Dermatology · Medicine
Drug eruptions
Also known as Drug eruptions · Cutaneous adverse drug reactions · cADR · Drug rash
Cutaneous adverse drug reactions (cADR) range from the common morbilliform exanthem (90%) to life-threatening severe cutaneous adverse reactions (SCAR) including DRESS/DIHS, AGEP, and SJS/TEN. Each pattern has a characteristic latency (urticaria minutes-hours; morbilliform 7-14 days; DRESS 2-8 weeks; AGEP less than 4 days; fixed drug eruption hours-days), culprit drug profile, and management pathway. Fellowship-level assessment demands mastery of the full cADR spectrum, the Type IV hypersensitivity subtypes that underpin delayed reactions, the RegiSCAR criteria for DRESS, the AGEP validation score, the distinguishing features between DRESS/AGEP/SJS-TEN, culprit drug lists (allopurinol, sulfonamides, anticonvulsants, aminopenicillins, minocycline, NSAIDs), and the severity-driven management from simple drug withdrawal to systemic immunosuppression.
On this page & tools
Your progress
Saved locally on this device.
Exam tags
Red flags
Definition & Classification
Cutaneous adverse drug reactions (cADR) [1]
[1]Quick numbers for the examiner
are skin manifestations of an adverse reaction to a systemically administered drug. They range from common, benign reactions to life-threatening severe cutaneous adverse reactions (SCAR):[3][9]
| Pattern | Latency | Key drugs | Severity |
|---|---|---|---|
| Morbilliform exanthem (~90%) | 7-14 days | β-lactams, sulfonamides, allopurinol, anticonvulsants | Mild |
| Urticaria / anaphylaxis | Minutes-hours | β-lactams, NSAIDs, contrast, opiates | Mild-severe |
| DRESS / DIHS | 2-8 weeks | Allopurinol, sulfonamides, anticonvulsants, minocycline, dapsone | Severe (mortality ~10%) |
| AGEP | ** less than 4 days** | Aminopenicillins, cephalosporins, pristinamycin, terbinafine, diltiazem | Severe (mortality ~5%) |
| SJS / TEN | 1-8 weeks | Allopurinol, anticonvulsants, sulfonamides, nevirapine, oxicam NSAIDs | Life-threatening |
| Fixed drug eruption | Hours-days | NSAIDs, paracetamol, sulfonamides, tetracyclines, phenolphthalein | Mild-moderate |
| Photosensitivity | Hours-days | Fluoroquinolones, tetracyclines, thiazides, amiodarone, NSAIDs | Mild-moderate |
| Drug-induced vasculitis | 7-21 days | Levamisole (cocaine), hydralazine, propylthiouracil, minocycline | Moderate-severe |
| Drug-induced pigmentation | Months-years | Minocycline, amiodarone, hydroxychloroquine, heavy metals, clofazimine | Mild |
| Acneiform eruption | Days-weeks | EGFR inhibitors, lithium, corticosteroids, isoniazid | Mild |
| Drug-induced lupus (DIL) | Months | Hydralazine, procainamide, minocycline, anti-TNF, isoniazid | Moderate |
Epidemiology & Risk Factors
- ~2-3% of hospitalised patients develop a cADR; they are the commonest cause of dermatology consultation in hospital.[9]
- Higher risk: immunocompromised (HIV/AIDS, SLE), female sex, polypharmacy, active malignancy, genetic predisposition (HLA associations).[3][7]
- SCAR incidence: DRESS ~1/million/year; AGEP ~3-5/million/year; SJS/TEN ~1-6/million/year.[7]
Pathophysiology

Most delayed cADR are Type IV (T-cell-mediated) hypersensitivity, subdivided by the dominant T-cell cytokine/effector profile:[3][7]
- Type IVa (Th1): IFN-γ dominant → morbilliform exanthem, allergic contact dermatitis.
- Type IVb (Th2): IL-4, IL-5, IL-13 dominant → DRESS/DIHS (eosinophilia, HHV-6 reactivation).
- Type IVc (cytotoxic T cells): perforin/granzyme → SJS/TEN and some cases of AGEP.
- Type IVd (T-cell/neutrophil): IL-8/CXCL8 → AGEP (neutrophilic pustules). [1]
Non-immunological mechanisms include cumulative toxicity, pharmacological side-effects (e.g. acneiform from EGFR inhibitors), photosensitivity (phototoxic vs photoallergic), and idiosyncratic reactions.[9]
Pharmacogenomics & HLA Screening
[1]High-yield HLA associations for the examination
Pharmacogenomic screening for high-risk drugs — when to test
HLA-B*15:02 and carbamazepine
The association between HLA-B*15:02 and carbamazepine-induced SJS/TEN was established in Han Chinese populations and replicated across Thai, Malaysian, Indian, and Vietnamese populations. The mechanism is a hapten-specific T-cell response where the carbamazepine-HLA-B*15:02 complex triggers CD8+ cytotoxic T cells releasing granulysin and perforin/granzyme B, producing keratinocyte apoptosis. The absolute risk in HLA-B*15:02-positive patients exposed to carbamazepine is approximately 5% for SJS/TEN, compared with ~0.01% in non-carriers. The FDA and EMA mandate screening in Asian populations; screening is cost-effective and recommended before carbamazepine in any patient of Asian descent.[7]
Cross-reactivity: aromatic anticonvulsants (phenytoin, phenobarbital, primidone, carbamazepine, oxcarbazepine, eslicarbazepine) share the B*15:02 risk and should be avoided. Safe alternatives in HLA-B*15:02-positive patients include levetiracetam, brivaracetam, gabapentin, pregabalin, vigabatrin, valproate (note valproate is not first-line in women of childbearing potential). Lamotrigine has its own SCAR risk; titrate slowly.[7]
HLA-B*58:01 and allopurinol
HLA-B*58:01 is strongly associated with allopurinol-induced SJS/TEN and DRESS in Han Chinese, Thai, and Korean populations (odds ratio ~80). The allele frequency is ~6-9% in Han Chinese, ~6-8% in Thai, and ~12% in Korean populations. Screening before first prescription is recommended in these populations. In other populations (European, African, Japanese), the allele frequency is low (< 1%) and the cost-effectiveness of universal screening is lower — but a strong family history of allopurinol SCAR should prompt testing. Hypersensitivity to allopurinol may also be driven by renal impairment (oxypurinol accumulates) and concurrent thiazide diuretic use (increases allopurinol hypersensitivity reaction risk).[11]
HLA-A*31:01 and carbamazepine
HLA-A*31:01 is associated with carbamazepine-induced DRESS, SJS, and TEN (broader spectrum than the B*15:02 SJS/TEN association) in European and Japanese populations. Positive predictive value is lower than B*15:02; routine screening is not universally recommended but is being adopted in some European centres, particularly before carbamazepine in patients of European descent with a family history of anticonvulsant hypersensitivity.[7]
HLA-B*57:01 and abacavir
HLA-B*57:01 screening is the gold standard for preventing abacavir hypersensitivity syndrome (AHS) — a multi-organ reaction with fever, rash, GI symptoms, and respiratory involvement. Universal pre-prescription screening is mandated in regulatory labelling; the positive predictive value is ~50% and the negative predictive value is ~100%. HLA-B*57:01-positive patients must never receive abacavir. This is the only universally mandated HLA screen before a drug and is the prototype for pharmacogenomic screening in drug hypersensitivity.[7]
Clinical Patterns in Detail
Morbilliform exanthem
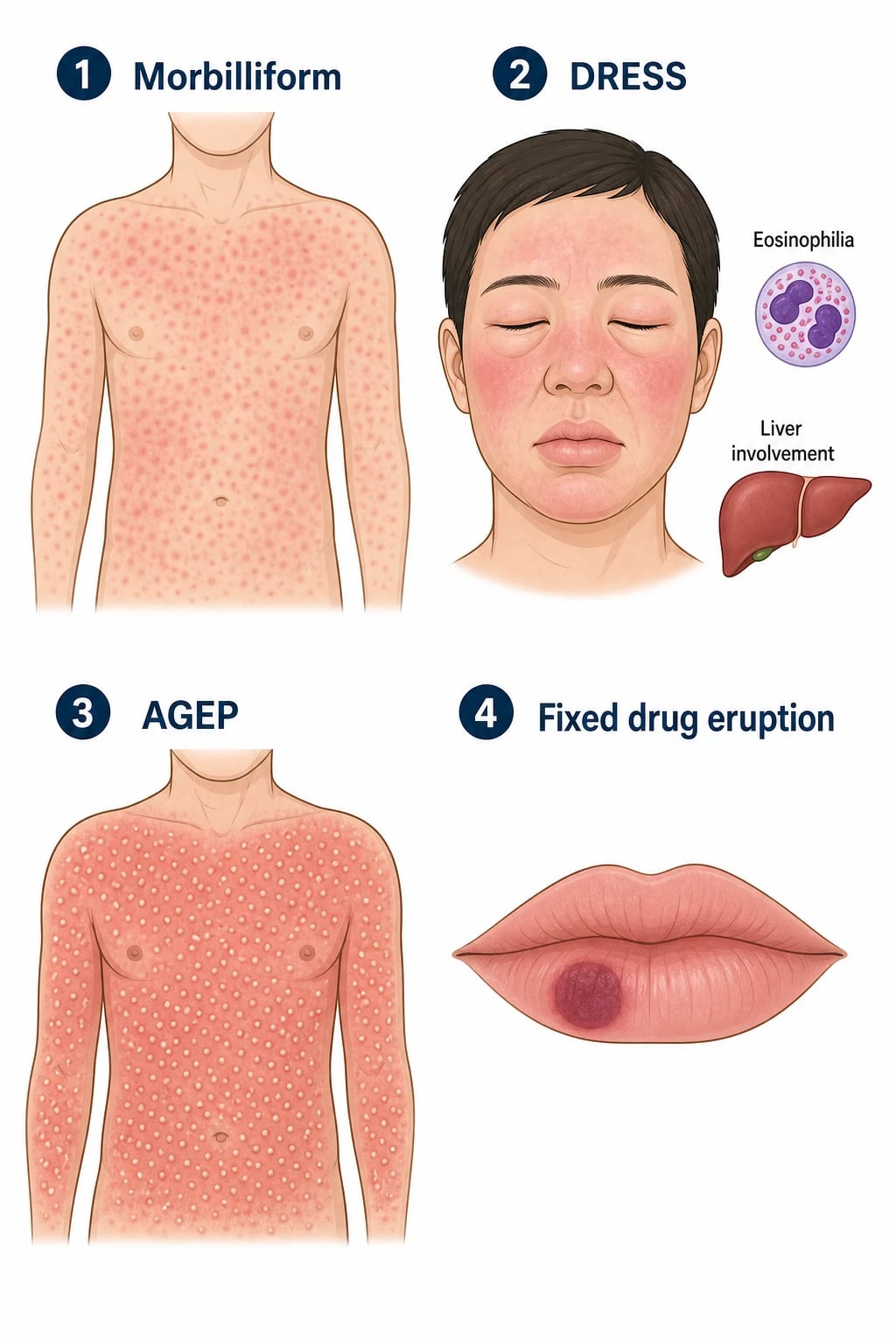
The commonest cADR (~90%). Symmetrical maculopapular erythematous rash on the trunk spreading to extremities, 7-14 days after drug initiation (or 1-3 days on re-exposure). May have mild fever and pruritus; mucous membranes spared. Resolves on drug withdrawal in 1-2 weeks. Culprit drugs: β-lactams, sulfonamides, allopurinol, anticonvulsants.[9]
DRESS / DIHS (Drug Reaction with Eosinophilia and Systemic Symptoms)
Latency: 2-8 weeks after drug initiation (longer than other cADR — examiners test this). Triad of: (1) rash (often a facial oedema with a maculopapular exanthem, sometimes with vesicles/pustules), (2) eosinophilia (>1.5 × 10⁹/L) and/or atypical lymphocytes, and (3) systemic organ involvement (hepatic > renal > pulmonary > cardiac). Fever and lymphadenopathy are common. HHV-6 reactivation is characteristic (DIHS = the Japanese term emphasising the viral reactivation). Mortality ~10%.[1][2]
RegiSCAR criteria for DRESS (≥3 of 7 for probable DRESS): hospitalisation; reaction suspected to be drug-related; acute rash; fever >38°C; enlarged lymph nodes; ≥1 internal organ involved; blood count abnormalities (eosinophilia or atypical lymphocytes).[2]
AGEP (Acute Generalised Exanthematous Pustulosis)
Latency: less than 4 days (faster than DRESS). Hundreds of small ( less than 5 mm) sterile pustules on a diffuse erythematous base, especially in the intertriginous areas. Fever and mild systemic involvement (but NOT the severe organ involvement of DRESS). Rapid resolution on drug withdrawal ( less than 15 days). Culprit drugs: aminopenicillins, cephalosporins, pristinamycin, terbinafine, diltiazem, hydroxychloroquine.[5][6][8]
Fixed drug eruption
Round, well-demarcated, erythematous-violaceous plaque that recurs at the SAME site on re-exposure to the culprit drug. Leaves residual hyperpigmentation. Common sites: lips, genitals, hands, face. Culprit drugs: NSAIDs, paracetamol, sulfonamides, tetracyclines, phenolphthalein.[9]
Other patterns in detail
Erythema multiforme (EM) and EM major. Acute, immune-mediated, target lesions (under 3 cm, three concentric zones, raised border) on the extremities (acral, palms, soles). Most commonly triggered by herpes simplex virus (recurrent EM) and Mycoplasma pneumoniae (EM with mucosal involvement, particularly in children). Drug-triggered EM is uncommon; the distinction is important — drug-induced EM-like eruptions overlap clinically with early SJS. Pathology shows a perivascular lymphocytic infiltrate with necrotic keratinocytes, mostly limited to the epidermis.[9]
Photosensitivity. Two mechanisms: phototoxic (UV-A generates reactive oxygen species that damage cell membranes; dose-dependent; any person; exaggerated sunburn on sun-exposed sites, often within hours; culprit drugs include fluoroquinolones, tetracyclines, especially demeclocycline and doxycycline, thiazide diuretics, amiodarone, NSAIDs, especially piroxicam, voriconazole and vemurafenib) and photoallergic (drug becomes a hapten, processed by Langerhans cells, T-cell mediated; eczematous, delayed onset 24-72 h, requires sensitisation, persists after drug withdrawal; culprits include phenothiazines, thiazides, quinidine, sulfonamides, NSAIDs). On examination the rash is sharply limited to sun-exposed sites — face, V of chest, dorsal hands, forearms — with sparing of submental, retroauricular and submandibular skin, a useful clue at the bedside.[9]
Drug-induced pigmentation. Can occur after weeks to years of therapy. (i) Minocycline — blue-grey to slate-grey on shins, acne scars, mucosa, teeth, sclera, sometimes the entire skin; (ii) amiodarone — blue-grey on malar areas, nose, ears ("smurf skin") after cumulative doses > 100 g; (iii) clofazimine — red-brown to black on lesional and sun-exposed skin; (iv) hydroxychloroquine — yellow-brown on shins, palate, nails and under the eyes after years; (v) heavy metals (silver = argyria, gold = chrysiasis, arsenic) — slate-grey in sun-exposed sites; (vi) methotrexate, zidovudine — transverse nail or mucosal hyperpigmentation. Resolution is slow after drug cessation (months to years), particularly for minocycline, which may never fully resolve.[9]
Drug-induced lupus (DIL). Subacute onset weeks to months after starting the drug, with arthralgia, myalgia, fever, serositis and cutaneous features (photosensitive malar rash, annular polycyclic or psoriasiform lesions). Renal and CNS disease are uncommon (in contrast to idiopathic SLE). Autoantibody profile: anti-histone antibodies positive in > 95% (the immunological hallmark), anti-dsDNA usually negative, ANA positive. Subtypes: systemic DIL (hydralazine, procainamide, isoniazid, minocycline, methyldopa, chlorpromazine, quinidine), cutaneous DIL (anti-TNF, terbinafine, thiazides, calcium channel blockers, proton pump inhibitors, statins, anti-histamines). Hydralazine, procainamide and isoniazid are "slow acetylators" — the genetic predisposition (N-acetyltransferase 2 slow acetylator phenotype) explains the higher DIL risk in this subgroup. Onset within weeks of starting therapy and resolution within weeks of stopping — rechallenge is contraindicated.[9]
Acneiform eruption. Monomorphic erythematous papules and pustules without comedones, on the face, scalp, chest and upper back. Typical of EGFR inhibitors (cetuximab, panitumumab, erlotinib, gefitinib, osimertinib; > 80% incidence), MEK inhibitors, mTOR inhibitors and corticosteroids. Also lithium, isoniazid, ciclosporin, vitamin B12, anabolic steroids. Distinguish from acne vulgaris by the absence of comedones and the uniform morphology; treat with topical metronidazole, oral tetracyclines, and for severe EGFR rash, oral minocycline and topical steroids; dose reduction of the culprit EGFR inhibitor is often necessary.[9]
Drug-induced bullous pemphigoid (BP). Tense subepidermal bullae on urticarial or erythematous base, often in the elderly, with pruritus, eosinophilia and positive anti-BP180/BP230 antibodies on ELISA and DIF showing linear IgG/C3 at the basement membrane zone. Commonest culprits: diuretics (loop and thiazide), penicillins, sulfonamides, NSAIDs, DPP-4 inhibitors (gliptins), antipsychotics, biologics (anti-TNF, immune checkpoint inhibitors). DPP-4 inhibitors carry the highest risk (~3-fold) and the latency may be years — a classic examination trap. Stop the drug and treat with topical or oral corticosteroids, doxycycline, or methotrexate as for idiopathic BP.[7][9]
Lichenoid drug eruption. Violaceous, polygonal, flat-topped, pruritic papules resembling lichen planus but with a more eczematous, eczematous and psoriasiform admixture, often photodistributed and involving sun-exposed sites; Wickham striae are usually absent. Latency weeks to months. Commonest culprits: thiazides, gold, antimalarials, ACE inhibitors, beta-blockers, sulfonamides, anti-TNF, immune checkpoint inhibitors (especially anti-PD-1/PD-L1), proton pump inhibitors. Pathology shows a lichenoid interface dermatitis with parakeratosis, eosinophils and focal necrotic keratinocytes — clues to drug aetiology. Slow resolution (weeks to months) after drug withdrawal.[7]
Pityriasis rosea-like drug eruption. Herald patch absent or atypical; multiple oval scaly papules and plaques following skin cleavage lines, often more inflammatory, itchy and persistent than idiopathic pityriasis rosea; associated with eosinophils on biopsy. Common culprits: captopril, isotretinoin, gold, methotrexate, barbiturates, metronidazole, omeprazole, beta-blockers, hepatitis B vaccine.[9]
Drug-induced vasculitis. Palpable purpura (most commonly cutaneous leucocytoclastic vasculitis, but larger vessel involvement in ANCA-associated vasculitis can occur). Commonest culprits: levamisole (cocaine cutting agent, ANCA-positive, retiform purpura on ears, cheeks, nose), hydralazine, propylthiouracil (p-ANCA, also MPO-ANCA), minocycline, allopurinol, sulfonamides, anti-TNF, immune checkpoint inhibitors. Document ANCA, anti-MPO, anti-PR3, complement, urinalysis (haematuria/proteinuria for renal involvement). Stop drug; treat with corticosteroids ± cyclophosphamide if severe.[7]
Serum sickness-like reaction. Urticarial or morbilliform rash with fever, arthralgia and lymphadenopathy 1-3 weeks after exposure (commonly cefaclor, cefuroxime, penicillin, sulfonamides, rituximab, infliximab). Immune-complex deposition drives the reaction; hypocomplementaemia is the immunological hallmark (true serum sickness, e.g. after antithymocyte globulin or rabies antiserum, has hypocomplementaemia; serum sickness-like reactions do not — useful bedside discriminator).[9]
Differential Diagnosis
| Mimic | Distinguishing features | [1]
| Mimic | Distinguishing features |
|---|---|
| Viral exanthem | No drug timeline; prodrome; coryza; resolves without drug withdrawal |
| Erythema multiforme | Target lesions; HSV/Mycoplasma trigger; no eosinophilia |
| Kawasaki disease | Children; fever 5+ days; strawberry tongue; coronary aneurysms |
| Connective tissue disease | ANA/dsDNA; no drug timeline; chronic course |
| Cutaneous lymphoma | Chronic, persistent; biopsy diagnostic |
Investigations
- FBC with differential: eosinophilia (DRESS), atypical lymphocytes (DRESS/DIHS), neutrophilia (AGEP).[1]
- LFTs, creatinine, urinalysis: organ involvement (DRESS, vasculitis).
- Serum tryptase (if Type I urticarial/anaphylactic reaction — within 1-2h of reaction).
- Skin biopsy: for DRESS (spongiotic dermatitis + eosinophils + necrotic keratinocytes), AGEP (subcorneal pustule), vasculitis (leucocytoclastic vasculitis), SJS/TEN (full-thickness necrosis).
- HHV-6 serology (rising titres in DRESS/DIHS).
- Patch testing (weeks after resolution — for delayed-type reactions; useful for some drugs).[3]
- Drug provocation testing (DPT): gold standard for confirmation, but contraindicated in SCAR (SJS/TEN, DRESS, AGEP).[3]

Causality Assessment — Naranjo Algorithm
[1]Naranjo algorithm — the 10 questions:[3]
| # | Question | Yes | No | Don't know |
|---|---|---|---|---|
| 1 | Previous conclusive reports on this reaction? | +1 | 0 | 0 |
| 2 | Did the adverse event appear after the suspected drug was given? | +2 | −1 | 0 |
| 3 | Did the reaction improve when the drug was stopped or a specific antagonist given? | +1 | 0 | 0 |
| 4 | Did the reaction reappear when the drug was readministered? | +2 | −1 | 0 |
| 5 | Are there alternative causes (other drugs, underlying disease) that could have caused the reaction? | −1 | +2 | 0 |
| 6 | Did the reaction reappear when a placebo was given? | −1 | +1 | 0 |
| 7 | Was the drug detected in blood (or other fluids) at a toxic concentration? | +1 | 0 | 0 |
| 8 | Was the reaction more severe with a higher dose, or less severe with a lower dose? | +1 | 0 | 0 |
| 9 | Has the patient experienced a similar reaction to the same or similar drugs in any previous exposure? | +1 | 0 | 0 |
| 10 | Was the adverse event confirmed by any objective evidence? | +1 | 0 | 0 |
Interpretation: ≥9 = definite; 5-8 = probable; 1-4 = possible; ≤0 = doubtful. For SCAR, rechallenge (Q4) is contraindicated — a positive readministration score is therefore seldom obtainable in practice. In this setting, questions 1, 2, 3, 5, and 10 carry most of the discriminatory weight. The Liverpool Adverse Drug Reaction Causality Assessment Tool (ADRAC) and the WHO-UMC standardised case causality assessment are complementary tools used in pharmacovigilance reporting.[3]
Bedside application in a suspected DRESS case: [1]
- Previous reports on this drug-ADR pair? (Q1) — e.g. allopurinol-DRESS: +1.
- Reaction appeared after the drug? (Q2) — latency 4 weeks after allopurinol: +2.
- Reaction improved on withdrawal? (Q3) — fever and rash settling after stop: +1.
- Readministration? (Q4) — contraindicated in SCAR, so 0.
- Alternative causes? (Q5) — viral exanthem excluded by serology, no other new drugs: +2.
- Placebo? (Q6) — not applicable: 0.
- Drug level? (Q7) — usually not done: 0.
- Dose relationship? (Q8) — no clear relation: 0.
- Previous similar reaction? (Q9) — no: 0.
- Objective evidence (eosinophilia, organ involvement)? (Q10) — yes: +1. Total = 7 → probable. [1]
Limitations: the algorithm is operator-dependent (inter-rater variability for Q5 and Q9), performs less well in delayed T-cell-mediated reactions, and does not capture the morphology of the rash. Always combine the Naranjo score with a morphology-based diagnostic algorithm (RegiSCAR for DRESS; AGEP EuroSCORE for AGEP; EuroSCAR for SJS/TEN) for a complete bedside assessment.[3]
Management

General principles
- STOP the culprit drug — establish the timeline; the drug started closest to the rash onset is the prime suspect.
- Document the reaction and culprit in the medical record; alert card/MedicAlert.[9]
By pattern
Morbilliform: withdrawal + antihistamines + emollients; resolves in 1-2 weeks.[9]
Urticaria / anaphylaxis: withdrawal + antihistamines + adrenaline (IM 0.5 mg) if anaphylaxis; check serum tryptase.[3]
- STOP drug immediately.
- Systemic corticosteroids (prednisolone 0.5-1 mg/kg/day); some centres use pulsed methylprednisolone for severe organ involvement.
- Ciclosporin (3-5 mg/kg/day) for refractory or rapidly progressive disease.
- SLOW taper over weeks to months (DRESS has a relapsing course; HHV-6 reactivation drives flares).
- Supportive care for organ failure (hepatic, renal).
- Monitor FBC, LFTs, creatinine during taper.
- STOP drug.
- Supportive care; topical corticosteroids for symptomatic relief.
- Usually self-resolving within ** less than 15 days** of drug withdrawal.
- AGEP validation score (EuroSCORE) assists diagnosis (points for pustules, erythema, acute onset, resolution less than 15 days, fever, previous AGEP).
Fixed drug eruption: stop drug; topical corticosteroid for the active lesion; warn about re-exposure; document allergen.[9]
Special Populations
- HIV/AIDS: markedly increased risk of cADR (sulfonamides, nevirapine, abacavir); higher rate of SCAR.[7]
- Children: viral exanthem is the main mimic; DRESS and SJS/TEN are rare but occur; careful drug history.[9]
- Elderly / polypharmacy: multiple potential culprits; careful timeline analysis; higher morbidity from SCAR.[9]
Prognosis
- Morbilliform, FDE, urticaria: excellent prognosis on drug withdrawal.
- DRESS: mortality ~10%; relapsing course over weeks-months; long-term autoimmune sequelae (autoimmune thyroiditis, type 1 diabetes) in some.[1][2]
- AGEP: mortality ~2-5%; generally rapid resolution on drug withdrawal; usually no long-term sequelae.[5]
- SJS/TEN: see dedicated topic; mortality 10-35%.[7]
Evidence, Guidelines & Regional Differences
- RegiSCAR criteria for DRESS (internationally validated).[2]
- AGEP EuroSCORE / European consensus 2024 (Tetart).[8]
- Spanish guidelines for DRESS diagnosis, management and prevention (Cabañas 2020).[2]
- HLA screening (B15:02 for carbamazepine; B58:01 for allopurinol) — population-specific.[7]
- Nat Rev Dis Primers 2024 (Hung) — comprehensive SCAR review.[7]
Drug-specific patterns and doses
Prevention [1]
- Document all drug allergies; MedicAlert; electronic alerts.
- Avoid re-challenge with the culprit and structurally related drugs.
- HLA screening before high-risk drugs in susceptible populations (carbamazepine, allopurinol).[7]
- Start allopurinol low (≤100 mg/day) and titrate slowly; lower dose in renal impairment.[2]
Exam Pearls
[1]Red Flags
Exam application bank (NEET-PG / INICET)
One-line answer
Cutaneous adverse drug reactions (cADR) range from the common morbilliform exanthem (90%) to life-threatening severe cutaneous adverse reactions (SCAR) including DRESS/DIHS, AGEP, and SJS/TEN. Each pattern has a characteristic latency (urticaria minutes-hours; morbilliform 7-14 days; DRESS 2-8 weeks; AGEP less than 4 days; fixed drug eruption hours-days), culprit drug profile, and management pathway. Fellowship-level assessment demands mastery of the full cADR spectrum, the Type IV hypersensitivity subtypes that underpin delayed reactions, the RegiSCAR criteria for DRESS, the AGEP validation score, the distinguishing features between DRESS/AGEP/SJS-TEN, culprit drug lists (allopurinol, sulfonamides, anticonvulsants, aminopenicillins, minocycline, NSAIDs), and the severity-driven management from simple drug withdrawal to systemic immunosuppression.
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard. [1]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes. [1]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change. [1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each. [1]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory. [1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Drug eruptions.
Expanded exam teaching (depth pass)
Clinical reasoning
For Drug eruptions, examiners test whether you can prioritise life threats, choose the right first test, and give specific therapy (agent, dose, route, timing). Generic phrases without numbers score poorly.
Mechanism → feature map
Build a short chain: cause → pathophysiologic intermediate → clinical feature → complication. Every major symptom in the classic vignette should sit on that chain.
Investigation strategy
- Bedside/first-line tests that change immediate management
- Confirmatory or staging tests
- What a normal result does not exclude
- When not to delay treatment for imaging (unstable patient)
Management ladder
- Resuscitation / ABC / sepsis or haemorrhage bundle as relevant
- Specific antidote / procedure / antimicrobial / reperfusion / surgery
- Supportive care and monitoring targets
- Definitive long-term therapy and secondary prevention
- Disposition and safety-net advice
Special populations
Always prepare one line each for children, pregnancy, elderly, renal/hepatic impairment, and immunocompromised patients when the topic allows.
Pitfalls that fail candidates
- Treating the number not the patient
- Missing pregnancy status when relevant
- Imaging before stabilisation
- Wrong empiric cover or wrong antidote timing
- Incomplete counselling on recurrence, adherence, or red-flag return
Cutaneous adverse drug reactions (cADR) range from the common morbilliform exanthem (90%) to life-threatening severe cutaneous adverse reactions (SCAR) including DRESS/DIHS, AGEP, and SJS/TEN. Each pattern has a characteristic latency (urticaria minutes-hours; morbilliform 7-14 days; DRESS 2-8 weeks; AGEP less than 4 days; fixed drug eruption hours-days), culprit drug profile, and management pathway. Fellowship-level assessment demands mastery of the full cADR spectrum, the Type IV hypersensitiv [1]
[1]References
- [1]Calle AM, Aguirre N, Ardila JC, et al. DRESS syndrome: A literature review and treatment algorithm World Allergy Organ J, 2023.PMID 37082745
- [2]Cabañas R, Ramírez E, Sendagorta E, et al. Spanish Guidelines for Diagnosis, Management, Treatment, and Prevention of DRESS Syndrome J Investig Allergol Clin Immunol, 2020.PMID 31932268
- [3]Wilkerson RG. Drug Hypersensitivity Reactions Immunol Allergy Clin North Am, 2023.PMID 37394254
- [4]Sharifzadeh S, Mohammadpour AH, Tavanaee A, et al. Antibacterial antibiotic-induced drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome: a literature review Eur J Clin Pharmacol, 2021.PMID 33025080
- [5]Parisi R, Shah H, Navarini AA, et al. Acute Generalized Exanthematous Pustulosis: Clinical Features, Differential Diagnosis, and Management Am J Clin Dermatol, 2023.PMID 37156992
- [6]Szatkowski J, Schwartz RA. Acute generalized exanthematous pustulosis (AGEP): A review and update J Am Acad Dermatol, 2015.PMID 26354880
- [7]Hung SI, Mockenhaupt M, Blumenthal KG, et al. Severe cutaneous adverse reactions Nat Rev Dis Primers, 2024.PMID 38664435
- [8]Tetart F, Walsh S, Milpied B, et al. Acute generalized exanthematous pustulosis: European expert consensus for diagnosis and management J Eur Acad Dermatol Venereol, 2024.PMID 39023187
- [9]Del Pozzo-Magaña BR, Liy-Wong C. Drugs and the skin: A concise review of cutaneous adverse drug reactions Br J Clin Pharmacol, 2024.PMID 35974692
- [10]Zhang J, Lei Z, Xu C, et al. Current Perspectives on Severe Drug Eruption Clin Rev Allergy Immunol, 2021.PMID 34273058
- [11]Sang H, Lee MW, Zhao Y, et al. Drug eruptions induced by allopurinol associated with HLA-B*5801 Indian J Dermatol Venereol Leprol, 2015.PMID 25566896
- [12]Kung S, Allen R, Devarakonda K, et al. Management of Psychotropic Drug-Induced DRESS Syndrome: A Systematic Review Mayo Clin Proc, 2016.PMID 27126302