Dermatology · Medicine
Alopecia areata
Also known as Patchy alopecia areata · Alopecia totalis · Alopecia universalis · Ophiasis · Sisaipho
Alopecia areata is an organ-specific autoimmune disease directed against anagen hair follicles, producing non-scarring hair loss that ranges from discrete patches to total scalp or body hair loss. Fellowship-level assessment requires mastery of pathophysiology (immune-privilege collapse, CD8+NKG2D+ T cells, JAK-STAT signalling), clinical patterns and prognostic variants, trichoscopic and histopathological clues, severity assessment with the SALT score, stepwise topical/intralesional/contact-immunotherapy management, and the place of oral JAK inhibitors (baricitinib, ritlecitinib, deuruxolitinib) in severe disease.
On this page & tools
Your progress
Saved locally on this device.
Exam tags
Red flags
Definition & Classification
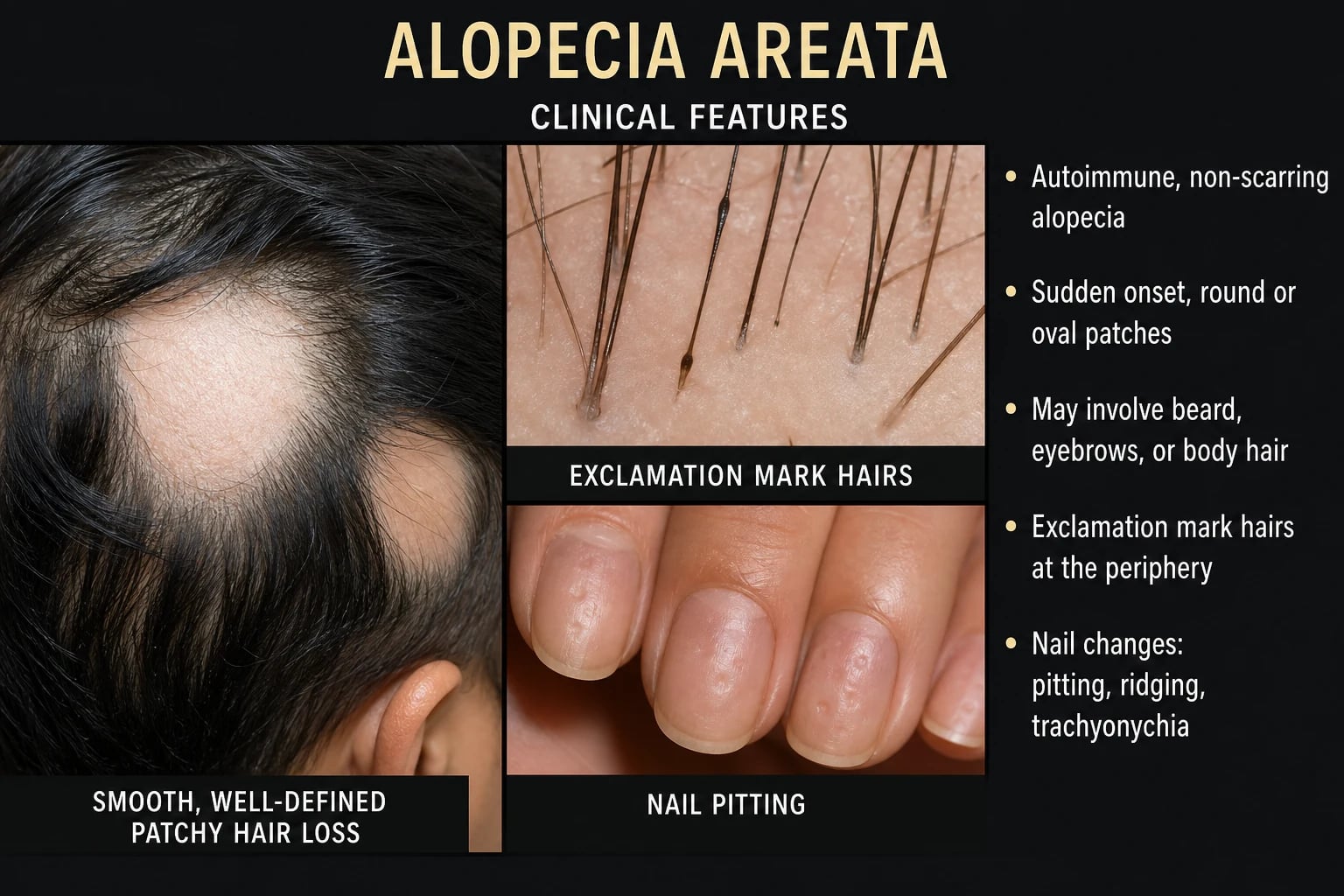
Alopecia areata (AA) is a T-cell-mediated autoimmune disease directed at anagen hair follicles. The characteristic lesion is a well-demarcated patch of non-scarring alopecia with preserved follicular openings, although the disease ranges from a single patch to complete body hair loss. The classification by extent, distribution, and morphology carries direct prognostic and therapeutic implications and must be specified in every clinic letter.[1]
Clinical patterns of alopecia areata
The six classically described clinical patterns span the full spectrum of disease, from self-limiting focal loss to total body alopecia. Each pattern has its own demographic tendency, prognostic signature, and expected treatment response, and the same patient can transition between patterns over time.[1][14]
Patchy alopecia areata is the commonest phenotype, accounting for the majority of new diagnoses. It presents as one or more discrete round or oval smooth bald patches, often first noticed by the patient, a hairdresser, or a family member. The patches are typically asymptomatic, may be associated with mild paraesthesia or pruritus in some patients, and demonstrate preserved follicular ostia on close inspection. Gentle traction at the active border extracts dystrophic anagen hairs, and exclamation-mark hairs (short broken shafts narrower proximally) are visible at the margin. Patchy disease carries the best prognosis, with spontaneous regrowth in 30–50% of patients within 6–12 months and the strongest response to intralesional and potent topical corticosteroids. Recurrence at the same or distant site is common, and patients should be counselled that one episode does not confer lasting immunity. [1]
Alopecia totalis (AT) denotes complete or near-complete (>95%) scalp hair loss without significant body-hair involvement. It represents the upper end of severity and is uncommon, occurring in approximately 5% of AA cohorts. AT carries a markedly poorer prognosis than patchy disease, with spontaneous regrowth occurring in fewer than 10% of patients. The psychological burden is high because the cosmetic change is complete and immediate, and AT is a recognised indication for early escalation to systemic immunomodulatory therapy, including oral JAK inhibitors, in adults and adolescents. [1]
Alopecia universalis (AU) is the most extensive phenotype, defined as complete loss of scalp hair and all body hair, including eyebrows, eyelashes, axillary, and pubic hair. Loss of nasal hair may produce rhinitis and dryness, and loss of eyebrow/eyelash hair removes important eye protection. AU is the most refractory form, with reported spontaneous regrowth below 5%. It is a formally recognised indication for systemic JAK inhibitor therapy, and the response rate to baricitinib, ritlecitinib, and deuruxolitinib in AU has been incorporated into the pivotal trial programmes.[17][18][20]
Ophiasis describes a band-like pattern of hair loss along the temporal, parietal, and occipital scalp margins, sparing the central vertex. The term derives from the Greek ophis (snake) because the affected area resembles a serpent encircling the scalp. Ophiasis accounts for 5–10% of paediatric cases and carries a poor prognosis, with limited response to local therapy and a high rate of progression to more extensive disease. The marginal distribution may relate to regional differences in follicular antigen expression or immune-cell trafficking. Patients with ophiasis should be considered for early systemic therapy even when the percentage scalp loss is modest, because the pattern is intrinsically resistant. [1]
Sisaipho (sometimes called inverse ophiasis) is the mirror image of ophiasis, with hair loss sparing the scalp periphery and involving the central scalp. The name is the reverse spelling of ophiasis. It is uncommon, often described in association with more aggressive disease, and may evolve into alopecia totalis. Like ophiasis, central/parietal-vertex sisaipho disease should be regarded as a poor prognostic marker and discussed with the patient when planning therapy. [1]
Diffuse alopecia areata (also called alopecia areata incognita) presents with widespread, often acute, hair thinning that can closely mimic telogen effluvium or early androgenetic alopecia. The diagnosis is easily missed without trichoscopy, which reveals the characteristic yellow dots, exclamation-mark hairs, and black dots that are not seen in true telogen effluvium. A high index of suspicion is warranted when "telogen effluvium" persists for more than 6 months or is unusually severe, particularly in adolescents and young adults. [1]
| Pattern | Definition | Prognostic notes |
|---|---|---|
| Patchy alopecia areata | One or more discrete round/oval bald patches | Often self-limiting; good response to local therapy |
| Alopecia totalis | Complete scalp hair loss | More refractory |
| Alopecia universalis | Complete scalp and body hair loss | Most refractory |
| Ophiasis | Band-like hair loss along the temporal/occipital scalp margins | Poor prognosis; resistant to treatment |
| Sisaipho | Hair loss sparing the periphery (inverse ophiasis) | Uncommon |
| Diffuse alopecia areata | Widespread thinning mimicking telogen effluvium | Easily missed without trichoscopy |
Nail changes occur in 10–30% of patients and include fine geometric pitting, trachyonychia, onychomadesis, or leukonychia; these can be the presenting feature in children.[1]
Epidemiology & Risk Factors
The lifetime risk of AA is approximately 2%, with a population prevalence commonly cited around 0.1–0.2% in community-based studies. It can begin at any age, but onset peaks in the second to fourth decades, and there is no consistent sex predominance.[2]
Genetic factors [1]
- Positive family history is reported in 10–25% of patients.
- Genome-wide association studies implicate HLA associations, CTLA4, IL2/IL21, STX17, and the ULBP gene cluster encoding NKG2D ligands.[4]
- Down syndrome carries a markedly increased risk of AA.[1]
Environmental and triggering factors [1]
- Psychological stress has long been linked anecdotally; recent work places greater emphasis on psychological comorbidity as a consequence requiring management rather than a sole cause.[1][25]
- Infections, trauma (Koebner phenomenon), and hormonal changes are recognised triggers in susceptible individuals.[1]
Pathophysiology
AA is best understood as a collapse of the hair-follicle immune privilege, followed by autoimmune attack on anagen follicles. [1]
The immune circuit
- Loss of immune privilege — normally anagen hair follicles down-regulate MHC class I and produce immune-privilege molecules (e.g., MIF, α-MSH, TGF-β). Triggering events are thought to expose follicular autoantigens.[1]
- CD8+NKG2D+ T cells — these cytotoxic T cells are the key effectors. They recognise hair-follicle antigens and release IFN-γ, which up-regulates MHC class I/II on follicular epithelium, perpetuating the attack.[5]
- JAK-STAT amplification — IFN-γ signals via JAK1/JAK2; IL-15 and other γc cytokines signal via JAK1/JAK3. Together they sustain CD8+ T-cell survival and cytotoxicity, creating a self-reinforcing inflammatory loop.[5]
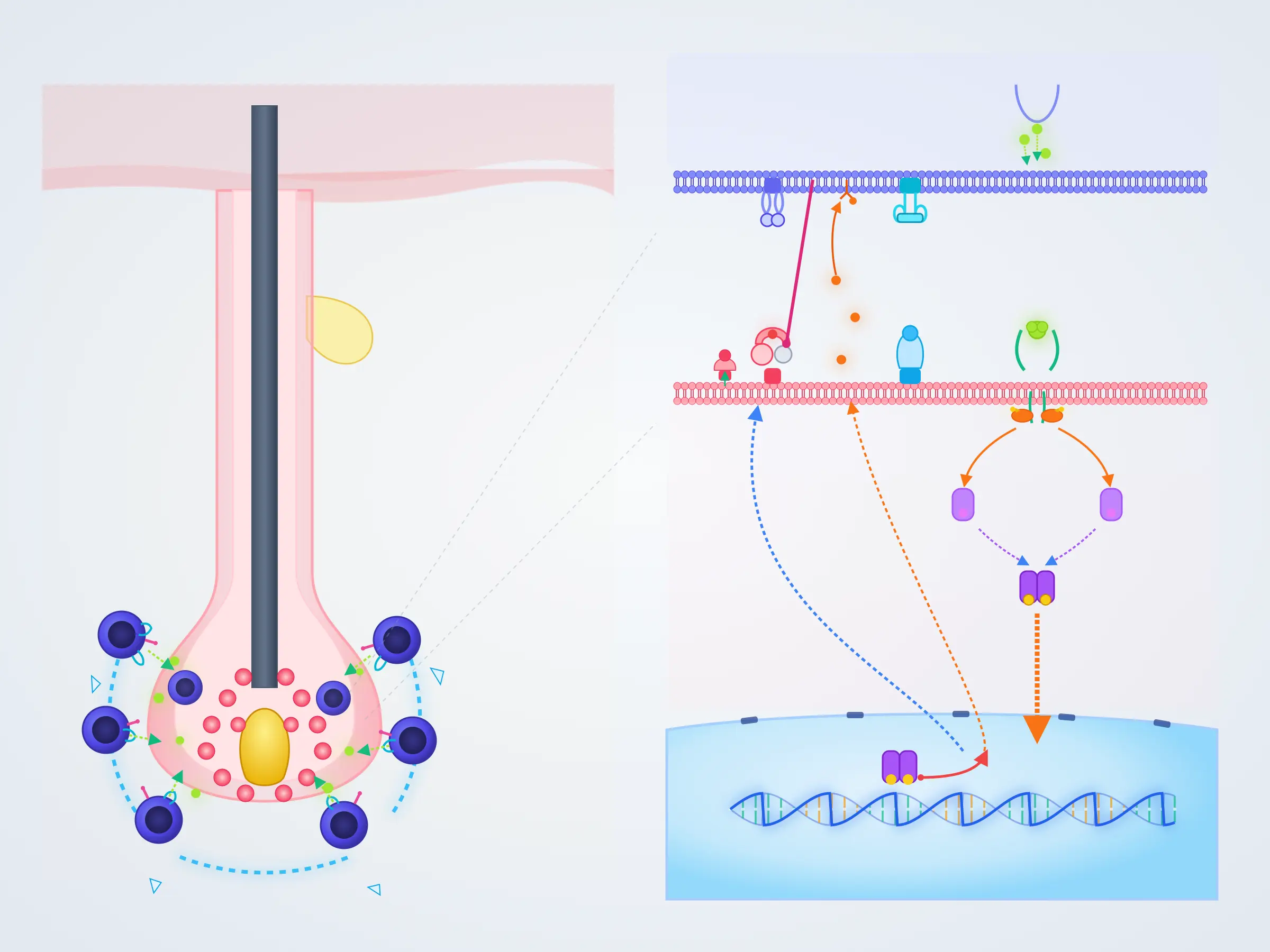
Why JAK inhibition works
Because IFN-γ and γc cytokines depend on JAK-STAT signalling, JAK inhibitors interrupt the central amplification loop. This mechanistic rationale underpins the efficacy of baricitinib, ritlecitinib, and deuruxolitinib in severe AA.[5]
Clinical Presentation
Patchy disease
- Sudden onset of one or more round/oval, smooth, non-scarring patches.
- Exclamation-mark hairs — short, broken hairs that are wider distally and narrower proximally — at the advancing edge are a classic sign of active disease.
- Gentle hair-pull testing at the patch margin may be positive (anagen hairs released). [1]
Extensive disease
- Alopecia totalis — complete scalp hair loss.
- Alopecia universalis — loss of scalp, eyebrows, eyelashes, beard, and body hair.
- Ophiasis — band-like involvement of the temporal and occipital scalp; associated with poorer prognosis and treatment resistance. [1]
Associated nail disease
Fine geometric pitting is the most characteristic; other changes include onychomadesis, trachyonychia, leukonychia, and nail thinning. Nail disease correlates with more severe scalp disease.[1]
Differential Diagnosis
[1]Quick comparison — alopecia areata versus its closest mimics
The three non-scarring and scarring phenotypes that most often confuse the bedside diagnosis can be distinguished by combining the history, scalp examination, and trichoscopy. [1]
Alopecia areata vs telogen effluvium vs scarring (cicatricial) alopecia
Alopecia areata
- Sudden, focal or extensive non-scarring loss
- Smooth bald patches with exclamation-mark hairs at the margin
- Trichoscopy: yellow dots, black dots, exclamation-mark hairs, broken hairs
- Follicular ostia PRESERVED — no scarring
- Often autoimmune/atopic comorbidity; nail pitting in 10–30%
- Autoimmune mechanism: CD8+NKG2D+ T cells, IFN-γ, JAK-STAT
- Treatment: topical/intralesional steroids, contact immunotherapy, JAK inhibitors
Telogen effluvium
- Diffuse shedding 2–3 months after trigger (illness, childbirth, surgery, weight loss, drugs)
- Positive hair-pull test (>6 telogen hairs); NO focal bald patches
- Trichoscopy: upright regrowing hairs, NO yellow or black dots
- Follicular ostia PRESERVED; non-scarring
- Trichogram shows >25% telogen hairs
- Resolves within 6 months in most; no active treatment
- Distinguish from diffuse AA (alopecia areata incognita) by trichoscopy and persistence
Scarring (cicatricial) alopecia
- Permanent destruction of follicles — irreversible hair loss
- Loss of follicular ostia, perifollicular erythema/scale, pustules, atrophy
- Trichoscopy: white patches, fibrosis, loss of ostia, tufted hairs
- Follicular ostia ABSENT — scarring is the discriminator
- Examples: lichen planopilaris, frontal fibrosing alopecia, DLE, CCCA
- Skin biopsy essential; horizontal sections most informative
- Treatment: anti-inflammatory (doxycycline, hydroxychloroquine, topical/intralesional steroid) to halt progression; no regrowth of lost follicles
Clinical & Bedside Assessment
Severity of Alopecia Tool (SALT)
The SALT score is the standard outcome measure in clinical practice and trials. It estimates the percentage of scalp hair loss on a 0–100 scale (0 = no loss, 100 = total loss). It is assessed visually or with computer-assisted methods by dividing the scalp into zones.[17]
| SALT score | Interpretation |
|---|---|
| 0 | No scalp hair loss |
| 1–24 | Mild |
| 25–49 | Moderate |
| 50–94 | Severe |
| 95–100 | Very severe / totalis |
Other useful instruments include the Alopecia Areata Patient Priority Outcomes (AAPPO) scale, which captures patient-reported scalp hair, eyebrow/eyelash, and emotional impacts.[23]
Prognostic assessment
Poor prognostic factors include:
- Onset in childhood
- Atopy
- Ophiasis pattern
- Alopecia totalis/universalis
- Long disease duration
- Positive family history
- Associated nail dystrophy [1]
Investigations
Trichoscopy
Trichoscopy is the first-line bedside investigation. The most characteristic findings are:[6][7]
| Finding | Significance |
|---|---|
| Yellow dots | Follicular infundibula filled with keratin and sebum; common and prominent in severe/chronic disease |
| Black dots (cadaverous hairs) | Broken hair shafts at the surface; marker of disease activity |
| Exclamation-mark hairs | Pathognomonic for active AA |
| Broken hairs | Common in patchy AA |
| Short vellus hairs | Suggest remission or regrowth |
| Tapered hairs (pencil-point) | Pohl-Pinkus constrictions; sign of ongoing activity |
| Clustered short vellus hairs | Marker of regrowth / response to therapy |
Histopathology
A 4-mm punch biopsy is indicated when:
- The diagnosis is uncertain.
- Scarring alopecia is suspected.
- The patient is being considered for systemic therapy requiring histological confirmation. [1]
Horizontal (transverse) sections are particularly helpful. Classic findings include:[8][9]
- Peribulbar lymphocytic infiltrate around anagen follicles — the "swarm of bees" appearance in active disease.
- Increased catagen/telogen ratio with miniaturisation.
- Pigment casts and melanin within fibrous tracts.
- In chronic disease the inflammatory infiltrate may be subtle or absent. [1]
Baseline work-up
- FBC, ferritin, TFT, B12/folate — screen for anaemia, thyroid dysfunction, and nutritional deficiencies that can compound hair loss.
- VDRL/TPPA if syphilis is suspected.
- KOH/culture/PCR if tinea capitis is suspected.
- Consider atopy, vitiligo, and autoimmune thyroid screening because of well-recognised associations.[3][4]
Management — Topical & Intralesional Therapy
Topical and intralesional corticosteroids remain first-line for limited patchy disease. [1]
Intralesional corticosteroids
- Triamcinolone acetonide 2.5–10 mg/mL injected into the dermis of active patches every 4–6 weeks.
- Meta-analysis supports efficacy for patchy AA, with higher concentrations generally more effective but carrying greater risk of atrophy.[11]
- Avoid injection into areas with visible vellus regrowth or atrophic skin.
Topical corticosteroids
- Potent steroids (e.g., betamethasone dipropionate, clobetasol propionate) applied to patches; scalp foam or solution can improve adherence.
- Topical calcineurin inhibitors (tacrolimus, pimecrolimus) are sometimes used on the face or in children where steroid atrophy is a concern, although evidence is mixed. [1]
Minoxidil and adjuncts
- Topical minoxidil can hasten cosmetically visible regrowth but does not treat the underlying inflammation; it is commonly used as an adjunct.
- Systematic reviews of light-based therapies combined with minoxidil suggest modest benefit in some patients.[12]
Management — Phototherapy
Excimer laser / excimer light (308 nm) and narrowband UVB have been used for patchy or extensive AA, particularly when topical therapy has failed. Systematic reviews show variable but measurable benefit, especially for patchy disease; relapse is common after stopping treatment.[12]
Management — Contact Immunotherapy
Topical immunotherapy with diphenylcyclopropenone (DPCP), squaric acid dibutylester (SADBE), or dinitrochlorobenzene (DNCB) is a mainstay for extensive, recurrent, or refractory patchy AA in specialist centres. The mechanism is thought to involve diversion of the local immune response and induction of follicular immune privilege.[10]
- Applied to the scalp weekly in gradually increasing concentrations to produce a mild eczematous reaction.
- Response rates vary widely (9–87% in historical series); best evidence supports use in patients with 30–80% scalp involvement.
- Common adverse effects include local eczema, urticaria, lymphadenopathy, and pigmentary change.[13]
Management — Systemic Non-JAK Therapy
Systemic corticosteroids, methotrexate, ciclosporin, and azathioprine have been used for severe AA, but high-quality evidence is limited. [1]
- Oral corticosteroids — short courses or pulse regimens can produce rapid regrowth, but relapse is common and adverse effects limit long-term use. A network meta-analysis suggests systemic steroids and oral JAK inhibitors both outperform placebo, with contact immunotherapy also effective in severe disease.[13]
- Methotrexate / ciclosporin — sometimes used as steroid-sparing agents or in combination, but robust trial data are lacking; decisions should follow specialist guidance and local formularies.
Management — JAK Inhibitors
Oral JAK inhibitors have transformed management of moderate-to-severe AA (typically SALT ≥50) that is refractory to or unsuitable for topical/contact therapy. They are not curative; relapse is typical after withdrawal.[14][15]
Baricitinib
- Oral JAK1/JAK2 inhibitor approved for adults with severe AA.
- Dose: 2 mg or 4 mg once daily.
- Evidence: In BRAVE-AA1 and BRAVE-AA2, 38.8% and 35.9% of patients achieved SALT ≤20 at week 36 with 4 mg; 22.8% and 19.4% with 2 mg; versus 6.2% and 3.3% with placebo (P<0.001 for each dose vs placebo). Three-year data show sustained benefit with continuous therapy.[17][22]
Ritlecitinib
- Oral selective dual JAK3/TEC-family kinase inhibitor approved for adults and adolescents aged 12 years and older with severe AA.
- Dose: 50 mg once daily (with or without a 4-week 200 mg loading dose per label).
- Evidence: In the ALLEGRO phase 2b/3 trial, 23% of patients on 50 mg achieved SALT ≤20 at week 24 versus 2% with placebo (P<0.001). Adolescent data support efficacy and safety in patients 12 years and older.[18][19]
Deuruxolitinib
- Oral selective JAK1/JAK2 inhibitor approved for adults with severe AA.
- Dose: 8 mg or 12 mg twice daily.
- Evidence: THRIVE-AA1 showed 29.6% (8 mg) and 41.5% (12 mg) achieved SALT ≤20 at week 24 versus 0.8% with placebo; THRIVE-AA2 confirmed efficacy.[20][21]
Pre-treatment screening and safety
Before starting any oral JAK inhibitor:[14][16]
- Screen for tuberculosis (IGRA or Mantoux), hepatitis B/C, HIV as per local guidance.
- Check FBC, LFT, renal function, lipids.
- Review cardiovascular risk, thromboembolic history, malignancy risk, and current infections.
- Update inactivated vaccines; live vaccines are contraindicated during therapy. [1]
Common adverse effects include upper respiratory tract infections, acne, headache, elevated creatine kinase, and lipid abnormalities. Rare but serious class risks include serious infections, herpes zoster, thrombosis, major adverse cardiovascular events, and malignancy; counsel patients and monitor regularly.[17][20]
Treatment doses — at a glance
Alopecia areata — treatment doses for the fellowship viva

Special Populations
Children and adolescents
- Limited patchy disease: topical/intralesional corticosteroids remain first-line; response is often better than in adults.
- Ritlecitinib is approved for adolescents ≥12 years with severe AA based on the ALLEGRO adolescent cohort.[19]
- Psychological support and school liaison are essential; a systematic review of paediatric treatments highlights the need for better paediatric trial data.[24]
Pregnancy and breastfeeding
- JAK inhibitors, methotrexate, and systemic retinoids are contraindicated in pregnancy and conception planning.
- Topical corticosteroids and intralesional corticosteroids can be used cautiously; avoid extensive treatment with potent agents.
- Management should be multidisciplinary with dermatology and obstetrics input. [1]
Comorbidities & Psychosocial Impact
AA is associated with a higher prevalence of atopic disease, autoimmune thyroid disease, vitiligo, type 1 diabetes, inflammatory bowel disease, and ** Down syndrome**; a holistic comorbidity screen is recommended.[3][4]
The psychosocial burden is substantial. A systematic review and meta-analysis found significantly increased odds of depressive and anxiety disorders and symptoms in both children and adults with AA compared with controls.[25] Screening for depression, anxiety, and quality-of-life impairment should be part of routine care.
Prognosis & Follow-Up
Prognosis is highly variable: [1]
- Limited patchy AA often regrows spontaneously within 6–12 months; recurrence is common.
- Ophiasis, AT, AU, childhood onset, atopy, and nail changes predict a more chronic course.
- JAK inhibitors produce meaningful regrowth in a minority to substantial minority of patients, but relapse after withdrawal is typical; long-term continuous therapy is often needed to maintain response.[22]
Follow-up intervals depend on therapy: [1]
- Topical/intralesional: review at 6–8 weeks.
- Contact immunotherapy: weekly applications with response assessment every 8–12 weeks.
- JAK inhibitors: baseline and periodic FBC, LFT, lipids; infection surveillance; vaccination review. [1]
Evidence, Guidelines & Regional Differences
Major guidelines
- British Association of Dermatologists (BAD) living guideline 2024 — comprehensive guidance on diagnosis, psychological support, topical/intralesional therapy, contact immunotherapy, systemic therapy, and JAK inhibitors in adults and children.[14]
- Japanese Dermatological Association (JDA) guidelines 2024 — detailed Japanese recommendations on topical, intralesional, contact, phototherapy, and JAK-inhibitor use.[15]
- Asia-Pacific modified Delphi consensus 2026 — regional expert recommendations emphasising SALT-based severity assessment, infection/vaccination screening, and practical JAK-inhibitor use.[16]
Landmark trials
- BRAVE-AA1 / BRAVE-AA2 (2022) — baricitinib phase 3 in adults; established JAK inhibition as an effective therapy for severe AA.[17]
- ALLEGRO (2023) — ritlecitinib phase 2b/3 in adults and adolescents; led to approval in patients ≥12 years.[18]
- THRIVE-AA1 / THRIVE-AA2 (2024/2026) — deuruxolitinib phase 3 in adults.[20][21]
Fellowship viva — high-yield mnemonic
Alopecia areata — the viva crib (CLINICS)
CLINICS
Cytotoxic T cells are the central effectors; recognise hair-follicle autoantigens after immune-privilege collapse and release IFN-γ to drive JAK-STAT signalling
Pathognomonic trichoscopic finding at the patch margin — short broken shaft wider distally, narrower proximally; also yellow dots and black dots
First-line for limited patchy AA: 2.5–10 mg/mL every 4–6 weeks; avoid face/brow; risk of dermal atrophy limits use on the scalp
Fine geometric pitting, trachyonychia, onychomadesis in 10–30% of patients; correlates with more severe or chronic scalp disease
Anagen follicles down-regulate MHC I and secrete MIF, α-MSH, TGF-β; JAK inhibition and contact immunotherapy (DPCP) restore privilege
Higher prevalence of autoimmune thyroid disease, atopic dermatitis, vitiligo, type 1 diabetes, IBD and Down syndrome — screen for these
Meta-analysis shows significantly increased odds of depressive and anxiety disorders in adults and children — screen with PHQ-9/GAD-7 at every visit
Exam Pearls
[1] [1]AA treatment doses quick numbers
PATCHY-AT-AU - AA severity mnemonic
Single or few patches; 30-50% spontaneous regrowth; topical/intralesional steroids; DPCP if extensive
Trichoscopy shows disease activity; treat aggressively to prevent progression
Alopecia totalis; 5-10% spontaneous regrowth; JAK inhibitors indicated
Topical/intralesional first-line; avoid JAK inhibitors under 12; ritlecitinib FDA-approved 12+
Indicates active disease; guides treatment intensity
More than 10 yr duration with no regrowth; consider avoiding aggressive systemic therapy
Most refractory; under 5% spontaneous regrowth; JAK inhibitors strongly indicated
10-15 mg daily; off-label; multiple case series showing efficacy
Vitiligo, autoimmune thyroid, type 1 diabetes, SLE, atopy; screen if symptomatic
20% of AA; geometric pitting; non-scarring; resolves with regrowth
Red Flags [1]
Exam application bank (NEET-PG / INICET)
One-line answer
Alopecia areata is an organ-specific autoimmune disease directed against anagen hair follicles, producing non-scarring hair loss that ranges from discrete patches to total scalp or body hair loss. Fellowship-level assessment requires mastery of pathophysiology (immune-privilege collapse, CD8+NKG2D+ T cells, JAK-STAT signalling), clinical patterns and prognostic variants, trichoscopic and histopathological clues, severity assessment with the SALT score, stepwise topical/intralesional/contact-immunotherapy management, and the place of oral JAK inhibitors (baricitinib, ritlecitinib, deuruxolitinib) in severe disease.
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard. [1]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes. [1]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change. [1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each. [1]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory. [1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Alopecia areata.
Expanded exam teaching (depth pass)
Clinical reasoning
For Alopecia areata, examiners test whether you can prioritise life threats, choose the right first test, and give specific therapy (agent, dose, route, timing). Generic phrases without numbers score poorly.
Mechanism → feature map
Build a short chain: cause → pathophysiologic intermediate → clinical feature → complication. Every major symptom in the classic vignette should sit on that chain.
Investigation strategy
- Bedside/first-line tests that change immediate management
- Confirmatory or staging tests
- What a normal result does not exclude
- When not to delay treatment for imaging (unstable patient)
Management ladder
- Resuscitation / ABC / sepsis or haemorrhage bundle as relevant
- Specific antidote / procedure / antimicrobial / reperfusion / surgery
- Supportive care and monitoring targets
- Definitive long-term therapy and secondary prevention
- Disposition and safety-net advice
Special populations
Always prepare one line each for children, pregnancy, elderly, renal/hepatic impairment, and immunocompromised patients when the topic allows.
Pitfalls that fail candidates
- Treating the number not the patient
- Missing pregnancy status when relevant
- Imaging before stabilisation
- Wrong empiric cover or wrong antidote timing
- Incomplete counselling on recurrence, adherence, or red-flag return
Alopecia areata is an organ-specific autoimmune disease directed against anagen hair follicles, producing non-scarring hair loss that ranges from discrete patches to total scalp or body hair loss. Fellowship-level assessment requires mastery of pathophysiology (immune-privilege collapse, CD8+NKG2D+ T cells, JAK-STAT signalling), clinical patterns and prognostic variants, trichoscopic and histopathological clues, severity assessment with the SALT score, stepwise topical/intralesional/contact-immu [1]
[1]References
- [1]Fukuyama M, Ito T, Ohyama M. Alopecia areata: Current understanding of the pathophysiology and update on therapeutic approaches, featuring the Japanese Dermatological Association guidelines J Dermatol, 2022.PMID 34709679
- [2]Villasante Fricke AC, Miteva M. Epidemiology and burden of alopecia areata: a systematic review Clin Cosmet Investig Dermatol, 2015.PMID 26244028
- [3]Arousse A, Boussofara L, Mokni S et al. Alopecia areata in Tunisia: epidemio-clinical aspects and comorbid conditions. A prospective study of 204 cases Int J Dermatol, 2019.PMID 30677128
- [4]Herrera-Rivero M, Gossmann Y, Awasthi S et al. Genome-wide association study of atopic and autoimmune comorbidities in alopecia areata Front Immunol, 2026.PMID 42079583
- [5]Xing L, Dai Z, Jabbari A et al. Alopecia areata is driven by cytotoxic T lymphocytes and is reversed by JAK inhibition Nat Med, 2014.PMID 25129481
- [6]Jha AK, Udayan UK, Roy PK et al. Dermoscopy of alopecia areata-a retrospective analysis Dermatol Pract Concept, 2017.PMID 28515996
- [7]Al-Dhubaibi MS, Alsenaid A, Alhetheli G et al. Trichoscopy pattern in alopecia areata: A systematic review and meta-analysis Skin Res Technol, 2023.PMID 37357664
- [8]Genedy RM, Badran FK, Tayae EM et al. Lesson to Learn From Cellular infiltrate in Scalp Biopsy of Alopecia Areata Am J Dermatopathol, 2021.PMID 33606369
- [9]Yadav D, Khandpur S, Ramam M et al. Utility of Horizontal Sections of Scalp Biopsies in Differentiating between Androgenetic Alopecia and Alopecia Areata Dermatology, 2018.PMID 30092597
- [10]Mateos-Haro M, Novoa-Candia M, Sánchez Vanegas G et al. Treatments for alopecia areata: a network meta-analysis Cochrane Database Syst Rev, 2023.PMID 37870096
- [11]Yee BE, Tong Y, Goldenberg A et al. Efficacy of different concentrations of intralesional triamcinolone acetonide for alopecia areata: A systematic review and meta-analysis J Am Acad Dermatol, 2020.PMID 31843657
- [12]Lee JH, Eun SH, Kim SH et al. Excimer laser/light treatment of alopecia areata: A systematic review and meta-analyses Photodermatol Photoimmunol Photomed, 2020.PMID 32745343
- [13]Guan R, Lin Y, Zhang C et al. Comparative efficacy and safety of systemic steroids, oral JAK inhibitors and Contact Immunotherapy in the Treatment of severe alopecia areata: a systematic review and network meta-analysis Arch Dermatol Res, 2024.PMID 39042154
- [14]Harries MJ, Ascott A, Asfour L et al. British Association of Dermatologists living guideline for managing people with alopecia areata 2024 Br J Dermatol, 2025.PMID 39432739
- [15]Ohyama M, Ito T, Amoh Y et al. Japanese Dermatological Association's Clinical Practice Guidelines for Alopecia Areata 2024: A Complete English Translated Version J Dermatol, 2025.PMID 40698756
- [16]Sinclair R, Yang CC, Chung WH et al. Epidemiology, Diagnosis and Management of Alopecia Areata: An Asia-Pacific Modified Delphi Expert Panel Recommendations Int J Dermatol, 2026.PMID 41699409
- [17]King B, Ohyama M, Kwon O et al. Two Phase 3 Trials of Baricitinib for Alopecia Areata N Engl J Med, 2022.PMID 35334197
- [18]King B, Zhang X, Harcha WG et al. Efficacy and safety of ritlecitinib in adults and adolescents with alopecia areata: a randomised, double-blind, multicentre, phase 2b-3 trial Lancet, 2023.PMID 37062298
- [19]Hordinsky M, Hebert AA, Gooderham M et al. Efficacy and safety of ritlecitinib in adolescents with alopecia areata: Results from the ALLEGRO phase 2b/3 randomized, double-blind, placebo-controlled trial Pediatr Dermatol, 2023.PMID 37455588
- [20]King B, Senna MM, Mesinkovska NA et al. Efficacy and safety of deuruxolitinib, an oral selective Janus kinase inhibitor, in adults with alopecia areata: Results from the Phase 3 randomized, controlled trial (THRIVE-AA1) J Am Acad Dermatol, 2024.PMID 39053611
- [21]Tsianakas A, Passeron T, Magnolo N et al. Efficacy and safety of deuruxolitinib, an oral selective Janus kinase 1/2 inhibitor, in adults with alopecia areata: Results from the THRIVE-AA2 Phase 3, randomized, double-blind, controlled trial J Am Acad Dermatol, 2026.PMID 41317911
- [22]Senna M, Mostaghimi A, Sinclair R et al. Maintenance of long-term efficacy with continuous baricitinib treatment in patients with severe alopecia areata: 3-year results from BRAVE-AA1 and BRAVE-AA2 J Am Acad Dermatol, 2026.PMID 41314424
- [23]Sinclair R, Mesinkovska N, Mitra D et al. Patient-Reported Hair Loss and Its Impacts as Measured by the Alopecia Areata Patient Priority Outcomes Instrument in Patients Treated with Ritlecitinib: The ALLEGRO Phase 2b/3 Randomized Clinical Trial Am J Clin Dermatol, 2025.PMID 39441519
- [24]Barton VR, Toussi A, Awasthi S et al. Treatment of pediatric alopecia areata: A systematic review J Am Acad Dermatol, 2022.PMID 33940103
- [25]Lauron S, Plasse C, Vaysset M et al. Prevalence and Odds of Depressive and Anxiety Disorders and Symptoms in Children and Adults With Alopecia Areata: A Systematic Review and Meta-analysis JAMA Dermatol, 2023.PMID 36696123