle branch block) and atrial fibrillation may appear. The ECG is usually normal in early chronic AR and a normal ECG never excludes severe disease.[4]
Chest X-ray
Cardiomegaly with a prominent, sometimes boot-shaped LV silhouette (the convex LV apex of eccentric hypertrophy), a dilated or unfolded ascending aorta, and, in heart failure, pulmonary venous congestion, interstitial oedema and Kerley B lines. A widened mediastinum (over 8 cm at the knuckle) raises concern for aortic dissection as the cause of acute AR and mandates urgent CT angiography. Calcification of the aortic valve or root may be visible, suggesting a degenerative or bicuspid substrate.[4]
Echocardiography (transthoracic — first line and central)
Transthoracic echocardiography (TTE) is the pivotal investigation in AR. It answers four questions, each of which drives management: (1) mechanism (leaflet disease versus root dilation), (2) severity, (3) LV size and systolic function (the surgical triggers), and (4) associated lesions and root anatomy.[4]
Severity parameters (ACC/AHA and ASE, reproduced verbatim):[1][4]
| Parameter | Mild | Severe |
|---|---|---|
| Jet width / LVOT width ratio (colour) | under 25 percent | 65 percent or above |
| Vena contracta width | under 3 mm | 6 mm or above |
| Regurgitant volume | under 30 mL/beat | 60 mL/beat or above |
| Regurgitant fraction | under 30 percent | 50 percent or above |
| EROA (effective regurgitant orifice area) | under 0.10 cm squared | 0.30 cm squared or above |
| Pressure half-time (PHT) | over 500 ms | under 200 ms |
| Diastolic flow reversal in descending aorta | brief | holodiastolic (severe) |
A holodiastolic flow-reversal signal in the descending (and particularly abdominal) aorta on pulsed-wave Doppler is one of the most reliable markers of severe AR. A short PHT reflects rapid equalisation of aortic and LV diastolic pressure and therefore more severe disease — the same mechanism that shortens the murmur. No single parameter is sufficient; severity grading integrates multiple measures.[4]
LV dimensions — the surgical triggers: LV end-systolic diameter (LVESD), LV end-diastolic diameter (LVEDD), plus ejection fraction. These three numbers, tracked serially, drive the timing of surgery (see Management). Indexed LVESD (per body surface area) refines the threshold in small and large patients.[1]
Transoesophageal echo (TOE/TEE)
Better than TTE for mechanism (bicuspid morphology, cusp prolapse or perforation, vegetations, abscess), aortic-root anatomy (annulus and sinus dimensions, intimal flap of dissection), and intra-operative assessment. Used when TTE windows are poor, when acute AR is suspected (endocarditis, dissection), and routinely during surgery to confirm the result.[4]
Cardiac MRI
The gold standard for LV volumes, mass and regurgitant fraction, especially when echo images are poor, when there is discordance between clinical and echo findings, or for serial follow-up of aortic-root aneurysms in connective-tissue disease. CMR quantifies AR by phase-contrast velocity mapping and characterises the entire aorta — invaluable in Marfan, Loeys-Dietz and bicuspid aortopathy.[2]
Cardiac CT and coronary angiography
Cardiac CT (CT angiography) defines aortic-root and annular dimensions, the distribution of aneurysmal change, and is used for procedural planning (surgical sizing, TAVR work-up); it also detects dissection and intramural haematoma. Coronary angiography is performed pre-operatively in patients over 40 (or with risk factors) to define coronary anatomy and disease so that CABG can be combined if needed; it is not required to diagnose AR in the echo era and adds nothing to severity grading.[1]
Exercise testing and biomarkers
In asymptomatic severe AR a treadmill exercise test can elicit symptoms the patient has not volunteered — a positive test (symptom-limited, exertional dyspnoea, or a failure of blood pressure to rise) reclassifies the patient as symptomatic and therefore surgical. BNP/NT-proBNP trending upward over serial visits suggests early decompensation and may lower the threshold for intervention in borderline cases.[1]
Management — Resuscitation
Acute severe AR is a surgical emergency. The regurgitant lesion itself cannot be stabilised medically for more than hours; the only durable treatment is restoration of valve competence by emergency surgery (AVR, valve-sparing root replacement, or repair depending on mechanism). All medical manoeuvres are a bridge to theatre, not a substitute.[1]
While preparing for theatre, manage the specific scenario: [1]
- Type A aortic dissection with AR — emergency surgical repair is the only definitive treatment. Control hypertension and pain with IV labetalol (20-80 mg bolus then 20-200 mg/hour infusion) or IV esmolol (loading 500 microgram/kg over 1 minute, then 50-300 microgram/kg/minute) plus a vasodilator such as IV sodium nitroprusside (0.3-3 microgram/kg/minute). A beta-blocker is essential here because it controls the dissection by lowering the rate of rise of arterial pressure (dP/dt), but it must be started only after a vasodilator is running — unopposed vasodilation raises dP/dt and may extend the dissection.
- Acute AR with pulmonary oedema — sit upright, high-flow oxygen, IV furosemide (40-80 mg bolus, repeated as needed), non-invasive ventilation (CPAP or BiPAP) to recruit alveoli and reduce preload, and an IV vasodilator (sodium nitroprusside or glyceryl trinitrate) to reduce afterload and forward run-off, as a bridge to surgery.
- Infective endocarditis with acute AR — draw three sets of blood cultures from separate sites before starting intravenous antibiotics per the local endocarditis protocol (benzylpenicillin/gentamicin or vancomycin/gentamicin depending on native versus prosthetic and presentation). Early surgery (within days, not after a fixed antibiotic course) is indicated for heart failure, uncontrolled infection, perivalvular extension (abscess, heart block) or large mobile vegetations — heart failure from AR in endocarditis is itself a surgical indication.[1]
Avoid pure beta-blocker monotherapy in acute AR unless specifically required (e.g., dissection): bradycardia lengthens diastole and increases regurgitant volume per beat, worsening pulmonary oedema. [1]
Management — Definitive & Stepwise
The strategy in chronic AR is surveillance until a surgical threshold is crossed, then operate. Medical therapy does not replace surgery when criteria are met; it is reserved for patients who cannot or will not undergo surgery, or as a bridge to surgery. The entire art of chronic AR management is timing — operate too early and the patient takes on lifelong prosthetic-valve risk unnecessarily; operate too late and the LV dysfunction may not recover.[1][2]
Surgical indications (ACC/AHA 2020, ESC/EACTS 2021)
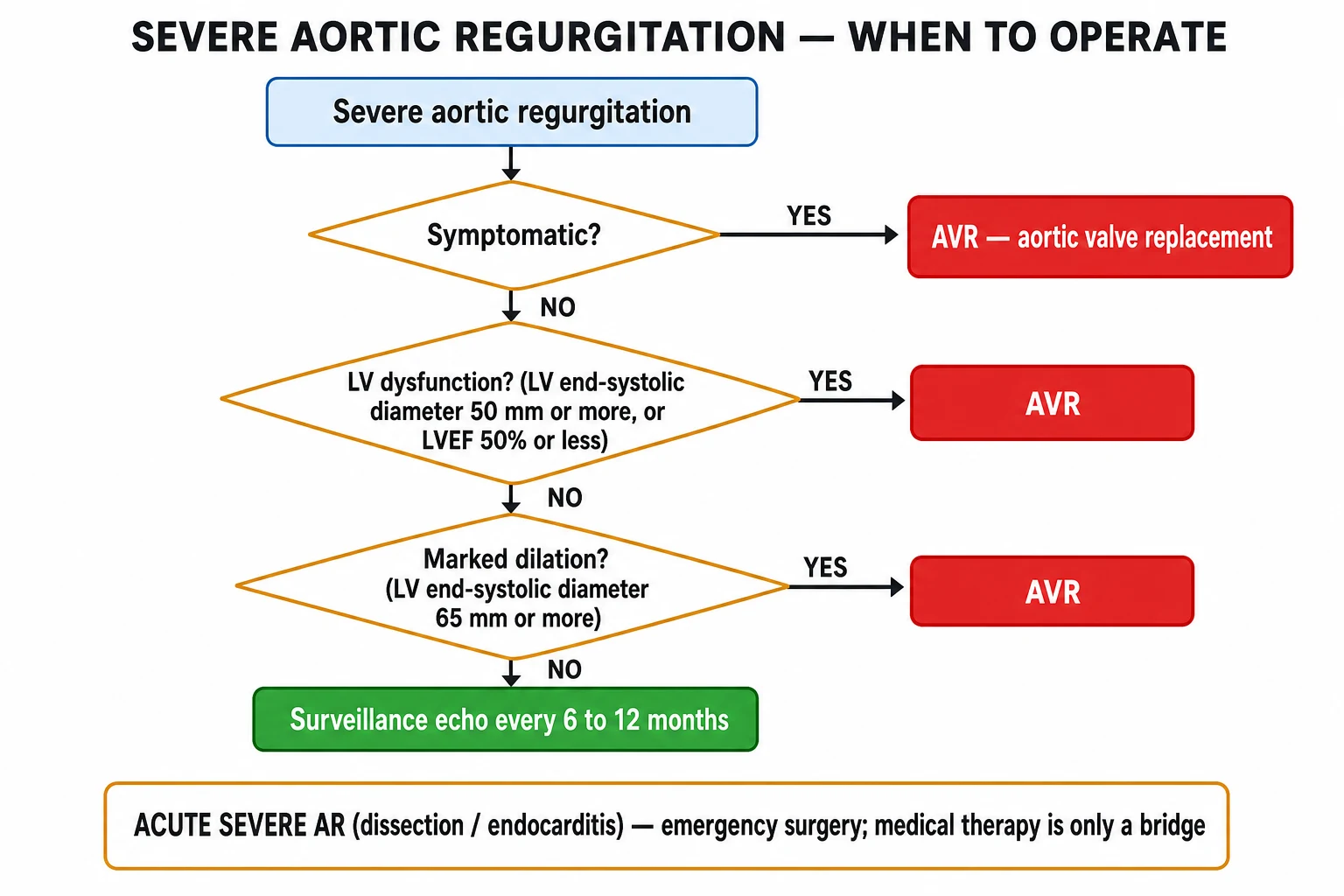
Surgery is recommended (Class I) for:[1][2]
- Symptomatic severe AR (dyspnoea, angina, syncope, heart failure) — regardless of LV function. Symptoms are the overriding trigger.
- Asymptomatic severe AR with LV systolic dysfunction — ejection fraction 50 percent or below.
- Asymptomatic severe AR with severe LV dilation — LV end-systolic diameter over 50 mm (ESC also uses indexed LVESD over 25 mm per metre squared). [1]
Surgery should be considered (Class IIa) for:[1]
- Asymptomatic severe AR with LVESD 45 to 50 mm and declining EF on serial imaging or progressive LV dilation.
- Severe AR discovered during other cardiac surgery (CABG, mitral surgery).
- Aortic-root or ascending-aortic aneurysm with severe AR. [1]
Aortic-root and ascending-aorta replacement thresholds (independent of AR severity):[2]
- Marfan and heritable thoracic aortic aneurysm: over 50 mm (or 45 to 50 mm with risk factors — family history of dissection, rapid growth exceeding 3 mm per year, severe AR, desire for pregnancy).
- Bicuspid aortic valve aortopathy: over 55 mm (or over 50 mm with risk factors — family history of dissection, rapid growth, severe AR, desire for pregnancy).
- Degenerative aneurysm: over 55 mm (over 50 mm with risk factors or if intervention on another indication). [1]
When to operate in chronic severe AR
SOFA
any symptom (dyspnoea, angina, syncope) = AVR
EF 50 percent or below = AVR
LV end-systolic diameter over 50 mm = AVR (indexed over 25 mm/m2)
root/ascending aneurysm over 55 mm (over 50 with BAV; over 45-50 in Marfan with risk factors)
Operative options
The choice of operation is dictated by the mechanism (leaflet versus root), the patient's age and anticoagulation suitability, and centre expertise. [1]
| Procedure | Indication and rationale |
|---|---|
| Surgical AVR (mechanical or bioprosthetic) | Standard for irreversible leaflet disease (rheumatic, calcific, destroyed by endocarditis). Mechanical in younger patients (with lifelong anticoagulation); bioprosthetic in older patients or when anticoagulation is undesirable. |
| Valve-sparing aortic-root replacement (David procedure) | Aortic-root aneurysm with structurally normal leaflets — re-implant the native valve inside a Dacron graft. Avoids anticoagulation entirely; the operation of choice in Marfan and bicuspid aortopathy with preserved leaflets. |
| Ross procedure (pulmonary autograft to aortic position; pulmonary homograft to right ventricular outflow tract) | Children and young adults; the autograft is living tissue that grows with the patient and does not need anticoagulation. Technically demanding; concentrated in specialist centres. |
| TAVR / TAVI | Investigational / off-label for pure native AR; approved and standard for aortic stenosis in inoperable or high-risk patients. Newer dedicated AR devices are under study; not routine. |
| Repair (valvuloplasty, cusp plication, triangular resection) | Selected centres, suitable anatomy (e.g., bicuspid cusp prolapse, isolated perforation); durable in expert hands but technically demanding. |
Valve choice — mechanical versus bioprosthetic
A common NEET/INICET question. Mechanical valves (bileaflet, e.g., St Jude) are durable (lasting decades) but require lifelong warfarin with a target INR typically 2.5 in the aortic position (3.0 with additional risk factors such as atrial fibrillation, prior thromboembolism, hypercoagulable state, or older-generation valves). Bioprosthetic valves (bovine pericardial or porcine) do not need routine anticoagulation but have a limited lifespan (structural valve degeneration at roughly 10-15 years, faster in younger patients). Current guidance favours mechanical valves under about 60 years and bioprosthetic valves over 65 years, with the choice individualised in between based on anticoagulation suitability, patient preference, and the trade-off between bleeding risk and reoperation risk. Direct oral anticoagulants (DOACs) are absolutely contraindicated in mechanical valves — the RE-ALIGN trial showed increased thromboembolism and bleeding with dabigatran.[1]
Medical therapy (adjunctive, not definitive)
- Vasodilators / afterload reduction — ACE inhibitors or angiotensin-receptor blockers (ARBs) reduce afterload and regurgitant volume and are reasonable in patients with hypertension or heart-failure symptoms who decline or cannot have surgery. Nifedipine (extended-release) was historically used to delay surgery in asymptomatic severe AR, but modern evidence (the smaller, modernised trials) shows no clear benefit and it is no longer routinely recommended for this purpose. Hydralazine and other direct vasodilators are second-line.
- Diuretics (furosemide, spironolactone) and ACE inhibitors/ARBs for heart-failure symptoms while awaiting surgery.
- Beta-blockers — avoid as sole therapy in significant AR (bradycardia worsens regurgitation); use only for specific indications such as atrial fibrillation rate control, post-myocardial infarction, hypertension, or dissection. In Marfan syndrome, beta-blockade plus an ACE inhibitor/ARB (losartan) is standard to slow aortic-root growth independent of the AR.
- Sodium-glucose cotransporter-2 (SGLT2) inhibitors and other guideline-directed heart-failure therapy may be added for the heart-failure phenotype that AR eventually produces, but do not substitute for valve correction.
- Endocarditis prophylaxis — only for the highest-risk cardiac conditions (prosthetic valve, previous infective endocarditis, certain congenital heart disease — unrepaired cyanotic, repaired with prosthetic material in the first 6 months, repaired with residual defect adjacent to prosthetic material) before dental procedures manipulating the gingiva or periapical region. Routine native-valve AR does not warrant prophylaxis.[1]
Surveillance
Serial echocardiography drives management in the asymptomatic patient: mild AR every 3 to 5 years, moderate AR every 1 to 2 years, and severe asymptomatic AR every 6 to 12 months (more frequently if approaching the surgical threshold or with progressive LV dilation). Patients are counselled to report new symptoms immediately — symptomatic progression reclassifies them as surgical regardless of the last echo.[1]
Specific Subtypes & Scenarios
- Bicuspid aortic valve with AR — the commonest congenital cause; the bicuspid valve prolapses and wears prematurely, and is associated with aortic coarctation (Turner syndrome co-occurrence is classic) and an aortopathy of the root and ascending aorta that progresses independently of the valve lesion and needs independent surveillance and operative thresholds (root over 55 mm, or over 50 mm with risk factors).
- Rheumatic AR — leaflet scarring and retraction typically produces mixed aortic disease (AS plus AR) and almost always coexists with mitral stenosis in endemic regions; the murmur is high-pitched and may carry a systolic component from associated stenosis.
- Marfan syndrome and heritable thoracic aortic aneurysm — root dilation with structurally normal leaflets is the ideal substrate for a valve-sparing David procedure; intervene on the aorta at lower thresholds than degenerative disease (over 50 mm, or 45 to 50 mm with risk factors). Loeys-Dietz and vascular Ehlers-Danlos carry even more aggressive aortic behaviour and lower thresholds.
- Infective endocarditis with acute AR — destruction, perforation or a vegetation preventing coaptation of a cusp causes acute AR; early surgery is indicated for heart failure, perivalvular abscess/heart block, or large mobile vegetations regardless of antibiotic duration. Heart failure in endocarditis AR is itself a surgical indication.
- Type A dissection with AR — the dissection flap detaches the commissure and prolapses a cusp, producing acute AR; emergency repair involves resuspension of the commissures, often with root replacement.
- Prosthetic valve dysfunction or paravalvular leak — new AR in a patient with a prosthetic valve suggests dehiscence, prosthetic-valve endocarditis, or structural valve degeneration; TOE is diagnostic and revision surgery may be required.
- Seronegative spondyloarthropathy (ankylosing spondylitis) — aortitis of the ascending aorta causes root dilation and AR; may coexist with conduction disease and aortic regurgitation that progresses even after valve replacement if the root is not addressed.
- Tertiary syphilis — luetic aortitis of the thoracic ascending aorta produces a tree-bark intimal appearance and an aneurysm that, characteristically, spares the sinuses of Valsalva (unlike other aortitides which involve the sinuses), with a normal-appearing valve pulled apart by the dilated supracoronary aorta. [1]
Complications & Pitfalls
Complications of untreated or advanced AR:[3]
- Left ventricular systolic dysfunction and heart failure — the cardinal and often irreversible complication if surgery is delayed beyond the point of LV decompensation; EF may not recover even after a technically perfect AVR once it has been below 30 percent for a sustained period.
- Infective endocarditis — diseased native and prosthetic valves carry higher risk; this is the rationale for selective prophylaxis in prosthetic valves.
- Atrial fibrillation (from left atrial stretch as LV filling pressure rises) and ventricular arrhythmias (ventricular tachycardia, fibrillation) in advanced disease with dilated cardiomyopathy.
- Sudden cardiac death — uncommon but reported in severe symptomatic disease, principally from ventricular arrhythmia.
- Aortic dissection or rupture in root-aneurysm disease (Marfan, Loeys-Dietz, bicuspid aortopathy) — the rationale for prophylactic aortic surgery at size thresholds.
- Surgical and prosthetic complications — paravalvular leak, prosthetic-valve endocarditis, structural valve degeneration (bioprosthetic), anticoagulant-related bleeding or valve thrombosis (mechanical), complete heart block (aortic valve surgery sits beneath the bundle of His), and reoperation risk. [1]
Classic pitfalls (examiner favourites): [1]
- Missing asymptomatic LV dysfunction by failing to perform serial echocardiography in "well-tolerated" severe AR — by the time symptoms appear, EF may not recover after AVR.
- Relying on murmur loudness — severity correlates inversely with murmur duration in acute AR; a soft short murmur may signal the worst disease.
- Using an IABP in significant AR — absolutely contraindicated.
- Overlooking the aortic root — operating only on the valve when a dilated root will continue to enlarge and dissect after isolated AVR; root dimensions must always be measured and reported.
- Confusing Graham Steell murmur (pulmonary regurgitation from pulmonary hypertension) with AR — check for signs of pulmonary hypertension (loud P2, RV heave, elevated JVP).
- Treating Austin Flint murmur as independent organic mitral stenosis and missing the underlying AR (no opening snap, no loud S1).
- Delaying surgery in endocarditis AR for an arbitrary antibiotic course — heart failure from AR in endocarditis is itself a surgical indication. [1]
Prognosis & Disposition
Asymptomatic severe AR with normal LV function has an excellent short-term prognosis — mortality under 0.2 percent per year, and progression to symptoms or LV dysfunction at a rate of roughly 3.5 percent per year. Risk rises with older age, LVESD over 50 mm, LVEDD over 70 mm, and a falling EF. Once symptoms develop, untreated severe AR carries mortality exceeding 10 percent per year — symptomatic severe AR is a surgical disease.[1][3]
After AVR, prognosis is good if surgery precedes irreversible LV dysfunction; EF and symptoms often improve substantially when EF was 30 to 50 percent at the time of operation. Recovery of EF is poor once EF has been below 30 percent for a sustained period, which is exactly why surgery is timed before that point is reached. Mechanical-valve patients need lifelong warfarin with its attendant bleeding and thrombosis trade-off; bioprosthetic-valve patients face reoperation for structural degeneration (roughly 10-15 years, faster in younger patients).[1]
Disposition: asymptomatic mild-to-moderate AR is managed in the outpatient setting with surveillance echo at the intervals above; asymptomatic severe AR requires close (6 to 12 monthly) echo follow-up and patient education about symptoms to report; symptomatic severe AR or AR meeting surgical thresholds warrants cardiology and cardiothoracic surgical referral; acute severe AR is admitted to a critical-care or HDU setting pending emergency surgery. [1]
Special Populations
- Pregnancy — chronic stable AR is generally well tolerated because pregnancy's tachycardia and reduced systemic vascular resistance both reduce regurgitant volume. Manage jointly with an obstetric-cardiology service; beta-blockers may be used cautiously if needed. Acute decompensation or symptomatic severe AR pre-pregnancy warrants pre-pregnancy valve surgery (preferably valve-sparing or bioprosthetic to avoid warfarin, which is teratogenic in the first trimester and causes fetal bleeding near term).
- Elderly — degenerative/calcific and mixed lesions dominate; the stiff, non-compliant LV decompensates at smaller regurgitant volumes. Consider surgical risk scores (STS, EuroSCORE) and TAVR (still investigational for pure AR) in the inoperable, and a multidisciplinary heart-team decision.
- Athletes — mild LV dilation from athletic remodelling ("athlete's heart") must be distinguished from pathological AR by echo (chamber dimensions, wall thickness, valve morphology, regurgitant fraction, reversal of findings with deconditioning). Severe AR is a contraindication to competitive sport.
- Marfan syndrome and heritable thoracic aortic disease — initiate beta-blocker and/or losartan from diagnosis, lifelong surveillance of the aorta, and lower operative thresholds (over 50 mm, or 45 to 50 mm with risk factors). Pregnancy in Marfan carries dissection risk when the aorta exceeds 40 mm.
- Bicuspid aortic valve — surveillance of the root and ascending aorta independent of the valve, because the aortopathy progresses even when the valve is replaced; a combined valve-and-root decision is made at surgery.
- Anticoagulated after mechanical AVR — warfarin with target INR typically 2.5 in the aortic position (3.0 with risk factors); DOACs are contraindicated; bridge with heparin for invasive procedures; manage vitamin-K interactions (diet, antibiotics, amiodarone).
- Children and young adults — Ross procedure (pulmonary autograft) or valve-sparing repair is favoured to avoid a prosthetic valve and lifelong anticoagulation in a growing patient; the autograft grows with the child. [1]
Evidence, Guidelines & Regional Differences
- ACC/AHA 2020 Guideline for the Management of Patients With Valvular Heart Disease (Otto et al.) — the North American standard; sets the surgical thresholds (symptomatic; EF 50 percent or below; LVESD over 50 mm).
- ESC/EACTS 2021 Guidelines for the management of valvular heart disease (Vahanian et al.) — the European standard; broadly concordant, and adds the indexed LVESD over 25 mm per metre squared to account for body size.
- ASE recommendations on quantitation of native valvular regurgitation (Zoghbi et al., 2003) — the reference for echo severity parameters (jet width, vena contracta, EROA, regurgitant volume and fraction). [1]
Key thresholds that examiners reward: EF 50 percent, LVESD 50 mm (indexed 25 mm per metre squared), aortic-root aneurysm 55 mm (50 mm in bicuspid; 45 to 50 mm in Marfan with risk factors). These three numbers — 50, 50, 55 — answer most surgical-timing MCQs.[1][2]
The IABP contraindication in significant AR is an absolute, repeatedly tested fact. [1]
[1]Regional and procedural deltas: the mechanical-versus-bioprosthetic choice varies by age, anticoagulation suitability, patient preference, and local resources; in resource-limited settings rheumatic mixed-valve disease dominates and mechanical valves are common because of younger age at presentation and the durability needs of a patient who may not have reliable access to reoperation. Valve-sparing root replacement (David procedure) and the Ross procedure are concentrated in specialised centres and require surgical expertise not available everywhere. Nifedipine, once a popular afterload-reducer in asymptomatic severe AR, is no longer recommended for delaying surgery on the basis of more recent trial data, though the practice persists in older textbooks.[1][1]
Exam Pearls
- Murmur: early-diastolic, high-pitched, blowing, decrescendo, best heard at the left 3rd intercostal space (Erb point) with the diaphragm, patient sitting forward, breath held in expiration; right 2nd ICS if root disease.
- Austin Flint murmur = apical mid-diastolic rumble from the AR jet striking the anterior mitral leaflet (functional MS; no opening snap, no loud S1).
- Wide pulse pressure with a water-hammer (Corrigan) pulse and a hyperdynamic displaced apex = chronic severe AR.
- Peripheral signs mnemonic: Corrigan, de Musset, Quincke, Traube (pistol-shot), Duroziez, Hill (leg SBP exceeds arm by over 20 mmHg), Mueller (uvula), Becker (retinal).
- Eccentric hypertrophy (volume overload, sarcomeres in series) distinguishes AR from the concentric hypertrophy of AS (pressure overload, sarcomeres in parallel).
- AVR when: symptomatic; EF 50 percent or below; LVESD over 50 mm (indexed over 25 mm per m squared); root over 55 mm (50 mm BAV; 45 to 50 mm Marfan with risk factors).
- NEVER use an IABP in significant AR — drives more blood back into the LV.
- Acute AR (endocarditis, dissection, trauma) — peripheral signs absent, murmur soft/short, emergency surgery.
- Graham Steell murmur is pulmonary regurgitation (pulmonary hypertension, loud P2) — the key differential of the AR murmur.
- Tertiary syphilis causes luetic aortitis of the ascending aorta that spares the sinuses (unlike other aortitides).
- Mechanical valves need lifelong warfarin (INR ~2.5); DOACs are contraindicated (RE-ALIGN trial).
- Surgical thresholds = 50, 50, 55: EF 50 percent, LVESD 50 mm, root 55 mm. [1]
Exam application bank (NEET-PG / INICET)
One-line answer
Aortic regurgitation (AR) is diastolic incompetence of the aortic-valve complex permitting backflow from the aorta into the left ventricle. In chronic AR the LV remodels by eccentric hypertrophy, giving the classic signs — early-diastolic decrescendo murmur at Erb point, wide pulse pressure, water-hammer (Corrigan) pulse and a constellation of peripheral signs (de Musset, Quincke, Traube, Duroziez, Hill). Causes are leaflet disease (rheumatic, bicuspid, endocarditis) or aortic-root dilation (Marfan, hypertension, ankylosing spondylitis, syphilis). Acute severe AR (endocarditis, type A dissection, trauma) presents as sudden pulmonary oedema without the classic signs. Diagnosis is by echocardiography, which grades severity (regurgitant volume, fraction, EROA, vena contracta). Definitive treatment is aortic valve surgery (AVR) when symptomatic, when EF is 50 percent or below, or when LV end
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard. [1]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes. [1]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change. [1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each. [1]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory. [1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Aortic Regurgitation.
References
- [1]Otto CM, Nishimura RA, Bonow RO, et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines J Am Coll Cardiol, 2021.PMID 33342587
- [2]Vahanian A, Beyersdorf F, Praz F, et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease Eur Heart J, 2022.PMID 34453165
- [3]Bekeredjian R, Grayburn PA. Valvular heart disease: aortic regurgitation Circulation, 2005.PMID 15998697
- [4]Zoghbi WA, Enriquez-Sarano M, Foster E, et al. Recommendations for evaluation of the severity of native valvular regurgitation with two-dimensional and Doppler echocardiography J Am Soc Echocardiogr, 2003.PMID 12835667
- [5]Bonow RO, Carabello BA, Chatterjee K, et al. 2008 Focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1998 Guidelines for the Management of Patients With Valvular Heart Disease): endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons Circulation, 2008.PMID 18820172