Dermatology · Medicine
Basal cell carcinoma
Also known as Basal cell carcinoma · BCC · Rodent ulcer · Basal cell epithelioma · Nevoid basal cell carcinoma syndrome (Gorlin)
Basal cell carcinoma (BCC) is the commonest human malignancy — a tumour of basal epidermal keratinocytes driven by aberrant Hedgehog signalling (somatic PTCH1 loss ~70%, SMO-activating mutations ~10%, TP53 ~50%) on a background of chronic ultraviolet damage. Clinically it presents as a pearly papule/nodule with a rolled border, arborising telangiectases and central ulceration (rodent ulcer), with superficial (eczema/psoriasis mimic), morpheaform (scar-like) and pigmented (melanoma mimic) variants. It rarely metastasises ( less than 0.1%) but is locally destructive, particularly at functionally/cosmetically critical sites (periocular, perinasal, periauricular — the 'H-zone'). Management is surgical — excision with 4-5 mm margins for low-risk, Mohs micrographic surgery for high-risk, recurrent or critical-site lesions — with topical imiquimod/PDT for low-risk superficial BCC, radiotherapy (contraindicated in Gorlin syndrome), and Hedgehog pathway inhibitors (vismodegib, sonidegib) for advanced disease. Fellowship-level assessment demands mastery of subtypes and their mimics, the Hedgehog pathway and PTCH1, dermoscopic criteria, Mohs indications, the high-risk feature set, Gorlin (nevoid BCC) syndrome, and the systemic options for locally advanced disease.
On this page & tools
Your progress
Saved locally on this device.
Exam tags
Red flags

Basal cell carcinoma at a glance
Definition & Classification
Basal cell carcinoma (BCC) is a malignant epidermal tumour arising from basal keratinocytes (or follicular outer-root-sheath cells), the commonest human malignancy.[1][4] It is locally invasive and destructive but rarely metastasises ( less than 0.1%); morbidity is driven by local invasion of critical facial structures (eye, nose, ear) and by the cumulative tumour burden in field-cancerised or syndromic patients. The disease is the prototype of pathway-defined oncogenesis (Hedgehog), and the disease in which targeted therapy (SMO inhibitors) first translated a developmental pathway into clinical benefit.
Classification — growth pattern drives behaviour and management:[2][4]
| Subtype | Frequency | Clinical clue | Recurrence risk |
|---|---|---|---|
| Nodular | ~60% | Pearly papule, rolled border, arborising telangiectases, central ulcer ("rodent ulcer"); face | Low–moderate |
| Superficial | ~15–30% | Flat scaly erythematous patch with thread-like pearly border; trunk and limbs | Low (topical candidates) |
| Morpheaform / sclerosing | ~5–10% | Ill-defined white scar-like indurated plaque; central face | HIGH — ill-defined margins, infiltrative strands |
| Pigmented | variable | Pearly nodule with dark brown/black pigment; mimics nodular melanoma | Depends on underlying pattern |
| Micronodular | ~5–10% | Clinically subtle; small (less than 0.15 mm) tumour nests on histology | HIGH — subclinical extension |
| Infiltrative | ~5–10% | Thin strands of basaloid cells; subtle clinical appearance, often on face | HIGH — wide subclinical spread |
| Basosquamous (metatypical) | ~2–5% | Mixed BCC/SCC; keratinisation within basaloid nests; most aggressive subtype | HIGH — metastatic potential |
| Fibroepithelioma of Pinkus | rare | Flesh-coloured pedunculated or sessile plaque on the lower back or thigh; histology shows branching cords of basaloid cells in fibrotic stroma | Low–moderate |

Low-risk BCC
- Primary nodular or superficial subtype
- Less than 2 cm (less than 1 cm on H-zone of face)
- Trunk or limbs — NOT H-zone of face
- Well-defined clinical margins
- Immunocompetent patient
- Treat with standard excision 4-5 mm or non-surgical (imiquimod / PDT) for superficial BCC
High-risk BCC
- Morpheaform, infiltrative, micronodular or basosquamous histology
- Above 2 cm (above 1 cm on H-zone of face)
- Located on H-zone (periocular, perinasal, nasal, periauricular, ear, scalp, temple)
- Recurrent tumour, prior radiotherapy at site
- Ill-defined clinical margins, immunosuppression
- Treat with Mohs micrographic surgery (highest cure rate)
Epidemiology & Risk Factors
BCC is the commonest cancer in humans — accounting for roughly one in two of all cancers in fair-skinned populations — and incidence continues to rise globally with an ageing, UV-exposed population and improved skin-cancer surveillance.[1][5] In Australia, the lifetime risk approaches 1 in 3, and in the United States the age-adjusted incidence is roughly 1,500–2,500 per 100,000 person-years. BCC affects men slightly more than women and the median age at diagnosis is around 65 years, although BCC is increasingly seen in patients under 50 — particularly women — reflecting cumulative UV exposure and indoor tanning.
Risk factors — host, environment and iatrogenic:[4]
- Fair skin / Fitzpatrick phototype I–II, red or blonde hair, blue or green eyes, freckling — the strongest host risk factor; phototype V–VI skin has approximately one tenth the incidence.
- Cumulative ultraviolet (UV) exposure — chronic, intermittent (childhood sunburn) and PUVA (8-methoxypsoralen + UVA for psoriasis) all raise BCC risk; UV-B drives the TP53 UV-signature mutation and chronic UV-A drives the PTCH1 footprint.
- Outdoor occupation / latitude — proximity to the equator, elevation, and outdoor work (farming, sailing) raise risk.
- Indoor tanning — tanning-bed exposure before age 35 raises BCC risk by approximately 70%.
- Personal / family history of skin cancer — a single prior BCC predicts a ~50% risk of a second BCC within five years.
- Chronic arsenic exposure — contaminated well water, industrial exposure (copper smelting, pesticides); produces multiple BCCs on sun-exposed and sun-protected sites.
- Ionising radiation — including radiotherapy for childhood tinea capitis, atomic-bomb survivors, and radiographers.
- Immunosuppression — solid-organ transplant recipients (3–10× BCC risk versus the general population; SCC predominates overall but BCC burden is high), chronic lymphocytic leukaemia, HIV, long-term azathioprine or ciclosporin.
- Inherited syndromes — Gorlin (nevoid BCC) syndrome (germline PTCH1), xeroderma pigmentosum (nucleotide-excision-repair defects), oculocutaneous albinism, Rombo syndrome, Bazex-Dupré-Christol syndrome, cartilage-hair hypoplasia, Muir-Torre (mismatch-repair; keratoacanthomas and sebaceous neoplasms).
- Chronic cutaneous ulcers, burn scars, vaccination scars and sites of trauma — rarely a substrate for BCC. [1]
Morbidity is local, not metastatic. Metastasis occurs in less than 0.1% of cases and is virtually confined to long-neglected, very large (>10 cm), morpheaform or basosquamous tumours; nodal disease is the most common presentation, followed by lung and bone.[5] However, local invasion of critical facial structures (periorbital invasion with exenteration, nasal alar destruction, auricular cartilage involvement) is the principal source of disfigurement, functional loss and operative morbidity.
Pathophysiology — The Hedgehog Pathway
BCC is the paradigm of pathway-defined oncogenesis — almost every tumour is driven by a single, druggable pathway:[4][5]
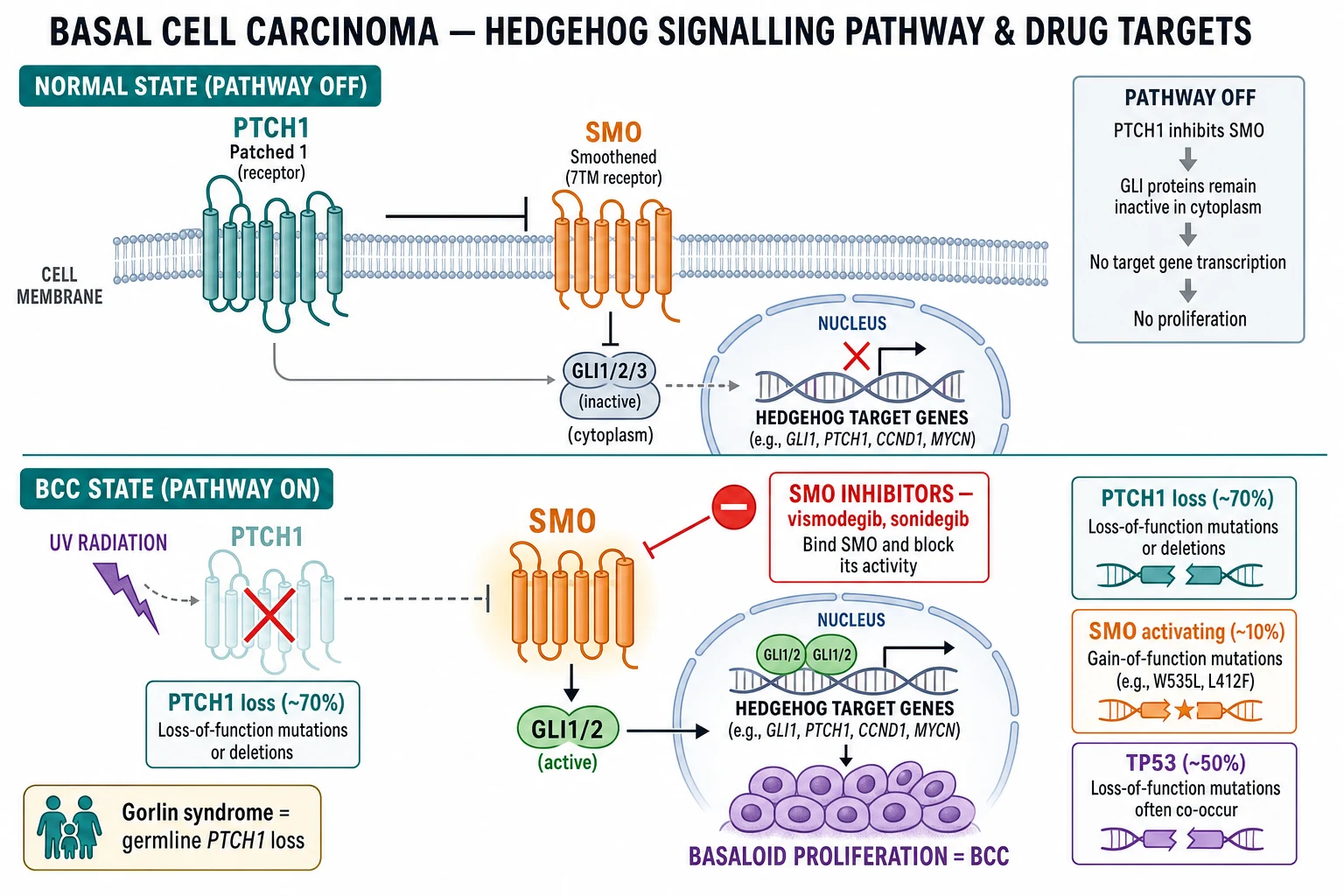
- Hedgehog signalling pathway is constitutively activated. Normally, the PTCH1 receptor (a 12-pass transmembrane protein) inhibits SMO (Smoothened) — a G-protein-coupled-like signalling protein. Hedgehog ligands (Sonic, Indian, Desert) bind PTCH1 and release this inhibition. In BCC, loss-of-function mutations of PTCH1 (~70% of tumours) or activating mutations of SMO (~10%) release SMO from inhibition independently of ligand.
- Activated SMO drives the GLI family of zinc-finger transcription factors (GLI1, GLI2) to the nucleus, switching on target genes that drive basaloid proliferation — the molecular basis of BCC. GLI1 mRNA is the most consistently overexpressed transcript in BCC and is the molecular signature used in research diagnostics.
- TP53 mutations in ~50% of BCCs, with the UV-signature C→T or CC→TT "punch" mutation at dipyrimidine sites — a footprint of UV-B damage and a founding lesion of UV-driven skin carcinogenesis.
- Secondary drivers — mutations in MYCN, CDKN2A, NOTCH1/2, PTPN14, KMT2D and TP63 modulate tumour behaviour, especially in aggressive subtypes; MMPs and PDGFRα signal sustain the desmoplastic stromal response of morpheaform BCC.
- Field cancerisation — chronic UV exposure produces multiple contiguous keratinocyte clones with TP53 / PTCH1 mutations; clinically normal but biologically altered skin explains the high rate of new BCCs adjacent to or remote from the index lesion.
- The Hedgehog pathway is the therapeutic target of the SMO inhibitors vismodegib and sonidegib for locally advanced / unresectable or metastatic BCC, and for tumour burden reduction in Gorlin syndrome.[5]
Hedgehog pathway in BCC — PEGS
PEGS
≈ 70% of BCCs; ligand-independent activation of SMO; germline in Gorlin syndrome
TP53 UV-signature mutation in ~50%; dominant somatic event in field cancerisation
GLI1 overexpression is the molecular signature; target of vismodegib/sonidegib upstream at SMO
≈ 10% of BCCs; ligand-independent activation; same downstream effect
Somatic vs germline: most BCCs are sporadic, somatic PTCH1 loss on a background of cumulative UV. A small but important minority is germline PTCH1 (Gorlin syndrome) or germline SUFU — with hundreds of BCCs from childhood. The pathway is identical, but the germline mutation shifts the burden from sporadic tumour to autosomal-dominant multiple tumour syndrome. [1]
Clinical Presentation
The clinical picture of BCC is dominated by subtype, site and chronicity. The classic patterns are: [1]
Nodular BCC (the commonest form, ~60%) — a pearly or translucent papule or nodule with a rolled, well-defined border, prominent arborising telangiectases crossing the surface, and a central crust or ulcer ("rodent ulcer", Jacob's ulcer on the eyelid); usually on the face (nose, nasolabial fold, cheek, lower eyelid, ear, temple) and slow-growing over months to years.[2] Bleeds with minor trauma.
Superficial BCC (~15–30%) — a flat, scaly, well-demarcated erythematous patch with a thread-like raised pearly border and focal erosions; trunk and limbs; mimics eczema, psoriasis or Bowen's disease — but does not respond to topical steroids and the border is sharper than eczema. [1]
Morpheaform / sclerosing BCC (~5–10%) — an ill-defined, white or skin-coloured scar-like indurated plaque with subtle surface telangiectases; commonly on the central face; clinically subtle but histologically infiltrative — it is the highest-recurrence clinical subtype and is frequently under-treated because the margins are not appreciated clinically. [1]
Pigmented BCC — a pearly nodule with dark brown or black pigmentation ± telangiectases; mimics nodular melanoma; dermoscopy distinguishes them (see Dermoscopy below). [1]
Basosquamous (metatypical) BCC — features of both BCC and SCC (keratinisation, intercellular bridges); tends to ulcerate early, behaves aggressively; has the highest metastatic potential of all BCC subtypes. [1]
Micronodular and infiltrative BCC — clinically subtle and frequently under-recognised; histology shows small (less than 0.15 mm) tumour nests or thin strands with little peripheral palisading — both confer high recurrence and mandate Mohs. [1]
High-risk sites (the 'H-zone'): periocular, perinasal / nasal ala, periauricular, ear, scalp, temple — define the central "mask area" of the face where recurrence rates after standard excision are 3–5 times higher than on the trunk/limbs.[1]
Symptoms and natural history — BCC is classically asymptomatic or non-tender, slow-growing over months to years, occasionally bleeds with minor trauma (a frequent first clue in elderly men), and rarely causes pain unless perineural involvement is present (a feature of morpheaform/infiltrative subtypes in the H-zone — a red flag for incomplete excision and recurrence). [1]
Differential Diagnosis
| Mimic | Distinguishing features |
|---|---|
| Squamous cell carcinoma | Hyperkeratotic, indurated, faster growth; dermoscopy: glomerular / polymorphous vessels, white circles around hair follicles |
| Pigmented / amelanotic melanoma | Variable pigment, ABCDE, ulceration; dermoscopy: atypical network, blue-white veil, irregular streaks, regression |
| Seborrhoeic keratosis | "Stuck-on", milia-like cysts, comedo-like openings; dermoscopy: cerebriform pattern |
| Actinic keratosis / Bowen's disease (SCC in situ) | Rough/scaly; dermoscopy of Bowen's: glomerular vessels in clusters |
| Intradermal naevus | Soft, long-standing, flesh-coloured; telangiectases may mimic BCC but no ulceration |
| Sebaceous hyperplasia | Yellowish, lobulated papule with central umbilicated telangiectasia (vs surface arborising in BCC); elderly face |
| Molluscum contagiosum | Umbilicated, central core, viral |
| Trichoepithelioma / trichoblastoma | Benign adnexal; histology: papillary mesenchymal bodies, stromal fibroblast aggregates |
| Microcystic adnexal carcinoma | Deeply infiltrative sweat-gland tumour of the central face; histology |
| Nummular eczema / psoriasis | Superficial BCC mimic — dermoscopy & biopsy |
Dermoscopy

Dermoscopy is the bedside diagnostic workhorse — in experienced hands the diagnostic accuracy exceeds 95% for nodular BCC, ~85% for superficial BCC, and the technique allows mapping of clinical margins before biopsy or surgery.[3]
Classic dermoscopic features (the presence of one is highly suggestive):[3]
- Arborising (tree-like) telangiectases — sharply in focus, branching, large-calibre vessels crossing the lesion; the single most specific sign.
- Blue-grey ovoid nests — large, well-circumscribed bluish-grey ovals corresponding to tumour nests in the dermis.
- Multiple blue-grey globules — smaller, round, well-circumscribed.
- Leaf-like areas — maple-leaf-like peripheral pigmentation corresponding to pigmented tumour nests; characteristic of pigmented BCC.
- Spoke-wheel areas — radial pigmented projections surrounding a central hub; highly specific for BCC.
- Large blue-grey structures / blue-white veil-like areas — overlap with pigmented BCC and melanoma; absence of a true pigment network and presence of arborising vessels favour BCC.
- Ulceration — non-pigmented areas of epidermal loss with adherent crust; a high-yield feature.
- Shiny white-red structureless areas — bright white-red zones (collagen and tumour stroma).
- Short fine telangiectases (superficial BCC variant) — fine, focused surface vessels. [1]
Subtype-specific patterns — nodular BCC: arborising telangiectases + blue-grey ovoid nests + ulceration. Superficial BCC: shiny white-red structureless zones + erosions + short fine telangiectases + small surface scale — overlap with Bowen's disease and psoriasis is the principal pitfall; lack of glomerular vessels helps exclude SCC in situ. Pigmented BCC: combined pigment pattern plus the BCC-specific vascular and ulceration features (separation from melanoma rests on presence of arborising vessels, leaf-like areas and spoke-wheel areas rather than atypical network and blue-white veil). Morpheaform BCC: scarce specific features — fibrosis, white structureless areas, minimal vessels; dermoscopy under-recognises the margins, and Mohs is justified by histology rather than dermoscopy. [1]
Histopathology

The histology is the diagnostic gold standard and drives the risk classification.[4][5]
- Basaloid tumour islands/nests of small hyperchromatic cells with scant cytoplasm arising from the epidermis or follicular outer-root sheath and invading the dermis.
- Peripheral palisading — columnar nuclei aligned at the periphery of each tumour island ("fence posts") — the diagnostic architectural feature.
- Retraction artefact (clefting) — a cleft between tumour island and surrounding stroma, containing basophilic stromal mucin — a fixation artefact that helps the pathologist.
- Stromal–epithelial interaction — fibromyxoid or mucinous stroma around tumour nests; a desmoplastic stroma characterises morpheaform BCC.
- Mitotic figures and apoptotic bodies are common, but bizarre pleomorphism is unusual (distinguishing BCC from SCC). [1]
Aggressive-subtype histology — the basis of the high-risk BCC label:[4]
- Infiltrative BCC — narrow, angulated strands and cords of basaloid cells; little peripheral palisading.
- Micronodular BCC — multiple small (less than 0.15 mm) tumour nests dispersed in a fibrous stroma.
- Morpheaform / sclerosing BCC — small compressed nests and cords within dense desmoplastic stroma — the most clinically deceptive subtype.
- Basosquamous (metatypical) BCC — keratinisation, intercellular bridges and SCC-like architecture within basaloid nests; behave like SCC with metastatic potential. [1]
Immunohistochemistry — BerEP4 (positive in BCC, negative in SCC and trichoepithelioma), EMA (negative in BCC, often positive in SCC), Bcl-2 (diffuse positivity in BCC) and CD10 (stromal in BCC) help distinguish BCC from SCC and from basal-cell–origin benign mimics in difficult cases. PHLDA1 and CK20 (Merkel cells) characterise trichoepithelioma (preserved Merkel cells, PHLDA1 positive) versus BCC (loss of Merkel cells, PHLDA1 negative). [1]
Perineural invasion (PNI) — tumour tracking along small nerves; a high-risk feature requiring Mohs ± adjuvant radiotherapy. [1]
Clinical & Bedside Assessment
- Full skin examination of every patient with a suspect lesion — BCC patients have a high rate of second primaries.
- Dermoscopy of every suspect lesion; measure and photograph the lesion before biopsy.
- Map the lesion relative to the H-zone (periocular, perinasal, periauricular, ear, scalp, temple) — drives Mohs decision-making.
- Palpate for induration, tethering, fixation, regional lymphadenopathy (BCC nodal disease is rare but must be sought).
- Assess for high-risk features (see below) at the bedside.
- Take a focused history — duration, growth rate, prior treatment, immunosuppression, family/syndromic features, prior radiotherapy at the site, occupational exposures. [1]
Investigations
- Biopsy is the diagnostic standard. Shave biopsy (into mid-reticular dermis) suffices for most nodular/superficial BCC on the trunk/limbs. Punch biopsy (2–4 mm) is preferred for H-zone or morpheaform lesions to capture deep infiltration, and excisional biopsy may be both diagnostic and therapeutic for small primary lesions. The histologic subtype drives management — partial biopsies may under-call morpheaform or infiltrative foci.[2]
- Imaging — CT/MRI is reserved for advanced disease with deep tissue invasion, perineural involvement, or for staging locally advanced BCC considered for Hedgehog inhibitor therapy; nodal ultrasound for clinically involved nodes.
- Genetic testing — germline PTCH1 / SUFU sequencing in suspected Gorlin syndrome (multiple childhood-onset BCCs, jaw keratocysts, palmar/plantar pits, falx calcification, family history).
- Gene-expression profiling (e.g. 40-GEP, Castle Biosciences) — supports clinical decision for an ambiguous periocular lesion with conflicting histology.
High-Risk Features & Staging
BCC rarely requires formal AJCC TNM staging (metastatic risk less than 0.1%), but high-risk features drive Mohs and recurrence decisions and are the cornerstone of risk-stratified care.[1][4]
Consensus high-risk clinical features: [1]
- High-risk site (H-zone): central face, periocular, perinasal, nasal ala, periauricular, ear, scalp, temple; periorbital, vermilion border and genitalia are included in many guidelines.
- Size: >2 cm on the trunk/limbs; >1 cm on the face/H-zone (low-risk thresholds: less than 2 cm trunk; less than 1 cm face).
- Aggressive histology: morpheaform/sclerosing, infiltrative, micronodular, basosquamous.
- Recurrent tumour or prior incomplete excision.
- Immunosuppression — transplant recipients, leukaemia, HIV, long-term immunosuppressants.
- Prior radiotherapy at the site — radiated skin has altered lymphatic drainage and wound-healing.
- Ill-defined clinical margins — morpheaform and infiltrative subtypes often have invisible extension.
- Perineural invasion — clinical (paraesthesia, formication, facial nerve palsy) or histologic.
- Patient factors — young age at first BCC (greater lifetime burden), inability to tolerate surgery, comorbidities precluding excision. [1]
AJCC 8th edition staging — T1 = BCC less than 2 cm with less than 2 high-risk features; T2 = BCC less than 2 cm with ≥2 high-risk features OR BCC ≥2 cm with less than 2 high-risk features; T3 = BCC ≥4 cm OR minor bone erosion OR perineural invasion; T4 = BCC with cortical bone / marrow / skull-base invasion. Stages I–II are localised disease; stages III–IV are locally advanced; metastatic (distant nodal/bone/lung) is stage IV — rare but the indication for Hedgehog inhibitor or immunotherapy. [1]
Management — Surgery

Surgery is first-line — definitive in >95% of primary BCCs.[1][2]
- Standard excision with clinical margins of 4-5 mm for low-risk nodular BCC on the trunk/limbs (extend to 6–10 mm for larger or less-defined lesions). Histologic examination confirms complete excision; expected 5-year cure rates exceed 95%.
- Mohs micrographic surgery (gold standard for high-risk BCC) for: H-zone (central face, periocular, perinasal, ear, periauricular, scalp, temple); morpheaform, infiltrative, micronodular, basosquamous subtypes; recurrent BCC; >2 cm lesions; immunosuppressed patients; ill-defined clinical margins; perineural invasion; and young patients in whom tissue conservation is critical (eyelid, digit, genital). Mohs reports the highest 5-year cure rates for high-risk BCC (≈ 97–99%), with maximal tissue conservation. The procedure maps 100% of the surgical margin via horizontal frozen sections; tumour-positive areas are re-excised layer by layer until clear.
- Curettage & electrodessication (electrodesiccation and curettage, EDC) for selected low-risk nodular BCC (less than 1 cm on trunk/limbs) in low-risk patients — three cycles of curettage followed by electrocautery — accepting a recurrence rate of 5–15% and inferior cosmetic outcome; not used on terminal-hair-bearing areas (BCC may track down the follicle) or on the H-zone.
- Positive / involved margins — re-excision (or Mohs if H-zone / high-risk histology) is standard. Adjuvant radiotherapy is an alternative where re-excision is impractical.
- Sentinel lymph node biopsy is not routinely indicated for BCC; reserved for advanced disease with nodal suspicion. [1]
Management — Topical, Photodynamic & Physical Therapies
For low-risk superficial BCC (and selected small nodular BCC in low-risk patients):[1]
- Topical imiquimod 5% cream — five applications per week for six weeks; immunomodulator (TLR7 agonist); clearance rates 75–85% at 5 years for superficial BCC. Inflammatory reaction is expected; limiting in fair-skinned patients. Not first-line for nodular, infiltrative or H-zone disease.
- Topical 5-fluorouracil (5-FU) 5% cream — twice daily for 2–4 weeks; clearance rates ~60–70% for superficial BCC; similar limits.
- Photodynamic therapy (PDT) — topical aminolaevulinic acid (ALA) or methyl aminolaevulinate (MAL) with red-light activation; clearance ~75–85% for superficial BCC, useful for multiple superficial lesions and large field disease in cosmetically sensitive sites; cosmetic outcome often excellent.
- Cryotherapy — single or double freeze-thaw cycle; effective for small superficial BCC in low-risk sites; inferior cosmetic outcome (hypopigmentation).
- Combination / sequential therapy — PDT + imiquimod or curettage + imiquimod improves clearance in comparative trials; field therapy of actinic damage adds value in field-cancerised patients. [1]
Management — Radiotherapy
- Primary radiotherapy — for patients unfit for, or refusing, surgery, particularly in elderly patients with large or inoperable primary tumours on the face, where surgery would be mutilating.[2]
- Adjuvant radiotherapy — for high-risk, incompletely excised BCC where re-excision is not feasible; long-term data support 5-year local control of ~90% when combined with thorough surgical debulking.
- Contraindications — Gorlin (nevoid BCC) syndrome and other DNA-repair disorders (xeroderma pigmentosum) — ionising radiation induces new BCCs along field portals.[5] Young patients (less than 60) — lifetime second-cancer risk after a radiotherapy field is unfavourable. Recurrent disease after prior radiotherapy — re-irradiation limited by cumulative dose.
- Modalities — orthovoltage, megavoltage electrons (preferred for superficial lesions; skin-sparing), or interstitial brachytherapy (selected periocular/nasal lesions).
Management — Advanced / Systemic Disease
Hedgehog pathway (SMO) inhibitors are the first systemic option for locally advanced, unresectable or metastatic BCC:[5]
- Vismodegib (Erivedge®) — 150 mg orally once daily; pivotal ERIVANCE / STEVIE trials show objective response rates of ~30–45% in locally advanced disease and ~15–30% in metastatic disease with median duration of response ~10–16 months. Common adverse effects (50–80%): muscle spasm/cramps, alopecia, dysgeusia (taste loss), ageusia, weight loss, fatigue, diarrhoea, nausea; ~20% discontinue for tolerability.
- Sonidegib (Odomzo®) — 200 mg orally once daily; BOLT trial demonstrated durable responses in locally advanced BCC; similar adverse-effect profile (muscle spasm, alopecia, dysgeusia, elevated CK, nausea); teratogenic.
- Mechanism and resistance — block SMO, prevent GLI activation. Resistance mechanisms: acquired SMO mutations (D473H, W281C), GLI2 amplification, upregulation of parallel pathways; ~20% acquire resistance at 1 year. Intermittent dosing schedules improve tolerability with retained efficacy. [1]
Immunotherapy — anti-PD-1: [1]
- Cemiplimab (Libtayo®) — FDA-/EMA-approved (2021) for locally advanced or metastatic BCC progressing on, or intolerant of, a Hedgehog pathway inhibitor; objective response rate ~21–32% (per pivotal EMPOWER-BCC 1/2 trials). Trials in first-line advanced BCC versus Hedgehog inhibitor are ongoing.
- Pembrolizumab — promising activity in advanced BCC; combined with vismodegib under study. [1]
Tumour reduction pre-surgery — neoadjuvant vismodegib for locally advanced BCC can downstage large or H-zone tumours, enabling a less mutilating excision or conversion to Mohs-feasible surgery; durable relapse after stopping HHI is a known limitation. [1]
Special Populations
- Gorlin (nevoid basal cell carcinoma) syndrome (NBCCS) — autosomal-dominant germline PTCH1 mutation (chromosome 9q22.3) — or rarely SUFU — produces hundreds of BCCs from childhood/adolescence; associated odontogenic keratocysts of the jaw (OKCs), palmar and plantar pits, bifid or fused ribs, calcification of the falx cerebri, macrocephaly with frontal bossing, medulloblastoma (desmoplastic subtype) risk in early childhood, and ovarian/cardiac fibromas. Diagnosis is clinical (Evans criteria); confirm with PTCH1 sequencing. Management: aggressive sun protection from infancy, field therapy of actinic damage, excision of symptomatic BCCs, avoid radiotherapy, consider Hedgehog inhibitor (vismodegib) for tumour burden reduction; MDT (dermatology / maxillofacial / genetics).[5]
Gorlin (NBCCS) — mnemonic
GORLIN
Autosomal dominant; hundreds of BCCs from childhood; Hedghog pathway constitutively active
Keratocystic odontogenic tumours (KCOT); mandibular cysts; require curettage ± marsupialisation
Bifid or fused ribs — the skeletal signature
Lamellar calcification on skull X-ray / CT
Childhood medulloblastoma (desmoplastic subtype); consider annual review until age 7
Palmar and plantar pits — tiny depressions; classic minor criterion
- Xeroderma pigmentosum (XP) — autosomal-recessive defects in nucleotide-excision repair; markedly elevated risk of BCC, SCC and melanoma from childhood; aggressive sun avoidance, isotretinoin chemoprevention, intensive surveillance.
- Oculocutaneous albinism — lack of melanin photoprotection; BCC/SCC in early adulthood; same surveillance framework.
- Immunosuppressed (solid-organ transplant) — BCC is the commonest cutaneous malignancy in transplant recipients in some series; risk rises with cumulative immunosuppression and duration; post-transplant switching to mTOR inhibitors (sirolimus, everolimus) modestly reduces skin-cancer burden alongside sunscreen and field therapy.
- Pregnancy — BCC during pregnancy is uncommon but should be excised under local anaesthesia; topical imiquimod and PDT are CONTRAINDICATED; radiotherapy avoided. [1]
Prognosis & Surveillance
- Excellent prognosis for low-risk BCC — surgical cure >95% at 5 years; Mohs achieves 99% 5-year cure for high-risk BCC.[1]
- Local recurrence is the principal concern, with risk highest in H-zone, morpheaform, infiltrative, micronodular, basosquamous, recurrent, >2 cm, immunosuppressed and incompletely excised lesions.
- Metastasis is rare ( less than 0.1%); lymph node > lung > bone; basosquamous is the subtype with the highest metastatic potential; prognosis for metastatic disease remains guarded despite SMO inhibitors and cemiplimab.
- Lifelong surveillance — patients with a single BCC have approximately a 50% risk of a second BCC within 5 years. Follow-up: full skin examination annually (more often if syndromic or immunosuppressed); sun protection and field therapy of actinic damage (imiquimod, 5-FU, PDT, cryotherapy); education on self-examination with urgent re-presentation for bleeding, ulceration, growth or new lesions.
Evidence, Guidelines & Regional Differences
- Guidelines — European interdisciplinary consensus-based guideline 2023 (Peris et al.) is the most current multiprofessional guideline and integrates Hedgehog inhibitor indications.[1] The NCCN BCC guideline (North America), AAD (American Academy of Dermatology) and BAD (British Association of Dermatologists) guidelines anchor North American and UK practice. Cancer Council Australia / Australian Cancer Network guidelines address the very high Australian incidence.
- Controversies and emerging evidence —
- Mohs vs standard excision for high-risk primary BCC — Mohs is guideline-preferred, but comparative data are limited; trials have not shown a large survival difference but show lower recurrence for H-zone and aggressive subtypes.
- Optimal duration and dosing of Hedgehog inhibitors — intermittent dosing (e.g. 12 weeks on / 8 weeks off) and lower doses are explored for improved tolerability.
- Cemiplimab positioning — current use is second-line (after HHI failure); first-line trials are ongoing.
- Gene-expression profiling (40-GEP) — for ambiguous periocular lesions.
- Topical Hedgehog inhibitors (patidegib) under study for field therapy in Gorlin syndrome.
- Chemoprevention — oral nicotinamide 500 mg twice daily lowers BCC and SCC incidence by ~20% in high-risk immunocompetent adults (ONTRAC trial); no benefit in transplant recipients.
Prevention
- Sun protection — broad-spectrum SPF 30+ sunscreen (UVA + UVB), UFP-rated clothing, wide-brimmed hat, sunglasses, shade from 10 a.m. to 4 p.m.; avoidance of indoor tanning.[4]
- Field therapy of actinic damage — imiquimod, 5-FU, PDT or cryotherapy to sun-damaged skin; reduce the burden of subsequent keratinocyte cancers.
- Gorlin / XP / albinism — intensive early surveillance (often 3–6-monthly full skin examination), strict radiation avoidance, and consider HHI for tumour burden; MDT input essential.
- Chemoprevention — nicotinamide 500 mg twice daily in high-risk immunocompetent adults; evidence lacking in transplant recipients.
- Self-examination education — patients taught the ABCDE for melanoma and the pearly / scaly / bleeding / non-healing features for BCC, with urgent re-presentation thresholds.
Exam Pearls
[1]Exam application bank (NEET-PG / INICET)
One-line answer
Basal cell carcinoma (BCC) is the commonest human malignancy — a tumour of basal epidermal keratinocytes driven by aberrant Hedgehog signalling (somatic PTCH1 loss ~70%, SMO-activating mutations ~10%, TP53 ~50%) on a background of chronic ultraviolet damage. Clinically it presents as a pearly papule/nodule with a rolled border, arborising telangiectases and central ulceration (rodent ulcer), with superficial (eczema/psoriasis mimic), morpheaform (scar-like) and pigmented (melanoma mimic) variants. It rarely metastasises ( less than 0.1%) but is locally destructive, particularly at functionally/cosmetically critical sites (periocular, perinasal, periauricular — the 'H-zone'). Management is surgical — excision with 4-5 mm margins for low-risk, Mohs micrographic surgery for high-risk, recurrent or critical-site lesions — with topical imiquimod/PDT for low-risk superficial BCC, radiotherapy
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard. [1]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes. [1]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change. [1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each. [1]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory. [1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Basal cell carcinoma.
[1]Clinical Pearls — Subtypes and Mimics
[1] [1]References
- [1]Peris K, Fargnoli MC, Kaufmann R, et al. European consensus-based interdisciplinary guideline for diagnosis and treatment of basal cell carcinoma-update 2023 Eur J Cancer, 2023.PMID 37604067
- [2]Heath MS, Bar A. Basal Cell Carcinoma Dermatol Clin, 2023.PMID 36410973
- [3]Reiter O, Mimouni I, Dusza S, et al. Dermoscopic features of basal cell carcinoma and its subtypes: A systematic review J Am Acad Dermatol, 2021.PMID 31706938
- [4]Kim DP, Kus KJB, Ruiz E. Basal Cell Carcinoma Review Hematol Oncol Clin North Am, 2019.PMID 30497670
- [5]Dika E, Scarfì F, Ferracin M, et al. Basal Cell Carcinoma: A Comprehensive Review Int J Mol Sci, 2020.PMID 32759706