Dermatology · Medicine
Erythema ab igne
Also known as Erythema ab igne · Toasted skin syndrome · Fire stains · Thermal keratosis
Erythema ab igne (EAI, toasted skin syndrome) is a localised cutaneous reaction caused by chronic, repeated exposure to moderate heat — insufficient to cause a thermal burn but enough to damage the superficial dermal vasculature — producing a characteristic reticulated (net-like), brownish-purple hyperpigmentation on the heat-exposed skin. Modern causes include laptop computers on the lap, heating pads, hot water bottles, heated car seats, space heaters, electric blankets, and open fires. Histology may mimic actinic keratosis (atypical keratinocytes — 'thermal keratosis'). Long-standing lesions carry a small but real risk of malignant transformation to squamous cell carcinoma. Management: remove the heat source (primary and most effective intervention); topical retinoids for hyperpigmentation; topical 5-fluorouracil for thermal keratosis; excision for SCC.
On this page & tools
Your progress
Saved locally on this device.
Exam tags
Red flags
Overview & Definition
Erythema ab igne — from the Latin erythema ("redness") ab ("from") igne ("fire") — is a cutaneous reaction pattern produced by chronic, repeated exposure to moderate heat at temperatures sufficient to injure the superficial dermal vasculature but insufficient to produce a thermal burn. It is also called toasted skin syndrome, fire stains, chronic moderate heat dermatosis, and, in its premalignant keratotic phase, thermal keratosis. The clinical signature is a reticulated (net-like or fishnet-pattern), brownish-purple to greyish hyperpigmentation that develops insidiously over the heat-exposed skin.[1][3]
The defining exposure lies in a narrow thermal window: skin temperatures sustained at approximately 43 to 47 degrees Celsius for prolonged or repeated periods. Below this range the heat is harmless; above it (typically 44 degrees C sustained for several hours or a brief peak above approximately 50 to 55 degrees C) the skin sustains an outright thermal burn (first, second, or third degree). EAI occupies the middle ground — enough heat to damage the vascular endothelium of the superficial plexus and to injure basal keratinocytes, but never enough to coagulate tissue wholesale. This is why EAI does not blister in the classic sense of a thermal burn; the rare bullae seen in advanced disease are a consequence of epidermal atrophy and basal layer necrosis, not of acute coagulative injury. [1]

Historically, EAI was the dermatological signature of the pre-central-heating era: it was common in people who huddled close to open fires, pot-bellied stoves, radiators, and hot brick walls — particularly elderly women, chronic pain sufferers, and patients with tuberculosis or chronic arthritis who sat for hours beside a heat source. With the introduction of central heating, the incidence fell dramatically. However, EAI re-emerged in the modern era with new heat sources: laptop computers (the ventilation fan and battery on the lap), electric heating pads (chronic back pain), hot water bottles (dysmenorrhoea, abdominal pain), heated car seats, space heaters, electric blankets, heated recliners, fire pits, and even repeated hot yoga practice. Occupational EAI persists in cooks, bakers, chefs, glassblowers, foundry workers, silversmiths, and blacksmiths whose torso or forearms are chronically exposed to radiant heat.[4]
EAI matters to the clinician for three reasons. First, it is a sentinel clue: its presence demands a focused search for the heat source and, frequently, for the underlying reason the patient is seeking heat (chronic pain, hypothyroidism, malignancy with cachexia, neurological disease, or domestic fuel poverty). Second, in its late stages it carries a small but real risk of malignant transformation to squamous cell carcinoma via thermal keratosis — a histological mimic of actinic keratosis. Third, although the early lesion is fully reversible, the late pigmentation and atrophy are permanent, and prevention (heat source elimination) is the only truly effective intervention. [1]
[1]Classification
EAI is best classified along two complementary axes: clinical stage (which reflects cumulative heat exposure and predicts reversibility) and aetiology / heat source (which dictates the counselling and prevention strategy). Both are clinically useful. [1]
By clinical stage
| Stage | Onset | Morphology | Reversibility |
|---|---|---|---|
| Stage 1 — Early erythema | Days to weeks of exposure | Mild, transient, reticular pink-red erythema that may blanch or fade with cooling; often unnoticed by the patient | Fully reversible within weeks of heat removal |
| Stage 2 — Reticular hyperpigmentation | Weeks to months of exposure | Classic brownish-purple to greyish, fixed, net-like pattern; mild overlying scaling; asymptomatic or mild pruritus | Slowly improves over months but may leave residual pigmentation |
| Stage 3 — Late atrophic / keratotic | Months to years of exposure | Atrophy, telangiectasia, mottled hyperpigmentation, keratoses (thermal keratosis), occasional bullae, and risk of SCC | Permanent; thermal keratosis is premalignant and requires active treatment |
The staging matters clinically because it predicts (a) whether the lesion will resolve with heat removal alone, and (b) whether biopsy is warranted for suspected dysplasia or malignancy. Stage 1 is essentially invisible to history — the patient often does not notice it. Stage 2 is the stage at which most patients present, having been alarmed by the cosmetic change. Stage 3 is the stage at which the condition stops being a curiosity and becomes a premalignant dermatosis.[1]
By aetiology (heat source)
This classification is the more useful one clinically because it directs prevention: [1]
Causes of erythema ab igne — the HEAT mnemonic
The aetiological categories are: [1]
- Domestic / recreational — laptop computers (the dominant modern cause in young people), heating pads and hot water bottles (chronic pain or dysmenorrhoea), electric blankets, heated car seats, space heaters, fire pits, infrared saunas, and repeated use of heated furniture. These together account for the great majority of cases seen in primary care and dermatology clinics in developed countries.[4]
- Occupational — cooks and chefs (forearms and abdomen over stoves), bakers (forearms over ovens), glassblowers (face, neck, forearms), foundry workers and smelters (face, forearms), silversmiths and jewellers (hands), blacksmiths (forearms), and welders. Occupational EAI is frequently bilateral and symmetric because both forearms are exposed.
- Cultural / regional — open-fire cooking on traditional stoves (chulha in South Asia), sitting close to brick or mud walls heated by an internal fire (the classic kang or ondol heated-bed cultures of East Asia), hookah use (anterior chest), and religious or ritual practices involving proximity to fires.
- Medical- and pain-driven — chronic low-back pain, osteoarthritis, rheumatoid arthritis, ankylosing spondylitis, fibromyalgia, endometriosis, dysmenorrhoea, neuropathic pain, and chronic abdominal pain all drive patients to apply heat repeatedly. In these cases the skin lesion is a clue to a treatable underlying condition that needs its own management.
In practice, most cases in young adults are laptop-induced, while most cases in the elderly are pain- or cold-intolerance-driven. A careful history of everyday heat exposure is the single most important diagnostic step. [1]
Epidemiology & Risk Factors
Precise prevalence figures for EAI are not available — the condition is under-reported because it is often asymptomatic, cosmetically mild, and self-attributed by patients to "bruising" or "age spots." However, several epidemiological patterns are well established.[1][3]
Age and demographics
- Young adults (15 to 35 years) — the laptop-induced form dominates. University students, software professionals, and gamers who use a laptop on the lap for several hours daily for weeks to months are the prototypical demographic. The anterior thigh is the classic site, and the lesion is often bilateral (because the laptop straddles both thighs). Female sex is slightly over-represented in case series, possibly because of thinner skin on the thighs and greater laptop use on the lap (rather than at a desk).
- Elderly (over 65 years) — the pain- and cold-intolerance-driven form dominates. Chronic osteoarthritis of the lumbar spine, hips, or knees drives daily use of heating pads, hot water bottles, or sitting close to a radiator. The lower back is the classical site. Polypharmacy-induced cold intolerance and reduced dermal vascularity (senile atrophy) amplify the injury. Elderly women living alone are over-represented.
- Children and adolescents — increasingly recognised with the rise of gaming laptops and tablets used on the lap, heated blankets, and gaming chairs with built-in heaters. Paediatric EAI is often misdiagnosed as child abuse (bruising), Mongolian spot, or post-inflammatory hyperpigmentation.[5]
- Occupational groups — middle-aged men working in foundries, glassworks, bakeries, commercial kitchens, and welding shops. The lesion is typically on the forearms, dorsal hands, face, and neck — the parts closest to the radiant heat source.
Systemic and behavioural risk factors
| Risk factor | Mechanism | Clinical clue |
|---|---|---|
| Chronic pain (osteoarthritis, RA, fibromyalgia, low back pain) | Drives daily, repeated use of heating pads and hot foments | EAI on the lower back, knee, or shoulder that corresponds to the painful joint |
| Hypothyroidism | Cold intolerance → heat-seeking behaviour (sitting close to heaters, layering blankets) | Diffuse, often bilateral EAI on shins or thighs; check TSH |
| Malignancy with cachexia | Constitutional coldness and weight loss → patient seeks external heat | EAI in a frail, weight-losing patient — investigate for occult cancer |
| Neurological disease (stroke, paraplegia, neuropathy) | Reduced mobility → patient sits with legs close to a heat source for hours; loss of protective sensation may permit more intense exposure | Asymmetric EAI on a paralysed limb; check for associated thermal burn |
| Diabetes mellitus | Diabetic neuropathy reduces pain/heat appreciation → prolonged, intense heat exposure | EAI on the feet (rare) or legs from heating pads |
| Dementia / cognitive impairment | Patient forgets to remove the heat source; cannot report early discomfort | Severe, fixed EAI in an institutionalised patient; risk of coexisting burn |
| Cold climates / winter | Greater ambient heating device use | EAI presents in winter; incidence rises in colder latitudes |
| Domestic fuel poverty | Patient cannot afford central heating; relies on single concentrated heat source | EAI on the side of the body facing the heater ("fireside keratosis") |
Modern and recreational heat sources
The modern EAI epidemic is driven by:
- Laptop computers — ventilation fan on the lap, battery heat, and the user's thighs absorbing radiant heat for hours. Modern gaming laptops with powerful GPUs run hotter and cause faster EAI than ultraportables.[4]
- Heating pads and electric blankets — direct skin contact, often overnight, for chronic pain.
- Hot water bottles — applied to the abdomen for dysmenorrhoea, endometriosis, or chronic pelvic pain.
- Heated car seats — prolonged driving with the seat heater on a high setting; asymmetric (only the driving-side buttock and posterior thigh).
- Space heaters and infrared heaters — close, prolonged exposure (under-desk heaters cause EAI on the shins).
- Heated recliners and massage chairs — prolonged seated exposure; back and posterior thighs.
- Fire pits, infrared saunas, hot yoga — newer recreational sources.
In children, gaming devices, tablets, and heated gaming chairs are increasingly reported.[5]
Pathophysiology
The pathogenesis of EAI is a cascade triggered by chronic infrared radiation injury to the superficial cutaneous vasculature. Unlike ultraviolet radiation (which damages DNA directly), infrared heat damages tissue thermally — by denaturing proteins, destabilising membranes, and inducing a chronic low-grade inflammatory state. The clinical net-like pattern emerges because the reticular subpapillary venous plexus is the anatomical structure that absorbs the brunt of the heat and reveals the injury. [1]
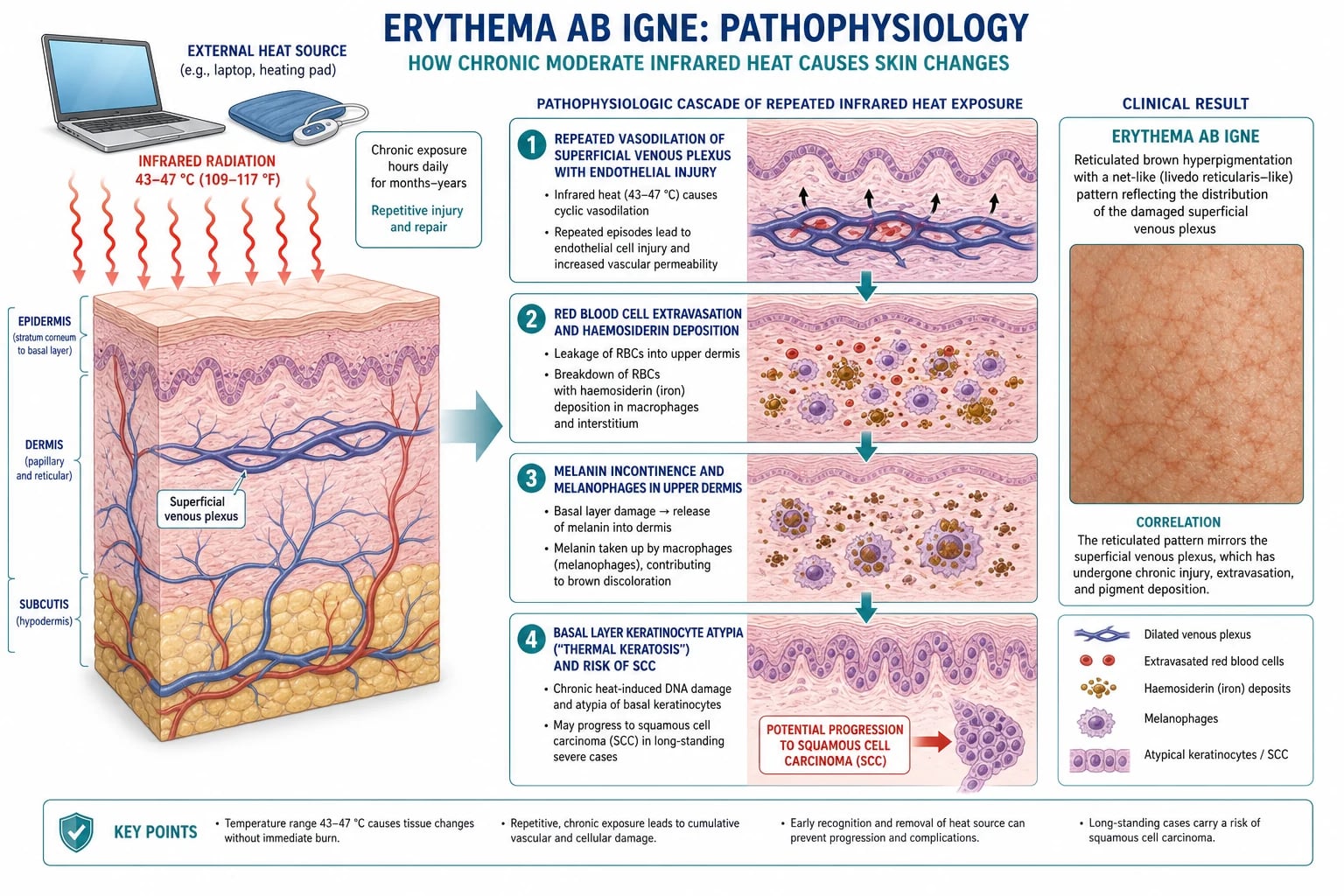
Step 1: Endothelial injury to the subpapillary venous plexus
Chronic, repeated moderate heat produces repeated cycles of vasodilation in the superficial dermal vessels. The subpapillary venous plexus — a network of small postcapillary venules lying immediately beneath the dermal papillae — is the most thermally sensitive cutaneous structure. Repeated vasodilation causes endothelial swelling, perivascular lymphocytic infiltrate, and ultimately red cell extravasation (erythrocyte diapedesis through damaged vessel walls). The reticular geometry of this plexus is what gives EAI its characteristic net-like pattern — the visible hyperpigmentation outlines the underlying damaged veins. [1]
The earliest change is purely vascular: transient, blanching, reticular erythema (essentially a fixed livedo pattern). At this stage the lesion is reversible within days of removing the heat. [1]
Step 2: Haemosiderin deposition
Extravasated red blood cells are phagocytosed by dermal macrophages, which break down haemoglobin through the sequence: haemoglobin → haemosiderin. Haemosiderin is a golden-brown, iron-storage complex that persists indefinitely within macrophages. Prussian blue staining of a biopsy specimen reveals this deposition in the upper dermis. Haemosiderin contributes the reddish-brown to purplish component of the lesion's colour. [1]
Step 3: Melanin incontinence
Concurrently, heat-induced injury to basal keratinocytes damages their capacity to retain melanin. Melanin granules are released into the upper dermis, where they are phagocytosed by melanophages (dermal macrophages laden with melanin). This process — called melanin incontinence — is the same mechanism seen in lichen planus, fixed drug eruption, and post-inflammatory hyperpigmentation, and it explains the persistent brown pigmentation of chronic EAI. Melanin incontinence is largely irreversible because dermal melanin cannot be cleared easily. [1]
Step 4: Epidermal changes — thermal keratosis
The most histologically significant change is in the basal epidermis. Chronic heat induces dyskeratotic (atypical) keratinocytes in the basal layer — large, hyperchromatic cells with pleomorphic nuclei and abnormal keratinisation. This change is termed thermal keratosis and is histologically indistinguishable from actinic keratosis, the UV-induced premalignant keratinocyte dysplasia.[2] Over years of exposure, thermal keratosis can evolve through increasing grades of dysplasia to squamous cell carcinoma in situ (Bowen's disease) and ultimately to invasive SCC. The proposed mechanism involves reactive oxygen species generation, chronic inflammation, DNA damage from heat, and p53 tumour suppressor mutation in a UV-independent pathway.
Step 5: Late atrophy and telangiectasia
Long-standing EAI shows epidermal atrophy (thinning of the stratum corneum and spinosum), dermal elastosis (degeneration of dermal collagen and elastic fibres resembling solar elastosis), and telangiectasia of the superficial plexus. Occasional subepidermal bullae form because the thinned, devitalised epidermis detaches from the dermis with minor trauma. The overall histological picture in advanced EAI is that of poikiloderma — atrophy + telangiectasia + pigmentation — a pattern also seen in chronic radiation dermatitis and in autoimmune connective tissue diseases ( dermatomyositis, lupus). [1]
Why the reticular pattern?
The fishnet / reticular pattern is the dermatological fingerprint of EAI. It reflects the anatomy of the subpapillary venous plexus, which forms a regular hexagonal or net-like network under the skin surface. Each "ring" of the net corresponds to the watershed area around a dermal papilla supplied by a vertical capillary loop. Heat damages the venous ends of this network preferentially, and the resulting pigmentation (haemosiderin + melanin) traces the venous pattern. Livedo reticularis shares this same anatomical substrate, which is why both conditions produce a net-like pattern — but livedo is vascular and reversible (constriction only), whereas EAI is pigmentary and fixed (structural vascular injury). [1]
Why EAI does not blister like a thermal burn
The threshold for outright burn injury (epidermal coagulative necrosis with dermo-epidermal separation and blister formation) is roughly 44 degrees C sustained for 6 hours, or any brief exposure above approximately 50 to 55 degrees C. EAI operates in the 43 to 47 degrees C window — enough to injure the endothelium and basal keratinocytes but not enough to coagulate tissue wholesale. The occasional bullae seen in advanced EAI are a feature of epidermal atrophy and basal layer necrosis in the late atrophic stage, not of acute thermal coagulation. [1]
Clinical Presentation
The clinical presentation of EAI is so characteristic that the diagnosis can often be made from across the room — provided the clinician thinks of it. The diagnosis rests on the triad of (1) reticular, brownish-purple hyperpigmentation, (2) distribution matching a recognisable heat source, and (3) a history of chronic moderate heat exposure.[1][3]
Morphology and evolution
The lesion evolves through three clinical stages: [1]
- Stage 1 (early erythematous) — mild, transient, reticular pink-red erythema that may blanch on diascopy or fade with cooling of the skin. Patients rarely notice this stage. There may be mild associated warmth or itching.
- Stage 2 (reticular hyperpigmentation) — the classic presentation. Brownish-purple to greyish, fixed, net-like hyperpigmentation. The colour deepens with continued exposure, evolving from pink-red to purple-brown to dark brown-grey. The lesion does not blanch. Mild overlying scaling and a subtle livedo-like cyanotic hue may be present. Asymptomatic is the rule; mild burning, pruritus, or paraesthesia may occur.
- Stage 3 (late atrophic / keratotic) — epidermal atrophy (skin appears thin, wrinkled, "cigarette-paper"), telangiectasia, mottled hyper- and hypopigmentation, keratoses (rough, scaly, sandpaper-like plaques — thermal keratosis), occasional bullae, and the eventual possibility of SCC (a new nodule, ulcer, or area of induration within the longstanding lesion). [1]
Distribution — heat source dictates site
The single most useful diagnostic clue is the distribution, which always corresponds to the heat source: [1]
The lesion is always sharply demarcated to the heat-exposed area — there is no gradual fade into surrounding skin. A clear geometric boundary (e.g., the rectangular imprint of a laptop base, or the curved edge of a heating pad) is highly characteristic and diagnostically useful. [1]
Symptoms
- Asymptomatic is the rule. Most patients notice the cosmetic change but feel nothing.
- Mild burning, pruritus, or paraesthesia may occur, particularly with continued heat exposure.
- Late-stage lesions with keratoses may feel rough or scaly; a developing SCC may be tender, bleeding, or non-healing. [1]
Timeline
- Onset: weeks to months of repeated heat exposure. Laptop-induced EAI may appear after 2 to 6 months of daily use for several hours.
- Resolution after heat removal: Stage 1 lesions resolve within days to weeks. Stage 2 lesions improve slowly over months but may leave residual permanent pigmentation. Stage 3 atrophic and keratotic changes are permanent.
- Malignant transformation typically requires years to decades of chronic exposure; the literature reports SCC arising in EAI lesions present for over 5 years, often over 10 to 30 years.[2]
Atypical presentations
Differential Diagnosis
The differential diagnosis of a reticular, brownish-purple lesion encompasses vascular, pigmentary, inflammatory, and neoplastic conditions. A systematic approach based on colour, blanching, distribution, and history is essential.[1]
Livedo reticularis (and cutis marmorata)
Livedo reticularis is the most important differential and is most easily confused with early EAI. Both produce a net-like pattern. The key distinguishing features: [1]
- Colour: livedo is violaceous (blue-purple) due to deoxygenated blood in dilated venules; EAI is brownish-purple to grey due to haemosiderin and melanin.
- Blanching: livedo blanches on warming (vascular constriction is reversible); EAI does not blanch (the pigmentation is fixed in the dermis).
- Course: physiological livedo (cutis marmorata) resolves completely with warming; idiopathic livedo reticularis is persistent but non-progressive. EAI deepens with continued heat and develops atrophy and keratoses in late stages.
- Underlying cause: livedo may be physiological (cold, neonatal), idiopathic, or secondary (antiphospholipid syndrome, polyarteritis nodosa, Sneddon syndrome, cryoglobulinaemia, hyperviscosity). EAI always implies a heat source. [1]
Cutis marmorata is the physiological, transient, cold-induced livedo seen in infants and young children on exposure to cold. It resolves within minutes of warming. It is symmetrical on the extremities and is never pigmented. [1]
Livedoid vasculopathy
Livedoid vasculopathy is a chronic, painful, ulcerative thrombo-occlusive disorder of the lower legs, often associated with Factor V Leiden, antiphospholipid syndrome, or other prothrombotic states. It produces small, painful ulcers that heal with white atrophic scars (atrophie blanche). The reticular pattern surrounding the ulcers may resemble EAI, but the painful ulceration and the atrophie blanche scars are absent in EAI. [1]
Cutaneous small-vessel vasculitis (leukocytoclastic vasculitis)
Cutaneous small-vessel vasculitis produces palpable purpura — typically on the dependent lower legs — that is non-blanching (because of extravasated blood in the vessel walls). The lesions are papular and palpable (unlike EAI, which is flat), often with surrounding erythema and systemic symptoms (fever, arthralgia, abdominal pain, renal involvement). It is not strictly reticular but may have a livedoid component. The history (recent infection, drug, autoimmune disease) and the palpable purpuric papules distinguish it. [1]
Erythema multiforme
Erythema multiforme produces target lesions — three-zone concentric rings with a dusky central bulla or crust, a pale oedematous middle ring, and an erythematous outer ring. The lesions are typically on the extensor extremities, palms, soles, and mucous membranes. They are acute in onset (over 24 to 48 hours), often following a herpes simplex infection or drug exposure. They are not reticular, and the target morphology is distinctive. Stevens-Johnson syndrome / toxic epidermal necrolysis is the severe mucocutaneous variant. [1]
Contact dermatitis (allergic and irritant)
Contact dermatitis produces an eczematous, pruritic, sharply demarcated eruption corresponding to the area of contact with the allergen or irritant. Allergic contact dermatitis (e.g., nickel, fragrances, topical medications) shows vesicles, oozing, crusting, and lichenification in chronic cases. Irritant contact dermatitis (e.g., from a hot-water-bottle rubber, adhesives) shows burning and erythema. The key distinguishing features from EAI: contact dermatitis is pruritic, eczematous (not reticular), and sharply demarcated to the contact area (which may match the shape of the heat source but lacks the net-like pattern). [1]
Poikiloderma
Poikiloderma is a cutaneous reaction pattern combining atrophy, telangiectasia, and mottled hyper- and hypopigmentation ("the three As: atrophy, angiectases, and alteration in pigmentation"). It resembles late-stage EAI histologically and clinically. Causes include chronic radiation dermatitis (prior radiotherapy), autoimmune connective tissue disease (dermatomyositis, lupus), mycosis fungoides (large plaque parapsoriasis), and Rothmund-Thomson syndrome (hereditary). Late EAI is essentially a heat-induced poikiloderma. The history of heat exposure and the early reticular pattern (before atrophy dominates) distinguish EAI. [1]
Post-inflammatory hyperpigmentation
Post-inflammatory hyperpigmentation follows any inflammatory dermatosis (eczema, lichen planus, drug eruption, acne). It is diffuse or patchy, not reticular, and follows the distribution of the original inflammation. The history of a preceding rash distinguishes it. [1]
Fixed drug eruption
Fixed drug eruption produces a well-demarcated, round, reddish-purple to brown plaque that recurs at the same site with each exposure to the offending drug (NSAIDs, paracetamol, sulfonamides, tetracyclines, barbiturates, oral contraceptives). It may blister centrally. Multiple lesions may be present. The drug history, round morphology, and recurrence at the same site distinguish it. [1]
Solar lentigo and actinic damage
Solar lentigo ("liver spot", "age spot") is a flat, brown, well-demarcated macule on sun-exposed skin (face, dorsal hands, forearms) in elderly, fair-skinned individuals. It is not reticular. Actinic keratosis is a rough, scaly papule on sun-exposed skin — a premalignant lesion analogous to thermal keratosis. The distribution (sun-exposed vs heat-exposed) and morphology (single papule vs reticular net) distinguish. [1]
Addison's disease
Addison's disease (primary adrenal insufficiency) produces generalised hyperpigmentation — most prominent on sun-exposed areas, palmar creases, oral mucosa, recent scars, and pressure points. It is diffuse, not reticular, and is accompanied by fatigue, weight loss, hyponatraemia, hyperkalaemia, and hypotension. [1]
DDx of reticular pigmentation — the NETS
Clinical & Bedside Assessment
EAI is fundamentally a clinical diagnosis. The bedside assessment has two goals: (1) confirm the diagnosis by identifying the heat source and excluding mimics, and (2) search for the underlying reason the patient is seeking heat, which is often more important than the skin lesion itself. [1]
History
A structured history should cover: [1]
- Onset and duration: when was the lesion first noticed? How has it changed? (EAI evolves slowly over weeks to months.)
- Heat source identification — the single most important question. Ask specifically about:
- Laptop / tablet / gaming device use on the lap — hours per day, weeks of use, vent position.
- Heating pads — site, temperature setting, duration, frequency.
- Hot water bottle use — for what symptom (dysmenorrhoea, abdominal pain, back pain)?
- Heated car seats, electric blankets, space heaters, heated recliners.
- Occupational heat exposure (stoves, ovens, furnaces, glass).
- Sitting close to fires, radiators, or chulhas.
- Symptoms: asymptomatic is typical. Mild burning, pruritus, or paraesthesia may occur. New tenderness, bleeding, or non-healing in a chronic lesion suggests SCC.
- Underlying cause of heat-seeking behaviour: chronic pain (osteoarthritis, low back pain, fibromyalgia, endometriosis), cold intolerance (hypothyroidism, cachexia, anaemia), neurological disease (paraplegia, neuropathy), dementia, or domestic fuel poverty.
- Drug history: medications causing cold intolerance (beta-blockers), photosensitivity that might suggest alternative diagnoses, or drugs causing fixed drug eruption.
- Systemic review: weight loss, fatigue, cold intolerance, constipation, dry skin (hypothyroidism); night pain, weight loss, cachexia (malignancy).
- Past medical history: prior radiotherapy (radiation dermatitis); autoimmune disease (lupus, dermatomyositis); immunosuppression (organ transplant, HIV — risk of SCC). [1]
Examination
The blanching test
Diascopy (pressing a glass slide or clear plastic over the lesion) is the key bedside manoeuvre to distinguish EAI from livedo reticularis. Livedo reticularis blanches (the deoxygenated venous blood is pushed out of the constricted venules); EAI does not blanch (the haemosiderin and melanin are fixed in the dermis). This single test, combined with the heat-exposure history, usually confirms the diagnosis. [1]
Signs suggesting SCC within EAI
The following features in a longstanding EAI lesion mandate urgent biopsy:
- A new nodule, papule, or plaque within the area of EAI.
- Ulceration that does not heal.
- Induration or firmness on palpation.
- Tenderness or bleeding on minor trauma.
- Rapid growth or change in morphology.
- Regional lymphadenopathy. [1]
Investigations
EAI is a clinical diagnosis. Investigations are not required in the typical case — the triad of reticular hyperpigmentation, distribution matching a heat source, and a corroborating history is sufficient. Investigations are reserved for: [1]
- Atypical presentation (no clear heat source; rapid evolution; extensive distribution).
- Suspicion of underlying systemic disease (hypothyroidism, malignancy, autoimmune disease).
- Suspicion of SCC (new nodule, ulcer, induration in a chronic lesion).
- Diagnostic uncertainty — to exclude mimics such as vasculitis, fixed drug eruption, or poikiloderma of autoimmune disease. [1]
Skin biopsy
When biopsy is performed, the histopathological features of EAI vary with stage:[2]
- Epidermis: atrophy (thinning of stratum spinosum), basal layer vacuolar change, and dyskeratotic (atypical) keratinocytes with hyperchromatic, pleomorphic nuclei — the hallmark of thermal keratosis, which is histologically indistinguishable from actinic keratosis. Long-standing lesions may show full-thickness keratinocyte atypia (Bowen's disease / SCC in situ) or invasive SCC.
- Dermis: haemosiderin deposition in the upper dermis (positive on Prussian blue stain — distinguishes from melanin, which is negative on Prussian blue), melanophages (melanin-laden macrophages), telangiectasia of the superficial plexus, dermal elastosis (degeneration of collagen and elastic fibres resembling solar elastosis), and a mild perivascular lymphocytic infiltrate.
- Subepidermal bullae may be present in advanced disease (epidermal atrophy with detachment). [1]
When biopsy is mandatory
Biopsy is mandatory if any of the following are present:
- A new nodule, ulcer, induration, or non-healing erosion within an EAI lesion — to exclude SCC arising in thermal keratosis.
- Rapid change in a previously stable lesion.
- A lesion whose diagnosis is uncertain despite a careful history and examination. [1]
Other investigations
- TFTs (TSH, free T4) — if heat-seeking behaviour suggests hypothyroidism (cold intolerance, fatigue, constipation, dry skin, bradycardia).
- Full blood count, ferritin — if anaemia (causing constitutional coldness) is suspected.
- Autoimmune screen (ANA, ENA, ANCA, complement) — if poikiloderma raises suspicion of lupus or dermatomyositis.
- Coagulation / thrombophilia screen — if livedoid vasculopathy is in the differential (painful ulcers, atrophie blanche).
- Imaging (CT, MRI) — if cachexia, weight loss, or night pain suggests underlying malignancy driving heat-seeking behaviour.
- Dermoscopy — may show a network of brownish-grey structures corresponding to the damaged venous plexus, but is not diagnostic. [1]
Management — Resuscitation
EAI is not a dermatological emergency in the classic sense, but several scenarios require prompt attention. [1]
The single most important intervention
Eliminate the heat source. This is both the resuscitative and the definitive treatment — there is no pharmacological substitute. The earlier the heat source is removed, the more likely the lesion will resolve completely. Counsel the patient specifically: [1]
- Laptop: use a desk or lap desk; never place the laptop directly on bare skin; reduce daily lap-use time.
- Heating pad: reduce temperature setting and duration; place a towel between the pad and the skin; never fall asleep with the pad on.
- Hot water bottle: wrap in a cloth; never apply directly to skin; limit contact time.
- Heated car seat: use the lowest setting; turn off periodically.
- Space heater / fire: maintain at least one metre of distance; never sit directly beside the heat source for prolonged periods. [1]
Acute symptom management
- Mild pruritus or burning: a cool compress (water-soaked cloth) and emollient (petrolatum-based moisturiser) provide symptomatic relief while the heat source is removed.
- Topical corticosteroids are NOT indicated for EAI itself — they do not help and may mask early SCC if present. [1]
When to suspect a coexisting thermal burn
If the heat exposure was particularly intense or prolonged, examine for superimposed thermal burn (blistering, full-thickness necrosis, eschar) — particularly in patients with neurological impairment, neuropathy, or dementia who cannot report early discomfort. Burns require standard burn management (cooling, dressing, tetanus prophylaxis, referral if extensive). [1]
When to suspect and treat cellulitis
If the EAI area develops spreading erythema, warmth, swelling, pain, fever, or systemic symptoms, treat as cellulitis (most often Staphylococcus aureus or beta-haemolytic streptococci): [1]
- Oral antibiotics: flucloxacillin 500 mg four times daily for 5 to 7 days (or cephalexin 500 mg four times daily); clindamycin if penicillin-allergic; consider MRSA cover (doxycycline, vancomycin in severe cases) if risk factors. [1]
When SCC is suspected
If a chronic EAI lesion has a new nodule, ulcer, induration, or non-healing erosion, this is a 2-week-wait / urgent dermatology referral for biopsy and definitive management of SCC. Do NOT delay for "watchful waiting." [1]
Management — Definitive & Stepwise
The management of EAI is built on three pillars: (1) eliminate the heat source (primary, mandatory, always); (2) treat the hyperpigmentation and keratoses (topical retinoids, hydroquinone, 5-fluorouracil); and (3) monitor for and treat SCC (biopsy, excision). Counselling and prevention are at least as important as pharmacological treatment. [1]

Step 1: Eliminate the heat source (primary, mandatory)
This is the single most effective intervention for EAI. Without it, no pharmacological treatment will succeed.[1][3]
Specific counselling points: [1]
- Laptop-induced EAI: stop using the laptop on the lap. Use a desk or a lap desk (a flat, insulated surface placed between the laptop and the thighs). Avoid prolonged use; take breaks. Modern gaming laptops with high-performance GPUs run particularly hot — counsel explicitly.
- Heating pad EAI: reduce the temperature setting, reduce duration (no overnight use), and place a towel or cloth between the pad and the skin. Treat the underlying pain (see Step 5).
- Hot water bottle EAI: never apply directly to skin; wrap in a cloth; limit to 15 to 20 minutes per session.
- Heated car seat: use the lowest setting; turn off periodically on long drives.
- Occupational EAI: work with occupational health to modify the work environment (heat shields, distance from radiant heat, rotating tasks, protective clothing).
- Open fire / stove / heater: maintain at least one metre of distance; sit to the side rather than directly facing the heat. [1]
Step 2: Treat hyperpigmentation (topical retinoids and adjuncts)
After heat removal, residual hyperpigmentation may take months to fade and may never fully resolve. [1]
| Agent | Concentration | Frequency | Duration | Rationale |
|---|---|---|---|---|
| Tretinoin (topical retinoid) | 0.025 to 0.05 per cent cream | Once daily at night | 3 to 6 months | Increases epidermal cell turnover, redistributes melanin, may fade pigmentation |
| Adapalene (third-generation retinoid) | 0.1 per cent gel | Once daily at night | 3 to 6 months | Better tolerated than tretinoin; useful for sensitive skin |
| Hydroquinone (bleaching agent) | 2 to 4 per cent cream | Once or twice daily | 2 to 4 months (max 6 months) | Inhibits tyrosinase, reduces melanin synthesis; for persistent pigmentation |
| Triple combination cream (hydroquinone 4%, tretinoin 0.025%, fluocinolone 0.01%) | — | Once daily at night | Up to 8 weeks | For refractory pigmentation; the corticosteroid reduces inflammation; monitor for steroid side effects |
| Kojic acid, azelaic acid, vitamin C, niacinamide | various | Once or twice daily | Long-term | Adjunctive skin-lightening agents; gentler than hydroquinone |
Sun protection is essential — UV exposure will deepen any residual hyperpigmentation. Counsel daily use of broad-spectrum sunscreen SPF 30 or higher, even on cloudy days. [1]
Step 3: Treat thermal keratosis (topical 5-fluorouracil)
If biopsy confirms thermal keratosis (atypical keratinocytes in a keratotic plaque within the EAI area), the standard field-therapy agent is topical 5-fluorouracil (5-FU), identical to its use in actinic keratosis:[2]
- 5-fluorouracil 5 per cent cream applied twice daily for 2 to 4 weeks to the affected area. The lesion will become inflamed, eroded, and crusted (this is the expected reaction — it indicates death of the dysplastic keratinocytes). Healing occurs over 2 to 4 weeks after cessation.
- Imiquimod 5 per cent cream applied 2 to 3 times per week for 4 to 16 weeks is an alternative immune-response modifier.
- Cryotherapy with liquid nitrogen is appropriate for isolated, focal keratoses.
- Photodynamic therapy (PDT) with aminolaevulinic acid (ALA) or methyl aminolaevulinate (MAL) is an option for field therapy of multiple keratoses. [1]
Step 4: Treat SCC (biopsy and surgical excision)
If a new nodule, ulcer, induration, or non-healing erosion within an EAI lesion suggests SCC, urgent biopsy and surgical referral are required:[2]
- Incisional or excisional biopsy of the suspicious area — confirm SCC histologically (invasive atypical squamous epithelium infiltrating the dermis).
- Surgical excision with a 4 to 6 mm margin for low-risk SCC (less than 2 cm diameter, well-differentiated, less than 2 mm depth) — the standard of care.
- Mohs micrographic surgery for high-risk SCC (face, ears, periocular, perinasal, large, deeply invasive, poorly differentiated, recurrent) — to maximise margin clearance while sparing tissue.
- Regional lymph node dissection if nodal metastasis is suspected (clinically or on imaging).
- Radiotherapy for inoperable tumours or patients unfit for surgery. [1]
Step 5: Treat the underlying cause of heat-seeking behaviour
EAI is frequently a cutaneous clue to an underlying treatable condition. Always investigate and address the reason the patient seeks heat: [1]
- Chronic pain (osteoarthritis, low back pain, fibromyalgia, endometriosis): refer to pain management, rheumatology, or gynaecology; optimise analgesia, physiotherapy, intra-articular injections, or surgical options.
- Hypothyroidism: check TSH and free T4; treat with levothyroxine (typical starting dose 1.6 micrograms per kg daily, titrated to TSH).
- Cachexia / weight loss / malignancy: investigate with imaging, tumour markers, and tissue diagnosis; refer to oncology.
- Neurological disease (paraplegia, stroke): occupational therapy review of positioning and protective devices.
- Domestic fuel poverty: refer to social services. [1]
Step 6: Long-term follow-up
Patients with chronic EAI of over 5 years' duration, or with confirmed thermal keratosis, should be enrolled in long-term dermatological surveillance for SCC — analogous to actinic keratosis surveillance. Re-examine every 6 to 12 months; educate the patient on self-examination and "red flag" features (new nodule, ulcer, induration, bleeding) that mandate urgent review. [1]
Specific Subtypes & Scenarios
Laptop-induced EAI (the modern epidemic)
Demographics: young adults (15 to 35 years), students, IT professionals, gamers. Slightly more common in women. [1]
Distribution: anterior thighs, often bilateral, with a rectangular geometric border corresponding to the laptop base. May extend to the lower abdomen if the laptop is large. [1]
Causative factors: ventilation fan exhaust, battery heat, GPU/CPU heat generation. Modern gaming laptops with discrete GPUs and high-performance cooling fans run particularly hot and produce EAI faster. [1]
Management: counsel on lap desk / desk use; never place the laptop directly on bare skin; take breaks. Topical retinoids for residual pigmentation. [1]
Prognosis: early lesions resolve with heat removal; chronic lesions may leave residual pigmentation. SCC risk is low because most laptop users reduce exposure once the diagnosis is made.[4]
Heating pad EAI (chronic pain subtype)
Demographics: elderly patients with chronic low back pain, osteoarthritis, fibromyalgia, post-surgical pain, or chronic pelvic pain. [1]
Distribution: lower back (lumbosacral), often with a curved border corresponding to the heating pad shape. May be unilateral (single pad) or bilateral. [1]
Causative factors: heating pad set to medium or high, used daily for weeks to months, often overnight. [1]
Management: reduce pad temperature and duration; place a towel between pad and skin; never sleep with the pad on. Critically, treat the underlying pain — physiotherapy, NSAIDs, intra-articular steroid injection, neuropathic agents, or surgical referral. Without pain control, the patient will not stop using the pad. [1]
Prognosis: SCC risk is higher than laptop-induced EAI because the same chronic pain patient often continues using the pad for years. Vigilant surveillance is essential. [1]
Hot water bottle EAI (dysmenorrhoea subtype)
Demographics: young women with primary dysmenorrhoea, endometriosis, adenomyosis, or chronic pelvic pain. [1]
Distribution: lower abdomen (hypogastrium), with a curved border corresponding to the bottle. [1]
Management: wrap the bottle in cloth; limit contact time; treat the underlying gynaecological condition (NSAIDs, combined oral contraceptive, levonorgestrel IUS, laparoscopic management of endometriosis). [1]
Occupational EAI (cooks, bakers, glassblowers, foundry workers)
Demographics: middle-aged workers in food preparation, metalworking, glassworking, and welding. [1]
Distribution: forearms, dorsal hands, face, neck — the parts nearest the radiant heat. Often bilateral and symmetric. [1]
Management: occupational health referral is essential. Interventions include heat shields, long-sleeved flame-retardant protective clothing, gloves, face shields, rotating tasks, and reducing proximity to the heat source. The lesion itself is treated as above; the underlying exposure must be addressed through workplace modification.[1]
Paediatric EAI
Demographics: children and adolescents using laptops, tablets, gaming devices, or heated blankets; sometimes from sitting close to heaters in cold rooms. [1]
Distribution: anterior thighs, lower legs, abdomen — depending on the source. [1]
Diagnosis pitfalls: paediatric EAI is frequently misdiagnosed as child abuse (bruising), Mongolian spot, café-au-lait macule, or fixed drug eruption. The fixed, reticular, brownish-purple pattern with a heat-exposure history distinguishes EAI. Multidisciplinary evaluation may be required to exclude non-accidental injury if the history is inconsistent. [1]
Management: parental counselling on device use (lap desk, breaks), heat source elimination, and topical retinoids for residual pigmentation.[5]
EAI in hypothyroidism and malignancy
When EAI is found without an obvious external heat source, consider an underlying systemic driver: [1]
- Hypothyroidism: cold intolerance drives the patient to sit close to heaters or layer heated blankets. Check TSH and free T4; treat with levothyroxine. The EAI will fade only after euthyroidism is restored and heat-seeking behaviour ceases.
- Malignancy with cachexia: constitutional coldness and weight loss drive heat-seeking. Investigate for occult cancer (lung, GI, haematological); EAI may be an early clue.
- Anaemia: chronic anaemia causes constitutional coldness; check FBC and ferritin. [1]
Complications & Pitfalls
Complications
- Squamous cell carcinoma — the most serious complication. SCC arises in thermal keratosis within long-standing (over 5 years, often over 10 to 30 years) EAI lesions. Reported in case series and case reports; the absolute risk is small but real. Any new nodule, ulcer, or induration within an EAI lesion must be biopsied.[2]
- Permanent hyperpigmentation and atrophy — stage 3 changes (atrophy, telangiectasia, mottled pigmentation) are permanent and do not improve with treatment.
- Thermal burn — if the heat exposure was particularly intense (especially in neuropathic or demented patients), a coexisting full-thickness burn may be present.
- Cellulitis — fissured, atrophic skin is a portal of entry for Staphylococcus aureus and streptococci.
- Psychological distress — the cosmetic change (especially in young women with thigh EAI) can cause significant distress; address explicitly.
- Missed underlying disease — EAI is a sentinel sign; failure to investigate the underlying cause of heat-seeking (hypothyroidism, malignancy, chronic pain) is a major pitfall.
Pitfalls
Pitfalls in EAI — the BURN mnemonic
Other pitfalls:
- Misdiagnosis as bruising / child abuse in paediatric EAI — the fixed, reticular pattern and heat history distinguish EAI.
- Misdiagnosis as livedo reticularis — livedo blanches, EAI does not.
- Failure to counsel on prevention — patients will relapse unless the heat source behaviour changes.
- Over-reassurance of chronic EAI as a "cosmetic problem" — the SCC risk mandates long-term surveillance. [1]
Prognosis & Disposition
Prognosis
The prognosis of EAI depends on the stage at which the heat source is eliminated:[1][3]
- Stage 1 (early erythema): fully reversible within days to weeks of heat removal. No residual pigmentation.
- Stage 2 (reticular hyperpigmentation): slowly improves over months. May leave residual permanent pigmentation, particularly in darker-skinned individuals.
- Stage 3 (late atrophic / keratotic): permanent changes. Atrophy, telangiectasia, and mottled pigmentation do not resolve. Thermal keratosis requires active treatment (5-FU, cryotherapy, PDT) and long-term surveillance for SCC. [1]
Predictors of malignant transformation
The following factors increase the risk of SCC arising in EAI:
- Duration: chronic EAI of over 5 years, particularly over 10 to 30 years.
- Thermal keratosis on biopsy.
- Late-stage atrophic changes.
- Immunosuppression (organ transplant, HIV, chronic corticosteroid use).
- Coexisting UV damage on sun-exposed sites (additive carcinogenic effect). [1]
Disposition
- Primary care / general practice: most cases are managed here with heat source elimination, topical retinoids, and patient education.
- Dermatology referral: for atypical presentation, diagnostic uncertainty, suspected thermal keratosis, or long-term surveillance of chronic EAI.
- Surgical / plastics referral: for biopsy and excision of confirmed SCC.
- Rheumatology / pain management / gynaecology referral: to treat the underlying cause of heat-seeking behaviour (chronic pain, endometriosis).
- Endocrinology referral: for management of hypothyroidism if identified.
- Occupational health referral: for workplace modification in occupational EAI. [1]
Follow-up
Patients with chronic EAI (over 5 years), confirmed thermal keratosis, or stage 3 changes should be reviewed every 6 to 12 months indefinitely for SCC surveillance. Educate on self-examination and red-flag features. [1]
Special Populations
Evidence, Guidelines & Regional Differences
Guidelines
There is no single international guideline for EAI management. Practice is based on narrative reviews, expert opinion, and the principles of actinic keratosis management applied to thermal keratosis. Key consensus statements:[1]
- British Association of Dermatologists — recommends heat source elimination as the primary intervention; topical retinoids for residual hyperpigmentation; biopsy of any suspicious lesion to exclude SCC; topical 5-FU for thermal keratosis.
- American Academy of Dermatology — emphasises laptop and heated car seat avoidance in young adults; sun protection; long-term follow-up of chronic EAI for SCC.
- NICE Clinical Knowledge Summaries (UK) — provides primary-care guidance on identification and counselling; dermatology referral for atypical or chronic lesions. [1]
Evidence base
The evidence base for EAI treatment is limited — most evidence is from case reports, case series, and narrative reviews, with no randomised controlled trials:[1]
- Harview and Krenitsky (2023) — a comprehensive clinical review synthesising modern literature; concluded that heat source elimination remains the primary intervention, with topical retinoids for hyperpigmentation and biopsy of any suspicious lesion. Limited evidence for 5-FU, imiquimod, and PDT in thermal keratosis.[1]
- Wilder and colleagues (2021) — reviewed malignant transformation to SCC; concluded that the risk is small but real, particularly with chronic (over 5 to 10 years) EAI, and that biopsy of any suspicious lesion is mandatory. Thermal keratosis is histologically indistinguishable from actinic keratosis.[2]
- Küçüktaş and colleagues (2010) — early case series of laptop-induced EAI; established the modern epidemiology.[4]
- Poddighe and colleagues (2023) — reviewed paediatric EAI; emphasised the rising incidence with gaming device use and the diagnostic pitfalls (child abuse, Mongolian spot).[5]
Controversies
- Role of topical retinoids — evidence is largely empirical; no RCTs. Most clinicians use them for residual hyperpigmentation with variable results.
- Role of laser therapy — Q-switched ruby laser, intense pulsed light (IPL), and fractional lasers have been reported in small case series for refractory pigmentation; results are variable and not first-line.
- Frequency of SCC surveillance — no consensus on interval; most authorities recommend 6 to 12 monthly review for chronic EAI with keratoses.
- Whether thermal keratosis warrants prophylactic 5-FU — some authorities recommend field therapy to all thermal keratoses (analogous to actinic keratosis); others reserve 5-FU for biopsy-confirmed dysplasia. [1]
Exam Pearls
[1]Red flags
Exam application bank (NEET-PG / INICET)
One-line answer
Erythema ab igne (EAI, toasted skin syndrome) is a localised cutaneous reaction caused by chronic, repeated exposure to moderate heat — insufficient to cause a thermal burn but enough to damage the superficial dermal vasculature — producing a characteristic reticulated (net-like), brownish-purple hyperpigmentation on the heat-exposed skin. Modern causes include laptop computers on the lap, heating pads, hot water bottles, heated car seats, space heaters, electric blankets, and open fires. Histology may mimic actinic keratosis (atypical keratinocytes — 'thermal keratosis'). Long-standing lesions carry a small but real risk of malignant transformation to squamous cell carcinoma. Management: remove the heat source (primary and most effective intervention); topical retinoids for hyperpigmentation; topical 5-fluorouracil for thermal keratosis; excision for SCC.
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard. [1]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes. [1]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change. [1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each. [1]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory. [1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Erythema ab igne.
[1]References
- [1]Harview CL, Krenitsky A. Erythema Ab Igne: A Clinical Review Cutis, 2023.PMID 37289686
- [2]Wilder EG, Frieder JH, Menter MA. Erythema Ab Igne and Malignant Transformation to Squamous Cell Carcinoma Cutis, 2021.PMID 33651859
- [3]Takahashi TA, Yuh Asukai I, et al. Erythema ab igne Dermatol Online J, 2011.PMID 22031654
- [4]Küçüktaş M, Demirkesen C, Aslan C, Aydemir EH. Laptop-induced erythema ab igne Clin Exp Dermatol, 2010.PMID 20089079
- [5]Poddighe D, Assylbekova M, Almukhamedova Z, Aman A, Mukusheva Z. Pediatric erythema ab igne: clinical aspects and diagnostic issues Eur J Pediatr, 2023.PMID 37661206