Dermatology · Medicine
ANCA-associated vasculitis
Also known as ANCA-associated vasculitis · AAV · GPA · MPA · EGPA · Wegener's · Churg-Strauss
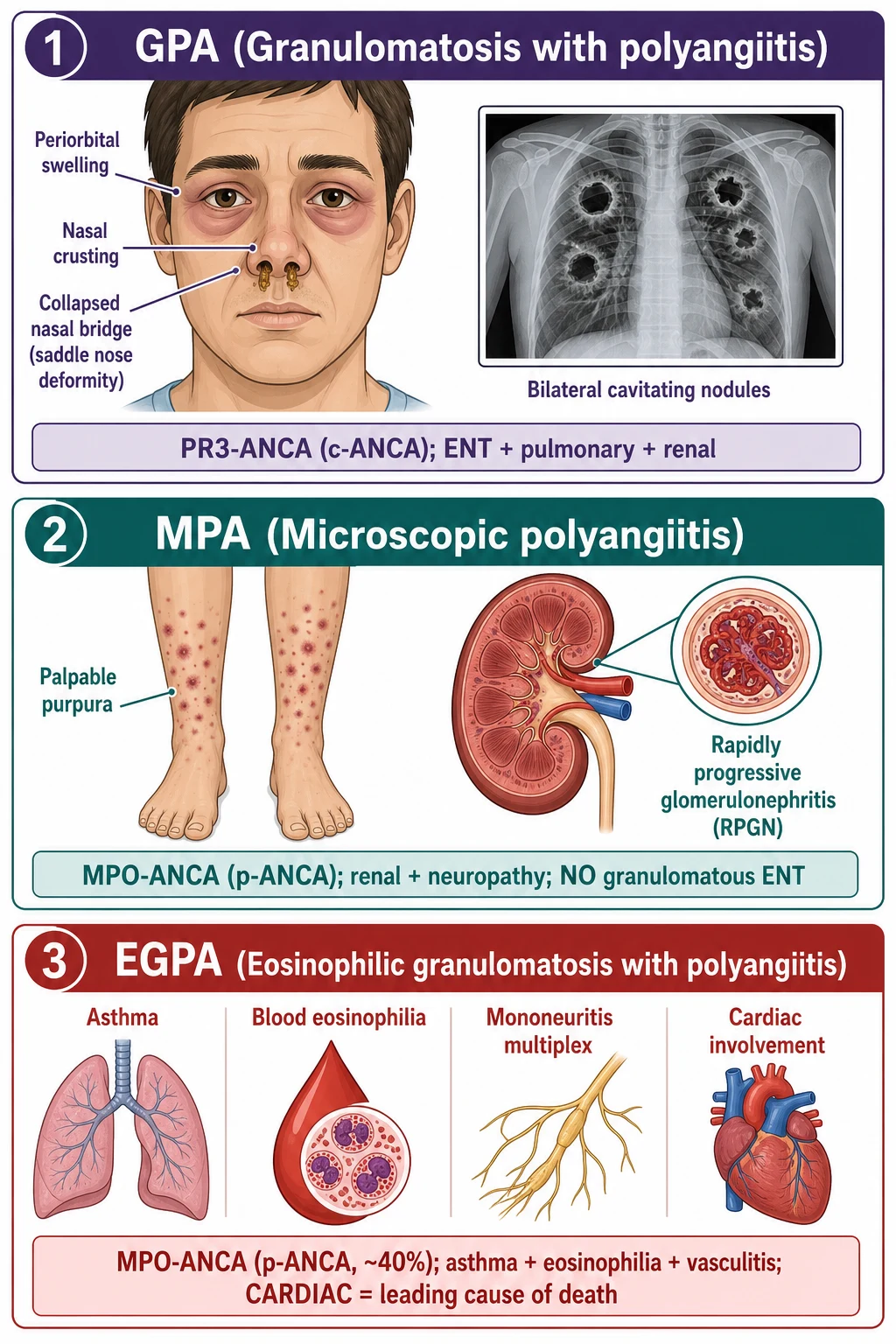
ANCA-associated vasculitis (AAV) comprises three necrotising small-to-medium vessel vasculitides: GPA (granulomatosis with polyangiitis — PR3/c-ANCA; ENT + pulmonary + renal), MPA (microscopic polyangiitis — MPO/p-ANCA; renal + pulmonary + neuropathy, no granulomatous ENT), and EGPA (eosinophilic granulomatosis with polyangiitis — MPO/p-ANCA in ~40%; asthma + eosinophilia + neuropathy + cardiac = leading cause of death). The hallmark renal lesion is pauci-immune crescentic glomerulonephritis (minimal immunoglobulin/complement deposition on IF — distinguishes from immune-complex GN). Cutaneous features include palpable purpura, nodules, ulcers and digital ischaemia. Management is divided into induction (rituximab or cyclophosphamide + high-dose corticosteroids — RAVE trial proved equivalence) and maintenance (rituximab or azathioprine/MMF + low-dose steroids), with plasma exchange for severe renal failure or pulmonary haemorrhage, and mepolizumab (anti-IL-5) for EGPA. Fellowship-level assessment demands mastery of the PR3/c-ANCA/GPA vs MPO/p-ANCA/MPA+EGPA correlation, the pauci-immune GN concept, the EGPA cardiac risk, the RAVE trial evidence, and the induction/maintenance ladder.
On this page & tools
Your progress
Saved locally on this device.
Exam tags
Red flags
Overview & Definition
ANCA-associated vasculitis (AAV) is an umbrella term for three necrotising, pauci-immune (little or no immunoglobulin or complement deposition on direct immunofluorescence) vasculitides of predominantly small and medium vessels, unified by the presence of circulating anti-neutrophil cytoplasmic antibodies (ANCA) directed against proteinase-3 (PR3) or myeloperoxidase (MPO).[1][2] AAV sits within the small-vessel vasculitis category of the 2012 Revised International Chapel Hill Consensus Conference (CHCC) nomenclature, alongside anti-GBM disease and immune-complex small-vessel vasculitis (IgA vasculitis, cryoglobulinaemic vasculitis, hypocomplementaemic urticarial vasculitis). The 2022 ACR/EULAR classification criteria further refine the diagnostic thresholds for each subtype using weighted clinical, serological, imaging and biopsy variables.
The three CHCC-recognised subtypes have overlapping but distinguishable phenotypes that an examiner expects the candidate to draw on the spot: granulomatosis with polyangiitis (GPA, formerly Wegener's) — PR3-ANCA / c-ANCA in 75-90% with the classic ENT, pulmonary and renal granulomatous triad; microscopic polyangiitis (MPA) — MPO-ANCA / p-ANCA in 40-80% with renal-predominant necrotising small-vessel vasculitis, pulmonary capillaritis and neuropathy but NO granulomatous inflammation; and eosinophilic granulomatosis with polyangiitis (EGPA, formerly Churg-Strauss) — MPO-ANCA in approximately 40%, characterised by adult-onset asthma followed by eosinophilia then small-vessel necrotising vasculitis in which cardiomyopathy is the leading cause of death.[1][3][4]
A fourth phenotype, renal-limited vasculitis (RLV), describes pauci-immune crescentic GN with ANCA positivity but no extrarenal disease, treated as an MPA-equivalent. Drug-induced AAV (propylthiouracil, hydralazine, levamisole-adulterated cocaine, anti-TNF agents) and anti-GBM / ANCA double-positivity are recognised scenario variants. The conceptual shift since 2020 is from immunofluorescence-pattern classification (c-ANCA / p-ANCA) toward antigen-based classification (PR3-AAV / MPO-AAV), because the antigen specificity predicts relapse rate, organ involvement, and response to therapy better than the older pattern labels do. [1]
The three CHCC-recognised AAV subtypes at a glance
GPA
Granulomatosis with polyangiitis (Wegener's)
- **PR3-ANCA / c-ANCA** in 75 to 90 percent of patients
- **Granulomatous** inflammation — ENT, lung, orbit
- Classic triad: **upper airway + lower airway + renal**
- Saddle-nose deformity, subglottic stenosis, cavitating nodules
- Relapsing course — rituximab preferred for both induction and maintenance
MPA
Microscopic polyangiitis
- **MPO-ANCA / p-ANCA** in 40 to 80 percent
- **NO granulomatous** inflammation anywhere
- Renal-predominant (RPGN), pulmonary capillaritis, mononeuritis multiplex
- Palpable purpura and constitutional features common
- Less relapsing than GPA — outcomes driven by renal biopsy chronicity
EGPA
Eosinophilic granulomatosis with polyangiitis (Churg-Strauss)
- **MPO-ANCA in ~40 percent** (more ANCA-positive in vasculitic phenotype; ANCA-negative more eosinophilic / cardiac)
- Three phases: **allergic (asthma) -> eosinophilic -> vasculitic**
- **Cardiomyopathy = leading cause of death**
- Mononeuritis multiplex (foot drop, wrist drop) very common
- Mepolizumab (anti-IL-5) for eosinophilic phenotype
Classification
The 2012 Revised International Chapel Hill Consensus Conference (CHCC) on vasculitis nomenclature is the current taxonomic anchor for AAV.[1][2] It places GPA, MPA and EGPA within small-vessel vasculitis, defined as vasculitis "with vessel calibre predominantly affecting small vessels (i.e., capillaries, venules, arterioles, and small arteries), although medium and large arteries may also be affected." An important CHCC phrase is "pauci-immune necrotising vasculitis" — meaning little or no immune-complex deposition on immunofluorescence, in contrast to immune-complex small-vessel vasculitides (IgA vasculitis, cryoglobulinaemic, anti-GBM). The 2022 ACR/EULAR classification criteria (Ann Rheum Dis 2022) provide weighted point-based criteria for each subtype, intended for use after a clinical diagnosis of small- or medium-vessel vasculitis has been made; they classify, they do not diagnose. EGPA classification draws on the 2022 ACR/EULAR criteria, which built on the 1990 ACR criteria (Lanham 1984 features — obstructive airway disease, nasal polyps, eosinophilia >10 percent, mono- or polyneuropathy, pulmonary infiltrates, sinus abnormality, extravascular eosinophils on biopsy).
The clinical phenotypes can also be stratified by ANCA antigen rather than by CHCC subtype. PR3-AAV is associated with granulomatous ENT disease, pulmonary nodules and a high relapse rate; MPO-AAV is associated with renal-predominant and pulmonary capillaritis disease, with a lower relapse rate and a higher chronic damage burden on renal biopsy. This antigen-first stratification is now used in registry analyses, biological sub-studies, and an increasing number of trial inclusion criteria. [1]
A purely clinical classification is also useful at the bedside: [1]
- Limited disease — ENT-only GPA, or RLV; no immediate organ threat.
- Early systemic disease — multi-organ but no critical organ (kidney, lung, brain, heart, gut) involved.
- Generalised disease — renal or other critical organ involvement.
- Refractory / relapsing disease — failure to remit, or relapse after remission.
- Severe disease — rapidly progressive GN (rising creatinine, red cell casts), pulmonary haemorrhage, CNS or cardiac involvement. [1]
Distinguishing severe from non-severe is the gate that decides whether the patient is admitted for IV induction or treated with oral methotrexate, mycophenolate or rituximab as an outpatient. [1]
Epidemiology & Risk Factors
AAV is rare but not vanishingly so. Population-based European registry data (UK, Norway, Sweden, Germany) report incidences of 10 to 20 per million per year and prevalence of 100 to 200 per million. The pattern is bimodal by age: a smaller younger-onset peak (often EGPA in women) and a larger older-adult peak (mostly GPA and MPA in the 65-75 bracket). The sex ratio is near 1:1 in older GPA and MPA, with a slight male excess; EGPA has a slight female excess in younger-onset disease. [1]
There is a striking geographic and ethnic gradient. Northern Europe favours PR3-AAV and GPA. Southern Europe and East Asia (Japan, China) favour MPO-AAV and MPA. African-American populations show a higher proportion of MPO-AAV and MPA, with renal-predominant disease and worse renal outcomes on average. [1]
The genetic architecture is complex. GWAS hits include HLA-DP (PR3/GPA), HLA-DQ (MPO/MPA), and the autoantigen genes themselves — PRTN3 (encoding PR3) and MPO. SERPINA1 (alpha-1-antitrypsin) deficiency predisposes to PR3-AAV, particularly with emphysema — a clinical clue worth knowing. The classical "dual hit" model invokes genetic susceptibility plus an environmental trigger. [1]
Established environmental and drug risk factors include silica exposure (mining, sandblasting, farming) — dose-dependent risk for AAV, particularly MPO; occupational solvents (painters, dry-cleaners); drugs — propylthiouracil (PTU), hydralazine, minocycline, levamisole-adulterated cocaine, anti-TNF agents (etanercept, infliximab, adalimumab), allopurinol, sulfonamides, penicillamine; chronic Staphylococcus aureus nasal carriage — independent risk for relapse in GPA; and smoking — accelerates and worsens GPA.[4]
Levamisole-adulterated cocaine deserves a specific mention because it is a contemporary epidemiological entity. Cocaine users who develop sudden AAV often have very high-titre p-ANCA and PR3-ANCA, characteristic ear-pinna necrosis, retiform purpura on the trunk and limbs, neutropenia, and a strongly positive ANA with anti-histone antibodies. The biopsy shows a leukocytoclastic vasculitis with thrombosis. Stopping the cocaine is the cornerstone of management. [1]
Pathophysiology
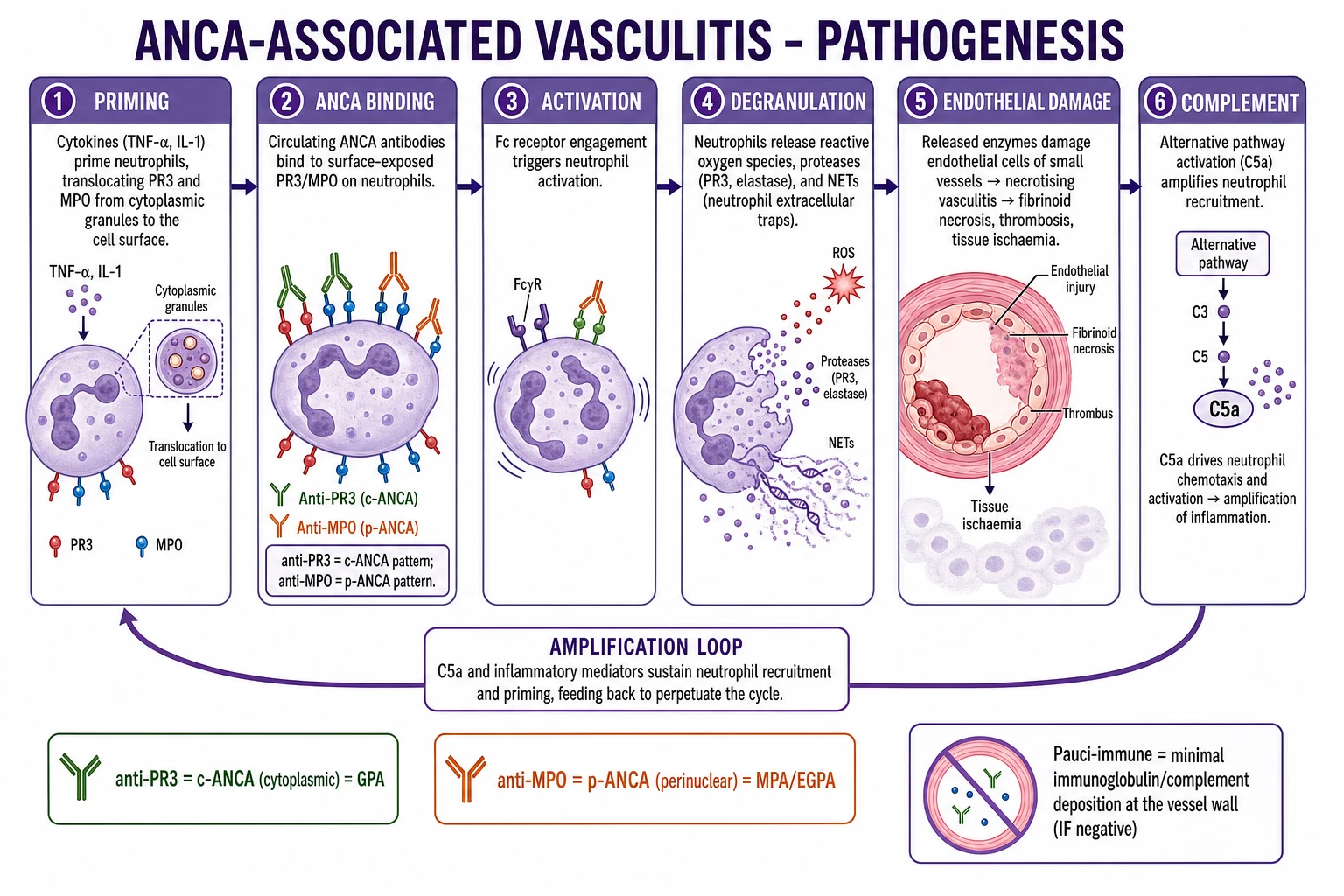
The central mechanistic model treats AAV as an ANCA-driven neutrophil-mediated endothelial injury with amplificatory loops (NETosis, alternative complement) but without significant immune-complex deposition.[2]
Step 1 — Priming of neutrophils. Pro-inflammatory cytokines (TNF-α, IL-1β, IL-6, IL-18, C5a) translocate the autoantigens PR3 (a serine protease of azurophilic granules) and MPO (a peroxidase of primary granules) from the cytoplasm to the plasma membrane of the neutrophil, where they become accessible to circulating IgG ANCA. Priming also induces the surface expression of adhesion molecules (β2 integrins) that mediate firm adhesion to endothelial cells. [1]
Step 2 — ANCA binding and neutrophil activation. IgG ANCA binds the membrane-bound antigen via its Fab' portion, while the Fc portion engages FcγRIIa and FcγRIIIb receptors, cross-linking and activating the neutrophil. Activated neutrophils undergo degranulation (releasing PR3, MPO, elastase, cathepsin G, lactoferrin), produce reactive oxygen species (ROS) through NADPH oxidase assembly, and release neutrophil extracellular traps (NETs) in a process called NETosis — extruded web-like chromatin decorated with PR3, MPO and citrullinated histones. [1]
Step 3 — Endothelial injury. Adherent neutrophils transmigrate across the endothelium and damage it through proteases (elastase, PR3) and ROS, exposing the subendothelial matrix, triggering microvascular thrombosis and producing the histological picture of fibrinoid necrosis of the vessel wall. [1]
Step 4 — NETs and autoantigen perpetuation. NETs contain PR3 and MPO in a configuration that is highly immunogenic — they bind anti-PR3 and anti-MPO B cells, drive ANCA class-switching (IgG1, IgG3, IgG4) via TLR9 and plasmacytoid dendritic-cell sensing of hypomethylated DNA, and deposit in glomeruli where they perpetuate injury. Elevated circulating NET markers (cell-free DNA, MPO-DNA complexes, citrullinated histone H3) are measurable in active AAV and are being studied as biomarkers. [1]
Step 5 — Alternative complement pathway amplification. ANCA-activated neutrophils release properdin and C5a, the most potent neutrophil chemoattractant, via the alternative complement pathway (with little classical-pathway immunoglobulin deposition — hence "pauci-immune" on IF). C5a primes more neutrophils, creating a feed-forward amplification loop in the vessel wall. This is the rationale for avacopan, an oral selective C5a receptor (C5aR1) antagonist that disrupts the loop and is now an option for steroid-sparing induction. [1]
Step 6 — T-cell help and granuloma formation. Autoreactive T-helper 17 (Th17) and T-follicular helper (Tfh) cells sustain B-cell ANCA production. In GPA, the antigen-specific CD4-positive T-cell response against PR3 drives granuloma formation — a Th1/Th17-driven organised lesion with epithelioid histiocytes, multinucleated giant cells and central necrosis, most evident in ENT and lung biopsies. In EGPA, a Th2-skewed response with IL-5 (eosinophil survival and activation), IL-4 and IL-13 drives the eosinophilic tissue infiltration and IgE elevation that characterise the prodromal and eosinophilic phases.[5][7]
Why is the biopsy "pauci-immune" despite complement involvement? The answer lies in the fact that the alternative pathway is amplifying inflammation at the tissue level without depositing large immune complexes — there is little immunoglobulin, and complement fragments act as anaphylatoxins (C3a, C5a) rather than as membrane attack complexes localised to glomerular basement membranes. Hence the seemingly paradoxical name. [1]
Distinguish PR3-AAV from MPO-AAV mechanistically. PR3 is a serine protease that degrades many substrates (elastin, collagen, cytokines) and, when expressed on neutrophil membrane, also signals. MPO is a peroxidase that catalyses halogenation and ROS generation. PR3-AAV is associated with granulomatous inflammation, more ENT involvement and a higher relapse rate; MPO-AAV is associated with sclerosis and chronic damage on renal biopsy and a lower relapse rate. [1]
PAVIA — the five-step ANCA-driven mechanism
PAVIA
TNF-α, IL-1, C5a prime neutrophils; PR3 and MPO translocate to the surface.
IgG ANCA binds via Fab'; Fc engages FcγR on the primed neutrophil.
Degranulation, ROS burst, NETosis (extruded chromatin + PR3/MPO).
Proteases plus ROS damage endothelium -> fibrinoid necrosis plus thrombosis.
Properdin and C5a create a feed-forward loop — target of avacopan.
Classification Schema — A clinical vignette
Viva vignette — what is the most likely diagnosis?
A 62-year-old man presents with three months of nasal crusting, epistaxis and recurrent sinusitis, two months of arthralgia and weight loss, and one week of rising creatinine (now 320 µmol/L) with microscopic haematuria and 1.5 g of proteinuria on urine PCR. ANCA returns as a strong c-ANCA with anti-PR3 positivity on ELISA. Chest CT shows two cavitating nodules in the right lung. [1]
Most likely diagnosis: GPA (granulomatosis with polyangiitis, PR3-AAV). The ENT, pulmonary and renal triad combined with PR3-ANCA is pathognomonic. The next steps are: ENT evaluation for subglottic stenosis if stridor is present, formal ANCA renal risk scoring, urgent renal biopsy if the creatinine is rising, screen for hepatitis B/C, HIV and TB, and start induction with IV methylprednisolone pulses followed by oral prednisolone plus rituximab 375 mg/m² weekly for four weeks (or cyclophosphamide). Plasma exchange is reasonable if the creatinine exceeds 500 µmol/L or the patient develops DAH.
Clinical Presentation
AAV presents with a combination of constitutional, organ-specific, and cutaneous features, and the phenotype dictates both the ANCA expected and the urgency of induction.[1][3][4] A comprehensive review-of-systems is mandatory at first contact — the patient who describes "sinus trouble, cough, dark urine and tingling feet" is a textbook GPA; the asthmatic on montelukast who develops a foot drop with new eosinophilia is a textbook EGPA.
GPA — Granulomatosis with polyangiitis
The ENT + respiratory + renal classic triad is taught everywhere, but each patient with GPA demonstrates a mix of: [1]
- ENT (≈90%): refractory sinusitis, nasal crusting, epistaxis, recurrent otitis media with effusion, saddle-nose deformity from septal cartilage destruction, subglottic stenosis (stridor; wheeze out of proportion to vocal cord dysfunction can be missed for years), chronic sinusitis with or without polyps, oral or nasal ulceration, recurrent parotid enlargement, proptosis and orbital pseudotumour from retro-orbital granuloma, sensorineural or conductive hearing loss.
- Lower respiratory (≈70 to 80%): persistent cough, dyspnoea, pleuritic chest pain, multiple pulmonary nodules that characteristically cavititate (about 50% of nodules cavitate), infiltrates, pleural effusion, and diffuse alveolar haemorrhage (DAH) — a medical emergency when hypoxaemia falls and fresh blood fills the alveoli.
- Renal (≈70 to 80% during disease): rapidly progressive glomerulonephritis (RPGN) — rising creatinine, microscopic haematuria with dysmorphic red cells and red cell casts, sub-nephrotic proteinuria, hypertension, fluid overload.
- Skin (≈35 to 50%): palpable purpura of the lower limbs, painful subcutaneous nodules (granulomatous vasculitis), pyoderma-gangrenosum-like ulcers, livedo reticularis, digital infarcts.
- Eye: scleritis (painful red eye with photophobia), peripheral ulcerative keratitis (sight-threatening — urgent ophthalmology), orbital pseudotumour, episcleritis, optic neuropathy.
- Peripheral nerves: mononeuritis multiplex (foot drop, wrist drop, sensory loss in a nerve-territory pattern).
- Other: constitutional features (fever, weight loss, night sweats, myalgia, arthralgia); pericarditis, myocarditis (rare); mesenteric vasculitis (abdominal pain, gut ischaemia); prostatic and urethral involvement (rare, can mimic prostatitis). [1]
GPA is the prototypical relapsing AAV. ENT involvement at presentation, lower serum creatinine at presentation, and chronic nasal S. aureus carriage predict relapse. [1]
MPA — Microscopic polyangiitis
MPA is the renal-pulmonary-neuropathy AAV without granulomas. It is the commonest AAV subtype in East Asian populations and is over-represented in elderly females. [1]
- Renal (≈90%): pauci-immune crescentic GN; often presents as subacute RPGN with reduced urine output, dark or tea-coloured urine, hypertension and oedema. Outcomes correlate tightly with the proportion of normal glomeruli, percentage crescents, and percentage chronic tubulointerstitial fibrosis on biopsy — the so-called ANCA Renal Risk Score.
- Pulmonary (≈30 to 50%): pulmonary capillaritis with or without DAH; recurrent haemoptysis, falling haemoglobin, diffuse ground-glass infiltrates; can mimic pneumonia or pulmonary oedema.
- Skin (≈30 to 50%): palpable purpura on dependent areas, livedo, nodules, ulcers, digital infarcts.
- Peripheral nerves (≈30 to 60%): mononeuritis multiplex — sural, peroneal, ulnar, median; often painful.
- Other: constitutional; abdominal pain (mesenteric vasculitis is uncommon but serious); pericarditis (rare); eye (scleritis).
- MPA does NOT cause granulomatous ENT disease — the absence of sinusitis or nasal crusting at presentation is a high-yield clue distinguishing MPA from GPA. Limited MPA may present with renal or pulmonary disease alone. [1]
EGPA — Eosinophilic granulomatosis with polyangiitis
EGPA classically unfolds over years in three overlapping phases that an examiner can ask the candidate to distinguish.[5][6][7]
- Allergic and prodromal phase: adult-onset asthma (almost universal; often begins 5-10 years before vasculitis), allergic rhinitis, nasal polyposis, recurrent sinusitis. Omalizumab initiation in this population has been associated with unmasking of EGPA — a classically tested pearl.
- Eosinophilic phase: peripheral eosinophilia greater than 1.5 × 10⁹/L or greater than 10 percent of leucocytes, tissue eosinophilic infiltration, transient pulmonary infiltrates (Loeffler-like), eosinophilic gastroenteritis.
- Vasculitic phase: small-vessel necrotising vasculitis; mononeuritis multiplex (most common extrathoracic manifestation — typically presents with foot drop or wrist drop); cardiomyopathy (eosinophilic myocarditis, pericarditis, heart failure — the leading cause of death); mesenteric vasculitis (abdominal pain, gut perforation); glomerulonephritis (less common than in MPA and GPA); skin (palpable purpura, nodules, livedo). [1]
The ANCA status partitions EGPA clinically: [1]
- ANCA-positive (MPO-ANCA in most) — predominantly vasculitic phenotype: neuropathy, GN, purpura, constitutional features.
- ANCA-negative — predominantly eosinophilic and cardiac phenotype: cardiomyopathy, asthma, sinusitis, eosinophilia over 30 percent. [1]
This phenotypic split is now considered a provisional classification by international consortia because it tracks prognosis and treatment response differently (mepolizumab works better in the ANCA-negative group; cyclophosphamide works better in the vasculitic group). [1]
Constitutional and cutaneous features (across all three)
- Fever, weight loss, night sweats, myalgia, arthralgia in nearly every patient at presentation.
- Skin: palpable purpura (leukocytoclastic vasculitis on biopsy) is the most common cutaneous lesion — distributed over dependent areas (lower legs, ankles), often in crops over weeks; subcutaneous nodules, digital infarcts and gangrene, ulcers with undermined violaceous borders, livedo reticularis with or without necrosis.
- Mucosal: oral ulceration and gingival hyperplasia ("strawberry gingivitis" is pathognomonic of GPA when present); nasal, laryngeal, laryngeal chondritis.
- Eyes: scleritis (deep, painful red eye), peripheral ulcerative keratitis (melt; sight-threatening; ophthalmology referral within 24 hours), orbital pseudotumour.
- Heart: pericarditis, myocarditis (especially EGPA), valvulitis (rare), accelerated atherosclerosis from chronic inflammation.
- Venous thromboembolism is increased two- to three-fold during active disease and the first six months of immunosuppression. [1]
Atypical and elderly presentations
Older patients present with more renal-predominant and pulmonary haemorrhage disease and less granulomatous ENT disease. They tolerate cyclophosphamide and high-dose steroids poorly — prefer rituximab and reduced-dose glucocorticoids (PEXIVAS-supported). Atypical and limited presentations include ENT-only GPA (often seronegative), isolated renal vasculitis, single-organ involvement and late-onset disease after age 80. [1]
Drug-induced AAV
Propylthiouracil (PTU, antithyroid drug), hydralazine (antihypertensive), levamisole-adulterated cocaine (illicit stimulant cut with levamisole to potentiate effect), minocycline, allopurinol, sulfonamides, penicillamine, anti-TNF agents: stop the offending drug; high-titre MPO-ANCA with or without PR3-ANCA, characteristic ear-pinna necrosis and retiform purpura, and ANA with anti-histone antibodies are typical. Renal-limited disease is common. [1]
Clinical & Bedside Assessment
A structured bedside examination supports the diagnosis, gauges severity, and identifies the biopsy site. [1]
Bedside examination checklist for any suspected AAV: [1]
- Vital signs: blood pressure (acceleration of hypertension suggests renal involvement), temperature, oxygen saturation. A falling SpO2 with rising respiratory rate and visible bloodstained sputum = DAH until proven otherwise.
- Skin: full body inspection, paying attention to dependent areas — palpable purpura, nodules, ulcers, livedo, digital ischaemia, ear-pinna necrosis (levamisole and cocaine). Photograph each lesion for serial comparison.
- ENT (and the often-neglected oral cavity): anterior rhinoscopy and nasal endoscopy (granular mucosa, crusting, septal perforation, saddle deformity), otoscopy (effusion), inspection for saddle nose and proptosis, oral cavity for strawberry gingivitis and ulcers, indirect laryngoscopy or fibreoptic nasendoscopy for subglottic stenosis in hoarse or stridulous patients.
- Respiratory: auscultate for crackles (DAH) and wheeze (subglottic stenosis, EGPA asthma).
- Cardiovascular: BP all four limbs if large-vessel involvement is in doubt; pericardial rub; careful volume assessment in renal disease.
- Abdomen: tenderness, organomegaly, mesenteric ischaemia, hepatosplenomegaly (drug-induced).
- Neurological: detailed examination of named peripheral nerves — foot drop (common peroneal), wrist drop (radial), foot sensory loss (sural), hand sensory loss (ulnar) — and document a sensorimotor map at each visit.
- Joints: non-erosive oligoarthritis is common. [1]
Disease activity instruments
- Birmingham Vasculitis Activity Score (BVAS) — nine-domain clinician-rated activity score (general, cutaneous, mucous membranes and ENT, chest, cardiovascular, abdominal, renal, nervous system, other). New or worsening features score higher. Used to define remission (BVAS = 0) and flare (BVAS greater than threshold) in trials. Drives induction intensity.
- Five Factor Score (FFS, 2009 revision — Guillevin) — prognostic, NOT activity. One point each for: age over 65 years, cardiac involvement, renal involvement (creatinine over 150 µmol/L or 1.7 mg/dL), gastrointestinal involvement, absence of ENT involvement. Score 0 vs 1 vs 2+ stratifies 5-year mortality roughly 12%, 26%, 46%.
- Vasculitis Damage Index (VDI) — cumulative irreversible damage (64-item checklist) — separates active inflammation from prior tissue loss.
- ANCA Renal Risk Score (ARRS) — biopsy-based prognostic score: percentage normal glomeruli, percentage crescents, percentage interstitial fibrosis and tubular atrophy. Predicts ESKD at 3 years. [1]
Standardised severity stratification
- Limited and non-severe: no critical organ involvement; outpatient management reasonable.
- Severe (organ-threatening): rapidly rising creatinine, DAH, CNS vasculitis, mononeuritis multiplex, mesenteric ischaemia, cardiac involvement — IV induction. [1]
Investigations
A diagnosis of AAV rests on a triad of serology (ANCA), histology (biopsy), and organ involvement — no single test is definitive. [1]
Serology — ANCA testing strategy
The standard approach is a two-step strategy: initial immunofluorescence (IIF) on ethanol-fixed neutrophils to identify the pattern (c-ANCA, p-ANCA, atypical), then a confirmatory antigen-specific ELISA for PR3 and MPO. The combination is the gold standard. Samples are venous blood; no fasting or special preparation is required. Repeat testing during follow-up is NOT driven by ANCA titre alone — clinical assessment and BVAS is the standard. [1]
IIF pattern | Target antigen | Typical phenotype c-ANCA (cytoplasmic, granular) | PR3 (70-80%); atypical MPO less commonly | GPA; MPO-ANCA MPA p-ANCA (perinuclear) | MPO (60-80%); PR3 uncommonly | MPA, EGPA, drug-induced a-ANCA and x-ANCA (atypical) | varies; often non-specific | UC, primary sclerosing cholangitis, infections Negative | — | Limited, burnt-out, treated disease; consider EGPA [1]
A negative ANCA does NOT exclude AAV if the clinical phenotype is typical — biopsy is the next move. Drug-induced AAV may be ANCA-positive, ANA-positive with anti-histone antibodies, with cytopenias. [1]
Routine laboratory and bedside
- FBC: anaemia of chronic disease, thrombocytosis, eosinophilia (EGPA, drug-induced), cytopenias from drug-induced marrow disease.
- ESR / CRP: usually elevated; CRP better than ESR for tracking activity.
- U&E: serum creatinine is the single most important trackable marker; trend it daily during induction.
- LFTs and albumin: low albumin in severe disease and nephrotic-range proteinuria.
- Urinalysis and microscopy: blood and protein on dipstick; dysmorphic red cells and red cell casts on phase-contrast microscopy — the renal-bedside diagnosis.
- Urine protein-to-creatinine ratio (uPCR) at presentation and serially.
- Blood cultures to exclude infective endocarditis before immunosuppression.
- HIV, hepatitis B, hepatitis C serology before rituximab or cyclophosphamide.
- QuantiFERON-TB Gold before immunosuppression.
- Troponin plus BNP if EGPA, or any cardiac symptoms.
- IgE and eosinophil count (EGPA; often elevated in EGPA and hyper-eosinophilic syndrome).
- Serum IgG4 if IgG4-related disease is in the differential (especially ENT-predominant disease). [1]
Tissue biopsy
Biopsy site, yield, and what it shows
Renal biopsy
Gold standard for renal AAV
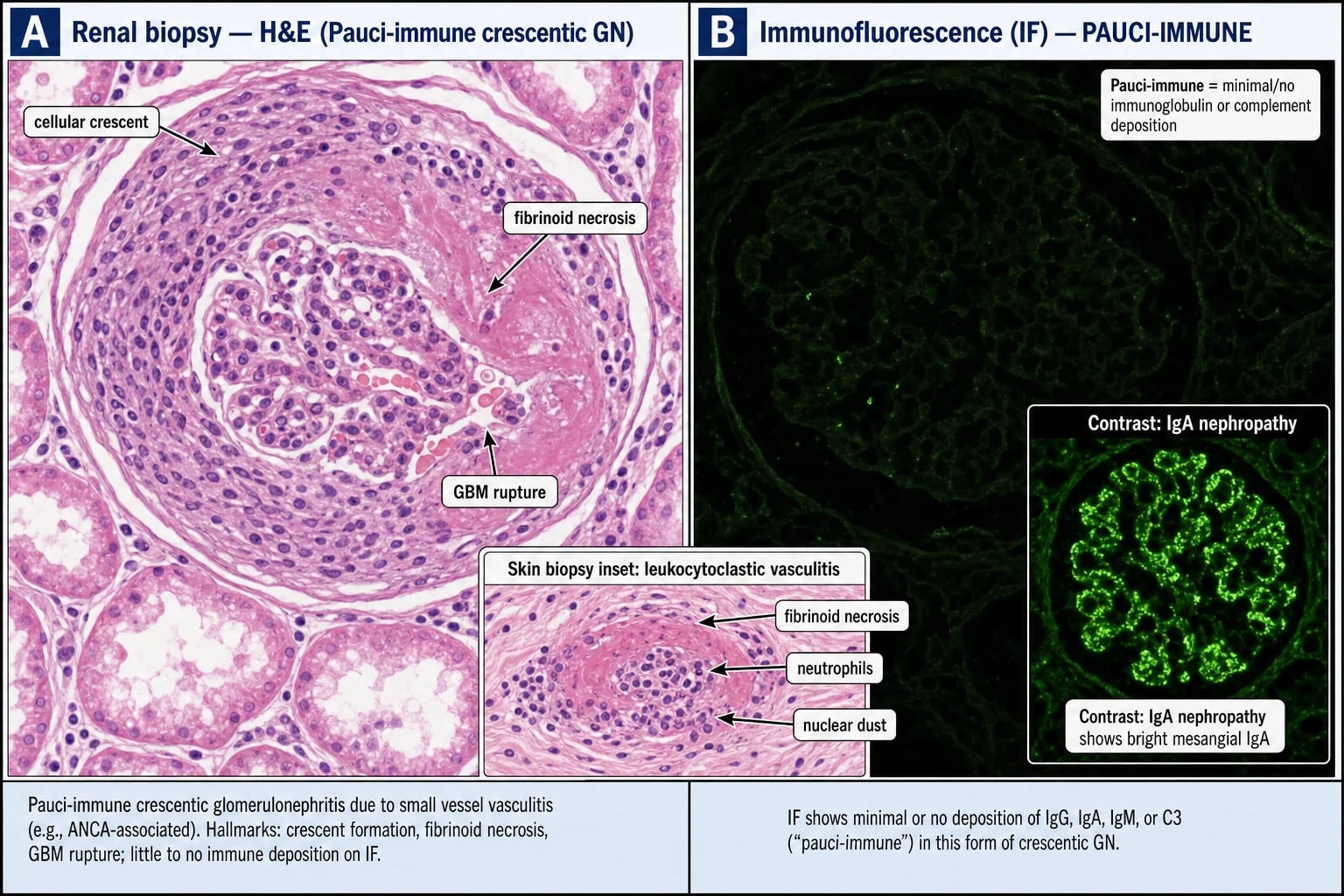
- **Pauci-immune necrotising crescentic GN**
- Focal and segmental fibrinoid necrosis of glomerular tuft
- **Cellular crescents** (epithelial cell proliferation + fibrin) — early
- Disrupted GBM; periglomerular inflammation
- IF: little / no IgG, IgM, IgA, C3, C1q
- EM: no dense deposits
- Chronic features: fibrous crescents, glomerulosclerosis, IFTA — drive prognosis
Skin biopsy
Affected purpuric lesion, including subcutis
- **Leukocytoclastic vasculitis** of dermal venules
- Neutrophilic infiltrate, fibrinoid necrosis, karyorrhectic debris
- **No immune deposits** on DIF (pauci-immune)
- Subcutaneous nodule may show **panniculitis with granulomas**
- Sural nerve biopsy may also show vasculitis if mononeuritis multiplex is present
Lung biopsy
Transbronchial / thoracoscopic if nodules present
- **Necrotising granulomas** with geographic necrosis in GPA
- Eosinophil-rich necrotising granulomas in EGPA
- Pulmonary capillaritis with alveolar haemorrhage in MPA
- Often too risky to biopsy — rely on HRCT and serology
Nasal / sinus biopsy
Reserved for atypical cases
- Often non-specific: chronic inflammation, fibrosis, granulomas in ~50%
- Useful to exclude lymphoma, sarcoidosis, IgG4-related disease, midline destructive lesion
- Granulomatous inflammation plus vasculitis is suggestive but not diagnostic
Imaging
- Chest X-ray then high-resolution CT chest (HRCT) — pulmonary nodules (often cavitating, 50% cavitation in GPA), infiltrates, ground-glass (DAH), waxing-and-waning opacities, pleural effusion, pericardial effusion.
- CT sinuses and orbits — sinus opacification, bony erosion, septal perforation, orbital pseudotumour.
- CT PET/CT — used in some centres for occult disease, but not routine.
- Angiography — usually NORMAL in AAV because vessels are too small; reserved for medium-vessel vasculitides (PAN) where microaneurysms are visible.
- Echocardiogram for EGPA — cardiac MRI with late gadolinium enhancement is more sensitive than echo for subclinical myocarditis.
- Bronchoscopy with bronchoalveolar lavage in suspected DAH — serial aliquots show progressively bloodier return; microbiology negative; haemosiderin-laden macrophages on cytology. [1]
Excluding mimics
Must-do exclusions before immunosuppression
Differential Diagnosis [1]
The differential of AAV is wide, and any exam answer should triage pauci-immune necrotising vasculitis plus ANCA before going to alternatives. The two most commonly tested mimics are outlined below. [1]
AAV vs PAN, IgA vasculitis, anti-GBM, cryoglobulinaemia, drug-induced
AAV
Pauci-immune necrotising vasculitis + ANCA
- Small-to-medium vessels; **pauci-immune** on IF
- Renal: **pauci-immune crescentic GN**
- Three subtypes: GPA, MPA, EGPA
- ANCA positive in 80 to 95%; ANCA-negative possible
PAN (polyarteritis nodosa)
Medium-vessel; ANCA-negative
- **No glomerulonephritis** — renal arteries affected, not glomeruli
- **No pulmonary involvement** (lungs spared)
- Hepatitis B associated in about 30 percent
- Microaneurysms on mesenteric and renal angiography
- Mononeuritis multiplex, abdominal pain, testicular pain
IgA vasculitis (HSP)
Childhood small-vessel
- Children and young adults; post-URI
- **Palpable purpura**, abdominal pain, arthritis, IgA nephritis
- IF: **IgA in mesangium** — immune-complex, NOT pauci-immune
- Usually self-limiting; renal involvement drives long-term outcome
Anti-GBM disease (Goodpasture)
Anti-GBM + pulmonary-renal
- Anti-GBM antibody; linear IgG on GBM
- Pulmonary haemorrhage + RPGN
- **Can coexist with ANCA** (double-positive — 5 to 10 percent of anti-GBM)
- Urgent plasma exchange + immunosuppression
Cryoglobulinaemic vasculitis
Immune-complex
- Type II and III mixed cryoglobulins; **low C4**
- **Hepatitis C** association
- Purpura, arthralgia, neuropathy, weakness
- IF: **IgM + IgG + C3 in vessel wall**
Drug-induced AAV
PTU, hydralazine, levamisole-cocaine, anti-TNF
- High-titre MPO with or without PR3, often anti-histone and ANA, cytopenias
- Renal-limited disease common
- Remits on drug cessation (with immunosuppression if organ-threatening)
- Levamisole-cocaine: ear and retiform purpura
Other differentials worth mentioning at the viva: [1]
- SLE / DLE / lupus nephritis — ANA positive, anti-dsDNA positive, low complement — and DAH from lupus pneumonitis.
- Sarcoidosis — ENT plus lung involvement, but bilateral hilar lymphadenopathy, hypercalcaemia, non-caseating granulomas; ANCA negative.
- IgG4-related disease — orbital pseudotumour, pancreatitis, retroperitoneal fibrosis; serum IgG4 elevated; ANCA negative.
- Midline destructive lesion and cocaine midline destruction — nasal septum perforation, ANCA sometimes positive (especially if levamisole); biopsy distinguishes.
- Infective endocarditis — positive blood cultures, valvular vegetations on echo, immune-complex phenomena (purpura, Osler nodes, Roth spots).
- Tuberculosis, atypical mycobacteria, fungal, nocardia — granulomatous inflammation; cultures and stains. [1]
Management — Resuscitation
AAV becomes a medical emergency when renal function is deteriorating rapidly, when alveolar haemorrhage is producing hypoxaemia, when mononeuritis multiplex is acutely disabling, when mesenteric ischaemia is producing pain or peritonitis, or when cardiac involvement is producing heart failure or arrhythmia.[1][3]
Immediate resuscitation bundle: [1]
- ABCs: high-flow oxygen; secure airway in subglottic stenosis; intubation by an experienced operator (the subglottic airway is fragile); avoid nasal intubation in GPA with severe nasal destruction.
- Cautious fluid resuscitation if hypotensive — but avoid volume overload in RPGN.
- Two large-bore IV cannulae; cross-match four units of packed red cells if DAH or active bleeding.
- IV methylprednisolone pulse 500 mg to 1 g daily for three days as the immediate induction backbone for organ-threatening or life-threatening disease, followed by oral prednisolone 1 mg/kg/day (maximum 60 to 80 mg). For less severe disease, start with oral prednisolone directly.
- Cautious but rapid blood-pressure control if hypertensive and renal; avoid ACE-inhibitors acutely if creatinine is rising or AKI is established — they may worsen renal function.
- Infection screen: blood cultures, urine culture, hepatitis B and C, HIV, QuantiFERON, CXR; this is critical because the next step is profound immunosuppression.
- Renal biopsy within 24 to 72 hours if feasible — proceeds or informs induction; do not delay induction to obtain the biopsy.
- Plasma exchange (PLEX) in selected severe cases — see below.
- Multi-specialty involvement at presentation: rheumatology, nephrology, respiratory, ENT, ophthalmology, pharmacy (for biologics and PLEX scheduling).
- Vaccinations before starting: influenza (any season), pneumococcal (PCV13 plus PPSV23), COVID-19 boosters; check hepatitis B surface antibody and vaccinate if non-immune. Avoid live vaccines (MMR, varicella, yellow fever, BCG) during and for months after immunosuppression. [1]
Management — Definitive & Stepwise
Definitive treatment is divided into two phases — induction (three to six months, high-intensity) and maintenance (24 to 48+ months, lower-intensity). The pivotal modern trials are RAVE (Stone NEJM 2010), RITUXVAS (Jones 2010), CYCLOPS (de Groot 2009), MAINRITSAN (Guillevin 2014), IMPROVE (Hiemstra 2010), MEPEX (Jayne 2007), PEXIVAS (Walsh 2020), MIRRA (Wechsler 2017) and ADVOCATE (Jayne 2021). [1]
Induction for severe and organ-threatening AAV
-
Rituximab — anti-CD20 monoclonal antibody; depletes CD20-positive B cells, including those producing ANCA. RAVE (Stone NEJM 2010) randomised 197 patients with severe AAV to rituximab 375 mg/m² weekly for four doses plus prednisone versus oral cyclophosphamide 2 mg/kg/day plus prednisone. Rituximab was non-inferior for complete remission off steroids at six months, and superior in relapsing disease at 12 and 18 months. RITUXVAS (Jones 2010) added an extra rituximab-only arm for patients with renal involvement, with comparable renal outcomes and similar infection rates. Rituximab is now first-line in relapsing AAV (after a prior cyclophosphamide remission), in PR3-AAV (higher relapse — rituximab maintenance is particularly effective), in women of childbearing potential (avoids cyclophosphamide gonadal toxicity), in those with previous cyclophosphamide exposure (to limit cumulative dose and bladder-cancer risk), and in EGPA in the ANCA-positive vasculitic phenotype.[1][3]
Dosing: 375 mg/m² weekly for four weeks (RAVE protocol; lymphoma style) OR 1 g on day 1 and 1 g on day 15 (rheumatology protocol). Premedicate with paracetamol, an antihistamine, and IV methylprednisolone 100 mg. Caution: HBV reactivation — screen and prophylax HBsAg-positive or anti-HBc-positive patients with entecavir or tenofovir; PML risk (very low, but check for new neurology); hypogammaglobulinaemia with repeated dosing; late-onset neutropenia two to three months after infusion; infusion reactions; progressive multifocal leukoencephalopathy (rare). [1]
-
Cyclophosphamide — prodrug metabolised to active alkylating species; cross-links DNA and depletes rapidly dividing cells including ANCA-producing plasmablasts. CYCLOPS (de Groot Ann Intern Med 2009) randomised 149 patients to IV pulse 15 mg/kg every two to three weeks versus daily oral 2 mg/kg/day. Pulse IV was non-inferior for remission and produced a lower cumulative dose but a slightly higher relapse rate in long-term follow-up. Caution: bladder toxicity (haemorrhagic cystitis, urothelial carcinoma) is cumulative-dose dependent; monitor urine; give MESNA with each IV bolus and encourage hydration; fertility (bank sperm and eggs before); cytopenias; secondary malignancy (bladder, lymphoma); SIADH. Reduce dose in renal impairment (CrCl below 30 mL/min) by about 25% and in age over 70 by about 25 to 50%. [1]
-
Glucocorticoids are the third pillar of induction. The PEXIVAS reduced-dose glucocorticoid regimen is now standard — start with pulse methylprednisolone 500 to 1000 mg for three doses, then oral prednisolone around 1 mg/kg (maximum 60 to 80 mg), and taper over months. Reduced-dose regimens were non-inferior for mortality and ESKD, with fewer infections (Walsh 2020). [1]
Plasma exchange (PLEX)
When to add plasma exchange to induction
Strong evidence
PEXIVAS and MEPEX support these settings
- **SCr over 500 µmol/L (~5.7 mg/dL)** — MEPEX showed plasma exchange increased dialysis-independence at three months vs IV methylprednisolone (69 vs 49 percent); long-term benefit attenuated
- **Anti-GBM overlap and double-positive** — daily PLEX until anti-GBM undetectable
- **Severe diffuse alveolar haemorrhage with hypoxaemia** — PEXIVAS supportive in this subgroup
Less strong and controversial
Consider case-by-case
- Rapidly progressive GN with SCr 300 to 500 µmol/L — discuss with nephrology
- Meningitis or mesenteric ischaemia from active vasculitis
- Refractory disease failing first-line induction
PLEX schedule: typically seven to 14 daily exchanges (one to 1.5 plasma volumes) using albumin or plasma replacement over two to four weeks, in parallel with induction. Central venous access (vascath) is required; bleeding and line sepsis are the principal complications. [1]
Avacopan — C5aR1 antagonist
ADVOCATE (Jayne NEJM 2021) randomised 331 patients with AAV to avacopan 30 mg orally twice daily versus prednisone taper on a background of rituximab or cyclophosphamide. Avacopan achieved higher sustained remission at 26 weeks and was steroid-sparing. It is particularly useful when avoiding high cumulative steroid dose (diabetes, osteoporosis, obesity, elderly, previous steroid intolerance). Caution: hepatotoxicity — monitor LFTs; avoid with strong CYP3A4 inhibitors; vaccination status; concomitant immunosuppression. [1]
EGPA-specific therapy
EGPA management by disease severity
Non-severe EGPA
Asthma, sinus polyps, eosinophilia, no organ-threatening vasculitis
- **Mepolizumab 300 mg SC every 4 weeks** (MIRRA, Wechsler 2017)
- Anti-IL-5 monoclonal antibody; reduces eosinophils, allows oral steroid taper
- Continue maintenance inhaled therapy for asthma
- Sinonasal polyps — intranasal steroids, dupilumab consideration
Severe and organ-threatening EGPA
Cardiac, GI, neuropathy, renal
- **Cyclophosphamide + high-dose corticosteroids** as per vasculitic induction
- Cardiac MRI and troponin at baseline and on follow-up
- ECG, telemetry for arrhythmia surveillance
- Continue mepolizumab post-induction in some protocols
Limited and non-severe AAV
- Methotrexate (up to 25 mg weekly plus folic acid) for limited GPA (no renal, no pulmonary, no CNS) — efficacy shown in the NORAM trial (de Groot 2005).
- Mycophenolate mofetil 2 g/day if methotrexate is contraindicated.
- Rituximab is increasingly used in this group to avoid the cumulative toxicity of low-dose cyclophosphamide.
- Cotrimoxazole (trimethoprim-sulfamethoxazole) 480 mg twice daily for three to six months in ENT-dominant GPA reduces relapse (Stegeman 1996) by reducing S. aureus nasal carriage — replicated in subsequent cohorts. Use cautiously with high-dose cyclophosphamide (cumulative marrow toxicity). [1]
Maintenance — after 3-6 months induction
- Rituximab is the preferred maintenance agent, particularly in PR3-AAV and relapsing disease. MAINRITSAN (Guillevin 2014) compared rituximab (fixed-schedule 500 mg x 2 at months 6 and 12 after induction) with azathioprine; rituximab had far fewer major relapses (5% vs 29%) at 28 months. MAINRITSAN 2 (Charles NEJM 2018) used a tailored-dose approach based on B-cell return and ANCA — also superior to azathioprine. The MAINRITSAN 3 extension confirmed sustained benefit.
- Azathioprine 2 mg/kg/day is the standard non-biologic maintenance — cheaper, oral, supported by IMPROVE for relapse-free survival, particularly in MPO-AAV. Test TPMT activity before starting (low activity leads to myelosuppression).
- Mycophenolate mofetil 2 g/day — IMPROVE showed azathioprine was superior; reserve as second-line maintenance.
- Methotrexate 20 to 25 mg weekly plus folic acid — limited disease only; avoid in renal impairment.
- Continue low-dose prednisolone 5 to 7.5 mg daily for at least 12 to 18 months.
- Total maintenance duration: at least 24 to 36 months, often longer in PR3-AAV. [1]
Supportive bundle
PROCTSS — every AAV patient gets this bundle
PROCTSS
Cotrimoxazole 480 mg daily OR 960 mg three times per week on cyclophosphamide, rituximab, or sustained high-dose steroids.
Volume, electrolyte, BP control; dialysis planning; nephrology early referral; renal transplant after disease quiescence.
Calcium 1 g + vitamin D 800 to 1000 IU daily; bisphosphonate if age over 50 or steroid for more than three months.
Lipids, BP, glucose, VTE prophylaxis during admissions; stop smoking.
Check TPMT activity to avoid myelosuppression.
Hepatitis B and C, HIV, TB; vaccine before live vaccines.
Sick-day rules, glucose monitoring, mood, sleep, weight, infection.
Specific Subtypes & Scenarios
The four AAV phenotypes and their clinical priority
GPA
Granulomatosis with polyangiitis
- **PR3-ANCA in 75 to 90 percent** — favour antigen-specific ELISA over IF
- **ENT + pulmonary + renal** is the classic triad
- Saddle nose, subglottic stenosis, orbital pseudotumour, cavitating nodules
- **Relapsing** — rituximab preferred for induction and maintenance
- Cotrimoxazole reduces relapse; ENT surgery rarely indicated acutely
MPA
Microscopic polyangiitis
- **MPO-ANCA in 40 to 80 percent**
- Renal-predominant (RPGN), pulmonary capillaritis, neuropathy; **no granulomas**
- Less relapsing than GPA; outcomes depend on renal biopsy chronicity
- Monitor renal function, urinalysis, and uPCR for relapse
EGPA
Eosinophilic granulomatosis with polyangiitis
- Three phases: asthma, eosinophilia, vasculitis
- **MPO-ANCA in ~40 percent**; ANCA-positive = vasculitic phenotype; ANCA-negative = eosinophilic/cardiac
- **Cardiac = leading cause of death** — ECG, troponin, echo, cardiac MRI
- Mononeuritis multiplex; mesenteric vasculitis; GN
- **Mepolizumab** for non-severe (MIRRA); **cyclophosphamide** for severe / organ-threatening
- Avoid high-dose steroids long-term
Renal-limited vasculitis (RLV)
Pauci-immune GN without systemic features
- Pauci-immune crescentic GN with MPO or PR3 positivity, no extrarenal disease
- Treated as MPA-equivalent
- Outcomes tied to creatinine at presentation and biopsy chronicity
- Differential is wide — exclude anti-GBM, IgA nephropathy, lupus nephritis
Drug-induced AAV
- Common culprits: propylthiouracil (PTU), hydralazine, minocycline, allopurinol, sulfonamides, penicillamine, anti-TNF agents, carbimazole, thiamazole.
- Levamisole-adulterated cocaine — characteristic ear-pinna necrosis, retiform purpura, neutropenia, high-titre MPO-ANCA with or without PR3-ANCA, ANA with anti-histone antibodies.
- Management: stop the culprit drug; immunosuppression only if organ-threatening.
- Prognosis: usually remits on drug cessation over weeks to months. [1]
Anti-GBM and ANCA double-positivity
- Pulmonary-renal syndrome with both anti-GBM antibodies and ANCA (PR3 or MPO).
- Daily plasma exchange until anti-GBM is undetectable, plus induction immunosuppression (rituximab or cyclophosphamide plus steroids).
- Higher relapse risk if anti-GBM persists.
- Treat as anti-GBM with the addition of the AAV immunosuppression protocol. [1]
EGPA cardiac involvement
- Cardiac involvement in EGPA is the leading cause of death in this subtype.
- Screening at diagnosis and during follow-up: ECG, troponin, BNP, transthoracic echo, cardiac MRI with late gadolinium enhancement.
- Eosinophilic myocarditis, pericardial effusion, valvulitis, heart failure, arrhythmia.
- Manage as severe EGPA with cyclophosphamide; consider temporary pacing for conduction block; anticoagulate if LV thrombus. [1]
Pregnancy in AAV
- Plan conception in quiescent disease (BVAS = 0, off cyclophosphamide more than three to six months, prednisolone under 10 mg/day).
- Rituximab: acceptable in early pregnancy; avoid third trimester (neonatal B-cell depletion).
- Azathioprine: compatible.
- Cyclophosphamide, mycophenolate, methotrexate, leflunomide: STOP — teratogenic. Mycophenolate particularly associated with miscarriage and birth defects.
- Low-dose aspirin for antiphospholipid overlap.
- Avoid live vaccines in the neonate during the first six months if the mother received rituximab in pregnancy. [1]
Paediatric AAV
- Rare, more often GPA phenotype.
- Weight-based dosing; consider cyclophosphamide cumulative-dose limits in young patients (fertility concerns).
- Rituximab 375 mg/m² weekly x 4 is the standard; growth, bone, vaccination are key concerns. [1]
Complications & Pitfalls
Disease-related complications
- End-stage kidney disease (ESKD) — most feared renal complication; ARRS predicts risk. Dialysis-dependent renal AAV has worse prognosis; transplant is safe after one to two years of quiescent disease.
- DAH — recurrent if ANCA persists; urgent plasma exchange plus induction.
- Subglottic stenosis — serial dilatation, intralesional steroids, surgical reconstruction; tracheostomy in severe stenosis.
- Saddle-nose deformity — cosmetic and functional; otolaryngology reconstruction after disease control.
- Peripheral neuropathy (mononeuritis multiplex) — usually improves with induction but residual deficits can persist.
- EGPA cardiomyopathy — eosinophilic myocarditis, heart failure, arrhythmia, sudden death.
- Mesenteric vasculitis — abdominal pain, bowel ischaemia, perforation.
- Venous thromboembolism — VTE rates two- to three-fold above baseline during active disease and the first six months of therapy.
- Accelerated atherosclerosis — chronic inflammation plus long-term steroids increase cardiovascular morbidity. [1]
Treatment-related complications
- Cyclophosphamide: cytopenias, haemorrhagic cystitis, urothelial carcinoma, infertility, lymphoma. Cumulative-dose limits guide the switch to maintenance.
- Rituximab: hypogammaglobulinaemia, late-onset neutropenia (three months post-infusion), HBV reactivation, PML (very rare), infusion reactions.
- Glucocorticoids: weight gain, diabetes, hypertension, osteoporosis and vertebral fracture, avascular necrosis, cataract, mood disturbance, infection.
- Azathioprine: myelosuppression (TPMT activity guides dose), hepatotoxicity, lymphoma.
- Plasma exchange: line complications (pneumothorax, arterial puncture, line sepsis), bleeding, hypocalcaemia, citrate toxicity.
- Mepolizumab: rarely anaphylaxis; no other class-specific complications.
- Avacopan: hepatotoxicity; monitor LFTs monthly. [1]
Pitfalls to avoid
- Treating the ANCA titre, not the patient. A rising PR3 titre predicts but does not equal relapse. Re-induction is on clinical grounds.
- Missing limited GPA — seronegative, ENT-only; the wrong biopsy site misses the diagnosis; do not ignore ENT-only disease because severe multi-organ relapse can emerge.
- Biopsying the wrong kidney — always confirm that the kidney for biopsy is the one with the worse function; biopsy correlates poorly with contralateral disease.
- Confusing DAH with pneumonia — haemoptysis plus falling Hb plus diffuse GGO plus rising KCO = DAH until proven otherwise; the BAL is "progressively bloodier."
- Treating double-positive AAV as anti-GBM alone — add PLEX plus AAV induction.
- Skipping Pneumocystis prophylaxis — cotrimoxazole is mandatory on cyclophosphamide, rituximab, and long steroids.
- Ignoring fertility concerns in cyclophosphamide exposure — discuss sperm and egg banking before therapy.
- Giving cyclophosphamide at full dose to an elderly patient — reduce for age over 65 and renal impairment. [1]
Prognosis & Disposition
Survival
Modern induction therapy has transformed AAV from a fatal illness to a chronic relapsing-remitting disease. 5-year survival is now 75 to 90% in severe disease, with rates higher in MPO-AAV (renal-limited, less relapse) than in PR3-AAV (multi-organ, more relapse). The leading causes of death are infection (first two years), active vasculitis (especially DAH), cardiovascular disease, and ESKD. [1]
Relapse
- PR3-AAV relapses in up to 50% at 5 years; MPO-AAV in 20 to 30%.
- Predictors of relapse: PR3-ANCA, ENT involvement at presentation, persisting PR3 positivity after induction, chronic nasal S. aureus carriage, prior relapse.
- Predictors of ESKD: dialysis at presentation, creatinine over 500 µmol/L, crescents in more than 50% of glomeruli, severe tubulointerstitial fibrosis, age, PR3 status.
- Maintenance therapy is given for at least 24 to 36 months (longer in PR3-AAV) — the MAINRITSAN trials show that early withdrawal is associated with rebound relapse. [1]
Disposition
- Renal replacement therapy: dialysis-dependent patients should be considered for renal transplant after one to two years of quiescent disease; recurrence post-transplant is uncommon if disease is quiescent. Living-donor transplantation is acceptable.
- Cardiology referral for EGPA patients (any evidence of cardiac disease warrants specialist review).
- ENT follow-up for GPA patients (subglottic stenosis, sinus disease, otitis media).
- Multidisciplinary vasculitis clinic is the standard of care in major centres — rheumatology, nephrology, nursing, pharmacy. [1]
Special Populations
Pregnancy
- Plan conception during a period of quiescent disease (BVAS = 0, off cyclophosphamide more than three to six months, on azathioprine or approved rituximab).
- Continue azathioprine if needed — compatible with pregnancy.
- Avoid: cyclophosphamide (especially first trimester), mycophenolate, methotrexate, leflunomide, and high-dose steroids (especially dexamethasone and betamethasone).
- Rituximab can be used in early pregnancy; defer last trimester infusion where possible to avoid neonatal B-cell depletion. The infant should receive no live vaccines for 6 to 12 months.
- Low-dose aspirin if antiphospholipid overlap.
- Multi-disciplinary care: obstetrics, rheumatology, nephrology, neonatology.
- Disease flare during pregnancy: oral prednisolone is safe; cyclophosphamide reserved for life-threatening disease (second and third trimester).
- Post-partum flare risk — continue close monitoring. [1]
Children
- Paediatric AAV is rare, more often GPA phenotype. Weight-based dosing of rituximab 375 mg/m² weekly x 4 and cyclophosphamide 15 mg/kg every three to four weeks.
- Growth, bone health, fertility, vaccination catch-up are particular concerns in chronic immunosuppression.
- School attendance, sport, and psychological support are part of the management plan. [1]
Elderly
- More MPO-AAV and renal-predominant disease in those over 65.
- Worse tolerance of cyclophosphamide and high-dose steroids.
- Prefer rituximab and reduced-dose glucocorticoids (PEXIVAS-supported). Use the reduced-dose steroid protocol if there is no contraindication.
- Bone protection, fall prevention, frailty assessment, polypharmacy review.
- Higher threshold for plasma exchange given line complications. [1]
Renal impairment and dialysis
- Cyclophosphamide dose reduces by 25% for CrCl below 30 mL/min.
- Rituximab, methylprednisolone, azathioprine, mycophenolate, mepolizumab, avacopan are unaffected by renal function.
- Avacopan is particularly useful in patients who cannot tolerate high-dose steroids and are already on dialysis — a steroid-sparing strategy.
- Renal transplant after one to two years of quiescent disease; low recurrence rate. [1]
Immunosuppression and infection
- Latent TB — screen (QuantiFERON) and treat with isoniazid plus pyridoxine if positive before immunosuppression.
- Hepatitis B — HBsAg-positive or anti-HBc-positive patients should receive entecavir or tenofovir prophylaxis for at least 12 months after rituximab; check HBV DNA at three months.
- Hepatitis C — DAA therapy before immunosuppression.
- HIV — antiretroviral therapy before immunosuppression.
- Pneumocystis jirovecii prophylaxis (cotrimoxazole) on cyclophosphamide, rituximab, or sustained high-dose steroids.
- Vaccinations: influenza (annual), pneumococcal (PCV13 then PPSV23), COVID-19, hepatitis B (before rituximab if non-immune), HPV, shingles (Shingrex non-live vaccine, often given in immunosuppression). Avoid live vaccines during immunosuppression and for months after (MMR, varicella, yellow fever, BCG, oral typhoid, rotavirus). [1]
Anticoagulated patients
- Active AAV increases VTE risk two- to three-fold; LMWH is preferred.
- Avoid NSAIDs in renal disease.
- Direct oral anticoagulants (DOACs) are used in non-valvular AF, with dose adjustment in renal impairment. [1]
Evidence, Guidelines & Regional Differences
Pivotal trials to cite in viva and academic answers
- CHCC 2012 — Jennette, Arthritis Rheum 2012/2013 (PMID 23045170): the standard nomenclature.
- RAVE 2010 — Stone NEJM 2010 (PMID 20647199): rituximab non-inferior to cyclophosphamide; superior in relapsing disease.
- RITUXVAS 2010 — Jones: rituximab-based regimen in renal AAV; comparable renal outcomes, lower cumulative cyclophosphamide.
- CYCLOPS 2009 — de Groot Ann Intern Med 2009 (PMID 20505178): pulse IV cyclophosphamide non-inferior to oral; lower cumulative dose.
- MEPEX 2007 — Jayne JASN 2007 (PMID 17582159): plasma exchange versus methylprednisolone in severe renal AAV; early benefit favouring PLEX, attenuated long-term.
- PEXIVAS 2020 — Walsh NEJM 2020 (PMID 32053298): plasma exchange did not reduce death or ESKD overall; reduced-dose glucocorticoid non-inferior with fewer infections.
- MAINRITSAN 2014 — Guillevin: rituximab superior to azathioprine for maintenance.
- MAINRITSAN 2 2018 — Charles NEJM 2018: tailored rituximab also superior.
- MAINRITSAN 3 2020: extended rituximab maintenance further reduced relapse versus azathioprine.
- IMPROVE 2010 — Hiemstra JAMA 2010 (PMID 21060104): azathioprine superior to mycophenolate for relapse-free maintenance.
- MIRRA 2017 — Wechsler NEJM 2017 (PMID 28514601): mepolizumab 300 mg SC every four weeks improved remission and steroid-sparing in relapsing or refractory EGPA.
- ADVOCATE 2021 — Jayne NEJM 2021: avacopan (C5a receptor blocker) achieved sustained remission with steroid sparing in AAV.
- NORAM 2005 — de Groot: methotrexate non-inferior to cyclophosphamide for limited disease induction. [1]
A management timeline for severe AAV
Exam Pearls
[1]Red Flags
Exam application bank (NEET-PG / INICET)
One-line answer
ANCA-associated vasculitis (AAV) comprises three necrotising small-to-medium vessel vasculitides: GPA (granulomatosis with polyangiitis — PR3/c-ANCA; ENT + pulmonary + renal), MPA (microscopic polyangiitis — MPO/p-ANCA; renal + pulmonary + neuropathy, no granulomatous ENT), and EGPA (eosinophilic granulomatosis with polyangiitis — MPO/p-ANCA in ~40%; asthma + eosinophilia + neuropathy + cardiac = leading cause of death). The hallmark renal lesion is pauci-immune crescentic glomerulonephritis (minimal immunoglobulin/complement deposition on IF — distinguishes from immune-complex GN). Cutaneous features include palpable purpura, nodules, ulcers and digital ischaemia. Management is divided into induction (rituximab or cyclophosphamide + high-dose corticosteroids — RAVE trial proved equivalence) and maintenance (rituximab or azathioprine/MMF + low-dose steroids), with plasma exchange for sev
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard. [1]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes. [1]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change. [1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each. [1]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory. [1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on ANCA-associated vasculitis.
[1]References
- [1]Kronbichler A, Bajema IM, Bruchfeld A, et al. Diagnosis and management of ANCA-associated vasculitis Lancet, 2024.PMID 38368016
- [2]Kitching AR, Anders HJ, Basu N, et al. ANCA-associated vasculitis Nat Rev Dis Primers, 2020.PMID 32855422
- [3]Hellmich B, Sanchez-Alamo B, Schirmer JH, et al. EULAR recommendations for the management of ANCA-associated vasculitis: 2022 update Ann Rheum Dis, 2024.PMID 36927642
- [4]Yaseen K, Mandell BF. ANCA associated vasculitis (AAV): a review for internists Postgrad Med, 2023.PMID 35831990
- [5]White J, Dubey S. Eosinophilic granulomatosis with polyangiitis: A review Autoimmun Rev, 2023.PMID 36283646
- [6]Emmi G, Bettiol A, Gelain E, et al. Evidence-Based Guideline for the diagnosis and management of eosinophilic granulomatosis with polyangiitis Nat Rev Rheumatol, 2023.PMID 37161084
- [7]Trivioli G, Terrier B, Vaglio A. Eosinophilic granulomatosis with polyangiitis: understanding the disease and its management Rheumatology (Oxford), 2020.PMID 32348510
- [8]Fraticelli P, Benfaremo D, Gabrielli A. Diagnosis and management of leukocytoclastic vasculitis Intern Emerg Med, 2021.PMID 33713282