Cardiology · Cardiology
Prosthetic Valves and Anticoagulation
Also known as Artificial heart valve · Mechanical valve · Bioprosthetic valve · TAVI · TAVR
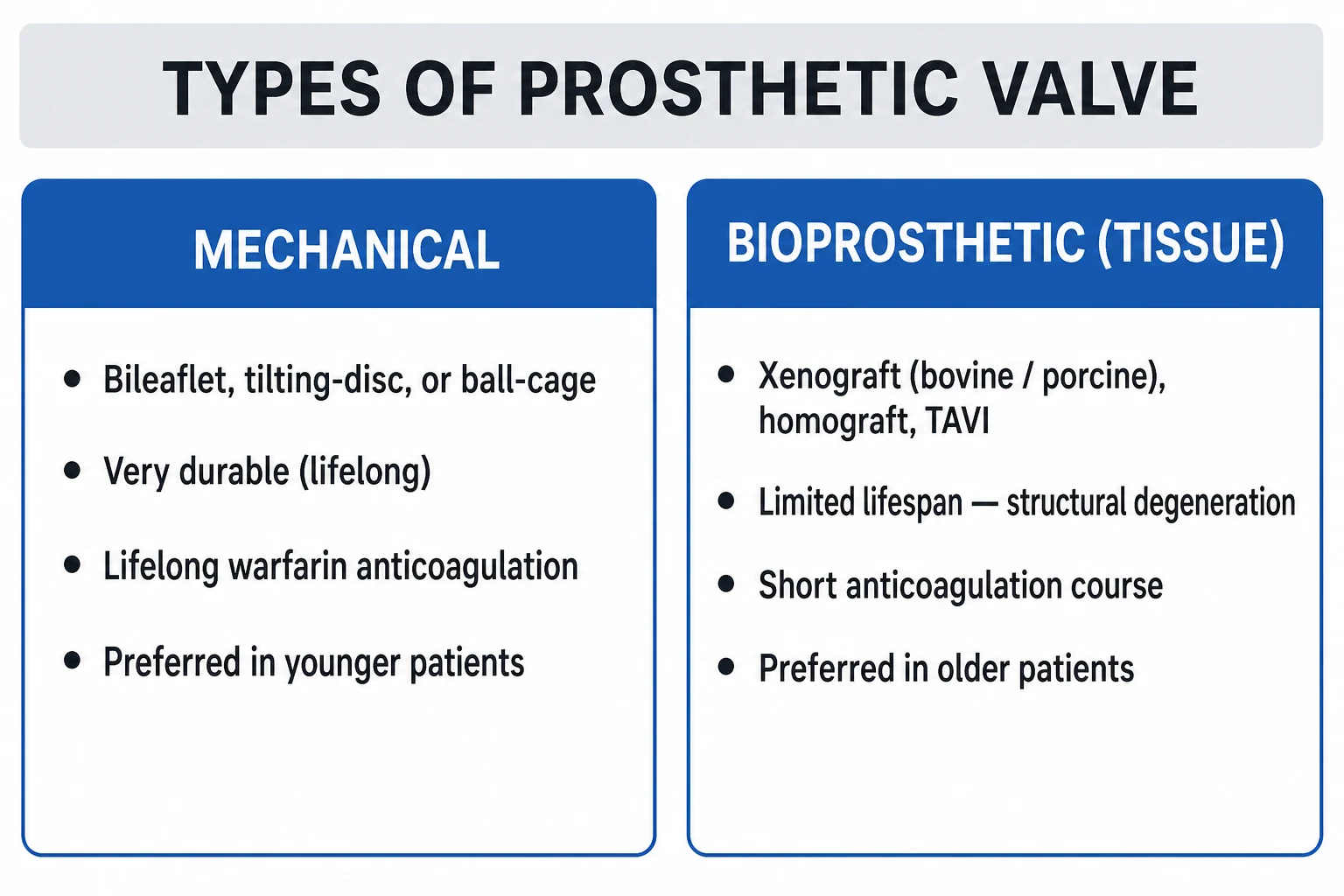
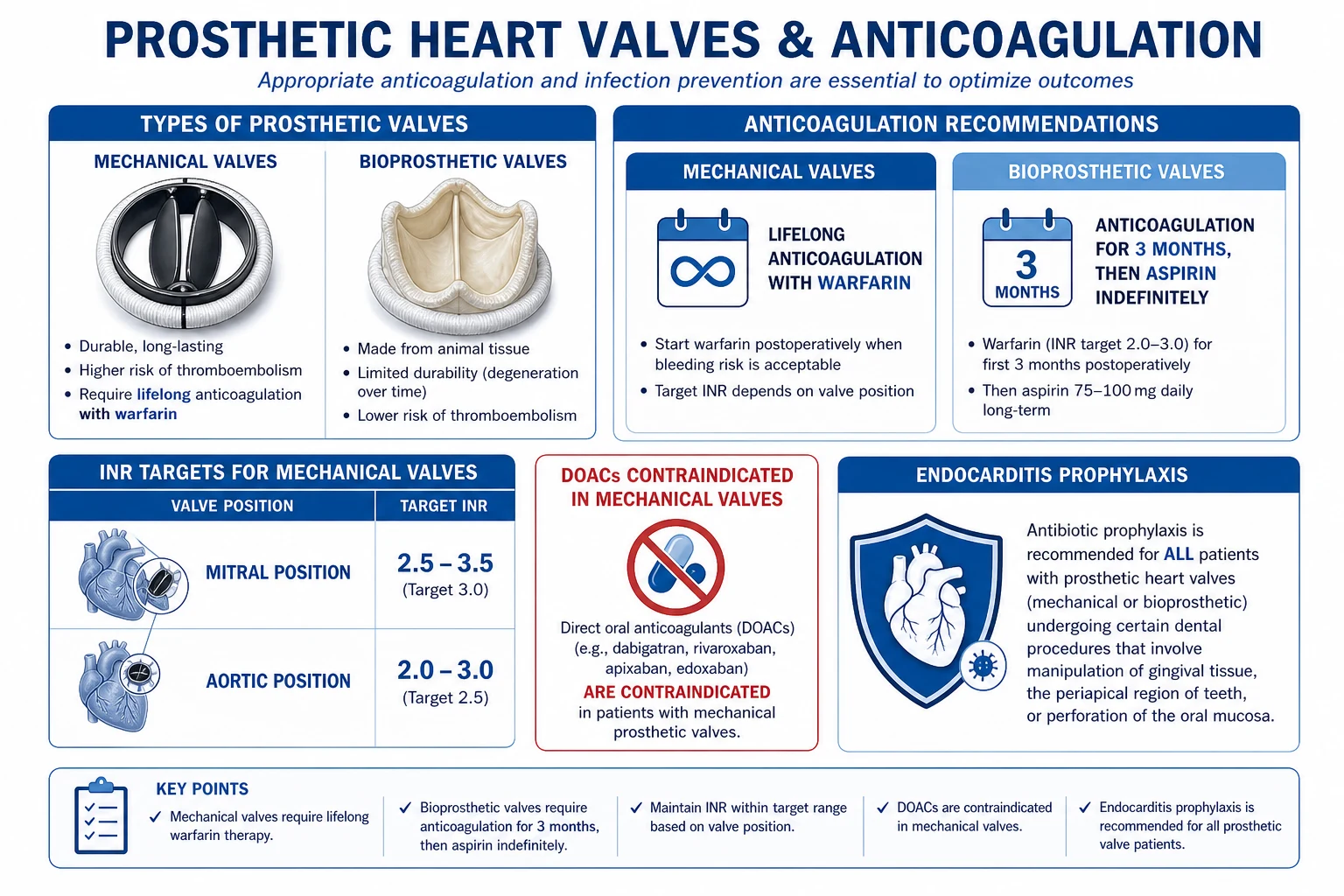
Prosthetic heart valves are either mechanical (pyrolytic carbon bileaflet, tilting disc, or caged ball; durable for life but thrombogenic, mandating lifelong warfarin — INR 2.5 to 3.5 mitral, 2.0 to 3.0 aortic) or bioprosthetic / tissue (bovine pericardial Carpentier-Edwards, porcine Hancock; no lifelong anticoagulation but structural deterioration over 10 to 15 years). Transcatheter (TAVI/TAVR) Edwards SAPIEN and Medtronic CoreValve/Evolut serve elderly high-risk severe aortic stenosis. DOACs are contraindicated in mechanical valves (RE-ALIGN trial). Bioprosthetic valves need warfarin for 3 months then aspirin. Acute valve thrombosis is an emergency: surgery if obstructive, thrombolysis if surgery unavailable.
On this page & tools
Your progress
Saved locally on this device.
Exam tags
Red flags
Overview & Definition
A prosthetic heart valve is an artificial device surgically or percutaneously implanted to replace a diseased native valve that can no longer be repaired. Roughly 100,000 valve replacements are performed each year in the United States, with comparable numbers across Europe, and the numbers are rising as the population ages and degenerative aortic stenosis becomes the dominant indication.[1]
Every prosthetic valve is a trade-off between durability and thrombogenicity. Mechanical valves, machined from pyrolytic carbon and titanium alloys, are essentially indestructible and outlive the patient — but their non-biological surfaces activate clotting on every heartbeat, mandating lifelong warfarin anticoagulation. Bioprosthetic (tissue) valves, fashioned from bovine pericardium or porcine aortic valve leaflets, are far less thrombogenic and need anticoagulation for only the first three post-operative months — but they undergo structural valve deterioration (SVD) as the tissue calcifies and tears, typically failing at 10 to 15 years and requiring re-operation or valve-in-valve intervention.[1][2]
The choice between these families is the single most consequential decision in the valve-replacement consultation, because it commits the patient to a lifelong pathway of either anticoagulation monitoring (mechanical) or anticipated re-intervention (bioprosthetic). The transcatheter revolution has added a third pathway — TAVI/TAVR — that delivers a bioprosthetic valve percutaneously for the elderly and inoperable patient with severe aortic stenosis, avoiding sternotomy and cardiopulmonary bypass entirely.[5]
Three guideline bodies define contemporary practice: the ACC/AHA 2020 Valvular Guideline (US standard), the ESC/EACTS 2021 Guidelines (European standard), and the NICE NG208 (UK). They are largely concordant on valve selection, INR targets, and the absolute contraindication of DOACs in mechanical valves, but differ in the fine print of valve choice thresholds and the timing of bioprosthetic anticoagulation.[1][2]
Classification
The classification of prosthetic valves runs along two axes — mechanism of construction (mechanical vs bioprosthetic vs transcatheter) and valve position (aortic, mitral, tricuspid, pulmonary). Both axes govern the anticoagulation strategy and the thrombosis risk.[1][2]
Mechanical valves
Bileaflet (St. Jude, CarboMedics, On-X)
- Two semicircular pyrolytic-carbon leaflets pivoting in a housing — the modern standard, over 80 percent of mechanical implants
- Central and two lateral orifices; near-physiological laminar flow
- Extremely durable (decades); hinge thrombosis the main risk if INR subtherapeutic
- On-X bileaflet permits a lower INR (1.5 to 2.0) in selected aortic patients (PROACT trials)
Tilting disc (Medtronic Hall, Bjork-Shiley)
- Single circular disc tilting open 60 to 75 degrees within a metal cage
- Two orifices of unequal size (major and minor); some flow stasis in minor orifice
- Largely superseded by bileaflet; Bjork-Shiley had strut fracture with outlet strut embolisation
- Still encountered in long-term follow-up of older implants
Caged ball (Starr-Edwards)
- Silicone elastomer ball within a metal cage — the first successful prosthetic valve (1960)
- Distinctive loud opening and closing clicks
- High profile (problematic in small LV cavities and mitral position); turbulent flow
- Historical importance only; no longer implanted but still encountered in long-term survivors
Bioprosthetic (tissue) valves
Stented bovine pericardial (Carpentier-Edwards PERIMOUNT)
- Three leaflets fashioned from glutaraldehyde-fixed bovine pericardium mounted on a stent
- Excellent haemodynamics; the most widely used surgical bioprosthesis
- SVD through calcification and tear typically at 12 to 15 years (faster in younger patients)
- No lifelong anticoagulation — warfarin 3 months then aspirin
Stented porcine (Hancock II, Mosaic)
- A preserved pig aortic valve mounted on a stent
- Slightly less favourable haemodynamics than bovine pericardial
- Comparable durability; SVD at 10 to 15 years
- Same anticoagulation strategy as bovine pericardial
Stentless (Freestyle, Toronto SPV)
- Porcine root or valve without a rigid stent — lower transvalvular gradient
- Used in younger patients, small aortic root, and for repair of aortic root pathology
- Technically demanding to implant; potential for longer durability
Sutureless / rapid deployment (Perceval, Intuity)
- Self-expanding or balloon-expandable sewing ring enables minimal-access surgery
- Reduces bypass and cross-clamp time in elderly and high-risk surgical patients
- Same anticoagulation profile as other bioprosthetic valves
Transcatheter valves (TAVI / TAVR)
Balloon-expandable (Edwards SAPIEN 3, SAPIEN XT)
- Bovine pericardial leaflets mounted on a cobalt-chromium balloon-expandable frame
- Delivered transfemorally (or transapical, trans-subclavian) and deployed by balloon inflation
- Indicated for severe symptomatic aortic stenosis in any age when patient choice after shared decision-making
- Risk of permanent pacemaker 5 to 10 percent; paravalvular leak the main complication
Self-expanding (Medtronic CoreValve Evolut)
- Porcine pericardial leaflets on a nitinol self-expanding frame; supra-annular design
- Larger effective orifice area and lower gradients, suited to small annuli
- Higher pacemaker risk (10 to 25 percent)
- Proven non-inferior or superior to surgery across risk strata (CoreValve US Pivotal, Evolut Low Risk)
By position
Mitral position
- Higher intrinsic thrombosis risk than aortic (lower flow velocities, larger atrial surface)
- Mechanical: target INR 3.0 (range 2.5 to 3.5)
- Bioprosthetic: warfarin INR 2.5 (range 2.0 to 3.0) for 3 to 6 months, then aspirin
- Mechanical preferred in patients under 65 who are already anticoagulated or in sinus rhythm with good compliance
Aortic position
- Mechanical + low risk (bileaflet, sinus rhythm, no LA enlargement, normal LV, no prior TE): INR 2.5 (range 2.0 to 3.0)
- Mechanical + any risk factor: INR 3.0 (range 2.5 to 3.5)
- Bioprosthetic: warfarin 3 months then aspirin; TAVI is now commonest in the elderly
- On-X mechanical valve permits lower INR 1.5 to 2.0 in selected aortic patients
Right-sided (tricuspid, pulmonary)
- Bioprosthetic strongly preferred — mechanical valves thrombose at unacceptable rates in the low-pressure right heart
- Tricuspid mechanical (if used): INR 3.0 (range 2.5 to 3.5)
- Percutaneous Melody valve for pulmonary position (often in congenital disease)
The 2020 ACC/AHA and 2021 ESC/EACTS guidelines now recommend that valve choice is a shared decision with the patient, not driven solely by age. The earlier age threshold of 65 years is a starting point, but the expected re-operation risk, anticoagulation burden, and patient preference all weigh in. The ESC explicitly recommends against a blanket age cut-off and emphasises individualised decision-making.[1][2]
Epidemiology & Risk Factors
The epidemiology of prosthetic valves is changing rapidly. Two decades ago, mechanical valves accounted for around half of all implants; today they comprise only 20 to 25 percent, displaced by bioprosthetic and transcatheter options as patients and clinicians increasingly trade durability for freedom from anticoagulation.[1]
Prosthetic valves by the numbers
The choice of valve is influenced by patient age (under 50: mechanical favoured for durability; over 70: bioprosthetic or TAVI favoured), life expectancy (a re-operation in 15 years is poorly tolerated in the elderly), ability to anticoagulate safely (compliance, no bleeding history, no high-fall risk, no planned pregnancy), comorbidities (chronic kidney disease accelerates bioprosthetic calcification but complicates warfarin; atrial fibrillation already mandates anticoagulation, tilting toward mechanical), valve position (mitral favours mechanical in younger patients due to higher bioprosthetic failure rates), and patient preference.[1][2]
The classic risk factors for valve thrombosis are the risk factors for any pro-thrombotic state in the setting of a foreign surface: subtherapeutic INR (the single biggest modifiable factor), mitral or tricuspid position, older-generation mechanical valves (caged ball, tilting disc), atrial fibrillation, left ventricular dysfunction, left atrial enlargement, prior thromboembolism, hypercoagulable states (pregnancy, malignancy, antiphospholipid syndrome), and infection (endocarditis disrupts flow and seeds thrombus).[1]
Pathophysiology
The pathophysiology of prosthetic valve complications is the pathophysiology of blood meeting a foreign surface — and it differs fundamentally between mechanical and bioprosthetic valves.[1]
Why mechanical valves thrombose
A mechanical valve is a permanent intravascular foreign body. Its pyrolytic carbon and metal surfaces trigger the coagulation cascade through contact activation (the intrinsic pathway, initiated when Factor XII meets the negatively charged prosthetic surface) and through tissue-factor expression by monocytes adherent to the sewing ring. Platelets adhere and activate on the foreign surfaces, releasing procoagulant microparticles. The flow patterns are abnormal: bileaflet valves create three orifices with central laminar flow but stagnation zones within the hinges (the classic site of valve thrombosis); tilting disc valves create unequal major and minor orifices with a stagnant minor orifice; caged ball valves generate highly turbulent flow with stagnation behind the ball. These sites of stasis plus the foreign surface fulfil the Virchow triad (endothelial/surface injury, abnormal flow, hypercoagulability) at every heartbeat — the inescapable reason that all mechanical valves require lifelong anticoagulation.[1]
The risk is position-dependent: mitral and tricuspid valves thrombose more often than aortic because the lower-pressure chambers of the right heart and left atrium produce slower flow across the valve. The very high flow of the systemic aorta is comparatively protective.[1]
Why bioprosthetic valves deteriorate
Bioprosthetic leaflets, although treated with glutaraldehyde to remove cellular antigenicity, retain a collagen scaffold that is subject to calcification, mechanical fatigue, and immunological injury. Calcium hydroxyapatite deposits within the collagen matrix of the leaflets, stiffening them and restricting motion; the constant flexing eventually produces leaflet tears (often at the base, near the stent post) and perforations. The result is structural valve deterioration (SVD) — a mixed stenotic and regurgitant lesion that progresses over months.[4]
The rate of SVD is accelerated in younger patients (whose more active calcium metabolism calcifies the leaflets faster), in the mitral position (higher mechanical stress on closure), in chronic kidney disease, and in pregnancy. A bioprosthetic valve that may last 15 years in a 75-year-old can fail in 5 to 8 years in a 40-year-old — the central reason that younger patients are still considered for mechanical valves despite the anticoagulation burden.[4][1]
The mechanism behind each complication
Valve thrombosis
- Thrombus forms on the leaflets, hinges, or sewing ring of a mechanical valve (or rarely a bioprosthesis)
- May be obstructive (acute heart failure, muffled clicks) or non-obstructive (incidental on echo)
- Precipitated by subtherapeutic INR, pregnancy, hypercoagulable states
Structural deterioration
- Calcification, tear, fibrosis of bioprosthetic leaflets
- Gradual onset over months — new murmur, rising gradient on serial echo
- Treated by re-operation or valve-in-valve TAVI
Paravalvular leak
- Defect between the sewing ring and native annulus — from suture dehiscence, infection, or calcified annulus
- Causes regurgitation and mechanical haemolysis (shear injury to red cells)
- May close percutaneously (Amplatzer occluder) or surgically
Pannus
- Fibrotic tissue overgrowth from the sewing ring onto the leaflets — gradually restricts opening
- Distinct from thrombus (chronic, organised, less responsive to anticoagulation)
- Often requires surgical excision or replacement
Patient-prosthesis mismatch (PPM)
- The prosthetic effective orifice area is too small for the patient's body size (indexed EOA under 0.85 cm2/m2)
- Persistent high gradient despite a normally functioning valve
- Prevented by sizing the prosthesis to the patient; severe PPM causes persistent heart-failure symptoms
Endocarditis (PVE)
- Infection of the sewing ring or leaflets; vegetation, abscess, dehiscence
- Early (under 1 year) is coagulase-negative Staph; late is viridans strep
- Modified Duke criteria; high surgical threshold
Clinical Presentation
Most patients are asymptomatic after an uncomplicated valve replacement, with only the prosthetic valve click on auscultation to remind the examiner of its presence. Symptoms develop when a complication supervenes — and the tempo of those symptoms is the most important clue to which complication is unfolding.[1]
The prosthetic valve click is the key auscultatory finding. A mechanical valve produces a sharp, metallic, high-pitched clicking sound at the moment of valve closure — loud at the apex for a mitral valve, at the right second intercostal space for aortic valve. A bioprosthetic valve produces a soft, native-sounding closing sound followed by normal S1 or S2; only the click of a mechanical valve is distinctive enough to be recognised at the bedside. Muffling or loss of the click is an alarming sign of valve thrombosis with restricted leaflet motion.[1]
The tempo of presentation discriminates the complications:[1]
- Acute (hours): sudden severe dyspnoea, pulmonary oedema, syncope, or cardiogenic shock in a mechanical-valve patient — think acute valve thrombosis until proven otherwise.
- Subacute (days to weeks): fever, sweats, malaise, new murmur, embolic phenomena — think prosthetic valve endocarditis.
- Gradual (months): slowly worsening dyspnoea and fatigue with a new murmur — think structural valve deterioration or pannus or patient-prosthesis mismatch.
- Insidious: anaemia, jaundice, dark urine from intravascular haemolysis — think paravalvular leak.
- Embolic: transient ischaemic attack, stroke, or systemic embolus — thrombus or vegetation.
- Bleeding: epistaxis, gastrointestinal bleed, bruising, intracranial haemorrhage — over-anticoagulation. [1]
Atypical presentations are deliberately tested. The elderly patient with a degenerating bioprosthetic valve may present with falls, delirium, or decompensated heart failure rather than dyspnoea. The pregnant patient with a mechanical mitral valve may have a first presentation of valve thrombosis in the second trimester as pregnancy-induced hypercoagulability overwhelms subtherapeutic LMWH. The post-operative patient with early PVE may have only low-grade fever and malaise for days before the new murmur emerges. A high index of suspicion and a low threshold for echocardiography are essential.[1][8]
Bedside signs that reward careful examination include the prosthetic click (mechanical), a new regurgitant or stenotic murmur, muffled or absent clicks (thrombosis), signs of heart failure (raised JVP, basal crackles, S3, peripheral oedema), peripheral stigmata of endocarditis (splinter haemorrhages, Osler nodes, Janeway lesions, Roth spots — rare but classic), conjunctival pallor and jaundice (haemolytic anaemia from paravalvular leak), and focal neurological deficit (embolic stroke).[1][8]
Differential Diagnosis
The differential of new symptoms in a patient with a prosthetic valve is the differential of the complications above. Each must be distinguished because management is entirely different.[1]
Valve thrombosis
- Acute dyspnoea, pulmonary oedema, syncope, muffled clicks, new murmur
- INR typically subtherapeutic; precipitant (non-adherence, pregnancy, infection) often identifiable
- TTE shows raised gradient or reduced leaflet motion; TEE confirms thrombus; fluoroscopy shows restricted disc excursion
Structural valve deterioration
- Gradual dyspnoea over months; new murmur in a bioprosthetic valve more than 5 years old
- Rising gradient and new regurgitation on serial echocardiography
- Most often affects a mitral bioprosthesis or a young patient with a bioprosthesis
Prosthetic valve endocarditis
- Fever, new murmur, embolic phenomena, positive blood cultures
- Vegetation, abscess, dehiscence, new regurgitation on TEE
- Modified Duke criteria; high surgical threshold
Paravalvular leak
- New regurgitant murmur, haemolytic anaemia (raised LDH, low haptoglobin, dark urine)
- Regurgitant jet seen on TEE; often posterior mitral or aortic root
- Percutaneous or surgical closure
Pannus
- Gradual valve dysfunction; late post-operative; subacute symptoms
- Restricted leaflet motion; differentiation from thrombus on MDCT (low attenuation = pannus; high attenuation with contrast = thrombus)
- Often requires surgical excision
Patient-prosthesis mismatch
- Persistent high gradient despite normal leaflet motion
- Indexed EOA under 0.85 cm2/m2 (moderate) or 0.65 (severe)
- Prevented at implantation by appropriate sizing
The can't-miss mimic is native-valve pathology in another valve — a patient with a prosthetic mitral valve can still develop critical aortic stenosis, aortic regurgitation, or tricuspid regurgitation that produces dyspnoea and a murmur. A complete echocardiographic survey is mandatory whenever a prosthetic-valve patient presents with new symptoms. Pulmonary embolism is a particular consideration in patients with right-sided prosthetic valves and right-heart symptoms.[1]
Clinical & Bedside Assessment
The focused assessment of a prosthetic-valve patient serves three goals: identify the valve type and position and the anticoagulation status, screen for complications, and detect any precipitant (infection, recent procedure, pregnancy, non-adherence).[1]
History must establish: the valve type and position (mechanical bileaflet aortic? bioprosthetic mitral? TAVI?), the date of surgery (early complications — under 60 days — are different from late), the current anticoagulation (drug, dose, last INR and target), recent procedures (dental work, GI endoscopy, surgery — sources of bacteraemia or interruptions in anticoagulation), adherence (the commonest cause of subtherapeutic INR), fevers, night sweats, weight loss (endocarditis), new symptoms (dyspnoea, chest pain, syncope, palpitations, neurological symptoms), and embolic phenomena (TIA, stroke, peripheral embolus). In women of childbearing age, pregnancy planning and contraception must be addressed because warfarin is teratogenic.[1]
Examination begins with vital signs — fever (endocarditis), blood pressure in both arms (aortic pathology), oxygen saturation, and JVP. The cardiac examination focuses on: the prosthetic valve click (present, muffled, or absent), new or changed murmurs (regurgitation, stenosis, paravalvular leak), signs of heart failure (raised JVP, basal crackles, S3 gallop, hepatomegaly, peripheral oedema), and peripheral stigmata of endocarditis (splinter haemorrhages, Osler nodes, Janeway lesions, Roth spots — rare but high-yield). A focused neurological examination is mandatory if any focal symptoms are reported, since cardioembolic stroke is a leading complication. Examination of the abdomen (splenomegaly in endocarditis, hepatic congestion) and the skin (bruising from over-anticoagulation, peripheral emboli) completes the survey. [1]
Investigations
The investigation of a suspected prosthetic-valve complication is an echocardiography-first strategy, supplemented by fluoroscopy, cardiac CT, and laboratory work tailored to the suspected problem.[1][2]
TTE (transthoracic echo)
- First-line for every prosthetic-valve patient
- Assesses gradients, effective orifice area, regurgitation, LV/RV function, pulmonary pressures
- Always compared with the post-operative baseline and the most recent prior study
- Less sensitive for prosthetic mitral pathology (acoustic shadowing by the prosthesis)
TEE (transoesophageal echo)
- Mandatory for suspected prosthetic mitral pathology, vegetation, abscess, paravalvular leak, thrombus
- Far superior to TTE for posterior structures and the left atrial appendage
- Essential pre-cardioversion and pre-pulmonary-vein isolation
- Required when TTE is non-diagnostic but suspicion is high
Fluoroscopy
- Mechanical valves only: directly visualises leaflet/disc excursion
- Reduced opening/closing angle = obstruction (thrombus or pannus)
- Quick, portable, low radiation; an old and underused tool
Cardiac CT (MDCT)
- Excellent for distinguishing thrombus (contrast-enhancing) from pannus (low attenuation)
- Identifies annular calcification, abscess, pseudoaneurysm
- Essential for TAVI planning (annular sizing, coronary height, access vessel calibre)
Bloods
- INR (therapeutic?), blood cultures × 3 if febrile (endocarditis)
- FBC, reticulocytes, haptoglobin, LDH, bilirubin, urinalysis (haemolysis from paravalvular leak)
- CRP/ESR (inflammation), U&E, LFT, troponin
CXR
- Cardiac silhouette, pulmonary oedema, prosthetic ring position and integrity
- May reveal prosthetic ring dehiscence or cardiomegaly
Named criteria reproduced verbatim
Modified Duke criteria for prosthetic valve endocarditis are the diagnostic standard and must be reproduced exactly as the examiner expects. They are the same criteria used for native-valve endocarditis but applied with the modifications relevant to prosthetic material.[8]
Definite IE is established by either pathological criteria or a combination of clinical criteria: [1]
[8]Clinical Definite IE requires two major, or one major and three minor, or five minor criteria. [1]
[8] [8]Possible IE requires one major and one minor, or three minor. Rejected when a firm alternative diagnosis is made, resolution occurs with antimicrobial therapy for under four days, no pathological evidence at surgery or autopsy, or does not meet criteria above. [1]
The echo findings that satisfy the major criterion are: oscillating intracardiac mass on valve or supporting structures (vegetation), abscess, or new partial dehiscence of a prosthetic valve. For prosthetic valves specifically, TEE is more sensitive than TTE and is recommended when PVE is suspected — the sensitivity of TTE for prosthetic vegetations is only 25 to 50 percent, rising to 82 to 96 percent with TEE. [1]
Prosthetic-valve endocarditis — early vs late
The temporal classification of PVE drives the most likely organism and the empirical antibiotic choice:[8]
Early PVE (under 1 year)
- Often acquired peri-operatively or from line/injection
- Predominant organism: coagulase-negative Staphylococcus (Staph epidermidis), then Staph aureus
- Higher mortality; more likely to need surgery
- Empirical: vancomycin + gentamicin + rifampicin (cover MRSA and Staph)
Late PVE (over 1 year)
- Acquired community — bacteraemia from dental, GI, or urinary source
- Organism profile mirrors native-valve IE: viridans streptococci, then Staph aureus, enterococci, HACEK
- Empirical: vancomycin + gentamicin ± cefepime while awaiting cultures
Management — Resuscitation
The time-critical emergency in prosthetic-valve medicine is acute obstructive valve thrombosis with cardiogenic shock or pulmonary oedema. The mortality approaches 50 percent untreated, and the diagnosis must be made and acted upon within minutes.[1]
The immediate bundle for the unstable prosthetic-valve patient:[1]
- Airway, breathing, circulation — high-flow oxygen, IV access, continuous monitoring.
- Bedside echocardiogram (TTE then TEE) to confirm the diagnosis before committing to fibrinolysis or surgery.
- Fluoroscopy if available — confirms restricted disc excursion in mechanical valves within minutes.
- Decision: surgery vs fibrinolysis — surgical centre available and patient fit for surgery: emergency redo surgery. No surgical centre or patient too unstable to transfer: fibrinolysis (alteplase 10 mg bolus then 90 mg over 90 min for left-sided; streptokinase 1.5 MU over 60 min acceptable for right-sided).
- Avoid thrombolysis if recent surgery, intracranial or gastrointestinal bleed, severe hypertension, or recent trauma.
- Bridging anticoagulation with UFH (aPTT 2 to 2.5 times control) once haemostasis secured.
- Mechanical circulatory support (IABP, Impella, VA-ECMO) as a bridge to definitive therapy in refractory cardiogenic shock. [1]
The other resuscitation scenarios — acute prosthetic valve endocarditis with heart failure or uncontrolled infection, acute paravalvular leak with haemodynamic compromise, acute mechanical valve failure — all converge on emergency or urgent surgery, with antibiotics, mechanical support, and transfusion as temporising measures. The threshold for surgical intervention in PVE is lower than in native-valve IE: heart failure from regurgitation, periannular extension (abscess, fistula, heart block), uncontrolled infection (persistent bacteraemia, fungal or resistant organism), and large mobile vegetation with embolic risk are all surgical indications.[8]
Management — Definitive & Stepwise
The definitive management of a prosthetic-valve patient is dominated by the anticoagulation strategy, which is governed by valve type, valve position, and patient risk factors. Every prescriber of anticoagulation to a prosthetic-valve patient must be able to recite the INR targets from memory.[1][2]
Anticoagulation — the INR targets
INR targets by valve (memorise these)
The full anticoagulation ladder, in the order the examiner expects it:[1][2]
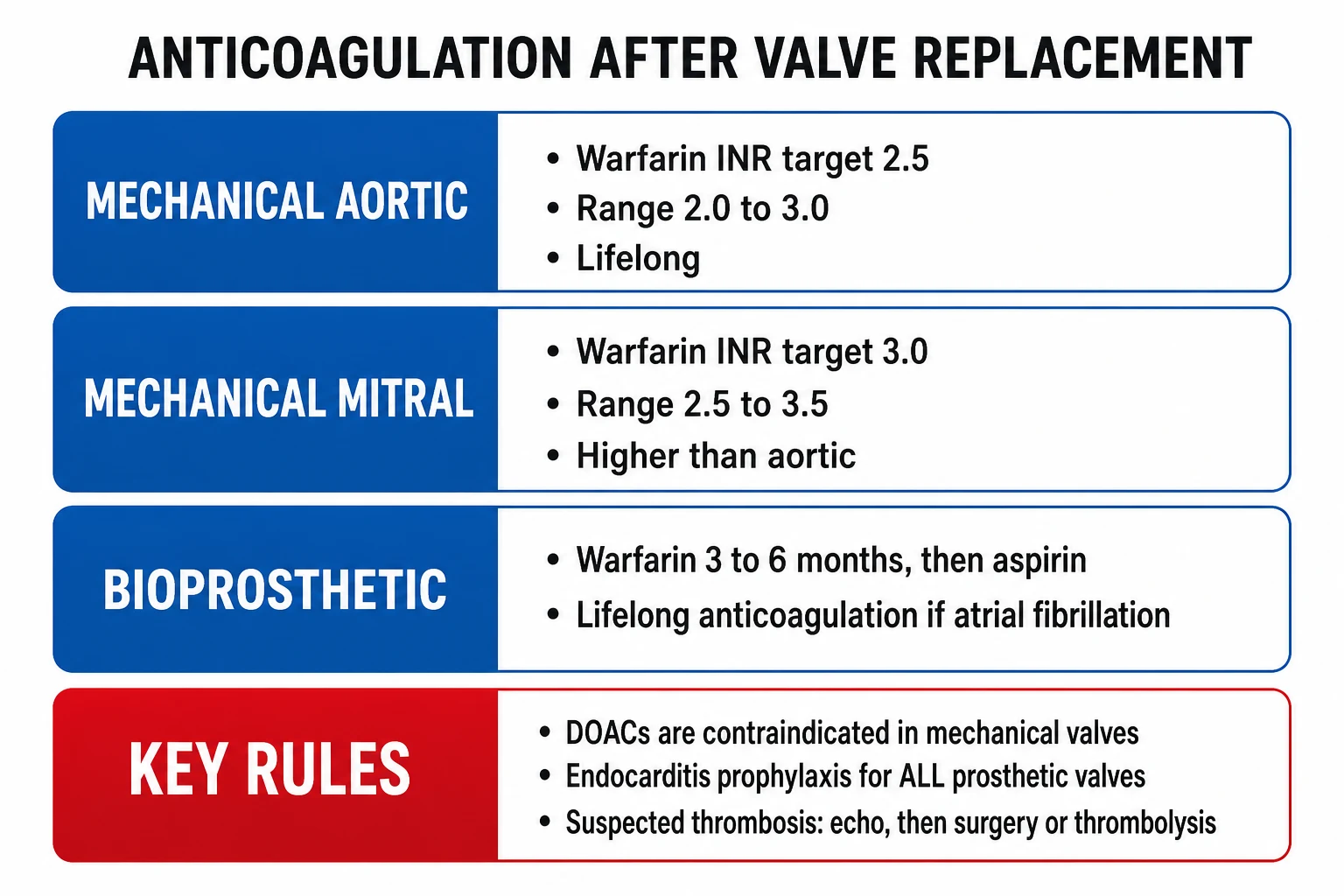
- Mechanical aortic valve, bileaflet, with all low-risk modifiers (sinus rhythm, no LV dysfunction, no left atrial enlargement, no prior thromboembolism): INR target 2.5 (range 2.0 to 3.0). Add aspirin 75 to 100 mg daily.
- Mechanical aortic valve with any high-risk modifier (older-generation valve, atrial fibrillation, prior thromboembolism, hypercoagulable state, LV dysfunction, left atrial enlargement): INR target 3.0 (range 2.5 to 3.5). Add aspirin 75 to 100 mg.
- Mechanical mitral valve: INR target 3.0 (range 2.5 to 3.5). Add aspirin 75 to 100 mg.
- Mechanical tricuspid valve: INR target 3.0 (range 2.5 to 3.5). Bioprosthetic is preferred when feasible because right-sided mechanical valves thrombose at unacceptable rates.
- On-X mechanical aortic valve in selected patients (the only mechanical valve with evidence for a lower INR): INR target 1.5 to 2.0 from 3 months post-implant, per the PROACT trials. Add aspirin 75 to 100 mg. This is the one exception to the standard aortic INR, and it requires the specific On-X valve.[9]
- Bioprosthetic valve (any position): warfarin INR 2.5 (range 2.0 to 3.0) for the first 3 months, then lifelong aspirin 75 to 100 mg daily. If atrial fibrillation coexists, anticoagulate long-term for AF.
- TAVI: lifelong aspirin 75 to 100 mg, with clopidogrel 75 mg for 1 to 6 months (no role for routine dual antiplatelet beyond 6 months). If atrial fibrillation coexists, anticoagulate for AF (warfarin or DOAC); the GALILEO trial showed rivaroxaban post-TAVI without AF caused harm and is not recommended.[7]
The absolute contraindication: DOACs in mechanical valves
For bioprosthetic valves with atrial fibrillation, the picture is different. The RIVER trial (Guimarães, NEJM 2020) randomised patients with a bioprosthetic mitral valve and atrial fibrillation to rivaroxaban versus warfarin and found rivaroxaban non-inferior for death or major bleeding at one year — establishing rivaroxaban as an option for bioprosthetic mitral valves with AF after the early post-operative window. For bioprosthetic aortic valves and TAVI with AF, DOACs are acceptable after the first 3 months.[6]
Management of anticoagulation around procedures
The interruption and bridging of anticoagulation for elective and emergency procedures is an examiner favourite and a daily clinical decision.[1]
Elective surgery — bridging protocol
Stop warfarin 5 days before the procedure (allows INR to fall below 1.5)
Bridge with therapeutic-dose LMWH (e.g. enoxaparin 1 mg/kg twice daily or 1.5 mg/kg once daily) starting 3 days pre-op if high thrombotic risk
Stop LMWH 24 hours before the procedure
Resume warfarin on the evening of, or the day after, the procedure (the same dose, no loading)
Resume LMWH 24 to 72 hours post-op depending on haemostasis, and continue until INR is therapeutic for 2 consecutive days
Check INR within 3 to 5 days of resuming warfarin
Who needs bridging? Bridging is reserved for high thrombotic risk — mechanical mitral valve, older-generation mechanical aortic (tilting disc, caged ball), any mechanical valve with prior thromboembolism, or any mechanical valve with multiple risk factors (AF, hypercoagulable). Low-risk mechanical aortic valves (bileaflet, sinus rhythm) do not require bridging; the BRIDGE trial (2015) showed that for low-risk mechanical aortic valves, omitting bridging was non-inferior for thromboembolism and significantly reduced bleeding. The PERIOP2 trial refined this further.[1]
Dental procedures deserve special mention because they are the commonest source of bacteraemia in prosthetic-valve patients. The 2020 ACC/AHA and 2015 ESC guidelines recommend antibiotic prophylaxis for invasive dental procedures (extractions, scaling, periodontal surgery, implant placement) in all patients with a prosthetic valve. The regimen:[1][8]
Amoxicillin — dental prophylaxis for prosthetic valves
First-line antibiotic prophylaxis against viridans streptococci before invasive dental procedures in patients with a prosthetic valve
Dose
2 g orally, 30 to 60 minutes before the procedure
Emergency surgery in an anticoagulated patient requires rapid reversal of warfarin. The options, in order of speed and completeness:[1]
- Vitamin K 5 to 10 mg intravenously (slow infusion over 20 to 30 minutes to avoid anaphylactoid reaction) — restores functional clotting factor synthesis in 6 to 12 hours but takes up to 24 hours for full effect; the reversal is sustained.
- Prothrombin complex concentrate (PCC) 25 to 50 IU/kg intravenously — reverses within minutes and is preferred for life-threatening bleeding or immediately before emergency surgery. May be combined with vitamin K for sustained reversal.
- Fresh frozen plasma 15 mL/kg — slower and less complete than PCC but widely available.
- Avoid abrupt reversal in mechanical-valve patients without life-threatening bleeding — the thrombotic risk is high. [1]
Pregnancy with a mechanical valve
Pregnancy in a mechanical-valve patient is high-risk by definition — the maternal thromboembolism rate is 5 to 15 percent even with optimal management, and warfarin is teratogenic. The strategy is determined pre-conception.[1]
Continue warfarin throughout
- Lowest maternal thrombosis risk (under 5 percent)
- Risk of warfarin embryopathy (nasal hypoplasia, stippled epiphyses, fetal haemorrhage) — 3 to 10 percent if taken in weeks 6 to 12
- Reasonable if warfarin dose under 5 mg daily (lowest embryopathy risk)
- Stop at 36 weeks and switch to UFH for delivery
Switch to dose-adjusted LMWH (weeks 6 to 12 and after 36)
- Avoids the embryopathy window (weeks 6 to 12 of gestation)
- Twice-daily enoxaparin at therapeutic dose, monitored by anti-Xa (peak 0.8 to 1.2 U/mL 4 to 6 hours post-dose)
- Higher maternal thrombosis risk (5 to 15 percent) — anti-Xa monitoring essential
- Most modern guidelines favour this approach with rigorous monitoring
Dose-adjusted UFH throughout
- Reserved for those who cannot be managed with LMWH
- aPTT target 2 to 3 times control; hospital admission for monitoring
- Less effective than LMWH; historic approach
Switch to LMWH throughout pregnancy
- Completely avoids warfarin (no embryopathy)
- Requires intensive anti-Xa monitoring; high adherence required
- Higher thrombosis risk; reserved for patients who choose to avoid warfarin entirely after counselling
Definitive treatment of each complication
The definitive treatments map onto the differential:[1][8]
- Valve thrombosis, obstructive with shock: emergency surgery; fibrinolysis if surgery unavailable.
- Valve thrombosis, non-obstructive or stable: slow UFH infusion and re-image; many small thrombi resolve with anticoagulation alone.
- Structural valve deterioration: re-operation (redo surgery) for younger surgical candidates; valve-in-valve TAVI for elderly or high-risk surgical patients with a degenerated bioprosthetic aortic valve.
- Paravalvular leak: percutaneous closure (Amplatzer vascular plug) for symptomatic or haemolysing leaks; surgical repair for large leaks or those with infection.
- Pannus: surgical excision or valve replacement (pannus does not respond to anticoagulation or fibrinolysis).
- Endocarditis: organism-targeted IV antibiotics for 4 to 6 weeks; surgery for heart failure, uncontrolled infection, large mobile vegetation, periannular extension (abscess, fistula, heart block), or infection with resistant organism.
- Patient-prosthesis mismatch: prevention at implantation; valve-in-valve or surgical replacement for severe symptomatic PPM. [1]
Stepwise management summary
- Diagnose the complication (TTE plus TEE, fluoroscopy for mechanical valves, MDCT to distinguish thrombus from pannus, blood cultures × 3 if febrile).
- Review anticoagulation — INR target, adherence, drug interactions, recent interruptions.
- Treat the complication — thrombolysis or surgery for thrombosis; antibiotics for endocarditis; re-operation or valve-in-valve TAVI for structural deterioration; closure for paravalvular leak.
- Bridge any interruption of anticoagulation with LMWH or UFH.
- Plan long-term follow-up — TTE annually for mechanical valves, annually for bioprosthetic valves after 5 years (more often if dysfunction suspected); INR monitoring and dose adjustment for mechanical valves.
- Endocarditis prophylaxis for invasive dental procedures (amoxicillin 2 g 30 to 60 min pre-procedure; clindamycin 600 mg if penicillin-allergic).
- Pregnancy planning for all women of childbearing age with mechanical valves — multidisciplinary pre-conception counselling. [1]
Specific Subtypes & Scenarios
TAVI (transcatheter aortic valve implantation) deserves a dedicated scenario because it is now the commonest aortic-valve procedure in the elderly. Indications have expanded from inoperable (PARTNER 1B, 2010) to high-risk (PARTNER 1A, CoreValve US Pivotal), to intermediate-risk (PARTNER 2, SURTAVI), and to low-risk patients (PARTNER 3, Evolut Low Risk), with TAVI showing non-inferiority or superiority over surgery across the spectrum. The anticoagulation strategy post-TAVI is lifelong aspirin 75 to 100 mg, with clopidogrel for 1 to 6 months. The GALILEO trial (Räber, NEJM 2020) tested rivaroxaban 10 mg versus aspirin post-TAVI in patients without another indication for anticoagulation and was stopped early for harm — rivaroxaban increased death, thromboembolism, and bleeding. The lesson: routine rivaroxaban post-TAVI is not recommended; anticoagulate only for AF or another clear indication.[5][7]
TAVI complications to know: new conduction disturbance and permanent pacemaker (5 to 10 percent balloon-expandable, 10 to 25 percent self-expanding — the self-expanding frame compresses the AV node and left bundle), paravalvular leak (more common than surgical; reduced with newer-generation valves and post-dilatation), coronary obstruction (rare but catastrophic — risk in low coronary ostia and native leaflet calcium), annular rupture (rare, in heavily calcified annuli), stroke (2 to 5 percent peri-procedural), and vascular access complications. Structural deterioration of TAVI valves is increasingly recognised at 5 to 10 years but the data are still maturing.[5][7]
On-X mechanical aortic valve with lower INR is the one modern exception to the standard aortic INR. The On-X bileaflet valve has a pure-carbon design with a smoother bileaflet surface and a more laminar flow profile, reducing thrombogenicity. The PROACT trials (initial PROACT and the subsequent PROACT Xa) demonstrated that selected aortic On-X patients can be safely managed at INR 1.5 to 2.0 (with aspirin) from 3 months post-implant, with non-inferior thromboembolism and reduced bleeding. The PROACT Xa trial design (Whalley, 2020) formally tested apixaban versus warfarin for On-X aortic valves but was discontinued early due to excess thromboembolic events with apixaban — reaffirming that even on the On-X platform, DOACs are not acceptable for mechanical valves.[9]
Bioprosthetic valve with atrial fibrillation — the modern evidence supports DOAC use after the early post-operative window. The RIVER trial (Guimarães, NEJM 2020) established rivaroxaban as non-inferior to warfarin in patients with a bioprosthetic mitral valve and AF, at 12 months. Sub-analyses of ARISTOTLE (apixaban) and ROCKET-AF (rivaroxaban) with small bioprosthetic subgroups also support DOAC use. The current consensus: warfarin for the first 3 months post-implant, then a DOAC may be used for the AF indication (apixaban or rivaroxaban) — DOACs are acceptable in bioprosthetic valves but absolutely contraindicated in mechanical valves.[6]
Mechanical mitral valve with subtherapeutic INR — urgent INR recheck; if asymptomatic, dose-adjust warfarin and recheck within days; if symptomatic (dyspnoea, new murmur, muffled click), admit, bridge with UFH, and image with TEE for thrombus. A small non-obstructive thrombus may resolve with UFH alone; an obstructive thrombus requires surgery or fibrinolysis.[1]
Pregnancy with a mechanical valve — high-risk; managed pre-conception in a joint obstetric-cardiac-haematology clinic. Strategy as above (continue warfarin if under 5 mg with counselling, or dose-adjusted LMWH with anti-Xa monitoring). Peripartum: switch to UFH at 36 weeks, stop at onset of labour, resume 4 to 6 hours postpartum, restart warfarin postpartum (safe in breastfeeding).[1]
Pulmonary position — most often a bioprosthesis (percutaneous Melody or Sapien valve) in congenital pulmonary regurgitation or stenosis (e.g. after repair of tetralogy of Fallot). Anticoagulation: aspirin alone; warfarin only if another indication.[2]
Complications & Pitfalls
The complications of a prosthetic valve are the complications enumerated above; the pitfalls are the classic errors that cost marks and lives.[1]
Complication rates (memorise the order of magnitude)
Mechanical thrombus vs pannus
- Both cause prosthetic valve obstruction with restricted leaflet motion
- Thrombus: acute, INR subtherapeutic, soft on imaging, responds to fibrinolysis
- Pannus: chronic, INR often therapeutic, dense fibrous tissue, does not lyse — needs surgery
- Cardiac CT distinguishes: thrombus enhances with contrast; pannus is low-attenuation
Paravalvular leak vs intravalvular regurgitation
- Paravalvular: outside the sewing ring — suture dehiscence, infection; causes haemolysis
- Intravalvular: through the prosthesis — structural leaflet deterioration or thrombus preventing closure
- TEE essential for the distinction; management differs (closure vs re-operation)
PPM vs structural dysfunction
- Both produce a high transprosthetic gradient
- PPM: indexed EOA under 0.85 cm2/m2 with normal leaflet motion; present from implant
- SVD: rising gradient over time with abnormal leaflet motion
- Surgical history and serial echo distinguish them
Classic pitfalls that examiners reward:[1]
- Prescribing a DOAC to a mechanical-valve patient — the single most preventable catastrophic error. Always check valve type before prescribing any anticoagulant.
- Assuming a normal TTE excludes prosthetic mitral pathology — acoustic shadowing by the prosthesis hides vegetations and thrombi; TEE is mandatory for suspected mitral pathology.
- Withholding endocarditis prophylaxis for dental procedures in a prosthetic-valve patient — prophylaxis is recommended for all prosthetic-valve patients, unlike in many lower-risk native-valve conditions.
- Treating over-anticoagulation too aggressively — giving high-dose vitamin K to a mechanical-valve patient with a slightly high INR and minor bleeding causes a difficult-to-reverse hypercoagulable rebound. The reversal strategy must match the bleeding severity.
- Failing to bridge high-risk patients for surgery — a mechanical mitral valve without bridging has an unacceptable thrombosis risk.
- Forgetting pregnancy planning in a young woman with a mechanical valve — warfarin is teratogenic and the strategy must be agreed pre-conception.
- Confusing warfarin embryopathy timing — the critical window is weeks 6 to 12 of gestation; warfarin is also avoided after 36 weeks for delivery. [1]
Prognosis & Disposition
The prognosis of a prosthetic-valve patient depends on valve type, patient age and comorbidity, and the occurrence of complications.[1]
Survival after valve replacement
Disposition is outpatient management for the uncomplicated prosthetic-valve patient, with regular INR monitoring (mechanical) and structured echocardiographic follow-up (all). Inpatient management is required for any complication — suspected or confirmed thrombosis, endocarditis, haemodynamically significant paravalvular leak, structural deterioration with heart failure, or bleeding from over-anticoagulation. The safety-net is a low threshold for echocardiography in any symptomatic prosthetic-valve patient and a low threshold for blood cultures in any febrile prosthetic-valve patient.[1]
- Baseline TTE before discharge after implantation (the reference for all future comparisons).
- TTE at 6 to 12 months post-implant (catches early dysfunction, PPM, paravalvular leak).
- TTE annually for mechanical valves from then on (asymptomatic thrombus, endocarditis surveillance, ventricular function).
- TTE annually for bioprosthetic valves after 5 years (or sooner if symptoms); before 5 years, every 1 to 2 years is acceptable.
- TTE any time there is a change in clinical status (new murmur, fever, dyspnoea, embolic event).
- INR monitoring for mechanical valves — every 4 weeks for stable patients; more frequently after dose changes, with new medications (especially antibiotics and amiodarone, which interact with warfarin), or with intercurrent illness. Self-monitoring devices improve time-in-therapeutic-range. [1]
Special Populations
Pregnancy is the highest-risk special population for mechanical-valve patients. The strategy is determined pre-conception: continue warfarin if dose under 5 mg daily after counselling about the 3 to 10 percent embryopathy risk, or switch to dose-adjusted LMWH (anti-Xa 0.8 to 1.2 U/mL peak) for weeks 6 to 12 and after 36 weeks. Multidisciplinary care (obstetric, cardiac, haematology, anaesthesia, neonatology) at a specialist centre is essential. The maternal thromboembolism rate remains 5 to 15 percent even with optimal management; valve thrombosis in pregnancy is treated with UFH, fibrinolysis, or surgery depending on the situation.[1]
Paediatric patients pose the dual problem of anticoagulation in active children and a growing annulus that will outgrow any fixed-size prosthesis. Mechanical valves are used for size mismatch in older children but require warfarin (challenging in active children); bioprosthetic valves avoid anticoagulation but degenerate faster in the young. The Ross procedure (autotransplant of the pulmonary valve to the aortic position, with a homograft in the pulmonary position) is the surgical choice for young patients with aortic valve disease, avoiding long-term anticoagulation at the cost of two-valve surgery. Anticoagulation is with aspirin alone after a Ross procedure.[2]
The elderly are best served by bioprosthetic or transcatheter valves. The lower anticoagulation risk, the lower tolerance of re-operation, and the competing risks of comorbidity all favour avoiding mechanical valves. TAVI is now the default for severe symptomatic aortic stenosis in patients over 75 to 80, and increasingly in younger patients after shared decision-making.[5]
Chronic kidney disease presents a genuine dilemma: bioprosthetic valves calcify faster in CKD (accelerated SVD), but warfarin monitoring is harder and the bleeding risk is higher. The trend is toward bioprosthetic valves in advanced CKD, recognising the limited life expectancy. TAVI is an option but contrast load for planning must be minimised.[1]
Atrial fibrillation changes the anticoagulation question decisively. In a mechanical valve, AF is an additional indication but the anticoagulation is already warfarin (often with INR pushed to 3.0 and aspirin added). In a bioprosthetic valve, AF mandates long-term anticoagulation — warfarin for the first 3 months, then a DOAC (apixaban, rivaroxaban, dabigatran, edoxaban) per the RIVER and post-marketing data.[6]
Anticoagulated elderly fall-risk patients present the recurrent dilemma of a mechanical valve and a high bleeding risk. Mitigation includes careful INR control, self-monitoring, falls-prevention programmes, and — in selected cases — conversion of a failed bioprosthetic to a valve-in-valve TAVI rather than re-operation. [1]
Evidence, Guidelines & Regional Differences
The evidence base for prosthetic-valve medicine has been transformed by three threads of trial data: the guideline updates (ACC/AHA 2020, ESC/EACTS 2021), the TAVI expansion (PARTNER, CoreValve, SURTAVI, Evolut Low Risk, PARTNER 3), and the anticoagulation trials (RE-ALIGN, RIVER, GALILEO, PROACT, PROACT Xa).[1][2]
RE-ALIGN
N Engl J Med (Eikelboom et al.)
Randomised phase II dose-finding trial of dabigatran versus warfarin in patients with mechanical mitral or aortic valves
Key finding
Stopped early for increased valve thrombosis, stroke, and major bleeding with dabigatran compared with warfarin
Practice change
DOACs are absolutely contraindicated in any mechanical valve — warfarin is the only acceptable anticoagulant
RIVER
N Engl J Med (Guimaraes et al.)
Randomised trial of rivaroxaban versus warfarin in patients with a bioprosthetic mitral valve and atrial fibrillation
Key finding
Rivaroxaban non-inferior to warfarin for the composite of death, major bleeding, or thromboembolic events at 12 months
Practice change
DOACs (rivaroxaban, and by extension apixaban) are acceptable for bioprosthetic mitral valves with AF after the early post-operative window
GALILEO
N Engl J Med (Raber et al.)
Randomised trial of rivaroxaban 10 mg plus aspirin versus clopidogrel plus aspirin after TAVI in patients without another anticoagulation indication
Key finding
Stopped early for harm — rivaroxaban increased death, thromboembolic events, and major bleeding compared with the antiplatelet strategy
Practice change
Routine rivaroxaban after TAVI is not recommended in patients without AF — anticoagulate only for a clear indication
PROACT and PROACT Xa (On-X lower-INR platform)
Am Heart J (Whalley et al. 2020, design) and J Am Coll Cardiol (PROACT)
PROACT: randomised trial of lower INR (1.5 to 2.0) versus standard INR (2.0 to 3.0) in selected aortic On-X mechanical valves. PROACT Xa: apixaban versus warfarin in On-X aortic valves
Key finding
PROACT: lower INR non-inferior for thromboembolism with reduced bleeding — On-X permits INR 1.5 to 2.0 from 3 months. PROACT Xa: discontinued early for excess thromboembolic events with apixaban
Practice change
On-X aortic valve uniquely permits lower INR 1.5 to 2.0 (with aspirin); DOACs remain contraindicated even on the On-X platform
CoreValve US Pivotal
N Engl J Med (Adams et al.)
Randomised trial of self-expanding CoreValve TAVI versus surgical AVR in high-risk severe aortic stenosis
Key finding
TAVI non-inferior (and numerically superior) to surgery for all-cause mortality at 1 year
Practice change
Established self-expanding TAVI as a standard alternative to surgery in high-risk severe AS, expanding the TAVI indication beyond inoperable patients
The 2021 ESC/EACTS Guidelines (Vahanian et al.) are the European standard. They are concordant with the ACC/AHA on the INR targets, the DOAC contraindication, and the role of TAVI, but are more directive on individualised decision-making and on the timing of bioprosthetic anticoagulation. The 2015 ESC IE Guidelines (Habib et al.) define the modified Duke criteria and remain the standard for prosthetic-valve endocarditis management (a 2023 update by Delgado et al. refines but does not replace them).[2][8]
Where the evidence is weak or controversial. The duration of clopidogrel after TAVI is unresolved (trials range from 1 to 6 months, with no clear signal for benefit beyond 6 months). The role of computed tomography for routine surveillance of structural deterioration is evolving. The optimal management of small subclinical leaflet thrombosis on CT (HALT — hypoattenuated leaflet thickening) is uncertain; most are managed with anticoagulation but the clinical significance is debated. The PROACT Xa trial was discontinued early, leaving open whether any DOAC strategy will ever be safe for mechanical valves (the current consensus: no).[9]
Exam Pearls
When NOT to use a DOAC
DOAC DENY
In any mechanical valve — RE-ALIGN (dabigatran harm)
Lower INR 1.5 to 2.0 OK (PROACT) — but still warfarin, not DOAC
Need warfarin lifelong + aspirin 75 to 100 mg
Three months — bioprosthetic valve, warfarin INR 2.5, then aspirin
All prosthetic valves need amoxicillin 2 g pre-procedure
Vitamin K 5 to 10 mg IV, or PCC 25 to 50 IU/kg for life-threatening bleed
BRIDGE/PERIOP2: omit bridging for low-risk mechanical aortic valves
Mechanical valve + pregnancy = pre-conception plan, anti-Xa monitoring
- Mechanical valve = lifelong warfarin — INR 3.0 (range 2.5 to 3.5) mitral or tricuspid; INR 2.5 (range 2.0 to 3.0) aortic with low-risk modifiers; add aspirin 75 to 100 mg.
- DOACs CONTRAINDICATED in any mechanical valve (RE-ALIGN trial — dabigatran caused more thrombosis and stroke).
- Bioprosthetic valve = warfarin INR 2.5 (range 2.0 to 3.0) for 3 months, then aspirin 75 to 100 mg lifelong.
- On-X aortic valve is the only mechanical valve that allows INR 1.5 to 2.0 (with aspirin).
- Acute valve thrombosis with shock = emergency surgery first; thrombolysis if surgery unavailable.
- Pregnancy with mechanical valve = pre-conception plan; warfarin if under 5 mg daily after counselling, or dose-adjusted LMWH (anti-Xa 0.8 to 1.2 U/mL); avoid warfarin weeks 6 to 12 and after 36 weeks.
- Dental prophylaxis = amoxicillin 2 g orally 30 to 60 min pre-procedure; clindamycin 600 mg if penicillin-allergic.
- Bridging for surgery = stop warfarin 5 days pre-op; bridge with LMWH if high thrombotic risk (mechanical mitral, prior TE, older-generation aortic, multiple risk factors); stop LMWH 24 hours pre-op.
- Emergency reversal = vitamin K 5 to 10 mg IV slowly; PCC 25 to 50 IU/kg for life-threatening bleed.
- New murmur + fever = prosthetic valve endocarditis — three sets of blood cultures, TTE and TEE (TEE mandatory for mitral), IV antibiotics; surgery for heart failure, uncontrolled infection, large vegetation, abscess.
- TTE every year for mechanical valves; bioprosthetic valves annually after 5 years.
- Rivaroxaban post-TAVI without AF = harm (GALILEO trial) — do not routinely anticoagulate post-TAVI.
- DOAC OK in bioprosthetic valve + AF after 3 months (RIVER trial for mitral; sub-analyses of ARISTOTLE/ROCKET for aortic).
- Modified Duke criteria — definite IE: 2 major, or 1 major + 3 minor, or 5 minor; TEE more sensitive than TTE for prosthetic valves.
- Thrombus vs pannus — thrombus is acute, soft, INR subtherapeutic, responds to fibrinolysis; pannus is chronic, dense, INR therapeutic, needs surgery; cardiac CT distinguishes them.[1][8]
Exam application bank (NEET-PG / INICET)
One-line answer
Prosthetic heart valves are either mechanical (pyrolytic carbon bileaflet, tilting disc, or caged ball; durable for life but thrombogenic, mandating lifelong warfarin — INR 2.5 to 3.5 mitral, 2.0 to 3.0 aortic) or bioprosthetic / tissue (bovine pericardial Carpentier-Edwards, porcine Hancock; no lifelong anticoagulation but structural deterioration over 10 to 15 years). Transcatheter (TAVI/TAVR) Edwards SAPIEN and Medtronic CoreValve/Evolut serve elderly high-risk severe aortic stenosis. DOACs are contraindicated in mechanical valves (RE-ALIGN trial). Bioprosthetic valves need warfarin for 3 months then aspirin. Acute valve thrombosis is an emergency: surgery if obstructive, thrombolysis if surgery unavailable.
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard. [1]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes. [1]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change. [1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each. [1]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory. [1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Prosthetic Valves and Anticoagulation.
References
- [1]Otto CM, Nishimura RA, Bonow RO, et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines Circulation, 2021.PMID 33332150
- [2]Vahanian A, Beyersdorf F, Praz F, et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease Eur Heart J, 2022.PMID 34453165
- [3]Eikelboom JW, Connolly SJ, Brueckmann M, et al. Dabigatran versus warfarin in patients with mechanical heart valves N Engl J Med, 2013.PMID 23991661
- [4]Capodanno D, Petronio AS, Prendergast B, et al. Standardized definitions of structural deterioration and valve failure in assessing long-term durability of transcatheter and surgical aortic bioprosthetic valves: a consensus statement from the European Association of Percutaneous Cardiovascular Interventions (EAPCI) endorsed by the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS) Eur Heart J, 2017.PMID 29020344
- [5]Adams DH, Popma JJ, Reardon MJ, et al. Transcatheter aortic-valve replacement with a self-expanding prosthesis N Engl J Med, 2014.PMID 24678937
- [6]Guimaraes HP, Lopes RD, de Barros E Silva PGM, et al. Rivaroxaban in Patients with Atrial Fibrillation and a Bioprosthetic Mitral Valve N Engl J Med, 2020.PMID 33196155
- [7]Raber L, Kalesan B, Pilgrim T, et al. A Controlled Trial of Rivaroxaban after Transcatheter Aortic-Valve Replacement N Engl J Med, 2020.PMID 31733180
- [8]Habib G, Lancellotti P, Antunes MJ, et al. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM) Eur Heart J, 2015.PMID 26320109
- [9]Whalley GA, Liu Y, Wang J, et al. Rationale and design of PROACT Xa: A randomized, multicenter, open-label, clinical trial to evaluate the efficacy and safety of apixaban versus warfarin in patients with a mechanical On-X Aortic Heart Valve Am Heart J, 2020.PMID 32693197