Dermatology · Medicine
Androgenetic alopecia
Also known as Androgenetic alopecia (AGA) · Male pattern hair loss (MPHL) · Female pattern hair loss (FPHL) · Pattern baldness · Common baldness · Pattern hair loss (PHL)
Androgenetic alopecia (AGA) is the commonest cause of hair loss in both sexes, driven by dihydrotestosterone (DHT)-mediated progressive miniaturisation of genetically susceptible scalp hair follicles. Male pattern (Hamilton-Norwood): bitemporal recession + vertex thinning → confluence. Female pattern (Ludwig): diffuse central thinning with frontal hairline preserved; the Olsen Christmas-tree pattern adds a frontal accentuation. Trichoscopy: hair diameter diversity 20% (anisotrichosis), peripilar sign, yellow dots. Treatment: minoxidil (topical 5% or oral low-dose; works in both sexes); finasteride 1 mg/day (5-alpha-reductase type II inhibitor; male only; contraindicated in women of childbearing potential — teratogenic); dutasteride (dual 5-AR I+II inhibitor; more potent); spironolactone (antiandrogen; female); hair transplant (FUE/FUT). All treatments require lifelong commitment — withdrawal reverses benefit in 3-6 months.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Exam tags
Red flags
1. Definition and Classification
Androgenetic alopecia (AGA) is the most common cause of hair loss in both men and women — a genetically determined, androgen-dependent, progressive miniaturisation of susceptible scalp hair follicles leading to patterned hair thinning. Three diagnostic pillars are used in the operating definition: (1) characteristic clinical pattern, (2) trichoscopic features (anisotrichosis), and (3) exclusion of scarring or inflammatory mimics.[1][7]
The terminology warrants precision because boards reward those who can name systems precisely: [1]
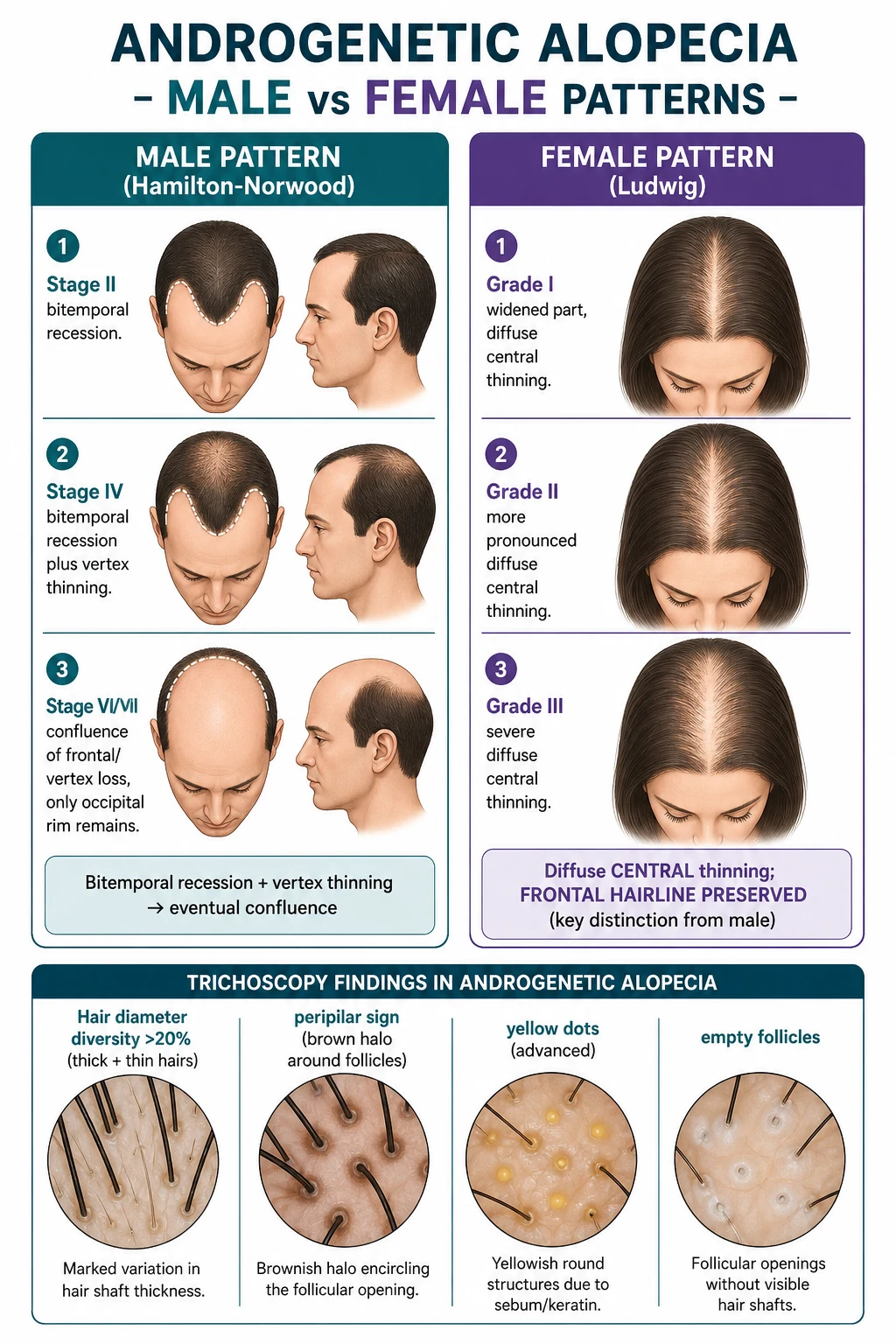
- Male pattern hair loss (MPHL) — Hamilton-Norwood classification (the most widely used; 7 stages with substages).
- Female pattern hair loss (FPHL) — most commonly Ludwig (3 grades); also Olsen "Christmas-tree" pattern (frontal accentuation).
- Pattern hair loss (PHL) — gender-neutral modern umbrella term.
- Diffuse unpatterned alopecia (DUPA) — uncommon female pattern; rapid, severe, often hyperandrogenic; biopsy for confirmation.[2]
AGA is a non-cicatricial (non-scarring) alopecia — the follicular ostia are preserved under trichoscopy, which is the single most useful discriminator from scarring alopecias (lichen planopilaris, frontal fibrosing alopecia, discoid lupus erythematosus). Within non-cicatricial alopecias, AGA is distinguished from telogen effluvium by hair diameter diversity >20% (anisotrichosis) — telogen effluvium shows uniform thinning of all hairs.[1][2][7]
Classification frameworks
Three classification systems are encountered in practice, and the examiner rewards the clinician who can name each: [1]
The terminal-to-vellus ratio on horizontal scalp biopsy is the histological signature of AGA: a ratio below 4:1 (normally 7-9:1) is diagnostic when the clinical picture is uncertain.[7]
2. Epidemiology
AGA is a near-universal feature of ageing in susceptible populations, but its prevalence, age of onset, and severity vary strikingly by sex, ethnicity, and genetics. Understanding these patterns helps the clinician set realistic expectations and screen appropriately.[8]
Age and sex distribution. Men typically present in their late teens to late 20s; one in four men is affected by age 30. Women usually notice thinning in their 40s-50s (perimenopausal transition), but PCOS, insulin resistance, and adrenal hyperandrogenism can produce early-onset FPHL in the 20s. The Ludwig grade at presentation tends to be milder in women, but progression is similar over decades.[2][8]
Ethnic variation. AGA prevalence is highest in Caucasians, intermediate in Asians, and lowest in Africans (the African occipital "halo" of DHT-resistant follicles is robust). The pattern also differs: Asian men have less bitemporal recession and more diffuse frontal/vertex thinning than Caucasians. African women have a higher rate of traction-related (cicatricial) marginal alopecia and a lower rate of FPHL, though androgenic contribution to frontal fibrosing alopecia is being increasingly recognised.[2][8]
Genetics. Inheritance is polygenic with a major X-linked component: [1]
- Androgen receptor (AR) gene — Xq12; the CAG repeat length in exon 1 modulates AR transcriptional activity (shorter repeats = more active receptor = more AGA).
- SRD5A2 (5-alpha-reductase type II) on chromosome 2p23; polymorphisms alter DHT output.
- WNT pathway genes (WNT10A, LEF1, DKK1 regulators) — control follicular fate and anagen entry.
- Paternal contribution has historically been over-emphasised; maternal line carries the AR allele, hence the bedside tradition of asking about the maternal grandfather.[2][8]
Cardiometabolic comorbidity. Early-onset AGA in men is now an established cardiovascular risk marker — associated with insulin resistance, metabolic syndrome, and diabetes, independent of BMI. The link is bi-directional: hyperinsulinaemia suppresses SHBG, raising free androgen availability. This does not change management of the hair loss but adds value to a dermatology consultation.[12][13]
3. Pathophysiology
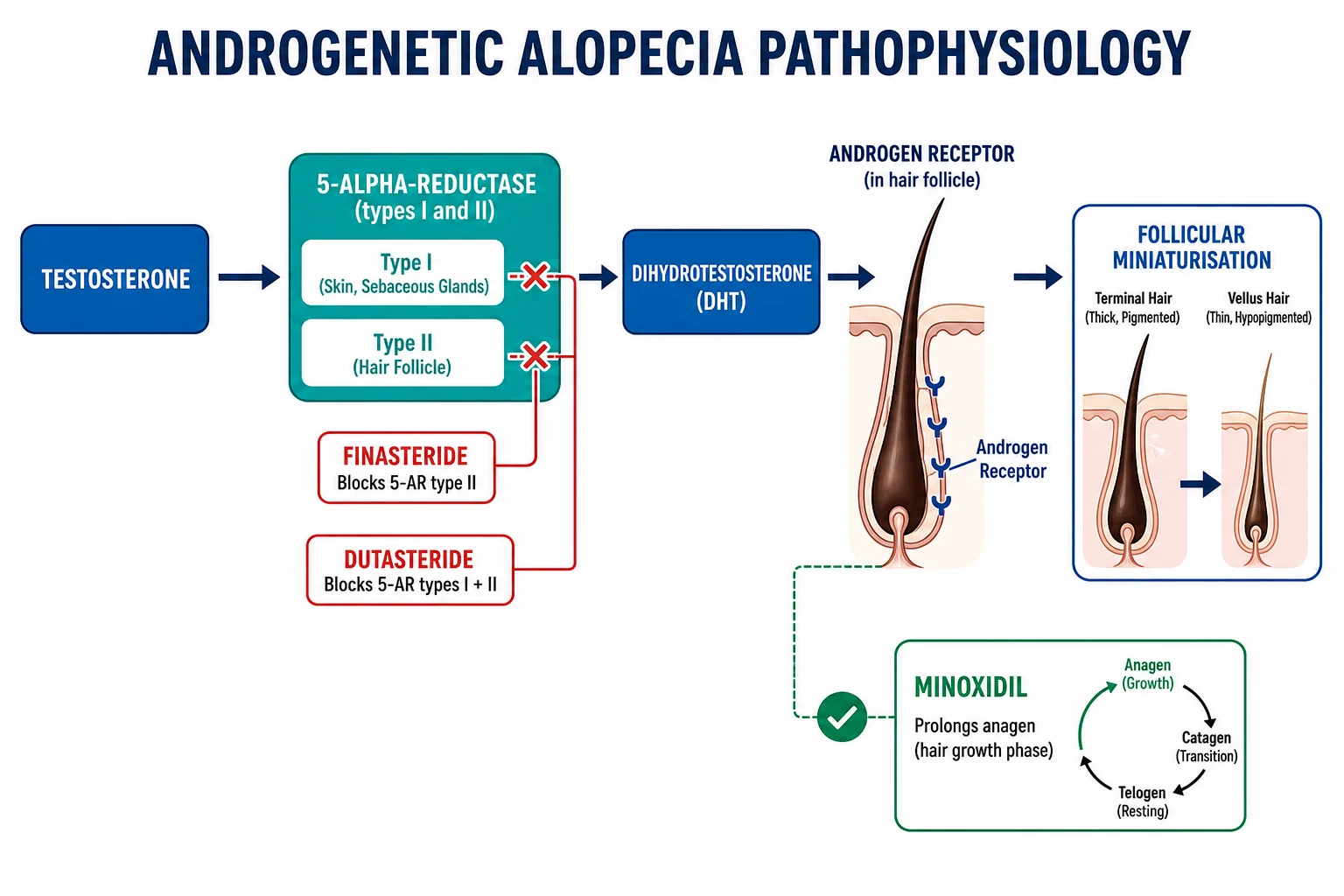
The biology of AGA is, at its core, androgen-driven follicular miniaturisation in genetically susceptible scalp. The stereotype "testosterone-causes-baldness" is wrong: testosterone alone does not miniaturise follicles — its reduced metabolite, dihydrotestosterone (DHT), is the culprit, and it acts only on follicles that express a permissive AR signature.[1][2][7]
In a genetically susceptible individual the cascade runs as follows:[1][2][7]
- Testosterone (T) enters dermal papilla cells of susceptible follicles and is converted to dihydrotestosterone (DHT) by 5-alpha-reductase.
- Type I 5-AR (SRD5A1) — predominantly in skin, sebaceous glands, and liver.
- Type II 5-AR (SRD5A2) — predominantly in prostate, hair follicles, beard, liver.
- DHT binds the androgen receptor with ~5× the affinity of testosterone; the activated AR translocates to the nucleus and modifies gene expression.
- Dermal papilla cells secrete paracrine factors — TGF-β1, TGF-β2, DKK-1 (dickkopf-1, a WNT antagonist), PGD2 (prostaglandin D2 via lipocalin-type PGD synthase), and IL-6 — that signal overlying matrix and epithelial cells to shorten anagen (the growth phase) and progressively shrink the follicular bulb.
- Over multiple hair cycles the follicle produces a thinner (vellus) hair with shorter length, lighter pigment, and a shallower bulb; the cycle ratio of anagen-to-telogen shifts from ~9:1 to ~2:1.
- With sufficient cycles, the follicle becomes so small it is invisible clinically — but it does not "die", which is why hair transplant (relocating occipital, DHT-resistant follicles) works.
- Occipital and lateral temporal follicles are DHT-resistant — the molecular basis is thought to be lower local 5-AR Type II expression and a different AR co-regulator milieu. These are the donor follicles of hair transplantation and explain the preserved "horseshoe" rim in advanced Hamilton-Norwood VII.[1][2]
5-alpha-reductase Type I
SRD5A1 — skin/liver
- Predominant in **skin, sebaceous glands, liver**
- Contributes modestly to scalp DHT
- Inhibited by **dutasteride** (and not by finasteride, which is Type-II-selective)
- Reduces scalp DHT by ~30% when blocked alone
5-alpha-reductase Type II
SRD5A2 — prostate/hair
- Predominant in **prostate, hair follicles, beard, liver**
- **Major driver of scalp DHT production** — finasteride blocks ~70% serum DHT; dutasteride blocks >90%
- Inhibited by **finasteride** and **dutasteride**
- Mutations cause **5-alpha-reductase type 2 deficiency** — a DSD in 46,XY males with ambiguous genitalia at birth
Androgen receptor (AR)
X-linked; CAG repeat polymorphism
- Encoded on **Xq12** — inherited predominantly from the maternal line
- **CAG repeat length** inversely correlates with AR activity (shorter = more active = more AGA)
- Blocked by **spironolactone, bicalutamide, flutamide, finasteride (partial AR inhibition at higher doses)**
- Mutation causes **complete androgen insensitivity syndrome (CAIS)** in 46,XY — scalp hair is preserved despite high testosterone, confirming that AR is essential
PGD2 and PTGDS
Newer pathway targets
- Lipocalin-type PGD2 synthase (PTGDS) and PGD2 are elevated in balding scalp
- PGD2 and its metabolite 15-dPGJ2 act on GPR44 (DP2) to **inhibit hair growth**
- Setipiprant (oral DP2 antagonist) was trialled for AGA — results modest
- Castration before puberty prevents AGA (Hamilton); AGA does not occur in CAIS males (functional AR essential)
Why occipital follicles escape
Occipital and lateral-temporal follicles retain their terminal-calibre growth even in advanced AGA (Norwood VII). The basis is donor dominance — a transplanted occipital follicle continues to behave as occipital even when relocated to a vertex recipient site. Molecularly, occipital follicular AR expression and 5-AR II activity are reduced compared with vertex follicles; they also express higher levels of WNT agonists. This contrast is the rationale for hair transplantation: each occipital graft is permanently programmed to resist DHT.[3]
DHT destruction chain — recall it in 4 letters
DHT-MAP
DHT enters dermal papilla cells and binds the androgen receptor (AR); the AR–DHT complex dimerises, translocates to the nucleus, and modulates gene expression. Susceptibility is determined by AR CAG repeat length, AR expression, and local 5-AR activity.
Anagen (growth phase) shortens from years to months; telogen (resting phase) lengthens; the proportion of growing to resting hairs falls from ~9:1 toward ~2:1, producing clinically visible shedding.
Follicles produce thinner, shorter, less-pigmented vellus hairs with each cycle. Trichoscopy shows anisotrichosis (>20% hair diameter diversity). Histology: terminal-to-vellus ratio falls below 4:1.
AGA is NON-SCARRING — follicular ostia are PRESERVED on trichoscopy. The follicle is miniaturised but alive. This is the discriminator from cicatricial alopecia and is the basis of hair transplantation (occipital donor grafts remain DHT-resistant in recipient sites).
Dermal papilla cells secrete TGF-β1/β2 (suppress matrix-cell proliferation), DKK1 (WNT antagonist — blocks anagen entry), and PGD2 (via PTGDS) acting on GPR44 (DP2) to inhibit hair growth. Setipiprant (DP2 antagonist) trialled with modest benefit.
4. Clinical Presentation
AGA presents with a clinically recognisable pattern of hair thinning that differs between men and women. The pattern is so characteristic that diagnosis is clinical — supplemented by trichoscopy when in doubt — and scalp biopsy is rarely needed.[1][2][7]
Male pattern (Hamilton-Norwood classification)
The Hamilton-Norwood classification is the most widely used staging system; it has 7 main stages plus 4 vertex substages (III vertex, III a, IV a, V a). The temporal recession and vertex thinning follow a predictable trajectory.[2][7]
The occipital and lateral-temporal "donor" rim is preserved in all stages and is the basis for hair transplantation. Patients will sometimes mis-name "vertex" as "crown" — these are the same region. In early-onset AGA (Norwood III before age 25), disease progression is faster and the family history is more often strong; these patients warrant counselling about more aggressive therapy.[1][2]
Female pattern
The most common FPHL pattern is Ludwig (3 grades). The frontal hairline is preserved in all grades — this is the discriminator from male pattern. [1]
Male pattern versus female pattern
The pattern differs by what is preserved, not by what is lost: [1]
Male pattern (MPHL)
Hamilton-Norwood
- **Bitemporal recession** is the FIRST visible change
- **Vertex thinning** follows; the two regions eventually merge
- **Frontal hairline RECOILS** — this is the visible hallmark
- Occipital and lateral temporal hair **PRESERVED** at all stages (donor dominance)
- Onset late teens to 30s; ~50% of men by age 50
- Scalp is rarely visible without hair styling; pattern is "hairline losing ground"
Female pattern (FPHL)
Ludwig / Olsen
- **Diffuse central thinning** at the crown and midline part
- **Frontal hairline PRESERVED** in all Ludwig grades (the discriminator)
- **Bitemporal recession ABSENT** (or only minimal)
- Widened midline part with visible scalp; Olsen "Christmas-tree" shows frontal accentuation along part
- Onset typically 40s-50s, accelerated by menopause; earlier with PCOS
- ~40% of women by age 70; lower in Asians and Africans
Age patterns and atypical presentations
Three patterns warrant a closer look: [1]
- Early-onset AGA in men (younger than 25) — more androgen-driven, faster progression, stronger family history, and frequently associated with cardiometabolic risk markers (insulin resistance, metabolic syndrome, dyslipidaemia). Counsel about cardiovascular health; consider early combination therapy.[12][13]
- Diffuse unpatterned alopecia (DUPA) in young women — rapid, severe, often hyperandrogenic; clinically mimics telogen effluvium. Biopsy confirms the diagnosis (terminal-to-vellus ratio dropping below 4:1; preserved follicular ostia).
- Sudden or rapid onset in either sex — reconsider the diagnosis; look for an inciting drug, nutritional deficiency, endocrine disorder, or inflammatory mimic.
Psychosocial impact
AGA is not "just cosmetic." Multiple systematic reviews have documented significant psychosocial burden: [1]
- Depression and anxiety are increased (OR 1.3-1.5); clinically meaningful in ~25% of patients, often uncorrelated with objective severity.
- Body dysmorphic disorder is over-represented (some studies suggest 10-15%, particularly in men who seek cosmetic procedures).
- Workplace and social confidence are affected in men with visible loss.
- The clinician should ask directly about mood, social withdrawal, and impact on relationships; referral for psychological support is sometimes more important than the next prescription.[3]
5. Differential Diagnosis — "The Big Five"
The bedside differential of pattern hair loss is wide, and every candidate must be excluded before committing a patient to lifelong therapy. The examiner almost always asks about at least one of these:[1][2][7]

Telogen effluvium
Diffuse uniform shedding — not patterned
- **Diffuse uniform thinning**; **frontal hairline preserved** (like FPHL)
- **Hair pull POSITIVE** (>6 telogen hairs); trichoscopy shows uniform hair diameter (NO anisotrichosis)
- **Trigger** 2-4 months before: childbirth, severe illness, surgery, crash diet, iron deficiency, hypothyroidism, drugs (heparin, retinoids, beta-blockers)
- **Acute TE** (duration under 6 months) self-resolves once trigger removed
- **Chronic TE** (>6 months) — investigate for ongoing triggers (iron, thyroid, nutritional, drugs)
- Biopsy: terminal-to-vellus ratio NORMAL (>8:1); increased telogen count without miniaturisation
Alopecia areata
Patchy smooth — autoimmune
- **Sudden patchy** smooth hair loss; "exclamation-mark hairs" at edge (distal wider than proximal)
- **Hair pull POSITIVE** at the edge of active patches; trichoscopy shows black dots, yellow dots, tapered hairs
- **Nail pitting** is supportive; associated with other autoimmune disease (thyroid, vitiligo, type 1 diabetes)
- Loss of follicular ostia is RARE (no scarring in classic AA); sparing of grey hairs in active AA is classical
- AA incognita and AA totalis/alopecia universalis are diffuse variants that mimic TE or severe FPHL
- Biopsy: peribulbar lymphocytic "swarm of bees" infiltrate; immunofluorescence shows anti-hair-follicle antibodies
Trichotillomania
Self-induced — variable length broken hairs
- **Irregular patches** with broken hairs of **varying length** (vs uniform in AA); the only hairs left are those broken by pulling
- Common in adolescents and young adults; female preponderance; body-focused repetitive behaviour
- Trichoscopy shows **trichoptilosis** (split ends), **trichomalacia**, **V-sign** (two hairs broken at same level from same ostium), **hair powder
- Often denied or minimised; biopsy shows **trichomalacia** and empty anagen bulbs
- Treatment: CBT, habit reversal therapy; SSRIs if comorbid anxiety/depression; N-acetylcysteine trial evidence
Tinea capitis
Children — scaly patches, broken hairs, KOH-positive
- **Children predominantly** (rare in adults); anthropophilic (Trichophyton tonsurans in the US/UK; Microsporum canis in Europe/Asia)
- **Scaly patches** with hairs broken at 2-3 mm above scalp ("grey patch"); "black dot" variant in darker hair
- **Kerion** = inflammatory mass with boggy swelling, pustules, crusting; can mimic abscess — do NOT incise
- Wood's lamp: green fluorescence with Microsporum spp. (not Trichophyton); KOH positive in all
- Trichoscopy: comma, corkscrew, "Morse-code" hairs; peripilar and interfollicular scaling
- Oral griseofulvin (or terbinafine) 6-8 weeks; household contacts treated; kerion adds oral corticosteroid
Cicatricial (scarring) alopecia
Loss of follicular ostia — never AGA
- **Lichen planopilaris (LPP)** — perifollicular erythema/scale, tufted folliculitis, occipital predilection
- **Frontal fibrosing alopecia (FFA)** — band-like frontal hairline recession with loss of follicular ostia and perifollicular erythema; postmenopausal women predominantly; associated with facial sunscreen use (controversial)
- **Discoid lupus erythematosus (DLE)** — central hypopigmentation, follicular plugging, adherent scale; positive ANA in 20%, anti-Ro/SSA more specific; can show discoid plaques with central scarring
- **Central centrifugal cicatricial alopecia (CCCA)** — vertex scarring in women of African descent; hair-care practices contributing
- **Folliculitis decalvans** — pustular, tufted folliculitis, Staphylococcus aureus; recurrent
- **Discriminator: follicular ostia LOST** — never AGA. Always biopsy if any doubt
Other important mimickers
- Drug-induced alopecia — anticoagulants (warfarin, heparin), retinoids (acitretin, isotretinoin), beta-blockers (especially metoprolol), lithium, valproate, carbamazepine, allopurinol, cimetidine, indinavir, and cytotoxics (always diffuse and reversible once drug stopped).
- Iron deficiency without anaemia — low ferritin even with normal Hb is associated with chronic TE and worse FPHL response.
- Endocrine — hypothyroidism, hyperthyroidism, hypopituitarism.
- Nutritional — protein-energy malnutrition, zinc deficiency, vitamin D deficiency, essential fatty acid deficiency.
- Syphilitic moth-eaten alopecia — secondary syphilis; non-specific patchy "moth-eaten" hair loss; positive VDRL/RPR; responds to penicillin.
- Hypotrichosis simplex — autosomal dominant; diffuse thinning from childhood; biopsy confirms normal terminal-to-vellus ratio but low total density.
- Pressure alopecia — post-operative or ICU; typically resolves over months.
- Traction alopecia — hairstyling practices (tight braids, ponytails, weaves, hair extensions); marginal and frontotemporal hair loss; reversible early, scarring late. [1]
6. Bedside Assessment
A structured bedside assessment is the cornerstone of the AGA consultation. The clinician who can demonstrate a systematic approach stands out at fellowship and is better positioned to triage referrals. [1]
History
- Onset and duration — sudden (alopecia areata, drug, TE), gradual (AGA), or seasonal variation.
- Pattern of shedding — patterned (AGA), diffuse (TE), patchy (AA, trichotillomania), marginal (FFA, traction).
- Family history — ask specifically about the maternal grandfather and uncles, the paternal line, and any female relatives with thinning.
- Medical history — PCOS, thyroid disease, anaemia, autoimmune disease, malnutrition, recent illness/surgery/childbirth, cancer treatment history.
- Drug history — anticoagulants, retinoids, beta-blockers, lithium, valproate, cytotoxics, recent anaesthesia.
- Hair care practices — chemical relaxers, hot combs, tight braids (traction), weaves, extensions (especially important in women of African descent).
- Psychosocial impact — ask directly about mood, social withdrawal, relationships, work impact. [1]
Examination
A standard scalp examination takes 2 minutes and should be reproducible: [1]
- General inspection — hair density by quadrant, pattern of thinning, occipital preservation.
- Hair pull test — 50-60 hairs grasped at the scalp, gentle pull; >6 telogen hairs dislodged = positive. Negative in stable AGA; positive in active AGA, TE, AA, loose anagen syndrome. Best done after 5 days without shampooing.
- Part-width comparison — central part widening (Ludwig); frontal accentuation (Olsen Christmas-tree).
- Hair calibre assessment — run fingers through the hair from frontal to vertex; reduced calibre at vertex is suggestive of AGA.
- Follicular ostia — preserved in AGA and TE/AA; LOST in cicatricial alopecia (single most useful bedside sign).
- Trichoscopy (dermoscopy of the scalp) — see below. [1]
Trichoscopy
Trichoscopy has become the standard diagnostic adjunct. It is non-invasive, takes 30 seconds with a handheld dermatoscope (ideally ×20-70 with polarised light), and provides diagnostic features that distinguish AGA from every important alternative.[1][7]
Standardised photography
Global standardised views (vertex, frontal, bitemporal, occipital) with consistent lighting and framing allow objective comparison over months. A 1 cm × 1 cm tattoo at the vertex (tattoo dot) defines the same scalp area for trichoscopy-photo-trichogram tracking. Most dermatology clinics now use automated camera systems (e.g. Canfield, Fotofinder). [1]
[1]7. Investigations
A targeted investigation set is essential before committing a patient to lifelong therapy. Most AGA cases need little beyond clinical assessment; the work-up is reserved for atypical presentations, women with signs of hyperandrogenism, and cases that might fail first-line therapy.[1][7][8]
Baseline workup for everyone
- Full blood count, ferritin — iron deficiency is common in women and worsens hair density; aim for ferritin >40-70 µg/L (some experts suggest >70 µg/L for hair).
- TSH — overt thyroid disease worsens hair loss; subclinical hypothyroidism often coexists with FPHL.
- Vitamin D, zinc — common deficiencies with reproducible links to hair loss. [1]
Female hyperandrogenism screen
If signs of hyperandrogenism (hirsutism, acne, irregular menses, central obesity) are present, add: [1]
- Total testosterone and SHBG (low SHBG raises free androgen index).
- Free testosterone / free androgen index if total testosterone is equivocal.
- DHEA-S — adrenal androgen; elevated in adrenal hyperplasia or androgen-secreting tumour.
- Androstenedione — ovarian and adrenal; useful in PCOS.
- 17-OH progesterone — to screen for non-classic congenital adrenal hyperplasia.
- LH : FSH ratio — classically elevated in PCOS (>2:1, though not specific).
- Prolactin — hyperprolactinaemia suppresses GnRH, producing secondary hypogonadism and diffuse hair loss.
- Pelvic ultrasound — to confirm polycystic ovarian morphology (Rotterdam criteria: ≥12 follicles per ovary, or ovarian volume >10 mL, in either ovary). [1]
Baseline workup before finasteride / dutasteride (men)
- Liver function tests — baseline; derangement is uncommon but should be checked.
- PSA (prostate-specific antigen) — finasteride and dutasteride reduce serum PSA by approximately 50%. Double the measured PSA in patients on these drugs for accurate prostate cancer screening interpretation.
- Consider documenting baseline sexual function (IIEF-5) for monitoring. [1]
When to biopsy
Reserved for genuinely uncertain cases: [1]
- Scalp biopsy (4 mm punch, vertical sections) from the leading edge of thinning (frontal vs vertex should both be sampled if possible).
- AGA signature — terminal-to-vellus ratio dropping below 4:1, normal to slightly increased telogen count, preserved follicular ostia, mild perifollicular lymphocytic infiltrate.
- Biopsies from DUPA show similar findings but more globally distributed. [1]
Trichoscan / phototrichogram
Objective hair-counting methods used in clinical trials; not routine in clinical practice. Trichoscan analyses hair density, growth rate, and anagen:telogen ratio from a defined scalp area photographed under magnification. Used by AGA research groups to compare therapeutic response. [1]
8. Resuscitation — Alopecia Emergencies
AGA itself is never an emergency. But the differential diagnosis of hair loss contains several emergencies that the clinician must recognise at the bedside and triage to the appropriate pathway. The examiner rewards recognition; management comes second.[2]
Kerion celsi (tinea capitis)
Inflammatory fungal mass
- Boggy, swollen, pustular, often painful mass — usually in a child
- Looks like an abscess but is **fungal**
- **DO NOT incise and drain** — worsens scarring and may spread disease
- **Oral griseofulvin 20-25 mg/kg/day** for 6-8 weeks (or terbinafine weight-based for 4 weeks)
- **Add oral corticosteroid (prednisolone 1 mg/kg)** in severe cases to reduce scarring and speed resolution
- Household contacts investigated; pets (cats/dogs) examined by vet for M. canis
Anaphylaxis to topical minoxidil
Rare; usually propylene glycol
- Anaphylaxis to topical minoxidil is **rare but reported**
- More common reactions are **contact dermatitis** to propylene glycol (PG) vehicle
- **Switch to foam** (PG-free) if contact dermatitis; if true allergy, stop and switch to oral (cautious titration)
- Anaphylaxis: **IM adrenaline 0.5 mg (1:1000)** into anterolateral thigh; IV hydrocortisone 200 mg; IV chlorpheniramine 10 mg; IV fluid resuscitation
- Refer to allergy specialist for skin-prick / IgE testing if recurrence suspected
Post-finasteride severe mood change
Stop and refer urgently
- Severe **depression, suicidal ideation** reported in men on finasteride
- The term "post-finasteride syndrome" describes persistent sexual, neurological, and psychiatric symptoms after stopping the drug — **controversial** but reported; FDA has updated labelling
- Stop the drug at the first sign of severe mood change
- Refer urgently to psychiatry / psychology
- Consider switching to **topical finasteride** (off-label) or **dutasteride** (off-label, longer half-life); patient must be counselled about persistence risk
Minoxidil cardiovascular adverse effects
Oral minoxidil — fluid retention
- Oral minoxidil at low doses (0.625-5 mg) is well tolerated but can cause **fluid retention, oedema, pericardial effusion** (rare at low doses)
- Pericardial effusion risk is dose-dependent; caution in cardiac disease
- **Baseline** ECG and review of cardiac history before starting oral minoxidil
- Monitor weight, blood pressure, oedema at 1 month, then 3-monthly
- Stop and refer to cardiology if suspected effusion
9. Management — Stepwise by Sex and Stage
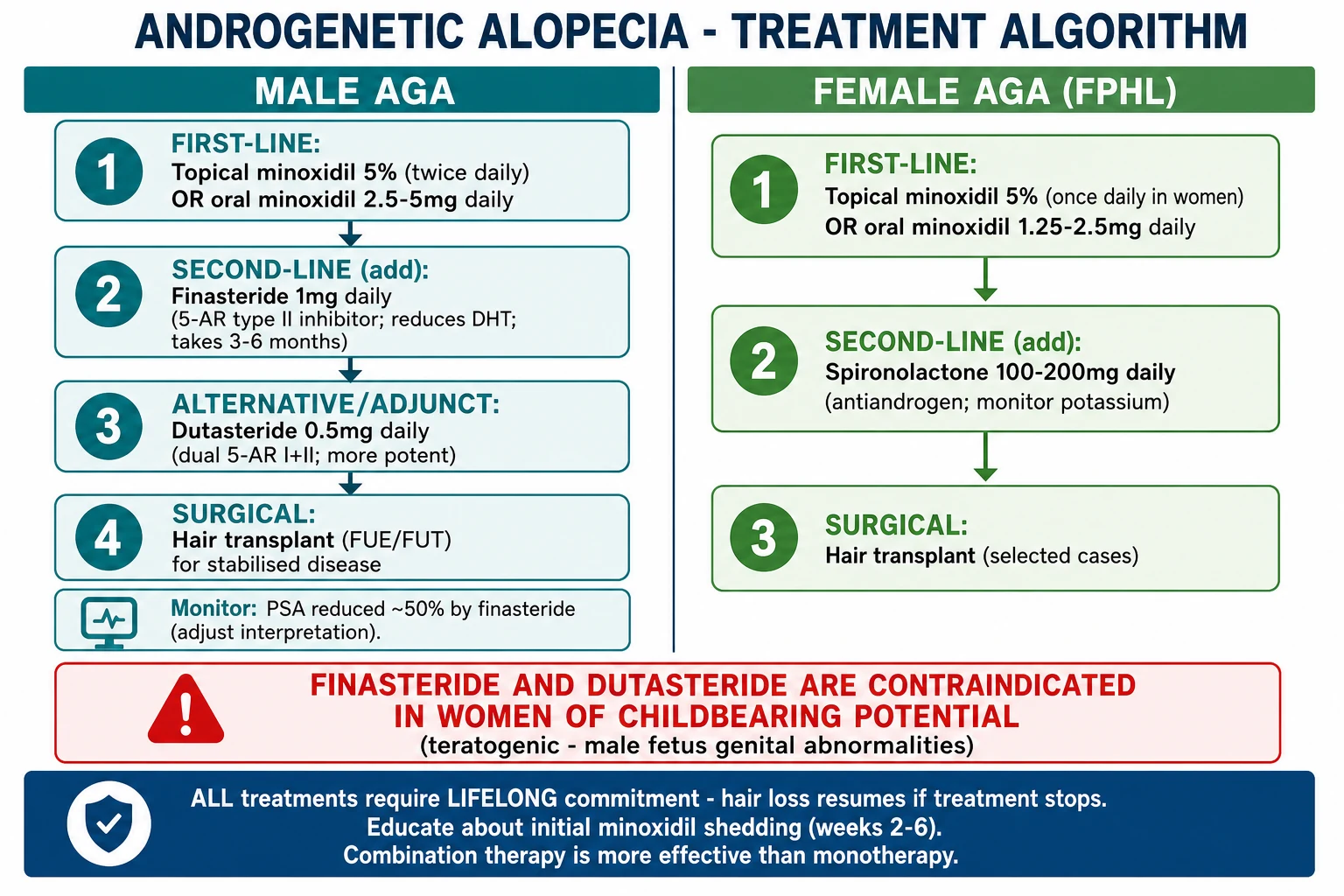
Treatment of AGA is longitudinal — the patient's response guides every adjustment — and lifelong — withdrawal reverses benefit within 3-6 months for medical therapies. The clinician who discusses adherence at the first visit prevents disappointment three years later.[1][2][3][5][6]
Drug comparison
Minoxidil — both sexes
Mechanism. Minoxidil is a potassium-channel opener and vasodilator that acts on the follicular dermal papilla and matrix cells to prolong anagen, increase follicular size, and stimulate vascular endothelial growth factor. Crucially, it is independent of the androgen pathway, which is why it works in both sexes.[6][10]
Topical 5% minoxidil:
- Men: twice-daily application to the vertex and frontal scalp; 1 mL per application.
- Women: once-daily 5% (off-label for women in some jurisdictions; 2% solution twice-daily is FDA-approved for women; in practice, 5% once-daily is widely used and effective).
- Foam is PG-free — preferred when contact dermatitis to propylene glycol is suspected.
- Initial shedding in weeks 2-6 — telogen-to-anagen transition pushes vellus hairs out before terminal regrowth; patients MUST be warned and encouraged to continue.[6]
Oral minoxidil (off-label):
- Low-dose range: 0.625 mg (women) to 5 mg (men), titrated to response and tolerability.
- Advantages — once-daily dosing, no scalp irritation, more uniform delivery, better compliance.
- Adverse effects — hypertrichosis (face, limbs; ~15-50% — usually mild and reversible on stopping or on dose reduction), fluid retention / peripheral oedema, pericardial effusion (rare at low doses; caution in cardiac disease), tachycardia, hypotension.
- Recent consensus recommendations (Gupta 2026) — low-dose oral minoxidil is a viable first-line option for both sexes when topical adherence is poor or scalp irritation limits use.[10]
Realistic counselling. Visible improvement at 3-6 months, maximum benefit at 1-2 years, lifelong commitment required. Stopping reverts any benefit within 3-6 months. [1]
Finasteride — male only
Mechanism. Selective 5-alpha-reductase type II inhibitor (Ki ~1 nM); reduces serum DHT by approximately 70% and scalp DHT by approximately 60-70%. Approved by the FDA at 1 mg/day for male AGA in 1997 (Kaufman KD 1998 — pivotal RCTs).[1][5]
Dosing. 1 mg orally once daily; can be taken with or without food. [1]
Efficacy. Kaufman 1998 demonstrated at 1 year: 48% vertex improvement vs 7% placebo by global photographic assessment; hair count increased by ~11% vs 3% placebo. Five-year extension: 90% maintained or improved vs baseline. Best response in vertex and mid-frontal scalp; bitemporal recession responds less predictably.[1][5]
Adverse effects. Sexual dysfunction is the most commonly cited concern:
- Decreased libido (~1.5%) — usually transient; resolves in 50-60% with continued therapy.
- Erectile dysfunction (~1.5%) — same pattern.
- Ejaculatory disorder (~1%).
- Gynaecomastia (~0.5%).
- Depression and suicidal ideation — rare; FDA has updated labelling (2011 update) to mention these. Stop the drug at the first sign of severe mood change.
- Post-finasteride syndrome (PFS) — persistent sexual, neurological, and psychiatric symptoms after stopping; reported and litigated but the causal link remains controversial in the literature; the FDA has not removed finasteride on this basis. [1]
PSA reduction. Finasteride reduces serum PSA by approximately 50%. Multiply the measured PSA by 2 in any man on finasteride or dutasteride to interpret prostate-cancer screening correctly. Some experts advise doubling + 10% additional correction after 2 years of use (Rossi formula).[1]
Pregnancy contraindication. Finasteride is Category X — absolutely contraindicated in women of childbearing potential. Pregnant women should not even handle crushed or broken tablets (DHT inhibition causes abnormal development of male fetal external genitalia). Safe in postmenopausal women (ineffective in FPHL unless PCOS-driven hyperandrogenism).[1]
Dutasteride — male only (off-label for AGA)
Mechanism. Dual 5-alpha-reductase type I AND II inhibitor; reduces serum DHT by >90% (more potent than finasteride). Long half-life (~5 weeks). Approved for BPH (0.5 mg/day Avodart) and used off-label for male AGA.[5]
Efficacy. Head-to-head with finasteride 1 mg (Rossi 2011, ARES trial), dutasteride produced superior vertex hair count at 12 and 24 weeks in AGA. Multiple meta-analyses confirm greater increase in total and terminal hair count vs finasteride, especially in vertex scalp.[5]
Adverse effects. Similar profile to finasteride; sexual dysfunction rates slightly higher in pooled analyses. Long half-life (5 weeks) — important for blood donation deferral and pregnancy planning (washout before trying to conceive). [1]
Special use cases. Men who fail or tolerate finasteride poorly; men with very aggressive early-onset disease; men with advanced Norwood patterns where maximum DHT suppression is desirable. Same pregnancy contraindication as finasteride. [1]
Spironolactone — female only
Mechanism. Androgen receptor antagonist (binds AR and prevents DHT activation) plus reduced testosterone production at higher doses. Off-label for FPHL but widely used.[7]
Dosing. 100-200 mg/day orally (some start at 50 mg and titrate up); often combined with an oral contraceptive containing an antiandrogenic progestin (drospirenone, dienogest) to provide contraception and synergistic antiandrogen effect. [1]
Adverse effects. Hyperkalaemia (monitor K⁺ at baseline, 1-2 months, then 6-monthly); menstrual irregularity; breast tenderness; gynaecomastia (rare); hypotension. Contraindicated in renal failure and Addison disease. [1]
NOT used in men (causes gynaecomastia and sexual dysfunction at the doses required). [1]
Other antiandrogens (female only)
- Bicalutamide 25-50 mg/day — pure AR antagonist; no steroid-like effects; promising in female FPHL but limited data.
- Flutamide 250-500 mg/day — older AR antagonist; hepatotoxicity concern; rarely used.
- Finasteride 2.5-5 mg/day — sometimes used off-label in postmenopausal women or PCOS-driven FPHL; lower response rate than in men.
- Oral contraceptives with antiandrogenic progestin — drospirenone, dienogest; modestly effective for FPHL with concurrent need for contraception. [1]
Hair transplantation
The surgical relocation of DHT-resistant occipital and lateral temporal follicles to balding recipient areas. Two main techniques, both with permanent results thanks to donor dominance.[3]
- FUT (follicular unit transplantation / strip): A strip of occipital scalp is excised, dissected into individual follicular units (1-4 hairs each), and transplanted. Leaves a linear scar; one procedure can move 2000-4000 grafts.
- FUE (follicular unit extraction): Individual follicular units are extracted one at a time using a 0.7-1.0 mm punch. No linear scar; more time-consuming; can move 2000-5000 grafts per session. [1]
Candidacy. Stable Norwood III-VI men with adequate donor density and realistic expectations. Women with Ludwig II-III thinning are less ideal (diffuse thinning reduces donor supply and recipient density). Smokers, diabetics with poor control, those with cicatricial or unstable disease, and those with body dysmorphic disorder are poor candidates. [1]
Pitfalls. "Shock loss" of adjacent native hair (10-20% of cases, usually temporary); donor depletion (irreversible); poor graft survival (smoking, sun, infection); wider strip scar than expected in FUT. [1]
Critical counselling point. Transplanted hairs are permanent (DHT-resistant occipital origin), but native (recipient-area) hairs continue to thin. All transplant recipients need ongoing medical therapy (minoxidil, +/- finasteride) to preserve the cosmetic result. [1]
Adjunctive therapies
- Low-level laser therapy (LLLT) — laser caps or combs (e.g. HairMax); mechanism thought to be mitochondrial photobiomodulation and increased follicular ATP; evidence variable but some RCTs show modest benefit. FDA-cleared for AGA.[3]
- Platelet-rich plasma (PRP) — autologous platelet concentrate injected into the scalp; growth factors (PDGF, TGF-β, VEGF, EGF) may prolong anagen and stimulate follicular activity. Evidence variable and technique not standardised; most useful as an adjunct.[3]
- Microneedling — 1.5 mm dermaroller or dermapen every 1-4 weeks; creates micro-wounds that release platelet-derived growth factors; enhances topical minoxidil penetration. Some evidence as an adjunct.[3]
- Ketoconazole 2% shampoo — has mild anti-inflammatory and anti-androgenic effect; useful adjunct; reduces scalp Malassezia colonisation.[3]
- Cosmetic camouflage — scalp micropigmentation (tattooing), hair fibres, wigs, weaves — psychologically important adjuncts.
- Micronutrient supplementation — correct deficiencies (iron, zinc, vitamin D) when present; no benefit from supplementation in replete individuals.[4]
Treatment memory — M.A.S.H.
MASH
Treatment algorithm by stage and sex
Men (Norwood II-IV):
- First-line — topical minoxidil 5% BD OR low-dose oral minoxidil 1.25-2.5 mg/day.
- Add finasteride 1 mg/day (vertex and mid-frontal disease); superior to monotherapy.
- Switch to dutasteride 0.5 mg/day if finasteride fails or patient prefers.
- Adjuncts — PRP, microneedling, LLLT, ketoconazole 2% shampoo.
- Transplant once disease stabilised (typically after 1-2 years of medical therapy). [1]
Men (Norwood V-VII):
- Combined finasteride + minoxidil (and consider dutasteride) is essential to preserve remaining native hair.
- Transplant often necessary; realistic counselling about donor supply. [1]
Women (Ludwig I-II, no hyperandrogenism):
- First-line — topical minoxidil 5% once-daily OR oral minoxidil 0.625-1.25 mg/day.
- Adjuncts — PRP, microneedling, LLLT, ketoconazole shampoo.
- Iron, vitamin D, zinc replaced if deficient. [1]
Women (Ludwig II-III, hyperandrogenism / PCOS):
- Topical or oral minoxidil PLUS
- Spironolactone 100-200 mg/day (with contraception) OR bicalutamide 25-50 mg/day.
- OC with antiandrogenic progestin (drospirenone) if contraception needed.
- Endocrinology referral for PCOS metabolic management. [1]
Transgender and gender-diverse individuals: Specialist-led care; AGA management is integrated into gender-affirming hormonal therapy (estrogen, antiandrogen). See Special Populations below.[9]
10. Subtypes and Pattern Variants
AGA is not one disease — it has multiple clinical phenotypes that reflect differing androgen sensitivity, distribution, and progress. Recognising the subtype changes prognosis and treatment intensity.[2][7]
Early-onset MPHL (under 25y)
Aggressive, androgen-driven
- Onset before age 25 — usually Hamilton-Norwood III or higher
- Stronger family history (maternal and paternal)
- More aggressive progression — reaches Norwood V-VII within 10-15 years
- **Cardiometabolic association** — insulin resistance, metabolic syndrome, dyslipidaemia, hypertension; counsel about cardiovascular risk
- Often warrants earlier, more aggressive therapy (finasteride or dutasteride + minoxidil from outset)
- Investigate for androgen-secreting tumour if very rapid and severe (rare)
Late-onset MPHL
Slower progression
- Onset after age 40 — usually vertex-predominant
- Slower progression — often stabilises at Norwood III-IV for years
- Lower cardiometabolic risk
- Mild disease may not require pharmacotherapy
- Monitor; treat if progression accelerates
DUPA (diffuse unpatterned alopecia)
Severe; biopsy-confirmed
- **Diffuse unpatterned alopecia** — male or female pattern; mimicker of telogen effluvium
- Bitemporal recession and vertex thinning occur but **do NOT follow the Norwood pattern**
- Donor density often also reduced — **poor transplant candidate**
- Biopsy confirms terminal-to-vellus ratio dropping below 4:1 with preserved ostia
- Aggressive medical therapy (finasteride + minoxidil) is the mainstay
- High androgen drive — investigate for endocrine cause if female
FPHL with PCOS
Hyperandrogenic FPHL
- 40-70% of women with PCOS show Ludwig I or higher
- Features — hirsutism, acne, irregular menses, central obesity
- Investigations — testosterone, SHBG, DHEA-S, LH/FSH ratio, pelvic US; fasting glucose, lipids (cardiometabolic risk)
- Management — spironolactone OR bicalutamide +/- metformin (insulin resistance) +/- minoxidil
- Endocrinology + gynaecology + dermatology input; PCOS is a lifelong metabolic condition
- Topical or oral minoxidil as adjunct
Postmenopausal FPHL
Multifactorial, declining estrogens
- Onset typically 50s-60s; Ludwig II-III common
- Contributing factors — declining estrogens, low SHBG, raised free androgen index, age-related follicular senescence
- Topical or oral minoxidil usually effective
- Spironolactone 50-100 mg/day may be used but monitor K⁺
- Avoid finasteride/ dutasteride (effective in postmenopausal women only at high doses; not FDA-approved)
- Investigate for other causes if rapid
FFA (frontal fibrosing alopecia)
Distinct — CICATRICIAL, not AGA
- **Cicatricial** — follicular ostia LOST in a band along the frontal hairline
- Postmenopausal women predominantly; some premenopausal cases
- Often with eyebrow loss, perifollicular erythema, facial papules
- Aetiology likely autoimmune + androgenic; association with facial sunscreen use is controversial
- Treatment — potent topical/intralesional steroid, hydroxychloroquine, doxycycline, 5-AR inhibitors; NOT AGA-specific treatments
- Critical to NOT mis-diagnose as AGA — biopsy shows lichenoid interface dermatitis around infundibulum
11. Complications
AGA itself causes no direct medical complications, but its treatment and its psychosocial impact generate a long list. The clinician must counsel patients before starting therapy and monitor proactively.[1][3][11]
Psychological
Psychiatric comorbidity
- **Depression and anxiety** — prevalence 25-40% in severe AGA; more in younger patients
- **Body dysmorphic disorder** — over-represented in patients seeking cosmetic procedures; screen with BDD questionnaire
- **Social withdrawal** and reduced quality of life
- **Workplace impact** — reduced confidence in appearance-driven professions (sales, performance, hospitality)
- **Suicidal ideation** in severe cases — flag and refer urgently
Drug adverse effects
Iatrogenic morbidity
- **Finasteride / dutasteride** — sexual dysfunction 1-5%; depression and suicidal ideation (rare but FDA-labelled); gynaecomastia (rare)
- **Topical minoxidil** — scalp irritation, contact dermatitis (propylene glycol), initial shedding
- **Oral minoxidil** — hypertrichosis (face/limbs), fluid retention, peripheral oedema, pericardial effusion (rare at low doses), tachycardia, hypotension
- **Spironolactone** — hyperkalaemia (monitor K⁺), menstrual irregularity, breast tenderness, hypotension
- **Bicalutamide / flutamide** — hepatotoxicity (especially flutamide; monitor LFTs)
Transplant complications
Surgical morbidity
- **Shock loss** — 10-20% of native hairs near the recipient site shed post-op; usually regrow in 3-6 months
- **Poor graft survival** — smoking, sun exposure, infection, dehydration of grafts
- **Donor depletion** — finite donor supply; over-harvesting can leave visible thinning at donor site
- **FUT scar** — linear occipital scar; wide in patients prone to keloid or with tension
- **FUE overharvest** — "moth-eaten" donor site if too many grafts taken
- **Unrealistic expectations** — patient satisfaction correlates with informed consent
Diagnostic pitfalls
Mis-diagnosis and missed diagnoses
- **Mis-diagnosing cicatricial alopecia as AGA** — treating with minoxidil and missing the window for immunomodulation
- **Prescribing finasteride to a woman of childbearing potential** — teratogenic (Category X); pregnancy test + contraception
- **Missing PCOS** — failing to investigate a young woman with Ludwig pattern + acne + hirsutism + irregular menses
- **Missing iron deficiency** — assuming AGA is the only cause when ferritin is 20 µg/L
- **Missing a drug-induced cause** — warfarin, retinoids, lithium, valproate, beta-blockers, cytotoxics
- **Missing secondary syphilis** — uncommon but still mis-attributed to AGA
Cardiometabolic
Comorbidity-driven morbidity
- Early-onset AGA in men associates with **insulin resistance, metabolic syndrome, type 2 diabetes**
- Higher rates of **hypertension, dyslipidaemia, ischaemic heart disease** in some cohorts
- Recent sex-stratified propensity-matched cohort data confirm the AGA-cardiovascular link (Husseinali 2026)
- Implication — dermatology consultation is an opportunity for cardiovascular risk assessment
- Female early-onset AGA with PCOS carries additional cardiometabolic risk via PCOS itself
12. Prognosis
AGA is progressive over decades if untreated. Treatment slows or halts progression and may regrow hair, but it does not cure — all medical therapies are lifelong and outcomes reverse within 3-6 months of stopping.[1][5]
Predictors of good response to medical therapy:
- Early treatment (within 5 years of perceived onset; before extensive follicular dropout).
- Younger age at initiation.
- Vertex and mid-frontal disease (responds better than bitemporal).
- Good adherence to daily therapy.
- Adequate donor supply if transplant is planned.
- No underlying untreated cause (iron, thyroid, androgen excess, drug). [1]
Predictors of poor response:
- Extensive disease (Norwood VI-VII).
- Long-standing miniaturisation (>10 years; many follicles may not be recoverable).
- Coexistent scarring alopecia.
- Non-adherence (the leading cause of treatment failure).
- Untreated hyperandrogenism.
- Donor depletion in transplant candidates. [1]
Transplanted hairs are permanent (donor dominance) but native (recipient-area) hairs continue to thin without medical therapy. This is why all transplant patients need ongoing minoxidil or finasteride to preserve the cosmetic result. [1]
Spontaneous stabilisation occurs in ~10-20% of men after Norwood IV-V; many will report "no further loss" for years, but most eventually continue. Counselling should set realistic expectations.[5]
13. Special Populations
AGA in special populations requires tailored counselling, alternative pharmacology, and active involvement of other specialties. [1]
Women of childbearing potential
Absolute rules:
- Finasteride and dutasteride are Category X — teratogenic. DHT inhibition in a male fetus causes ambiguous external genitalia. Pregnant women should not even handle crushed or broken tablets.
- Prescribing these drugs mandates a pregnancy test and highly effective contraception (long-acting reversible contraception or two forms of contraception).
- Washout period after stopping before attempting conception: finasteride ~1 month; dutasteride ~6 months (long half-life).[1]
Topical minoxidil in pregnancy: Category C; defer until postpartum. Minoxidil enters breast milk — avoid during lactation. [1]
Children and adolescents
- AGA in children is uncommon. If present, investigate:
- Hyperandrogenism — PCOS (peripubertal girls), late-onset congenital adrenal hyperplasia (CAH), androgen-secreting adrenal or gonadal tumour.
- Endocrine — thyroid dysfunction, pituitary disease.
- Nutritional — protein-energy malnutrition, zinc deficiency, vitamin D deficiency.
- Genetic — hypotrichosis simplex, ectodermal dysplasia, alopecia areata.
- Children cannot consent to finasteride/dutasteride/spironolactone; topical minoxidil is the only widely accepted pharmacotherapy (off-label in children).
- Hair transplant is inappropriate before adulthood because the donor area is not yet stable. [1]
Elderly patients
- Cardiovascular comorbidity is common; oral minoxidil requires lower starting dose (0.625 mg) and careful monitoring.
- Polypharmacy — check for interactions (antihypertensives may potentiate minoxidil hypotension; anticoagulants may worsen bruising from PRP).
- Transplant candidacy depends on donor supply, realistic expectations, and cardiovascular fitness for surgery. [1]
Transgender and gender-diverse individuals
AGA care is integrated into the gender-affirming pathway; this population requires special attention.[9]
- Trans women / transfeminine: Estrogen-based gender-affirming hormone therapy slows or reverses AGA; finasteride may be added (categorised with androgen-blocker therapy). Monitor for drug interactions with estradiol (no major issues).
- Trans men / transmasculine: Testosterone-based gender-affirming hormone therapy worsens AGA in those predisposed. Counsel before starting; consider prophylactic finasteride; topical or oral minoxidil.
- Non-binary individuals: Discuss goals; tailor therapy; integrate with hormonal goals.
- Mental-health input, peer support, and culturally competent care are essential. [1]
PCOS and metabolic syndrome
- 40-70% of women with PCOS have AGA; treat the AGA and the PCOS in parallel.
- PCOS-specific care — metformin or inositol for insulin resistance; lifestyle modification; combined oral contraceptive (with antiandrogenic progestin) for hirsutism + contraception + cycle regulation; consider letrozole for fertility.
- AGA-specific care — spironolactone or bicalutamide; topical/oral minoxidil.
- Coordinate with endocrinology and gynaecology. [1]
Cardiovascular and prostate disease
- Finasteride / dutasteride reduce serum PSA by ~50%; multiply measured PSA by ~2 for accurate cancer screening.
- Symptomatic BPH benefits from the same drugs (different dose).
- Recent large TriNetX cohort data (Spindler 2026) found no increased cardiovascular hazard with oral 5-AR inhibitors for AGA — reassuring for prescribers.[11]
- Minoxidil (oral) is a vasodilator — caution in heart failure, severe aortic stenosis, recent MI.
Cultural and religious considerations
- Hairstyle practices (hijab, wigs, weaves, braids) can hide or contribute to hair loss. Traction alopecia from religious head coverings or tight braiding is a recognised cause.
- Discuss cosmetic options (scalp micropigmentation, wigs, head coverings) where appropriate.
- Patient autonomy and dignity are paramount; religious head covering should not be discouraged if hair loss is present. [1]
14. Evidence Base — Key Studies
The AGA literature is extensive but mostly moderate-quality; the highest-tier evidence for each major therapy is summarised below. The examiner frequently asks about the pivotal trials.[1][3][5][7][10]
Kaufman 1998 — finasteride FDA approval
Pivotal RCT
- **Kaufman KD et al., J Am Acad Dermatol 1998** — two pivotal RCTs
- Men aged 18-41 with vertex AGA; 1 mg finasteride vs placebo
- **48%** vertex improvement vs **7%** placebo at 1 year (global photographic assessment)
- Hair count +11% vs +3% placebo
- 5-year extension: 90% maintained or improved vs baseline
- Established finasteride as the standard of care for male AGA
Lucky 2004 — finasteride in women
Women RCT
- **Lucky AW et al., J Am Acad Dermatol 2004**
- Postmenopausal women with FPHL; finasteride 1 mg vs placebo
- **No significant benefit** vs placebo in postmenopausal FPHL
- PCOS subgroup showed some benefit at higher doses (2.5-5 mg)
- Established finasteride as INEFFECTIVE in postmenopausal FPHL at standard dose
Rossi 2011 / ARES — dutasteride vs finasteride
Head-to-head RCT
- **Rossi A et al., 2011** — dutasteride vs finasteride head-to-head
- Dutasteride produced **superior vertex hair count** vs finasteride at 12 and 24 weeks
- Multiple meta-analyses confirm superior efficacy in vertex total and terminal hair counts
- Dutasteride is not FDA-approved for AGA but is widely used off-label
- Concern — slightly higher sexual adverse effects
Sinclair 2018 — oral minoxidil in women
Women oral minoxidil
- **Sinclair RD et al., 2018**
- Female FPHL given low-dose oral minoxidil (0.625-2.5 mg/day)
- Significant improvement in hair density; well tolerated
- Hypertrichosis is the most common adverse effect
- Established oral minoxidil as a viable off-label option for women
Gupta 2026 — oral minoxidil consensus
Expert consensus
- **Gupta AK et al., Expert Opin Pharmacother 2026**
- International consensus on low-dose oral minoxidil (LDOM) in male and female pattern hair loss
- Recommends LDOM 0.625-5 mg/day as a viable first-line option
- Practical dosing, monitoring, and adverse effect management
- Highlights hypertrichosis, fluid retention, and pericardial-effusion caveats
Adil & Godwin 2017 — AGA systematic review
JAMA Dermatol review
- **Adil A, Godwin M, JAMA Dermatol 2017** — comprehensive systematic review
- Established efficacy and safety of minoxidil, finasteride, and low-level laser therapy
- Variable evidence for PRP, microneedling, ketoconazole, nutritional supplements
- Confirmed combination therapy superior to monotherapy
- Standard reference for clinical guidelines
Recent large cohort data (2026):
- Spindler 2026 (J Am Acad Dermatol) — TriNetX propensity-matched cohort; no increased cardiovascular hazard with oral 5-AR inhibitors for AGA — supports the safety profile.[11]
- Husseinali 2026 (Dermatol Online J) — sex-stratified propensity-matched cohort confirming cardiometabolic comorbidity association with AGA.[12]
- He 2026 (J Am Acad Dermatol) — early AGA associated with diabetes mellitus and cardiovascular risk in cross-sectional data.[13]
- Li 2026 (BMC Public Health) — systematic review and meta-analysis of AGA risk factors.[8]
- Ramos-Rodriguez 2026 (Dermatol Ther) — narrative review of AGA in transgender and gender-diverse individuals.[9]
15. Exam Pearls and Clinical Reasoning
The fellowship examiner builds questions around pattern recognition, drug pharmacology, and clinical decision-making. The points below synthesise the high-yield material for both viva and SAQ. [1]
Five anti-AGA therapy memory cards — for viva
FADMS
Rapid Self-Test
A 28-year-old man presents with progressive bitemporal recession over 18 months. His maternal grandfather was 'completely bald by 30.' What is the most likely diagnosis and what investigations would you arrange?
Androgenetic alopecia (AGA) — male pattern (Hamilton-Norwood stage II-III). Family history is positive (maternal grandfather — reflects X-linked AR inheritance). Investigations are limited: clinical diagnosis and trichoscopy suffice. Trichoscopy will show hair diameter diversity >20% (anisotrichosis), peripilar sign, and preserved follicular ostia. Baseline ferritin and TSH are reasonable. PSA should be measured before starting finasteride if the patient is over 40. First-line management is finasteride 1 mg/day plus topical minoxidil 5%, combined.[1][2]
A 36-year-old woman with a widened midline part, mild hirsutism, irregular menses, and acne. Hormonal workup shows total testosterone 1.8 ng/mL (mildly elevated), SHBG low-normal, normal TSH. Pelvic ultrasound shows bilateral polycystic ovaries. What is the unifying diagnosis and how would you manage her alopecia?
Polycystic ovary syndrome (PCOS) with female pattern hair loss (Ludwig I-II) driven by hyperandrogenism. The alopecia is androgen-mediated. Management is multidisciplinary: (1) endocrinology/gynaecology for PCOS (lifestyle, metformin if insulin-resistant, combined oral contraceptive with antiandrogenic progestin); (2) dermatology for the alopecia — topical minoxidil 5% once-daily PLUS spironolactone 100-200 mg/day (with contraception). Monitor potassium, menstrual pattern, androgens. Avoid finasteride until postmenopausal.[7][8]
Why are occipital follicles not affected by AGA, and how does this allow hair transplantation to work?
Occipital and lateral-temporal follicles have lower local 5-alpha-reductase type II activity and a different androgen receptor co-regulator milieu than vertex follicles. They remain DHT-resistant even in advanced Norwood VII disease — preserving the donor "horseshoe" rim. When transplanted to a balding vertex, they retain this DHT-resistant behaviour in their new location — this is donor dominance. The transplanted hairs are permanent, but the surrounding native (recipient) hairs continue to thin, which is why all transplant patients need ongoing medical therapy (minoxidil, +/- finasteride).[3]
Compare the mechanisms and adverse effects of finasteride and dutasteride.
Both are 5-alpha-reductase inhibitors that reduce DHT production and slow AGA progression. Finasteride 1 mg/day selectively inhibits 5-AR type II, reducing serum DHT by ~70% and scalp DHT by ~60%. Dutasteride 0.5 mg/day is a dual inhibitor (Type I AND II), reducing serum DHT by >90% and scalp DHT more than finasteride. Dutasteride has a much longer half-life (~5 weeks vs ~6-8 hours), so washout takes longer. Adverse effect profiles are similar: decreased libido, ED, ejaculatory disorder (~1.5% each), gynaecomastia (~0.5%), depression and suicidal ideation (rare). Both are Category X in pregnancy and reduce PSA by approximately 50% — multiply the measured PSA by 2 for cancer screening. Dutasteride is not FDA-approved for AGA but is widely used off-label due to superior vertex efficacy.[1][5][11]
A 45-year-old man on finasteride 1 mg/day has a PSA of 1.0 ng/mL. How should this be interpreted?
Finasteride reduces serum PSA by approximately 50%, so the true PSA in this patient is approximately 2.0 ng/mL — clinically significant for prostate cancer screening. The standard correction is to double the measured PSA (or use the more accurate Rossi formula: multiply by 2, then add 10% additional correction after 2 years of use). Otherwise, finasteride would mask prostate cancer and delay diagnosis. This PSA correction should be communicated to all clinicians managing the patient.[1]
Why are finasteride and dutasteride absolutely contraindicated in women of childbearing potential?
Both drugs inhibit the conversion of testosterone to dihydrotestosterone (DHT), which is essential for the normal development of male fetal external genitalia. Pregnant women exposed to even crushed or broken tablets can deliver male infants with ambiguous or female-appearing genitalia (failure of the genital tubercle to masculinise, persistent urogenital sinus). The drugs are Category X — absolutely contraindicated in pregnancy and in women of childbearing potential who cannot guarantee contraception. Pregnant women should not even handle broken tablets. Washout periods are needed before attempting conception: ~1 month for finasteride, ~6 months for dutasteride (long half-life).[1]
One-Pager Summary
[1]- Definition: progressive androgen-dependent miniaturisation in genetically susceptible scalp follicles.
- Male (Hamilton-Norwood I-VII): bitemporal recession + vertex thinning → confluence; occipital preserved.
- Female (Ludwig I-III): diffuse central thinning; frontal hairline preserved; Olsen Christmas-tree variant.
- Pathophysiology: testosterone → 5-alpha-reductase (Type II in follicle) → DHT → AR in dermal papilla → TGF-β, DKK-1, PGD2 → shortened anagen + terminal-to-vellus conversion.
- Trichoscopy: hair diameter diversity >20% (anisotrichosis), peripilar sign, yellow dots, preserved follicular ostia.
- Investigations: ferritin, TSH, vitamin D, zinc; female hyperandrogenism panel; PSA baseline before 5-AR inhibitors; biopsy if uncertain.
- Treatments: minoxidil (topical/oral), finasteride 1 mg (men), dutasteride 0.5 mg (men, off-label), spironolactone 100-200 mg (women), transplant (FUE/FUT), PRP, microneedling, LLLT.
- Counselling point: AGA is progressive and lifelong — therapy halts loss, regrows modestly, and reverses within 3-6 months of stopping.
- Red flag: prescribing finasteride/dutasteride to a pregnant woman or woman of childbearing potential (Category X, teratogenic).
- Exam discriminator: AGA = non-scarring alopecia; follicular ostia PRESERVED. Cicatricial alopecia = LOST. [1]
Red Flags and Pitfalls
Exam application bank (NEET-PG / INICET)
One-line answer
Androgenetic alopecia (AGA) is the commonest cause of hair loss in both sexes, driven by dihydrotestosterone (DHT)-mediated progressive miniaturisation of genetically susceptible scalp hair follicles. Male pattern (Hamilton-Norwood): bitemporal recession + vertex thinning → confluence. Female pattern (Ludwig): diffuse central thinning with frontal hairline preserved; the Olsen "Christmas-tree" pattern adds a frontal accentuation. Trichoscopy: hair diameter diversity >20% (anisotrichosis), peripilar sign, yellow dots. Treatment: minoxidil (topical 5% or oral low-dose; works in both sexes); finasteride 1 mg/day (5-alpha-reductase type II inhibitor; male only; contraindicated in women of childbearing potential — teratogenic); dutasteride (dual 5-AR I+II inhibitor; more potent); spironolactone (antiandrogen; female); hair transplant (FUE/FUT). All treatments require lifelong commitment — w [1]
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard. [1]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes. [1]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change. [1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each. [1]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory. [1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Androgenetic alopecia.
[1]Quick-Reference Cards
[1] [1] [1] [1] [1]Practice MCQs
Which hormone is the central mediator of follicular miniaturisation in androgenetic alopecia, and where is it produced from testosterone?
Dihydrotestosterone (DHT) is the central mediator of follicular miniaturisation in AGA. It is produced from testosterone by 5-alpha-reductase, predominantly Type II in the hair follicle (Type I in skin/sebaceous glands/liver). DHT binds the androgen receptor in dermal papilla cells of genetically susceptible (vertex, mid-frontal, bitemporal) follicles, leading to shortened anagen and terminal-to-vellus conversion.[1][2]
Which trichoscopic feature is the single most useful for diagnosing androgenetic alopecia on bedside examination?
Hair diameter diversity exceeding 20% (anisotrichosis) — thick and thin hairs coexisting in a single region — is the diagnostic hallmark on trichoscopy. Preserved follicular ostia exclude cicatricial alopecia. Yellow dots, peripilar sign, and empty follicles are supportive but not diagnostic. In telogen effluvium, hair diameter remains uniform (under 10% variability), which distinguishes it from AGA.[1]
Why are finasteride and dutasteride absolutely contraindicated in pregnant women, and how should this translate into prescribing?
Both drugs inhibit 5-alpha-reductase, reducing dihydrotestosterone (DHT) production. DHT is essential for male fetal external genitalia development; suppression causes ambiguous genitalia in 46,XY fetuses. They are US FDA Category X — teratogenic. Prescribing mandates a pregnancy test and highly effective contraception (typically two forms or a long-acting reversible method). Pregnant women must not even handle broken tablets. Washout: ~1 month for finasteride, ~6 months for dutasteride (long half-life) before conception.[1]
References
- [1]Devjani S, Ezemma O, Kelley KJ, et al. Androgenetic Alopecia: Therapy Update Drugs, 2023.PMID 37166619
- [2]Oiwoh SO, Enitan AO, Adegbosin OT, et al. Androgenetic Alopecia: A Review Niger Postgrad Med J, 2024.PMID 38826011
- [3]Nestor MS, Ablon G, Gade A, et al. Treatment options for androgenetic alopecia: Efficacy, side effects, compliance, financial considerations, and ethics J Cosmet Dermatol, 2021.PMID 34741573
- [4]Wang R, Lin J, Liu Q, et al. Micronutrients and Androgenetic Alopecia: A Systematic Review Mol Nutr Food Res, 2024.PMID 39440586
- [5]Gupta AK, Talukder M, Williams G. Comparison of oral minoxidil, finasteride, and dutasteride for treating androgenetic alopecia J Dermatolog Treat, 2022.PMID 35920739
- [6]Gupta AK, Talukder M, Venkataraman M, et al. Minoxidil: a comprehensive review J Dermatolog Treat, 2022.PMID 34159872
- [7]Kearney CA, Brinks AL, Lawrence CN, et al. Androgenetic Alopecia in Women: A Narrative Review of Pathophysiology, Clinical Evaluation, and Treatments Am J Clin Dermatol, 2026.PMID 41714473
- [8]Li H, Li W, Zhang J, et al. Risk factors for androgenetic alopecia: a systematic review and meta-analysis BMC Public Health, 2026.PMID 41606541
- [9]Ramos-Rodriguez D, Sanchez-Baez D, Cabrera-Garcia P, et al. Characterization and Management of Androgenetic Alopecia in Transgender and Gender-Diverse Individuals: A Narrative Review Dermatol Ther (Heidelb), 2026.PMID 41920277
- [10]Gupta AK, Talukder M, Williams G, et al. Low-dose oral minoxidil (LDOM) and topical minoxidil: consensus recommendations for managing male and female pattern hair loss in hair transplant patients using a modified Delphi process Expert Opin Pharmacother, 2026.PMID 41782304
- [11]Spindler A, Maas D, Adler R, et al. No increased cardiovascular hazard with oral 5-alpha-reductase inhibitors in treatment of androgenetic alopecia: A TriNetX retrospective cohort study J Am Acad Dermatol, 2026.PMID 42036027
- [12]Husseinali M, Engineer N, Asempa O, et al. Cardiometabolic comorbidities associated with androgenetic alopecia: Findings from a sex-stratified, propensity-matched national cohort Dermatol Online J, 2026.PMID 42246337
- [13]He J, He M, Zhang D, et al. Early androgenetic alopecia as a possible indicator of diabetes mellitus and its link to cardiovascular risks: A cross-sectional study J Am Acad Dermatol, 2026.PMID 41785995