Cardiology · Cardiology
Chronic Coronary Syndrome
Also known as Stable angina · Stable ischaemic heart disease · SIHD · Stable angina pectoris · Chronic coronary disease
Chronic coronary syndrome (CCS) is the modern umbrella term replacing "stable angina" for the long-term presentations of coronary artery disease. Defined by the 2019 ESC Guidelines as the spectrum of clinical presentations driven by chronic, often predictable, myocardial ischaemia typically precipitated by exertion or emotional stress and relieved by rest or sublingual nitrates. Anatomically it is the consequence of fixed or dynamic epicardial coronary stenosis (atherosclerotic plaque with intact fibrous cap), microvascular dysfunction, or vasospasm. The classic presentation is substernal chest discomfort provoked by exertion, lasting under 10 minutes, and relieved by rest or nitroglycerin (CCS grade I-IV / Canadian Cardiovascular Society grading). Diagnosis is clinical plus exclusion of ACS (serial hs-troponin negative, no dynamic ST-T changes); risk stratification uses pre-test probability, coronary CT angiography or functional stress imaging, with invasive angiography reserved for high event risk or refractory symptoms. Management rests on four pillars: (1) disease-modifying secondary prevention (aspirin, high-intensity statin with LDL target below 1.4 mmol/L in very high risk, ACE inhibitor where indicated), (2) symptom control (beta-blocker or calcium-channel blocker first-line, nitrates for acute relief, ranolazine/ivabradine second-line), (3) lifestyle and risk-factor modification, and (4) revascularisation for prognostic left-main/multivessel disease or refractory angina despite optimal medical therapy.
On this page & tools
Your progress
Saved locally on this device.
Exam tags
Red flags

Overview & Definition
Chronic coronary syndrome (CCS) is the umbrella term introduced by the 2019 ESC Guidelines on the Diagnosis and Management of Chronic Coronary Syndromes to replace the older binary "stable angina / unstable angina" nomenclature.[1] The concept recognises that coronary artery disease is not a single event but a dynamic continuum, and that patients move between phases of stability and instability along a lifelong trajectory.
The 2019 ESC definition frames CCS as the spectrum of clinical presentations driven by chronic, often predictable, myocardial ischaemia, typically precipitated by exertion or emotional stress and improved by rest or sublingual nitrates — distinct from the acute coronary syndromes (ACS) that arise from acute plaque rupture, thrombosis, and abrupt coronary occlusion.[1] The terminology unifies what were previously six discrete "presentations of stable coronary artery disease" in the 2013 ESC guideline into a single, evolving entity.
CCS encompasses six clinical scenarios listed in the 2019 ESC document:[1]
- Patients with suspected coronary artery disease and "stable" anginal symptoms, with or without dyspnoea.
- Patients with new-onset heart failure or left ventricular dysfunction and suspected CAD (including silent ischaemia).
- Patients with stabilised symptoms after an ACS (after the acute phase has resolved and the patient is on guideline-directed therapy).
- Patients one year or more after revascularisation, with stable symptoms or silent ischaemia.
- Patients with angina and non-obstructive coronary arteries (INOCA) — ischaemia with documented supply-demand mismatch but no flow-limiting epicardial stenosis.
- Patients with silent ischaemia documented on provocative testing.[4]
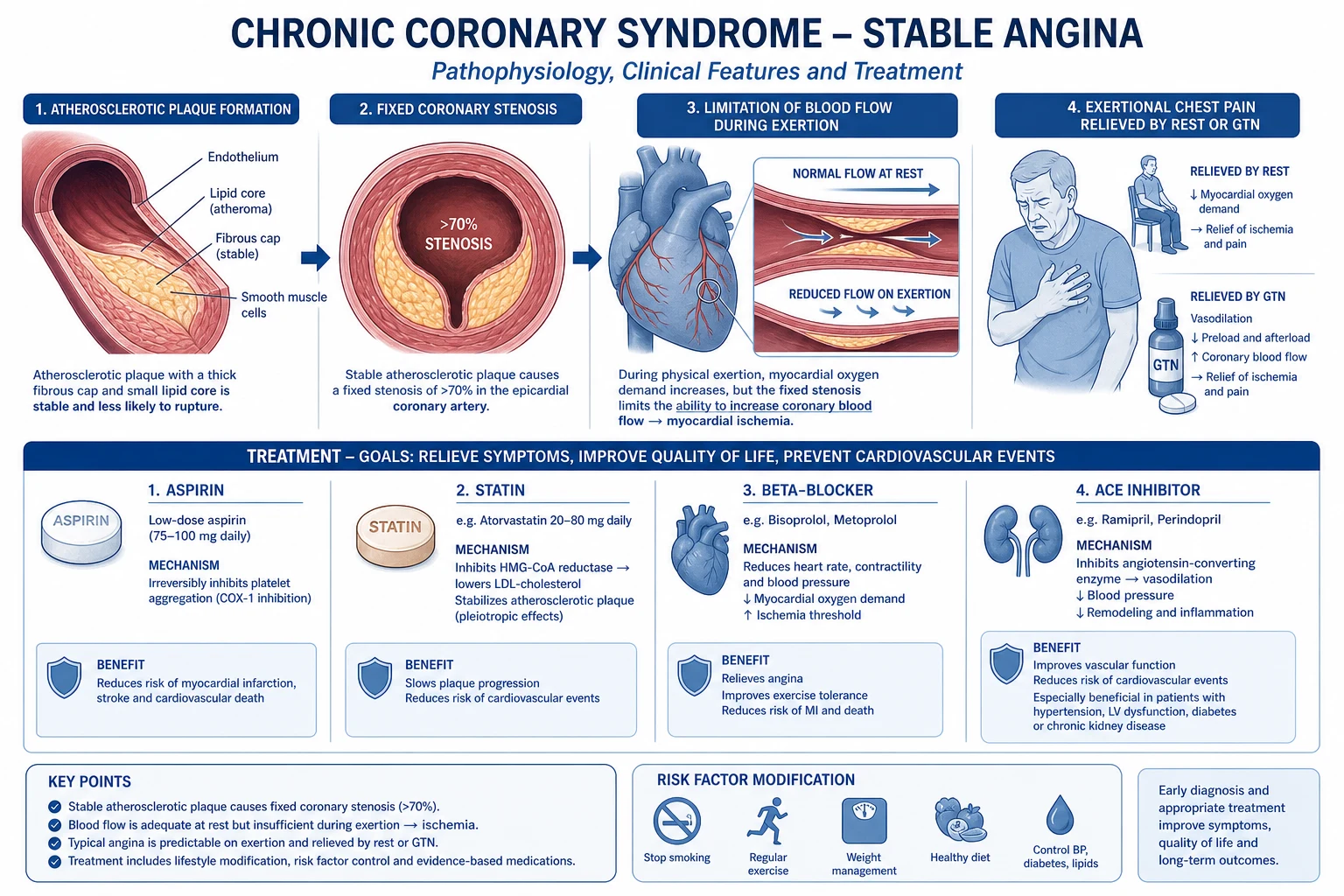
The anatomical substrate in classic CCS is a fixed atherosclerotic stenosis of one or more epicardial coronary arteries, with an intact fibrous cap, in which the lumen is sufficiently narrowed that myocardial oxygen demand during exertion exceeds supply. The physiological substrate is the supply-demand mismatch between myocardial oxygen demand (driven by heart rate, contractility, wall tension) and supply (coronary flow, which is limited by the stenotic segment and by coronary vasodilator reserve).[4]
The therapeutic objectives in CCS are threefold: (1) prognosis improvement — prevention of myocardial infarction, stroke, and cardiovascular death through anti-atherosclerotic therapy (antiplatelet, lipid-lowering, RAAS blockade); (2) symptom relief — anti-anginal therapy and revascularisation when needed; (3) preservation of function — secondary prevention and rehabilitation to maintain activity, cardiac function, and quality of life.[2]
The annual mortality of CCS varies enormously with risk profile. In contemporary registries, all-cause mortality ranges from under 1 percent per year in low-risk stable outpatients to over 5 percent per year in those with severe ischaemia, heart failure, diabetes, or CKD — emphasising the need for risk stratification rather than a one-size-fits-all approach.[3]
Classification
CCS is classified in three complementary ways: by clinical severity (CCS grading), by pathophysiology (anatomical vs functional obstruction), and by risk (low / intermediate / high — used to decide on invasive investigation).[3]
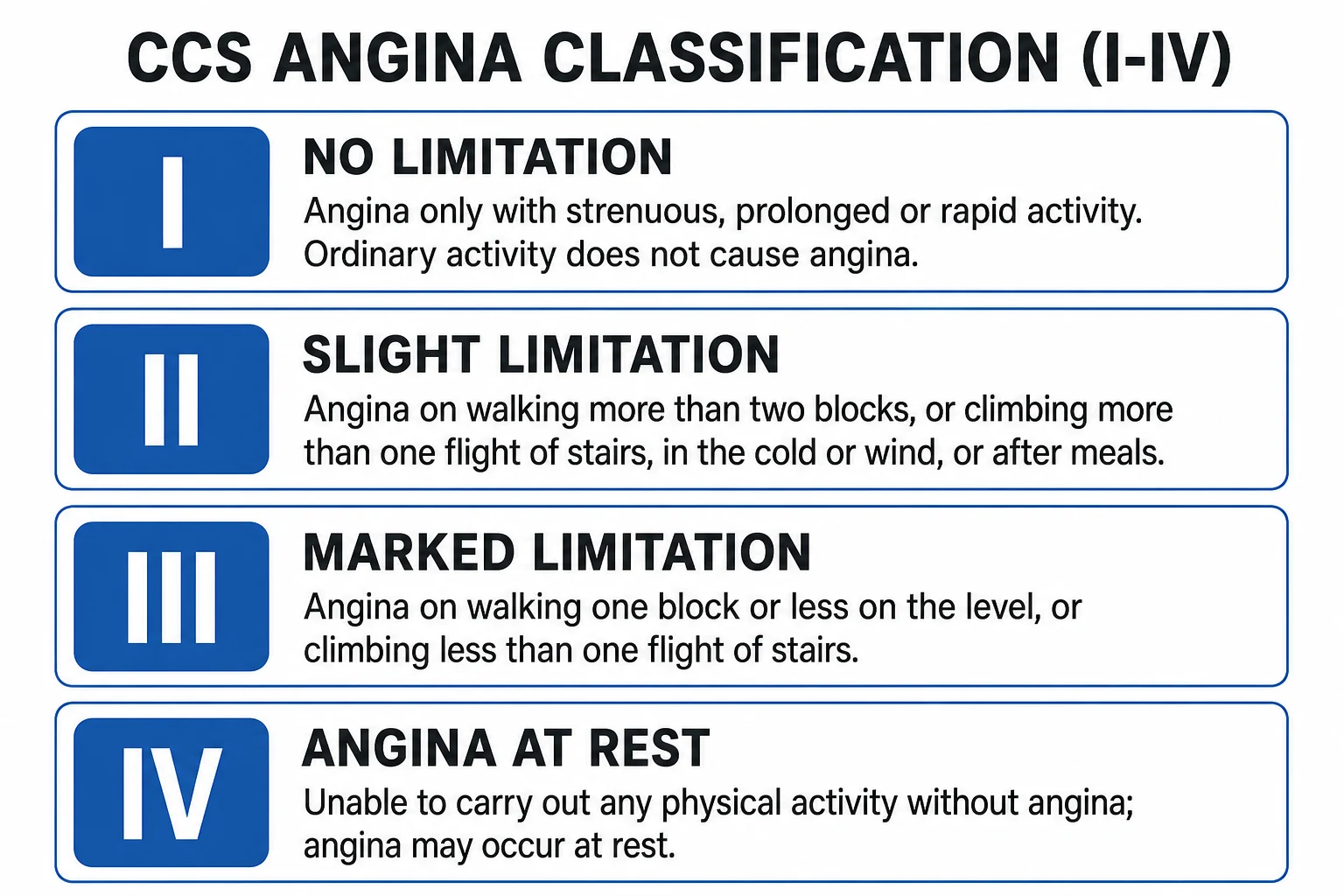
1. Canadian Cardiovascular Society (CCS) Angina Grading — the bedside severity scale. This patient-reported functional scale has been the clinical lingua franca since 1976 and is required in the workup of every CCS topic.[7]
CCS grade and clinical implication
- CCS I — Ordinary physical activity (walking, climbing stairs) does NOT cause angina; angina appears with strenuous, rapid, or prolonged exertion.
- CCS II — Slight limitation of ordinary activity; angina with walking or climbing stairs rapidly, in cold, emotional stress, or after a meal. Walking more than 100 to 200 m on the flat or climbing more than one flight of stairs provokes symptoms.
- CCS III — Marked limitation of ordinary activity; angina with walking 100 to 200 m on the flat or climbing one flight of stairs.
- CCS IV — Angina at rest or with any physical activity; unable to carry on any physical activity without discomfort; often indicates unstable angina or imminent ACS.
A practical refinement, the NYHA functional class (used for heart failure), is often used alongside CCS class when there is concurrent LV dysfunction.[1]
2. Pathophysiological classification — anatomical vs functional:[1]
- Anatomical (obstructive) CAD — fixed epicardial stenosis of a major coronary artery, typically above 50 to 70 percent diameter reduction. The "classic" substrate of stable angina.
- Functional microvascular angina (microvascular CAD) — anginal symptoms with ischaemic ECG changes on stress testing but no epicardial stenosis on angiography; due to coronary microvascular dysfunction (CMD), impaired coronary flow reserve, often in women and in patients with diabetes and hypertension.
- Vasospastic (Prinzmetal) angina — focal or diffuse epicardial coronary spasm causing transient transmural ischaemia. May be associated with atherosclerotic plaque or occur in near-normal vessels. Diagnosis by acetylcholine or ergonovine provocation test during angiography.
- Mixed forms — variable combinations of fixed stenosis, microvascular dysfunction, and vasospasm; increasingly recognised by intracoronary physiology and provocative testing.[4]
3. Anatomical disease burden — based on invasive angiography or CTCA:[1]
- One-vessel disease — isolated proximal LAD, LCx, or RCA stenosis.
- Two-vessel disease — combinations, of which proximal LAD involvement escalates risk.
- Three-vessel disease — multivessel disease, particularly with proximal LAD or left main involvement.
- Left main disease — the highest anatomical risk; usually a revascularisation indication (CABG preferred by trial evidence; PCI increasingly used in selected low surgical-risk cases).
- No-obstructive disease — under 50 percent epicardial stenosis on angiography but symptoms or ischaemia present (INOCA).[4]
4. Risk classification (to drive investigation strategy): The 2019 ESC guideline recommends pre-test probability modelling (using age, sex, symptom character) plus clinical risk modifiers (diabetes, CKD, LV dysfunction, abnormal resting ECG, prior revascularisation) to assign patients to low, intermediate, or high pre-test probability and to direct them to either functional testing (stress echo / MRI / MPS), anatomical testing (CTCA), or direct invasive evaluation.[3]
Epidemiology & Risk Factors
CCS is the commonest manifestation of ischaemic heart disease and the leading cause of stable outpatient cardiology consultations in adults over 40. The global prevalence of stable CAD is in the order of 20 to 40 per 1,000 adults depending on age and region, with higher rates in high-income populations, the elderly, and certain ethnic groups (South Asian, Afro-Caribbean).[1]
Age-specific prevalence increases steeply after 45 years in men and after 55 years in women; male sex confers roughly a 2 to 3-fold higher age-adjusted risk until the seventh decade, after which female prevalence catches up. In contemporary practice, women present later, with more atypical features, and have higher rates of INOCA than obstructive CAD.[1]
Non-modifiable risk factors:[1]
- Age — the dominant predictor; prevalence doubles every decade after age 45.
- Male sex — earlier onset and roughly twice the age-adjusted risk until menopause.
- Family history of premature CAD: first-degree male relative with CAD below 55 or female relative below 65; doubles risk.
- Genetics — polygenic risk scores contribute meaningfully; rare monogenic lipid disorders (familial hypercholesterolaemia) accelerate disease by decades.[6]
Modifiable risk factors (the "interventional targets"):[1]
- Dyslipidaemia — elevated LDL-C, low HDL-C, elevated lipoprotein(a). Each 1 mmol/L rise in LDL-C raises CAD risk by roughly 50 percent at age 40; statins and ezetimibe / PCSK9 inhibition reduce events.
- Hypertension — systolic and pulse pressure both drive endothelial injury and atherogenesis; tight control reduces coronary events.
- Diabetes mellitus — both type 1 and type 2; accelerates atherosclerosis, predisposes to multivessel disease and silent ischaemia.
- Tobacco smoking — current > former; dose-response with pack-years; secondhand exposure increases risk by 25 to 30 percent.
- Obesity — central adiposity (waist circumference, visceral fat); mediator through insulin resistance, hypertension, dyslipidaemia, inflammation.
- Physical inactivity — sedentary lifestyle roughly doubles CAD risk; structured exercise confers a 20 to 30 percent relative-risk reduction.
- Diet — high saturated fat, trans-fat, refined carbohydrate, sodium, low fruit and vegetable intake.
- Alcohol — J-shaped relationship with CAD; excess alcohol raises triglycerides and BP.
- Psychosocial factors — chronic stress, depression, social isolation, shift work; modest independent effect.
- Chronic kidney disease — both a risk marker and a risk multiplier; calcific atherosclerosis.
- Autoimmune inflammatory disease — rheumatoid arthritis, SLE, psoriasis; chronic systemic inflammation.[6]
Calculating absolute risk. In primary prevention, the SCORE2 (Europe) and PREVENT (US) equations use age, sex, smoking, BP, non-HDL-C, and (for PREVENT) diabetes and kidney function to estimate the 10-year cardiovascular risk, which then informs intensity of lipid and BP targets. In patients with established CCS the risk is by definition high, and the focus shifts from prediction to aggressive secondary prevention.[1]
Pathophysiology
The pathophysiology of CCS rests on three interlinked pillars: atherosclerosis, plaque stability, and the supply-demand mismatch that triggers ischaemia and symptoms.[1]
1. Atherosclerosis — the lesion and its evolution. Coronary atherosclerosis begins in childhood (fatty streaks in the intima) and progresses over decades through fatty-streak, intermediate, fibrous-plaque, and complicated-plaque stages. It is driven by endothelial injury (BP, smoking, glucose, LDL), LDL infiltration and retention in the intima, oxidative modification, monocyte recruitment and foam-cell formation, smooth-muscle migration, and fibrous-cap formation. The hallmark lesion of stable CAD is a fibrofatty plaque with an intact, thick fibrous cap overlying a necrotic lipid core — a lesion that has been remodeled and stabilised over years.[1]
2. Plaque stability determines clinical presentation.[1]
- Stable plaques — thick fibrous cap, small lipid core, calcification predominates; produce fixed stenosis and predictable, exertion-related symptoms.
- Vulnerable plaques — thin-cap fibroatheroma, large lipid core, dense macrophage infiltrate, neovascularisation; prone to rupture or erosion, with platelet activation, thrombosis, and the abrupt vessel occlusion that drives ACS.[4]
The transition from stable to unstable disease underpins the ESC's reframing of CCS as a continuum: plaques do change over time, and a patient with stable angina today is one plaque rupture away from ACS tomorrow.[6]
3. Supply-demand mismatch on exertion.[1]
Myocardial oxygen demand is determined by heart rate, contractility, and wall stress (preload, afterload). Supply is determined by coronary blood flow, which depends on perfusion pressure, diastolic time (coronary flow is largely diastolic), and coronary vascular resistance. In a healthy artery, autoregulation maintains flow over a wide perfusion-pressure range. As stenosis narrows the lumen, distal resistance rises and the coronary flow reserve is exhausted at lower levels of demand — meaning that small increases in heart rate, inotropy, or wall stress during exertion produce ischaemia.[4]
Ischaemia cascade. During exercise in a patient with fixed stenosis:[4]
- Flow heterogeneity between ischaemic and normal territories — earliest sign, can be detected by myocardial perfusion imaging.
- Diastolic dysfunction — impaired relaxation of ischaemic segments.
- Regional wall motion abnormality — hypokinesia or akinesia on stress echo.
- ECG changes — ST depression (subendocardial ischaemia) or, less commonly, ST elevation (transmural ischaemia).
- Chest discomfort — angina, often preceded by the other findings by seconds to minutes.[4]
4. Stable angina physiology. The classic pattern is exertional substernal discomfort (or pressure, heaviness, squeezing) precipitated by increased myocardial oxygen demand (exertion, emotion, cold, post-prandial state) and relieved by reducing demand (rest) or increasing supply (nitrates). The reproducible threshold (e.g. "five flights of stairs reliably brings it on") is the marker of fixed stenosis as opposed to vasospasm or microvascular disease.[4]
5. Endothelial dysfunction and microvascular angina. In patients with INOCA, the epicardial arteries are often angiographically normal but the microcirculation (arterioles under 500 micrometres) is dysfunctional, with impaired flow reserve, increased vasoconstriction, and patchy ischaemia on stress testing. Up to half of women and a third of men undergoing elective angiography for typical chest pain have non-obstructive CAD, and a substantial proportion have demonstrable microvascular dysfunction.[1]
6. Coronary vasospasm. Prinzmetal angina is driven by focal or diffuse epicardial spasm, often without significant fixed atherosclerosis. Mechanisms include endothelial dysfunction, autonomic dysregulation, and heightened vascular smooth-muscle reactivity to vasoconstrictors. Spasm may occur at a fixed atherosclerotic site, producing mixed presentations.[6]
7. Plaque progression, regression, and the role of therapy. Statins stabilise plaques (reduce lipid core, thicken fibrous cap), improve endothelial function, lower LDL-C, and reduce events. ACE inhibitors lower vascular resistance, improve endothelial function, and reduce adverse remodelling post-MI. Antiplatelet therapy reduces thrombus formation on eroded or ruptured plaques. Lifestyle modification and risk-factor control address the upstream drivers.[2]
Clinical Presentation
The clinical presentation of CCS varies enormously, and recognition depends on probability-adjusted history-taking rather than textbook descriptors alone. Roughly 80 to 90 percent of patients have chest pain or discomfort, but up to a third in women, the elderly, and diabetics have anginal equivalents — dyspnoea, fatigue, epigastric discomfort, nausea, or isolated exertional fatigue.[1]
Typical angina (high specificity, roughly 90 to 95 percent for obstructive CAD in middle-aged men):[1]
- Substernal chest discomfort (pressure, heaviness, squeezing, burning, not usually described as "pain").
- Provoked by exertion or emotional stress, cold, after meals.
- Relieved by rest or sublingual nitroglycerin within minutes (usually under 5 minutes).
- Lasting under 10 minutes by definition for stable disease (longer suggests ACS).[7]
Atypical chest pain (lower specificity, but most chest pain that is not obviously musculoskeletal is investigated for CAD until proven otherwise): pain located outside the substernal region, not clearly related to exertion, not relieved by nitrates, or described as sharp, pleuritic, or positional.[1]
Anginal equivalents (especially in women, elderly, diabetics): exertional dyspnoea, fatigue, epigastric discomfort, light-headedness, nausea, or isolated exercise-induced deconditioning.[1]
Canadian Cardiovascular Society (CCS) angina classification:[7]
- CCS I — Ordinary physical activity does not cause angina; only strenuous, rapid, or prolonged exertion does.
- CCS II — Slight limitation of ordinary activity; angina on rapid climbing, walking uphill, after meals, in cold or emotion.
- CCS III — Marked limitation; angina on walking 100 to 200 m on the flat or climbing one flight of stairs.
- CCS IV — Angina at rest or with any activity.[6]
Silent ischaemia. Common in diabetics (cardiac autonomic dysfunction), the elderly, and post-CABG patients. Documented by ECG changes (ambulatory ST monitoring, stress test) without symptoms; carries the same prognostic weight as symptomatic ischaemia. Prevalence rises with multivessel disease, prior MI, and CKD.[1]
Associated symptoms to ask about: dyspnoea (concurrent HF or extensive ischaemia), palpitations (arrhythmia), syncope or presyncope (life-threatening ischaemia or arrhythmia), fatigue, peripheral oedema (right HF secondary to LV dysfunction), and orthopnoea / paroxysmal nocturnal dyspnoea (elevated LV filling pressures).[1]
Risk-factor history is integral — smoking (current or past, pack-years), diabetes (type and control), hypertension, dyslipidaemia, family history of premature CAD, prior events (MI, stroke, PCI, CABG), medications (statins, anti-platelets, anti-hypertensives, contraception).[2]
Differential Diagnosis
The diagnosis of CCS is fundamentally clinical — based on the history of characteristic chest discomfort relieved by rest or nitrates — but the differential of non-cardiac causes of chest pain (and the cardiac mimics within CCS) is what the examiner assesses.[1]
Differential of anginal chest pain:[1]
- Oesophageal causes — gastro-oesophageal reflux disease (burning, positional, post-prandial, nocturnal); oesophageal spasm (may mimic angina, including transient ST changes). Trial of PPI and ambulatory pH monitoring often separates them.
- Musculoskeletal chest pain — costochondritis (Tietze syndrome, reproducible tenderness on palpation), intercostal neuralgia, pectoral strain, cervical radiculopathy. Usually positional and reproducible on examination.
- Anxiety, panic disorder, and hyperventilation — chest tightness, air hunger, perioral tingling, light-headedness; young patients, often with normal investigation. Pickup of autonomic symptoms, situational triggers.
- Pulmonary causes — pulmonary embolism (pleuritic, dyspnoeic, hypoxia), pneumothorax (sudden pleuritic and dyspnoeic), pneumonia or pleuritis (fever, cough, pleuritic features).
- Aortic dissection — sudden severe "tearing" chest or back pain, pulse deficit, BP differential between arms, mediastinal widening on CXR.
- Pericarditis — pleuritic, positional, friction rub, diffuse concave-upward ST elevation with PR depression.
- Mitral valve prolapse — atypical chest pain, palpitations, mid-systolic click.
- Microvascular angina (INOCA) — typical anginal symptoms with positive stress test but no obstructive epicardial stenosis on angiography; the diagnosis rather than a differential.
- Vasospastic (Prinzmetal) angina — often rest pain (nocturnal, early morning), transient ST elevation, normal exercise capacity; confirmed with intracoronary acetylcholine challenge.[1]
Differential of silent ischaemia equivalents: dyspnoea on exertion in a smoker may reflect COPD, anaemia, deconditioning, diastolic dysfunction, or HF; the workup must include ECG and, when pre-test probability is sufficient, stress imaging.[1]
Exclusion of ACS. Any patient presenting with new-onset chest pain at rest, crescendo angina, prolonged pain above 20 minutes, or dynamic ECG changes should be evaluated as suspected ACS through the universal chest-pain pathway — high-sensitivity troponin, repeat ECG, risk stratification (GRACE, HEART) — irrespective of CCS history.[2]
Clinical & Bedside Assessment
1. The history remains the cornerstone of the diagnosis. Pre-test probability of obstructive CAD is estimated by combining age, sex, and symptom character (typical, atypical, non-anginal) using the 2019 ESC diamond-modified model.[1] Effective communication is essential: ask the patient to describe the symptom in their own words before ticking boxes.
Key history elements:[1]
- Symptom character (substernal? pressure or pain? provoked by exertion? relieved by rest or nitrates?).
- Duration of each episode and total symptom duration in weeks to months.
- Provoking factors — exertion type and threshold, emotion, cold, meals.
- Relieving factors — rest, nitrates (and how quickly), posture.
- Associated symptoms — dyspnoea, palpitation, syncope, sweating, nausea.
- Functional impact — CCS class, what the patient can and cannot do, days off work.
- Risk factor inventory — smoking, diabetes, hypertension, lipid profile, family history, kidney disease, prior vascular events.
- Medication review — antianginals currently and previously, anti-hypertensives, lipid-lowering agents, contraception, recent medication changes.
- Comorbidities and their treatment — especially CKD, atrial fibrillation, anticoagulation, COPD, anaemia, peripheral arterial disease.
- Psychosocial and cultural context — exercise habits, dietary patterns, language and literacy, health beliefs, access to care.[1]
2. Targeted examination. Often normal between episodes. The aim is to elicit cardiovascular risk markers and end-organ damage, not to confirm ischaemia per se.[1]
- Vital signs — BP in both arms (suggests subclavian or aortic disease), resting heart rate, rhythm.
- General — obesity, central adiposity, xanthelasma, corneal arcus, skin stigmata.
- Carotid, abdominal, and femoral bruits — diffuse atherosclerosis.
- Cardiovascular — apex beat (laterally displaced cardiomegaly), S3 or S4 (LV dysfunction), murmurs (aortic stenosis — a key mimic; mitral regurgitation — papillary muscle dysfunction).
- Respiratory — bibasal crackles (pulmonary oedema); air entry (pneumothorax, effusion).
- Peripheral pulses — dorsalis pedis, posterior tibial, popliteal; document any peripheral arterial disease.
- Abdomen — hepatomegaly (right HF), pulsatile mass (aortic aneurysm).
- Ankle-brachial pressure index (ABPI) — if symptoms of leg claudication coexist; an ABPI below 0.9 confirms PAD.[4]
3. Initial bedside tests. Resting 12-lead ECG, pulse oximetry, finger-prick glucose, capillary haemoglobin / point-of-care troponin if pain at rest.[3]
Investigations
Investigation in CCS serves three purposes: (1) confirm the diagnosis, (2) stratify risk and quantify ischaemic burden, and (3) identify candidates for revascularisation.[1] The 2019 ESC guideline emphasises pre-test probability-based selection of the first test — functional versus anatomical — to avoid low-yield testing and incidental findings.
Step 1 — Baseline tests for every patient with suspected CCS.[1]
- 12-lead resting ECG — baseline for comparison, may show ischaemia, prior infarction (Q waves), LV hypertrophy, conduction disease, arrhythmia. Often normal between episodes.
- Laboratory — full blood count (anaemia precipitates angina), renal function (relevant for contrast and ACEI/ARB), lipid profile (LDL-C, HDL-C, triglycerides; consider lipoprotein(a)), glycated haemoglobin (HbA1c) and fasting glucose, thyroid function (anaemia and hyperthyroidism both precipitate angina), NT-proBNP if heart failure signs.
- Chest radiograph — cardiomegaly, pulmonary oedema, calcification, alternative diagnoses (pneumothorax, aortic dissection contour).[6]
Step 2 — Functional testing. Used when pre-test probability is low-to-intermediate and the goal is to detect or exclude inducible ischaemia.[1]
- Exercise ECG (treadmill) — sensitivity around 65 to 75 percent and specificity 75 to 85 percent for obstructive CAD; the standard first-line test where there is no resting ECG abnormality, baseline conduction abnormality (LBBB, paced rhythm, LVH with strain), or inability to exercise. ST depression above 1 mm at low workload, sustained ST changes, hypotension during exercise, or arrhythmia are high-risk markers.
- Stress echocardiography — adds regional wall-motion analysis to functional testing. Sensitivity 80 to 90 percent, specificity 80 to 90 percent in expert hands. Better than exercise ECG in patients with baseline ECG abnormalities.
- Myocardial perfusion scintigraphy (MPS) — single-photon emission CT (SPECT) with technetium-99m or thallium; quantifies perfusion territory, ejection fraction. Useful when stress echo is unavailable or operator-dependent.
- Stress cardiac MRI — superior to SPECT for some indications; assesses perfusion, wall motion, viability (late gadolinium enhancement), and right ventricle. Preferred in younger patients, especially women (no radiation).
- Coronary flow reserve (CFR) or index of microcirculatory resistance (IMR) — used at the time of invasive angiography when microvascular angina is suspected.[4]
Step 3 — Anatomical testing. Used when the diagnosis is more likely or functional testing is unreliable or unavailable.[1]
- CT coronary angiography (CTCA) — visualises coronary anatomy non-invasively with high negative predictive value; preferred over functional testing for intermediate pre-test probability in many 2019 ESC scenarios, especially in younger patients. Calcium score (Agatston) quantifies plaque burden.
- Invasive coronary angiography — the gold-standard anatomical test; performed when CTCA is non-diagnostic, when pre-test probability is high, when non-invasive testing is positive or high-risk, or in patients with refractory symptoms.[3]
Step 4 — Physiological assessment at the time of angiography.[1]
- FFR (fractional flow reserve) — ratio of distal coronary pressure to aortic pressure during maximal hyperaemia (adenosine 140 microg/kg/min IV or regadenoson). FFR below 0.80 signifies haemodynamically significant stenosis and is the threshold for stenting per FAME 2.[4]
- iFR (instantaneous wave-free ratio) — resting index; a value under 0.89 indicates haemodynamic significance (DEFINE-FLAIR, iFR-SWEDEHEART).
- RFR (resting full-cycle ratio) and other resting indices are alternative measurements.
- CFR and IMR — for assessing microvascular function when epicardial stenosis is absent or after revascularisation.
Step 5 — Plaque characterisation (CT and MRI):[1]
- CT-derived plaque composition (calcified, non-calcified, low-attenuation) and perivascular fat attenuation are emerging markers of vulnerability.
- MRI — for viability assessment in regions of abnormal wall motion (infarcted vs hibernating vs stunned).[1]
Differential testing decisions in special groups:[1]
- Women — stress echo or stress MRI preferred over exercise ECG (pretest probability of obstructive CAD lower; functional tests perform better).
- Diabetes — aggressive imaging because of multivessel and silent disease; CTCA reasonable in some programmes.
- CKD — avoid iodine contrast where possible (consider CTCA with contrast-sparing protocols, MRI stress perfusion, MPS).
- Prior CABG — CTCA interpretation is constrained by graft metal artefact and clips; functional testing more reliable.
- Young adults with symptomatic but low-probability disease — calcium scoring may avoid unnecessary testing when zero.[1]
Management — Resuscitation
CCS is, by definition, a stable outpatient presentation — there is no "resuscitation" of chronic disease itself. However, two clinical scenarios require immediate management outside the framework of routine CCS care:[4]
(A) Acute chest pain in a patient with known or suspected CCS.[1]
- Triage with the universal chest-pain pathway — resting ECG within 10 minutes, high-sensitivity troponin, GRACE / HEART score. Differential: ACS, aortic dissection, PE, pericarditis, oesophageal, MSK.
- If the presentation is consistent with ACS, manage per ACS pathway — dual antiplatelet therapy (aspirin 300 mg loading then 75 to 100 mg daily plus a P2Y12 inhibitor), anticoagulation, anti-ischaemic therapy (sublingual nitrates, morphine if needed, oxygen only if SpO2 under 90 percent), high-sensitivity troponin, early invasive strategy per ESC NSTE-ACS risk (within 2, 24, or 72 hours).[3]
(B) Acute heart failure triggered by ischaemia.[1]
- Sit the patient up, oxygen if SpO2 under 90 percent, IV loop diuretic (furosemide 20 to 40 mg IV), GTN infusion for BP and preload, transfer to coronary care.
- Treat concurrent arrhythmia — AF, VT, bradyarrhythmia.
- Identify the trigger — new ischaemia, anaemia, hypertension, infection, non-adherence.[2]
(C) Sudden cardiac arrest survivor with known CCS — emergency coronary angiography, ICD consideration, family screening.[1]
Escalation criteria in any CCS patient: crescendo angina (CCS class IV), angina at rest, dynamic ECG changes, new heart failure signs, syncope, or arrhythmia — admit and escalate to inpatient cardiology.[5]
Management — Definitive & Stepwise
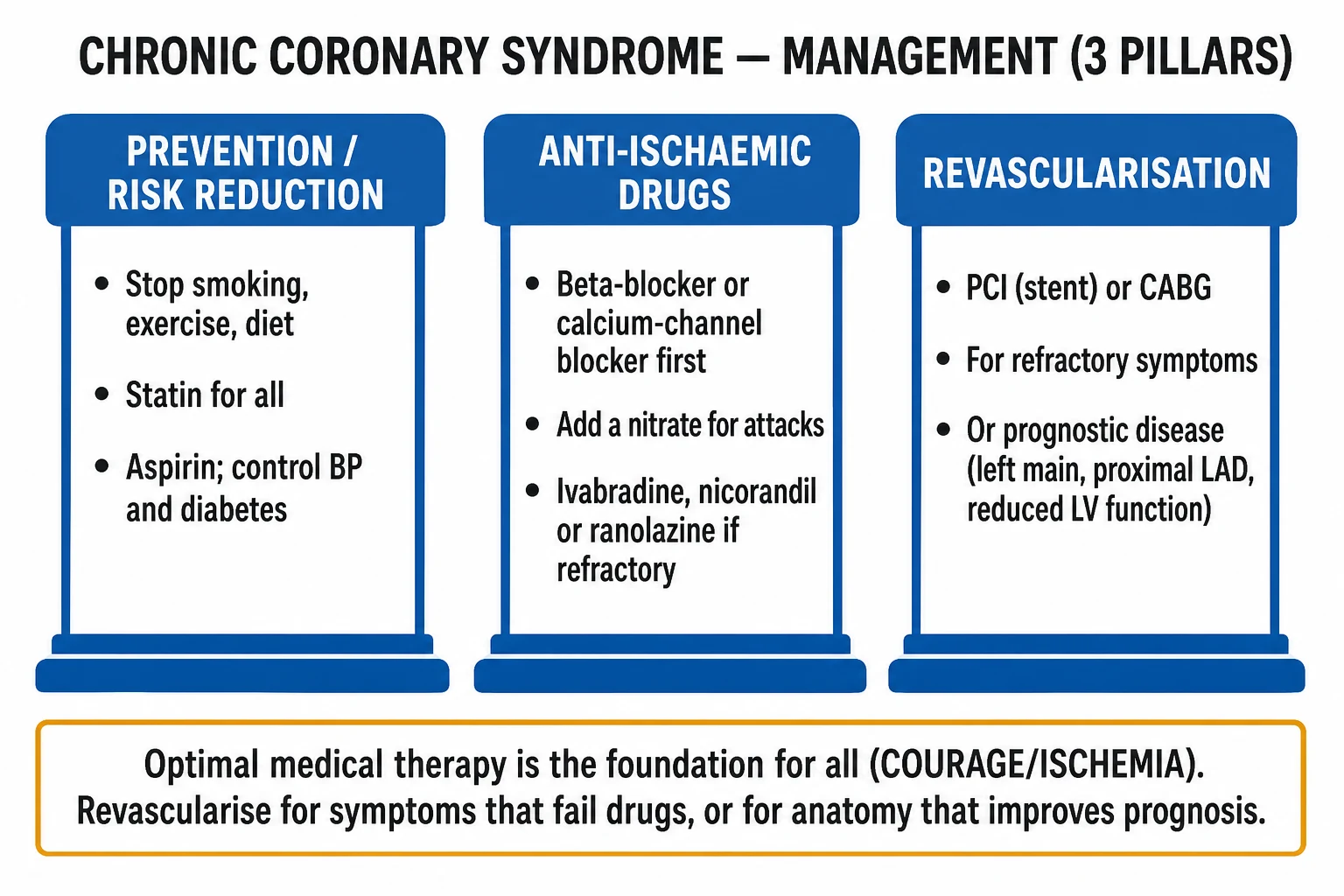
The definitive management of CCS is organised along four pillars: lifestyle, disease-modifying pharmacological therapy, anti-anginal therapy, and revascularisation when indicated. The 2019 ESC framework emphasises event-free survival and the role of FFR-guided revascularisation; COURAGE and ISCHEMIA established that optimal medical therapy alone is reasonable for most patients without high-risk anatomy (left main, proximal LAD, severe ischaemia).[1][2][3]
Pillar 1 — Lifestyle modification (the foundation, reinforced at every visit):[1]
- Smoking cessation — the single most impactful lifestyle intervention; counselling, nicotine-replacement therapy, varenicline, bupropion, behavioural support. Reduces mortality by 25 to 50 percent over 5 to 10 years.
- Mediterranean-style diet — vegetables, fruit, wholegrains, nuts, olive oil, fish, modest dairy; reduces events (PREDIMED, Lyon Diet Heart Study).
- Physical activity — at least 150 minutes per week of moderate-intensity aerobic exercise, individually prescribed in cardiac rehabilitation.
- Weight — target BMI 20 to 25; each 5 kg of weight loss reduces SBP roughly 5 mmHg and lipids proportionally.
- Alcohol — under 14 units per week; lower threshold in heart failure, atrial fibrillation, or hypertriglyceridaemia.
- Stress and sleep — sleep hygiene, screening for obstructive sleep apnoea.
- Cardiac rehabilitation — structured supervised exercise, education, and psychosocial support; class I recommendation after MI and revascularisation; improves survival, function, and adherence.[2]
Pillar 2 — Disease-modifying pharmacological therapy (secondary prevention):[2]
- Antiplatelet therapy — aspirin 75 to 100 mg daily lifelong for all patients with established CCS (and as primary prevention in selected high-risk individuals per ESC 2021). Clopidogrel 75 mg daily is an alternative where aspirin intolerance exists. After PCI, dual antiplatelet therapy (aspirin plus a P2Y12 inhibitor) is given for 6 to 12 months depending on bleeding and ischaemic risk.
- Lipid lowering — atorvastatin 40 to 80 mg nocte (or rosuvastatin 20 to 40 mg nocte) for all patients regardless of baseline LDL-C; high-intensity statin therapy is the default in CCS. Add ezetimibe 10 mg daily if LDL-C above 1.8 mmol/L (above 1.4 mmol/L in very high risk). PCSK9 inhibitors (evolocumab 140 mg subcutaneously every 2 weeks, alirocumab 75 to 150 mg every 2 weeks) for those with persistent LDL-C above target despite maximally tolerated statin plus ezetimibe. Lipoprotein(a) measured once; emerging targeted therapies.
- Renin–angiotensin blockade — ACE inhibitor (ramipril 2.5 to 10 mg daily) or ARB in CCS patients with hypertension, diabetes, CKD, prior MI, or LV dysfunction; cough or angioedema may force an ARB.
- Beta-blocker — additional benefit beyond anti-anginal action in patients with prior MI or LV dysfunction; metoprolol 25 to 100 mg twice daily or bisoprolol 2.5 to 10 mg daily.
- Blood pressure control — individually tailored; systolic under 130 mmHg where tolerated.
- Glycaemic control — metformin first-line; SGLT2 inhibitor or GLP-1 receptor agonist when diabetes plus high cardiovascular risk (dapa-, empa-, and lira-class effects).
- Annual influenza vaccination and pneumococcal vaccination.
- Phosphodiesterase-5 inhibitor (PDE5i) interactions — nitrates are contraindicated within 24 hours of PDE5i use.[2]
Pillar 3 — Anti-anginal therapy:[1][7]
The aim is to reduce myocardial oxygen demand (rate, contractility, wall stress) or increase supply (coronary vasodilation, diastolic time, oxygen-carrying capacity). First-line is usually a beta-blocker in patients without contraindication, with calcium-channel blockers as alternatives. Combination therapy is the rule in refractory cases.[2]
- Beta-blockers — first-line for rate and effort-related angina; metoprolol 25 to 100 mg twice daily or bisoprolol 2.5 to 10 mg daily (or carvedilol, atenolol). Goal resting HR 55 to 60 bpm; reduce or stop if symptomatic bradycardia, AV block, decompensated HF, or asthma.
- Long-acting calcium-channel blockers — amlodipine 5 to 10 mg daily (dihydropyridine, no rate effect; can be combined with beta-blocker where BP permits). Diltiazem or verapamil are rate-lowering non-dihydropyridines but contraindicated with beta-blocker because of bradycardia and AV block.
- Long-acting nitrates — isosorbide mononitrate 30 to 60 mg daily (asymmetrical dosing to preserve nitrate-free interval and prevent tolerance). Sublingual GTN spray or tablet for acute episodes and prophylaxis before exertion.
- Nicorandil — a nicotinamide derivative that opens ATP-sensitive potassium channels and has nitrate-like venodilation; nicorandil 5 to 30 mg daily in two divided doses, titrated up. Effective add-on or alternative where nitrates are not tolerated; benefit on rehospitalisation in IONA trial.
- Ranolazine — late sodium current inhibitor that reduces intracellular calcium overload and improves diastolic relaxation; ranolazine 375 to 500 mg twice daily, titrated to 750 mg twice daily. Useful in microvascular angina, diabetes, and refractory symptoms.
- Ivabradine — selective funny-channel (If) inhibitor that lowers heart rate without inotropy; ivabradine 5 to 7.5 mg twice daily in patients in sinus rhythm, HR above 70 bpm despite maximally tolerated beta-blocker; contraindicated in AF.
- Trimetazidine — metabolic modulator; inhibits long-chain 3-ketoacyl CoA thiolase, shifting substrate utilisation from fatty acid to glucose; 35 mg twice daily; useful add-on.
- Allopurinol — for patients with documented hyperuricaemia or those on high-dose diuretics; emerging evidence of anti-ischaemic effect in selected populations.[6]
Pillar 4 — Revascularisation:[1]
- Percutaneous coronary intervention (PCI) — drug-eluting stent deployment after appropriate antiplatelet loading; reserved for patients with haemodynamically significant disease (FFR below 0.80) or refractory symptoms despite optimal medical therapy. ORBITA documented that the placebo-controlled symptomatic benefit of PCI over best medical therapy is smaller than previously thought (around 25 to 30 percent improvement in stress capacity, narrower on symptom scores at 6 weeks), reinforcing the role of shared decision-making and intensive medical therapy before PCI.[6]
- Coronary artery bypass grafting (CABG) — preferred for left main disease (especially low SYNTAX score) and multivessel disease with diabetes (FREEDOM trial), reduced ejection fraction, or complex anatomy. Use bilateral internal mammary grafts where feasible.
- Hybrid revascularisation — LIMA-LAD by surgery with PCI to non-LAD lesions in selected patients.
Goals of therapy — first, event-free survival (no MI, stroke, cardiovascular death); second, anginal symptom control (target CCS class I or zero angina on optimised medical therapy); third, functional improvement and quality of life.[2]
Stepwise Management
The stepwise sequence for an outpatient with newly suspected CCS follows the 2019 ESC framework: (1) confirm the diagnosis and stratify risk; (2) initiate disease-modifying and anti-anginal therapy; (3) review response at 4 to 6 weeks; (4) decide on invasive investigation or revascularisation.[2]
Step 1 — Initial assessment and pre-test probability.[3]
- Take a focused history to classify symptom as typical, atypical, or non-anginal.
- Use age, sex, and symptom character to estimate pre-test probability (low < 5 percent, intermediate 5 to 15 percent, high > 15 percent).
- Modify with risk factors (diabetes, dyslipidaemia, hypertension, smoking, CKD, family history) and resting ECG.[2]
Step 2 — First-line testing.[2]
- Low pre-test probability — reassure and modify risk factors; do not test.
- Low-to-intermediate — functional testing (stress echo or CTCA in 2019 ESC).
- Intermediate — CTCA (ESC favours anatomical in this zone).
- High — invasive angiography; or non-invasive testing if patient prefers a non-invasive strategy.[3]
Step 3 — Initiate disease-modifying therapy.[2]
- Aspirin 75 to 100 mg daily lifelong.
- Atorvastatin 40 to 80 mg nocte (or equivalent high-intensity statin).
- ACE inhibitor (or ARB) where hypertension, diabetes, CKD, prior MI, or LV dysfunction present.
- Lifestyle modification advice, ideally with structured referral to cardiac rehabilitation.
- Annual influenza vaccination.[2]
Step 4 — Initiate anti-anginal therapy.[2]
- First-line — bisoprolol 2.5 to 10 mg daily (or metoprolol 25 to 100 mg twice daily) for effort-related angina; check resting HR and BP. Counsel on dose titration, side effects, and when to stop.
- Sublingual GTN — for acute episodes and pre-exertional prophylaxis; instruct on use, storage, and what to do if pain persists beyond 10 minutes (call emergency services).
- Add second agent if symptoms persist — amlodipine 5 to 10 mg daily (where BP permits and HR controlled) or isosorbide mononitrate 30 to 60 mg daily (preserving nitrate-free interval).
- Third-line options — nicorandil 5 to 30 mg daily, ranolazine 375 to 500 mg twice daily, ivabradine 5 to 7.5 mg twice daily (in sinus rhythm, HR > 70).
- Address non-cardiac contributors — anaemia (transfuse if symptomatic and Hb below 7 to 8 g/dL), thyrotoxicosis, hypertension, hypoxia, anxiety.[6]
Step 5 — Review at 4 to 6 weeks.[2]
- Check symptoms (CCS class), functional capacity, BP, HR, lipid panel (fasting), renal and liver function, side effects, adherence.
- Titrate doses to symptom control or maximal tolerated.
- Reinforce lifestyle and cardiac rehab referral.
- Reassess risk — if symptoms persist despite optimal medical therapy, refer for invasive investigation.[2]
Step 6 — Decide on invasive strategy.[1][2][3][4]
- Refractory anginal symptoms despite two anti-anginal agents at optimal doses → invasive angiography with physiological assessment (FFR, iFR).
- High-risk anatomy on non-invasive imaging (left main, severe proximal LAD, three-vessel disease with diabetes, LVEF below 50 percent with ischaemia) → invasive strategy earlier.
- FFR below 0.80 in a coronary segment with appropriate target vessel anatomy → PCI or CABG (per anatomy).
- The FAME 2 trial demonstrated that FFR-guided PCI plus optimal medical therapy reduced the composite of death, MI, and urgent revascularisation versus optimal medical therapy alone, primarily driven by lower urgent revascularisation.[4]
- COURAGE showed no overall mortality benefit of PCI over optimal medical therapy for most stable CAD, but subgroups with significant ischaemia or proximal LAD involvement benefited.[2]
- ISCHEMIA showed no overall benefit of an initial invasive strategy on mortality or MI in moderate ischaemia but better symptom control in high-angina patients.[3]
- Revascularisation for prognosis is generally reserved for left main disease, three-vessel disease with LV dysfunction, proximal LAD disease in large territory, and patients with LV dysfunction and viable myocardium.
- Revascularisation for symptoms is the larger driver in CCS; offer when symptoms limit daily life despite optimal medical therapy.
Step 7 — Long-term review. Stable patients are reviewed at 3 to 6-month intervals, with annual lipid and renal review and review of secondary prevention targets.[2]
Specific Subtypes & Scenarios
CCS subtypes — six faces (2019 ESC framework):[1]
- Silent ischaemia — ST changes or perfusion defects on stress testing or ambulatory monitoring in the absence of symptoms. Common in diabetes, CKD, elderly, post-CABG; same prognostic implications as symptomatic ischaemia.
- INOCA (Ischaemia with Non-Obstructive Coronary Arteries) — anginal symptoms, positive stress test, but no obstructive epicardial stenosis on angiography. Often microvascular dysfunction, vasospasm, or both. More common in women; treated with anti-anginals directed at supply-demand matching (beta-blocker first-line; ranolazine, CCB, ACEI add-on).
- MINOCA (Myocardial Infarction with Non-Obstructive Coronary Arteries) — distinct from INOCA; defined as MI per the Fourth Universal Definition with no obstructive lesion above 50 percent stenosis. Mechanisms include plaque rupture with lysis, epicardial vasospasm, microvascular dysfunction, coronary thromboembolism, myocarditis (mimic), takotsubo (mimic).
- Post-revascularisation CCS — patients more than 12 months after PCI or CABG with stable symptoms. Workup differentiates in-stent restenosis (especially first 12 months), graft disease (CABG: venous grafts degenerate after 7 to 10 years; arterial grafts longer), and native disease progression. Cardiac MRI and CTCA have roles.
- Vasospastic (Prinzmetal) angina — focal or diffuse epicardial spasm producing transient transmural ischaemia; rest pain, ST elevation, normal exercise capacity. Provoked at angiography by acetylcholine or ergonovine. Treatment: calcium-channel blocker first-line, nitrates, smoking cessation; avoid beta-blockade in monotherapy.
- Refractory angina — chronic anginal symptoms (above CCS III) for over 3 months despite optimal medical therapy and revascularisation where feasible. Options include enhanced external counterpulsation, spinal cord stimulation, transmyocardial revascularisation, chronic total occlusion PCI in selected centres, and structured cardiac rehab.[2]
Other scenarios to recognise:[1]
- Diabetes and CCS — accelerated atherosclerosis, multivessel involvement, impaired pain perception; lower threshold for revascularisation.
- Elderly — atypical presentations, polypharmacy, higher procedural risk; respect patient preference.
- Chronic kidney disease — bleeding risk with anti-thrombotics; contrast sparing for CTCA and angiography.
- Pregnancy — rare; CCS-like symptoms should prompt peripartum cardiology review; some anti-anginal agents are not safe in pregnancy.[5]
Complications
If untreated or inadequately controlled, CCS progresses along several adverse trajectories: acute coronary syndrome, heart failure, arrhythmia, and functional decline.[1]
Acute coronary syndrome (ACS). The dominant event — plaque rupture or erosion transitioning stable to unstable disease, presenting as NSTEMI or STEMI. Risk is highest in patients with multivessel disease, prior MI, diabetes, CKD, smoking, or known low ejection fraction. Reducing risk requires aggressive lipid lowering, antiplatelet therapy, and BP control.[2]
Heart failure. Two main mechanisms: (1) acute ischaemic dysfunction — regional stunning followed by adverse remodelling; (2) chronic hibernation — chronic hypoperfusion of viable myocardium producing reversible dysfunction that improves with revascularisation. Both can produce HFpEF or HFrEF depending on disease pattern.[1]
Arrhythmias. Atrial fibrillation is common in CCS due to atrial ischaemia, hypertension, and age. Ventricular arrhythmia (VT, VF) is more common in the presence of scar from prior MI, LV dysfunction, or critical ischaemia. Sudden cardiac death risk stratification (LVEF) drives decisions on ICD for primary prevention.[1]
Cerebrovascular events. Strokes (ischaemic and haemorrhagic) are the second-most frequent major event in CCS, particularly in hypertensive, diabetic, or AF patients.[1]
Chronic total occlusion. Complete occlusion of an epicardial artery beyond 3 months may develop silently and contribute to LV dysfunction, or symptomatically through recurrent angina despite medical therapy.[2]
Functional and quality-of-life decline. Uncontrolled angina, dyspnoea, and fatigue limit activity, employment, social engagement, and independence. Depression and anxiety are common and exacerbate symptoms.[6]
Bleeding. Antiplatelet and anticoagulant therapy confer bleeding risk, particularly gastrointestinal and intracranial. Combination DAPT plus anticoagulant therapy (post-PCI with AF) further escalates risk; the 2019 ESC AF-PCI algorithm provides a structured framework.[2]
CKD progression. Contrast imaging, RAAS blockade, and diuretics all affect renal function; monitor creatinine, potassium, and weight.[1]
Mortality. Annual all-cause mortality in modern CCS cohorts: roughly 1 percent in low-risk outpatients, 1 to 2 percent in those on optimal medical therapy with low ischaemic burden, 3 to 4 percent with diabetes or reduced LV function, and over 5 percent with multivessel disease and LV dysfunction.[2]
Prognosis & Disposition
The prognosis of CCS depends on three axes: baseline LV function, ischaemic burden, and comorbidity (especially diabetes, CKD, prior MI). Risk stratification tools are used to estimate event risk per year and to guide the intensity of investigation and treatment.[1]
Risk modifiers that worsen prognosis:[1]
- Reduced LV ejection fraction (LVEF below 50 percent).
- Diabetes mellitus.
- CKD (eGFR below 60 mL/min/1.73 m²).
- Multivessel or left main disease.
- Proximal LAD disease.
- High ischaemic burden (above 10 percent of LV ischaemia on MPS).
- Persistent angina on optimal medical therapy.
- Ankle-brachial pressure index below 0.9 (PAD coexistence).
- High-sensitivity troponin elevation in the absence of ACS.
- Heart failure signs.
- Inflammatory biomarkers (hsCRP).
- Peripheral arterial disease, prior cerebrovascular disease, frailty.[2]
Stratification pathway. Use clinical risk scores (ESC SYNTAX II, EuroSCORE II for surgical, ACEF; SCORE2 / PREVENT for primary prevention in relatives). Choose management intensity accordingly.[1]
Events and durations. Untreated stable angina — major adverse cardiovascular event (MACE) rates rise roughly 3 to 5 percent per year. Aggressive management with statin, antiplatelet, ACEI, and revascularisation when indicated — cumulative MACE approaches 1 to 2 percent per year in low-risk patients, higher in selected groups. The recent LoDoCo2 and COMPASS trials demonstrated that low-dose colchicine and low-dose rivaroxaban in addition to standard therapy reduce cardiovascular events in stable CAD (rivaroxaban with aspirin in COMPASS, aspirin alone), changing the secondary prevention landscape.[2]
Disposition. Most CCS patients are managed as outpatients with structured follow-up in cardiology and primary care. Indications for inpatient admission and inpatient cardiology review: crescendo angina, rest pain, suspicion of ACS, syncope, arrhythmia, new heart failure, post-revascularisation complication, severe uncontrolled symptoms, abnormal stress test at high risk.[5]
Follow-up cadence:[1]
- Stable, well-controlled — every 3 to 6 months with primary care; cardiology review at least annually.
- Recent revascularisation — cardiology review at 6 weeks, 6 months, then annually.
- Heart failure, CKD, diabetes — closer follow-up (1 to 3 months) for titration.
- New symptoms — same-day review through chest-pain service.[5]
Rehabilitation and return to function. Cardiac rehabilitation after MI, PCI, or CABG is class I — start within 4 weeks, structured for 8 to 12 weeks, with maintenance thereafter.[2]
Special Populations
Women. Atypical presentations dominate — dyspnoea, fatigue, epigastric discomfort more than substernal pressure; lower pre-test probability of obstructive CAD. Higher rates of INOCA, microvascular angina, and coronary vasospasm. Exercise ECG less specific; stress echocardiography, MRI perfusion, and CTCA more reliable. Anti-anginal choice similar, but beware ACEi/ARB teratogenicity and ACEi cough, and recognise that women get less aggressive secondary prevention despite higher absolute risk.[6]
The elderly. Multivessel disease, prior MI, CKD, and atrial fibrillation commonly coexist. Atypical presentations (fatigue, falls, confusion, decreased exercise tolerance). Polypharmacy and ADR risk require careful dose titration and deprescribing review. Major clinical decisions on revascularisation should be guided by biological rather than chronological age and involve shared decision-making.[4]
Diabetes mellitus. Higher prevalence, accelerated atherosclerosis, multivessel involvement, silent ischaemia, and poorer prognosis. Lower threshold for invasive investigation. SGLT2 inhibitors and GLP-1 receptor agonists confer cardiovascular benefit beyond glycaemic control. PERICLES, EMPA-REG OUTCOME, and LEADER trial implications. PCI vs CABG in multivessel disease — FREEDOM favoured CABG, but contemporary drug-eluting stents have narrowed the gap.[3]
Chronic kidney disease. Both a risk marker and a therapeutic limit (no NSAIDs, dose adjust contrast, monitor creatinine with ACEI/ARB and aldosterone blockade). Bleeding risk is high; cardiology and nephrology joint review for advanced CKD. CTCA feasible with contrast-sparing protocols; stress MRI preferred where available.[5]
Prior CABG. CTCA challenging because of metal-clip artefact; stress imaging more reliable. Consider redo CABG vs PCI in graft vs native disease individually.[2]
Patients on dialysis. Risk-benefit calculus favours medical therapy; revascularisation is reserved for refractory symptoms or prognostically critical disease.[2]
Ethnicity and access. South Asian populations have higher CAD prevalence at younger ages; aggressive risk-factor modification is essential. Socioeconomic deprivation limits access to cardiac rehab, healthy food, and fresh food; structured nurse-led programmes help.[1]
Evidence & Guidelines
Foundational guidelines:[1]
- 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes (Knuuti et al.) — reframes "stable angina" as CCS, defines the six clinical scenarios, emphasises pre-test probability-based testing, hierarchical anti-anginal algorithm.[1]
- 2013 ESC Guidelines on the Management of Stable Coronary Artery Disease — predecessor; introduced CCS concept and the diamond pre-test probability model.[7]
- 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the Diagnosis and Management of Patients With Stable Ischemic Heart Disease (Fihn et al.) — parallel North American guideline; still referenced for nuanced risk recommendations.[5]
- NICE Clinical Guideline CG95 (UK, 2016) — chest pain of recent onset assessment; provides a UK NHS-aligned diagnostic algorithm.
Landmark trials every cardiology trainee knows:[5]
- COURAGE Trial (Boden 2007, NEJM) — 2,287 patients with stable CAD randomised to PCI plus optimal medical therapy versus optimal medical therapy alone. No significant difference in mortality or MI over 4.6 years; better early symptom control with PCI, narrowing over time. Reinforced OMT as first-line and PCI as add-on for symptom control.[2]
- FAME 2 Trial (De Bruyne 2014, NEJM) — 888 patients with FFR 0.80 or below randomised to FFR-guided PCI plus OMT vs OMT alone. PCI reduced the composite of death, MI, and urgent revascularisation, driven primarily by fewer urgent revascularisations; mortality and MI alone did not differ. Established FFR 0.80 as the physiology threshold for intervention.[4]
- ORBITA Trial (Al-Lamee 2018, Lancet) — 200 patients with stable angina and single-vessel disease randomised to PCI vs sham procedure. At 6 weeks, PCI did not significantly improve exercise time versus sham (the placebo-controlled difference was small); symptom scores improved more with PCI but the exercise increment was less than previously believed. Reframed the role of PCI in stable disease and required transparent informed consent in elective angioplasty.[6]
- ISCHEMIA Trial (Maron 2020, NEJM) — 5,179 patients with moderate or severe ischaemia on stress testing randomised to initial invasive versus conservative strategy. No significant difference in mortality or MI over 3.2 years; invasive strategy better for symptom control in those with daily/weekly angina. Reinforced optimal medical therapy first for many patients.[3]
- ISCHEMIA-Extend and ISCHEMIA-Chronic Kidney Disease — extended follow-up and CKD subgroup; emphasise CKD-specific risks.
- FREEDOM Trial (Farkouh 2012) — CABG vs PCI in patients with diabetes and multivessel disease; CABG superior for mortality and composite outcomes.
- SYNTAX Trial — PCI vs CABG in three-vessel or left main disease; CABG superior in higher SYNTAX scores.
- EXCEL and NOBLE — PCI vs CABG in left main disease; nuanced comparative outcomes (PCI acceptable in selected low-SYNTAX-score patients).
- COMPASS Trial (Eikelboom 2017) — low-dose rivaroxaban 2.5 mg twice daily plus aspirin vs aspirin alone in stable CAD/PAD; reduced composite cardiovascular events; expanded secondary prevention options.
- LoDoCo2 Trial (Nidorf 2020) — low-dose colchicine 0.5 mg daily reduced ischaemic events in stable CAD.
- EMPA-REG OUTCOME, LEADER, REWIND — SGLT2 inhibitors and GLP-1 receptor agonists reduced cardiovascular events in patients with diabetes and established CAD; inform secondary prevention.
- SPRINT — intensive BP control below 120 mmHg systolic reduced cardiovascular events; informs target BP in CCS.
- FOURIER (PCSK9) and IMPROVE-IT (ezetimibe) — additional LDL-C lowering on top of statins reduces events in CCS.
Regional practice nuances.[2]
- UK NICE — favours CTCA for intermediate probability; functional testing for those unable to have CTCA.
- US ACC/AHA — favours stress imaging or functional testing; invasive strategy reserved for high-risk.
- ESC Europe — favours CTCA, encourages FFR-guided PCI; sex-specific recommendations.[3]
Areas of debate. (1) The role of routine FFR-CT derived from CTCA (FFR-CT), (2) the value of invasive physiology in the left main stem, (3) the role of chronic total occlusion PCI in angina relief, (4) the optimal duration of DAPT after PCI (1 to 3 months under current evidence-based regimens), (5) expanded use of low-dose anticoagulants in CCS (COMPASS, THEMIS).[2]
Exam Pearls
- CCS = chronic stable presentations of CAD, NOT one acute event. Defined by 2019 ESC as a continuum. Six clinical scenarios: suspected CAD with stable symptoms, new heart failure with suspected CAD, stabilised post-ACS, over 12 months post-revascularisation, INOCA, silent ischaemia.[1]
- Classic stable angina: substernal discomfort, provoked by exertion or emotion, relieved by rest or nitroglycerin, lasting under 10 minutes.
- CCS grading — Class I (vigorous activity), II (rapid stairs / cold), III (one flight / 100 to 200 m flat), IV = rest angina (unstable angina until proven otherwise).
- Differentials to recall: microvascular angina (women, normal angiogram), vasospastic / Prinzmetal angina (rest pain, transient ST elevation), MSK (costochondritis), oesophageal (reflux, spasm), anxiety / hyperventilation, pulmonary (PE, pneumothorax), aortic dissection, pericarditis, mitral valve prolapse. ACS must always be excluded for new rest pain.
- Pre-test probability from age, sex, and symptom character (2019 ESC diamond modified). Use it to avoid low-yield testing.
- Investigations — resting ECG (often normal), exercise ECG (first-line if no baseline ST abnormality), stress echo / MPS / MRI (more sensitive), CTCA (anatomical, high NPV, preferred in younger women), invasive angiography (gold standard). Use FFR or iFR during angiography; FFR below 0.80 = significant (FAME 2); iFR below 0.89 = significant.
- Medical therapy backbone — aspirin 75 to 100 mg daily, atorvastatin 40 to 80 mg nocte, ACE inhibitor (ramipril 2.5 to 10 mg daily) in hypertension / diabetes / CKD / post-MI, bisoprolol 2.5 to 10 mg daily for rate / symptom control, amlodipine 5 to 10 mg daily for afterload lowering, isosorbide mononitrate 30 to 60 mg daily, nicorandil 5 to 30 mg daily, ranolazine 375 to 500 mg twice daily, ivabradine 5 to 7.5 mg twice daily (sinus rhythm, HR above 70 despite beta-blocker). Sublingual GTN spray 0.4 mg per dose PRN and prophylactically before exertion.
- Revascularisation for prognosis — left main disease (CABG preferred by trial evidence), proximal LAD, three-vessel disease with LV dysfunction or diabetes (FREEDOM favours CABG), critical anatomy with ischaemia.
- Revascularisation for symptoms — when symptoms limit daily life despite two anti-anginal agents at optimal dose; FFR-guided.
- What trials say — COURAGE no mortality benefit of PCI over OMT; FAME 2 PCI reduces composite events (driven by urgent revascularisation); ISCHEMIA initial invasive no overall benefit in moderate ischaemia; ORBITA PCI has small placebo-controlled benefit in stable disease.
- Subtypes to recall — INOCA, MINOCA, Prinzmetal (vasospasm), silent ischaemia (diabetics, CKD), post-revascularisation (in-stent restenosis vs progression), refractory angina.
- Red flags — crescendo angina, rest pain above 20 minutes, syncope, new heart failure, dynamic ECG, post-PCI chest pain — call for inpatient cardiology review.
- Complications to know — ACS, heart failure, arrhythmia (AF, VT/VF), stroke, CKD progression, mortality 1 to over 5 percent per year depending on risk.
- Special populations — women (atypical presentation, more INOCA), diabetes (multivessel, silent), CKD (bleeding risk, contrast limits), elderly (polypharmacy, atypical), prior CABG (graft disease).
CCS — key numbers
CCS subtypes — six faces
SCIMPR
ST changes without symptoms; diabetics, CKD, elderly
Classic exertional pain; fixed plaque; refractory angina if persists despite OMT
Ischaemia with no obstructive CAD on angiography — microvascular
MI with non-obstructive CAD; mechanism varies — investigate
Rest pain, transient ST elevation, provoked on acetylcholine challenge
Above 12 months post-PCI / CABG — restenosis vs progression
Exam application bank (NEET-PG / INICET)
One-line answer
Chronic coronary syndrome (CCS) is the modern umbrella term replacing "stable angina" for the long-term presentations of coronary artery disease. Defined by the 2019 ESC Guidelines as the spectrum of clinical presentations driven by chronic, often predictable, myocardial ischaemia typically precipitated by exertion or emotional stress and relieved by rest or sublingual nitrates. Anatomically it is the consequence of fixed or dynamic epicardial coronary stenosis (atherosclerotic plaque with intact fibrous cap), microvascular dysfunction, or vasospasm. The classic presentation is substernal chest discomfort provoked by exertion, lasting under 10 minutes, and relieved by rest or nitroglycerin (CCS grade I-IV / Canadian Cardiovascular Society grading). Atypical presentations are common in women, diabetics and the elderly. Investigations progress from resting ECG through functional testing
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard.[2]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes.[7]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change.[1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each.[1]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory.[1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Chronic Coronary Syndrome.
[1]References
- [1]Knuuti J, Wijns W, Saraste A, et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. European Heart Journal, 2020.PMID 31504439
- [2]Boden WE, O'Rourke RA, Teo KK, et al. (COURAGE Trial Research Group) Optimal medical therapy with or without PCI for stable coronary disease. New England Journal of Medicine, 2007.PMID 17387127
- [3]Maron DJ, Hochman JS, Reynolds HR, et al. (ISCHEMIA Investigators) Initial Invasive or Conservative Strategy for Stable Coronary Disease. New England Journal of Medicine, 2020.PMID 32227755
- [4]De Bruyne B, Fearon WF, Pijls NH, et al. (FAME 2 Trial Investigators) Fractional flow reserve-guided PCI for stable coronary artery stenosis. New England Journal of Medicine, 2014.PMID 25176289
- [5]Fihn SD, Gardin JM, Abrams J, et al. 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the diagnosis and management of patients with stable ischemic heart disease. Journal of the American College of Cardiology, 2012.PMID 23182125
- [6]Al-Lamee R, Thompson D, Dehbi HM, et al. (ORBITA Investigators) Percutaneous coronary intervention in stable angina (ORBITA): a double-blind, randomised controlled trial. Lancet, 2018.PMID 29103656
- [7]Task Force Members, Montalescot G, Sechtem U, et al. 2013 ESC guidelines on the management of stable coronary artery disease: the Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Eur Heart J, 2013.PMID 23996286