Dermatology · Medicine
Erythema nodosum
Also known as Erythema nodosum (EN) · Septal panniculitis · Subacute nodular migratory panniculitis
Erythema nodosum (EN) is an acute septal panniculitis — the commonest panniculitis. Clinical: bilateral, symmetric, tender, erythematous subcutaneous nodules on the anterior shins; NO ulceration, NO scarring (resolves like a bruise: red then purple then brown). Self-limiting over two to six weeks. Causes (screen for ALL): streptococcal infection (most common in children), sarcoidosis (Lofgren syndrome: EN plus bilateral hilar lymphadenopathy plus ankle arthritis; excellent prognosis), inflammatory bowel disease (Crohn's more often than UC), drugs (oral contraceptive pill, sulphonamides, penicillins, bromides), pregnancy, and other infections (TB, histoplasmosis, coccidioidomycosis, Yersinia, Chlamydia). About 30 to 50 percent remain idiopathic. Histology: septal panniculitis (thickened inflamed septa; lobules spared; Miescher radial granulomas; no vasculitis). Management: treat the underlying cause first; bed rest and leg elevation; NSAIDs; potassium iodide, colchicine or hydroxychloroquine for refractory disease.
On this page & tools
Your progress
Saved locally on this device.
Exam tags
Red flags

Overview and Definition
Erythema nodosum (EN) is an acute, reactive, septal panniculitis — a delayed-type hypersensitivity reaction expressed in the connective-tissue septa that divide the subcutaneous fat into lobules. The fat lobules themselves are spared, and the overlying epidermis is normal. It is, by a wide margin, the commonest form of panniculitis encountered in clinical practice.[1][3]
Clinically it declares itself as crops of bilateral, symmetric, tender, erythematous, subcutaneous nodules, classically on the anterior (pretibial) shins. The defining behaviours that separate EN from every other nodular eruption of the legs are three: the nodules never ulcerate, they never scar, and they evolve through a bruise-like colour sequence (bright red, then purple, then brownish-yellow) before flattening over two to six weeks.[1]
Crucially, EN is not a primary disease of skin. It is a cutaneous alarm signal — a stereotyped cutaneous response to a remote antigenic stimulus. The workup, prognosis and management are therefore dominated not by the skin lesions themselves (which are self-limiting) but by identifying the trigger: streptococcal pharyngitis, sarcoidosis, inflammatory bowel disease, a drug, pregnancy, or one of a long list of infections. In roughly a third to a half of patients no cause is found despite a complete workup, and these are labelled idiopathic.[1]
[1]Classification
EN does not have named subtypes in the way lupus or vasculitis do, but it sits within a classification of panniculitis that every candidate must be able to draw: the divide between septal and lobular panniculitis, and whether vasculitis is present. This single frame organises the entire differential of "tender leg nodules".[3]
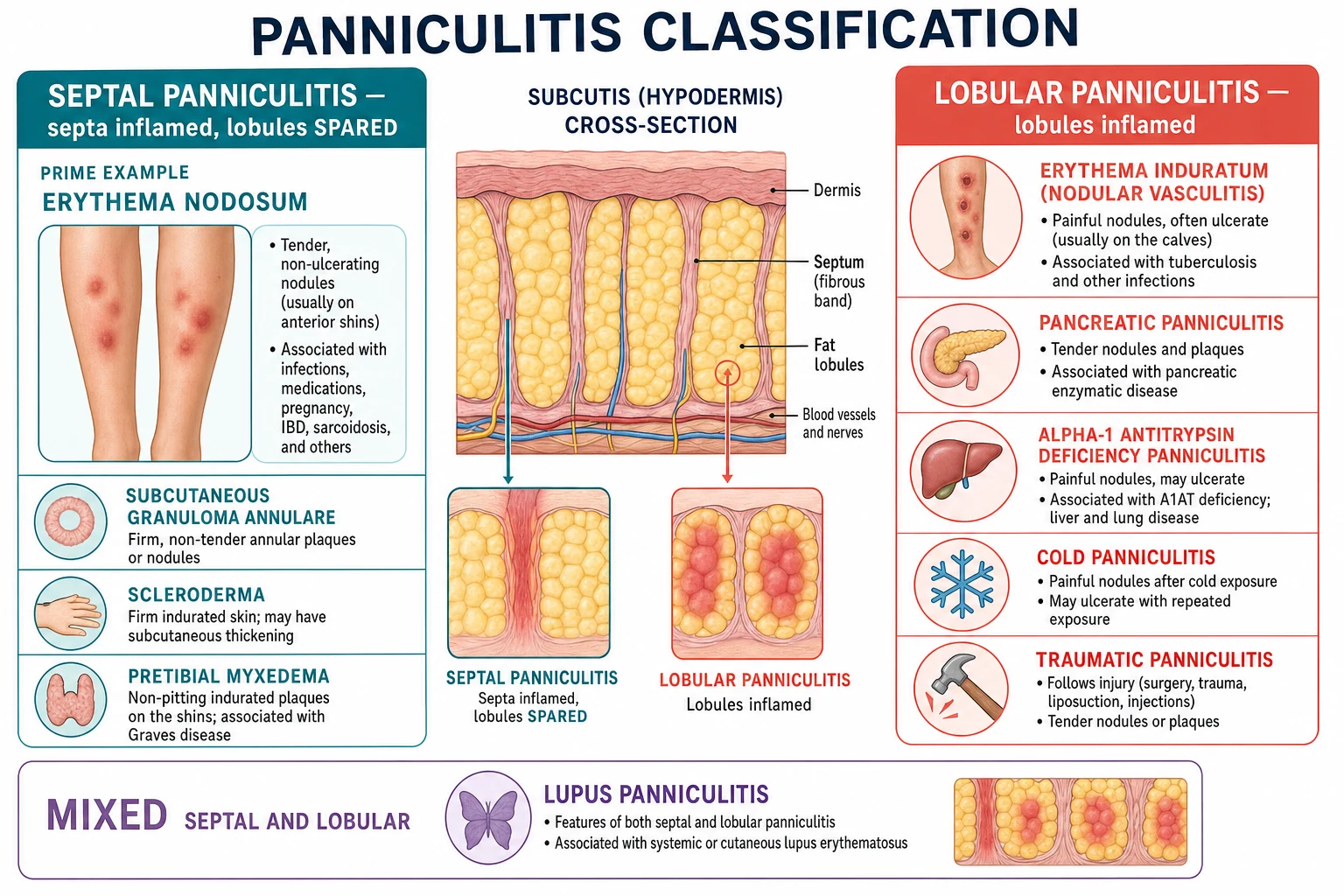
SEPTAL panniculitis (EN prototype)
LOBULAR panniculitis
MIXED septal + lobular
A clinically useful variant worth naming is subacute nodular migratory panniculitis (migratory subcutaneous nodules that enlarge and coalesce, usually unilateral, often following minor trauma or streptococcal infection, responding well to potassium iodide). Some authors regard it as a unilateral or migratory forme fruste of EN rather than a separate disease.[1]
Epidemiology and Risk Factors
EN is uncommon but not rare, with an estimated incidence of one to five cases per 100,000 person-years. It is overwhelmingly a disease of young adults, peaking between the second and fourth decades (20-40 years), and it has a striking female predominance of roughly three to five to one — a sex skew shared with most autoimmune and reactive dermatoses.[1]
Risk factors are simply the triggers themselves. Anything that elicits a brisk cell-mediated immune response in a genetically susceptible host can precipitate EN: a recent streptococcal pharyngitis (the single most common identifiable cause in children), oral contraceptive use, pregnancy and the postpartum state, established or occult inflammatory bowel disease, and exposure to endemic fungi or mycobacteria.[1][3]
The cause profile shifts with age and geography. In children, group A streptococcal pharyngitis dominates. In young adults, sarcoidosis (Lofgren syndrome) and IBD rise in importance. In TB-endemic regions (much of South Asia and sub-Saharan Africa), tuberculosis and the BCG vaccine are prominent precipitants, while in the American Southwest the endemic mycosis coccidioidomycosis ("valley fever") is a leading cause, and in the Ohio and Mississippi river valleys histoplasmosis heads the list.[1]
Pathophysiology
EN is a type IV (cell-mediated, delayed) hypersensitivity reaction unfolding in the subcutaneous septa, with a contributing immune-complex component. A remote antigen — streptococcal M protein, mycobacterial antigen, a drug hapten, a fungal antigen, or an as-yet-uncharacterised sarcoidal antigen — is presented to antigen-specific T lymphocytes within the fat. The resulting cytokine cascade recruits neutrophils, then lymphocytes and histiocytes, and finally organises into granulomas, all concentrated in the connective-tissue septa between fat lobules. The lobular adipocytes are largely bystanders and are spared.[1][3]

The histological tempo mirrors this. Early lesions (first 24-72 hours) show septal oedema and a neutrophilic infiltrate. Established lesions show thickened septa infiltrated by lymphocytes, histiocytes and multinucleated giant cells. Late lesions may be frankly granulomatous. The histological hallmark — Miescher radial granulomas — are small, tight knots of histiocytes (and occasionally neutrophils) arranged radially around a central cleft or small vessel within a septum. They are characteristic of EN but, importantly, are not pathognomonic (they can appear in other conditions), and their absence does not exclude EN.[1][3] At the molecular level the reaction is driven by a TH1-polarised cytokine milieu — interleukin-2, interferon-gamma and tumour necrosis factor-alpha (TNF-alpha) — which activates macrophages, upregulates adhesion molecules on septal venules, and recruits the waves of neutrophils and mononuclear cells seen histologically. Circulating immune complexes deposit in septal vessels, generating a brisk complement cascade (C3a, C5a) that amplifies neutrophil recruitment; the combination of cell-mediated and immune-complex injury localised to the septa is what produces the dense, band-like infiltrate that characterises EN. Two clinical observations fall out of this mechanism. First, TNF-alpha is central, which is why anti-TNF agents (infliximab, adalimumab, etanercept) are highly effective for EN refractory to standard therapy. Second, and paradoxically, the same anti-TNF agents can themselves precipitate EN as a paradoxical drug reaction — a favourite examination wrinkle that resolves the apparent contradiction between "anti-TNF treats EN" and "anti-TNF causes EN".[1][3]
The most pathologically and prognostically important negative is that blood vessels are intact: there is no vasculitis, no fibrinoid necrosis of vessel walls, no leucocytoclasia. This single fact — septal inflammation without vasculitis — is what separates EN from erythema induratum (nodular vasculitis), where a lobular panniculitis with vasculitis produces nodules that ulcerate, scar and recur. It also explains why EN is self-limiting and benign: the tissue architecture is preserved, and once the antigenic stimulus is cleared or withdrawn, the reaction resolves without a trace.[3] This vascular integrity also explains why EN does not cause the livedo, necrosis, neuropathy or digital infarction that accompany a true vasculitic panniculitis such as cutaneous polyarteritis nodosa. The clinician at the bedside should therefore look specifically for these "vasculitic companions" — livedo reticularis, a mononeuritis, ulceration, or necrosis — because their presence immediately reclassifies the eruption away from EN and toward a vasculitic or lobular process requiring a very different workup.[3]
A genetic background modulates susceptibility and outcome. The best-characterised association is with the HLA-DRB1*03 allele, which is strongly linked to the Lofgren syndrome phenotype of sarcoidosis and predicts a favourable prognosis (spontaneous resolution within two years).[4][8]
Causes: the differential diagnosis of the trigger
Because EN is a reactive pattern, "the diagnosis of EN" is never complete until the trigger has been named or excluded. The mnemonic below ties the cause categories to the very site EN favours — the SHINS. [1]
SHINS

The table below ranks the causes and pairs each with the single highest-yield investigation. [1]
| Cause category | Relative frequency | Single highest-yield test |
|---|---|---|
| Streptococcal infection (group A) | Most common identifiable cause, especially in children | ASO titre plus throat swab; lesion appears 1-3 weeks after pharyngitis |
| Sarcoidosis | Common in young adults; Lofgren syndrome | Chest X-ray for bilateral hilar lymphadenopathy |
| Inflammatory bowel disease | Crohn more often than UC; parallels gut activity | Stool calprotectin; colonoscopy if GI symptoms |
| Drugs | OCP, sulphonamides, penicillins, bromides, iodides, TNF inhibitors | Thorough drug history; withdrawal and rechallenge |
| Pregnancy | Hormonal; postpartum also reported | Pregnancy test in any woman of reproductive age |
| Tuberculosis | Prominent in TB-endemic regions; BCG vaccine | IGRA (or Mantoux) plus chest X-ray and sputum if cough |
| Endemic mycoses | Coccidioidomycosis (US Southwest), histoplasmosis (Ohio/Mississippi), blastomycosis | Fungal serology / antigen; chest X-ray; travel and exposure history |
| Other infections | Yersinia, Salmonella, Campylobacter, Chlamydia, Mycoplasma, hepatitis B, EBV | Stool culture/serology directed by GI or respiratory symptoms |
| Behcet disease | EN-like nodules (a vasculitis mimic) | History of recurrent oral aphthae plus genital ulcers plus uveitis |
| Malignancy (rare) | Hodgkin / non-Hodgkin lymphoma, leukaemia | Lymph node biopsy, CBC with film, LDH |
| Idiopathic | 30-50% after a complete workup | A diagnosis of exclusion — implies the workup was thorough |
Lofgren syndrome (acute sarcoidosis)
The single most important cause-pattern to recognise at the bedside is Lofgren syndrome: the triad of erythema nodosum plus bilateral hilar lymphadenopathy plus ankle arthritis or peri-arthritis (often with fever). It is an acute presentation of sarcoidosis with an outstanding prognosis — most patients resolve within two years without specific therapy — and is strongly associated with HLA-DRB1*03.[4][8] When the full triad is present the diagnosis is clinical and no biopsy is required: the combination is specific enough that tissue confirmation adds risk without benefit. A non-caseating granuloma on biopsy would be confirmatory but is not necessary. This is a favourite viva point because it is one of the few situations in dermatology where the diagnosis is made by a chest X-ray and clinical pattern rather than by skin biopsy.[4]
Clinical Presentation
The onset is acute. Over hours to a few days, crops of bilateral, symmetric, tender, erythematous nodules appear, most often on the anterior shins (pretibial region) — the dependent, relatively immobile subcutis overlying the tibia. Individual nodules measure 1 to 5 cm, are deeply situated in the subcutaneous fat (so their borders may be poorly demarcated), and are warm, firm and exquisitely tender. They never break the surface and never suppurate.[1]
A typical patient reports the following evolution. First come prodromal symptoms one to three weeks before the nodules: fever, malaise, and an arthralgia (especially of the ankles and knees) that may precede the skin lesions by several days and occurs in roughly half of patients. Then the nodules erupt bilaterally. Each individual lesion then runs a stereotyped colour evolution over one to two weeks — bright red, deepening to purple, then fading through brown and yellow-green — exactly like a resolving bru. The nodules flatten and disappear over two to six weeks leaving no ulceration and no scar. New crops may appear for several weeks if the trigger persists.[1]
Natural history of a single erythema nodosum lesion
Distribution beyond the shins. Less commonly the nodules appear on the thighs, forearms, and (rarely) the trunk or face. Bilateral shin involvement is so characteristic that a strictly unilateral distribution should prompt reconsideration of the diagnosis (trauma, insect bite, superficial thrombophlebitis, localised infection).[1]
Atypical and tricky presentations that examiners probe deliberately: [1]
- Lofgren triad without a throat complaint — EN plus ankle arthritis plus a clear chest X-ray that the candidate must remember to scrutinise for bilateral hilar lymphadenopathy.
- EN as the first manifestation of occult IBD — a patient with EN plus loose stools, abdominal pain or rectal bleeding may have undiagnosed Crohn disease; EN frequently parallels intestinal disease activity and may flare before a clinical relapse.[2][5]
- EN in pregnancy or the puerperium — may be the only clue; resolve with symptomatic care, avoiding NSAIDs late in pregnancy and any drug contraindicated in lactation.
- Recurrent EN in Behcet disease — the nodules of Behcet are histologically an EN-like septal panniculitis or vasculitis; the discriminating features are recurrent oral and genital aphthae, uveitis, and a positive pathergy test.[6]
- Childhood EN — almost always streptococcal; Bartonella (cat-scratch) and Yersinia are additional paediatric considerations.
Constitutional symptoms — low-grade fever, fatigue, malaise — accompany roughly half of cases and reflect the underlying systemic trigger rather than the skin itself. Hilar lymphadenopathy with cough points to sarcoidosis; diarrhoea and abdominal pain point to IBD or Yersinia; a productive cough and weight loss in an endemic-area patient demand exclusion of tuberculosis before any corticosteroid is contemplated.[1]
Differential Diagnosis
The differential of "tender nodules on the legs" is wide, but the single most examined discriminator is EN versus erythema induratum (nodular vasculitis). Get this comparison right and the rest follows.[3]

Erythema nodosum
Erythema induratum (nodular vasculitis)
The broader differential and the features that separate each: [1]
- Nodular vasculitis / erythema induratum — calves, ulcerates, lobular panniculitis with vasculitis, TB-associated. The contrast above settles it.
- Cutaneous polyarteritis nodosa — painful nodules on the lower legs with livedo reticularis and a sensory or motor neuropathy; a medium-vessel vasculitis localised to skin. Biopsy shows neutrophilic vasculitis at the dermal-subcutaneous junction.
- Superficial migratory thrombophlebitis — tender linear cord-like induration along the course of a superficial vein (often the great saphenous); associated with varicose veins, intravenous cannulae, occult malignancy (Trousseau) or Behcet.
- Insect bites / hypersensitivity — usually unilateral, intensely itchy, with a visible punctum; resolve with topical steroid.
- Subcutaneous granuloma annulare (children, rheumatoid-factor-negative) — painless or mildly tender nodules, often on the feet and hands rather than shins; biopsy shows palisading granulomas with mucin.
- Nodular scabies or pre-tibial myxedema — distinguished by context and distribution.
- Cutaneous lymphoma / leukaemia cutis / metastatic deposits — if nodules are persistent, atypical in distribution, or refractory, biopsy is mandatory; subcutaneous panniculitis-like T-cell lymphoma is the rare but dangerous mimic (fever, cytopenia, haemophagocytic syndrome).[3]
Clinical and Bedside Assessment
The skin itself tells most of the story. Examine the lesions in good light, palpate them (deep, tender, non-fluctuant, non-ulcerated), and document the colour evolution of each crop — the presence of lesions at different stages (red, purple, brown simultaneously) is itself diagnostic of EN. Then move systematically away from the skin to hunt the trigger, because that is where the diagnosis lives.[1]
A focused bedside assessment for the underlying cause: [1]
- Throat — exudate, cervical lymphadenopathy (recent streptococcal pharyngitis).
- Chest — auscultation and a chest X-ray (sarcoidosis, TB, fungal, bacterial pneumonia).
- Abdomen — tenderness, mass, perianal disease (Crohn); hepatosplenomegaly.
- Joints — ankles, knees, wrists (arthralgia of EN itself; also Lofgren and IBD-associated arthritis).
- Eyes — uveitis (sarcoidosis, IBD, Behcet).
- Genital and oral mucosa — recurrent aphthae and genital ulceration (Behcet).[6]
- Skin elsewhere — erythema multiforme-like target lesions, livedo, necrosis (alternative diagnoses).
The Lofgren triad should be confirmed or refuted at the bedside: bilateral tender shin nodules plus tender ankles plus a chest X-ray reporting bilateral hilar lymphadenopathy. When all three are present, the diagnosis is made and no biopsy is required.[4]
Investigations
Investigation has two aims: to confirm the cutaneous diagnosis when atypical, and — more importantly — to find the trigger. In a classic case (bilateral tender shin nodules with the expected colour evolution) the clinical diagnosis is secure and skin biopsy is not mandatory; investigation effort goes into the cause. Biopsy is reserved for atypical, ulcerating, persistent, recurrent, or immunosuppressed presentations.[1]

Skin biopsy (deep incisional or punch, including subcutaneous fat)
A punch biopsy that does not reach the subcutaneous fat is useless — it will show normal epidermis and dermis and miss the panniculitis entirely. Always specify that subcutaneous fat is required, and favour an incisional or wedge biopsy for a deep nodule. Histology shows:[1][3]
- Septal panniculitis — thickened, inflamed connective-tissue septa.
- Lobular sparing — adipocytes preserved.
- Evolving inflammatory infiltrate — neutrophils early, then lymphocytes and histiocytes, then granulomas with multinucleated giant cells.
- Miescher radial granulomas — radial collections of histiocytes around a central cleft within a septum; characteristic but not pathognomonic.
- NO vasculitis — vessels intact; the critical negative that separates EN from erythema induratum.
- No necrosis, no caseation (distinguishes from infectious panniculitides; stains and tissue culture for AFB and fungi if any concern). [1]
Cause-directed workup
In every patient, perform at minimum the core panel: a chest X-ray (sarcoidosis, TB, fungal, bacterial), an ASO titre and throat swab (streptococcal), a careful drug history including over-the-counter and the oral contraceptive pill, and a pregnancy test in any woman of reproductive age. Add directed tests as the history demands.[1]
| Test | Looking for | When to order |
|---|---|---|
| Chest X-ray | Bilateral hilar lymphadenopathy (sarcoidosis), TB, fungal, pneumonia | Every patient — one of the highest-yield single tests |
| ASO titre + throat swab | Group A streptococcal pharyngitis | Children; any recent sore throat |
| Drug history (incl. OCP) | Drug trigger | Every patient |
| Pregnancy test (beta-hCG) | Pregnancy / postpartum | Any woman of reproductive age |
| CBC, ESR, CRP | Inflammation, infection, leukaemia | Every patient (non-specific but supportive; ESR/CRP usually raised) |
| Stool culture + Yersinia serology | Yersinia, Salmonella, Campylobacter | Diarrhoea, abdominal pain, endemic exposure |
| IGRA (or Mantoux) | Tuberculosis | Endemic region, cough, weight loss, or before corticosteroid |
| Fungal serology / antigen | Histoplasma, Coccidioides, Blastomyces | Endemic exposure or travel history |
| Stool calprotectin | Intestinal inflammation of IBD | GI symptoms; a sensitive screen to decide on colonoscopy |
| Colonoscopy ± biopsy | Crohn disease, ulcerative colitis | GI symptoms, perianal disease, anaemia, raised calprotectin |
| HLA-B51, pathergy test | Behcet disease | Recurrent oral/genital aphthae, uveitis |
| ACE level | Sarcoidosis (supportive, not diagnostic) | If Lofgren not classic; modest utility |
| Tissue culture + stains (AFB, fungal) | Infectious panniculitis | Ulcerating, persistent, or immunosuppressed |
Interpreting results
A normal chest X-ray, normal ASO, negative pregnancy test, no drug culprit and no GI symptoms after this panel places a patient in the idiopathic group (30-50% of all EN). This is a legitimate conclusion only after the panel is complete — "idiopathic" is never an excuse to stop workup early. A raised ESR/CRP is expected and non-specific. A chest X-ray showing bilateral hilar lymphadenopathy in the setting of EN and ankle arthritis completes Lofgren syndrome and obviates biopsy.[1][4] The practical diagnostic algorithm runs as follows. At the first visit, confirm the clinical pattern (bilateral tender shin nodules, bruise-like colour evolution, no ulceration) and order the core panel — chest X-ray, ASO titre, throat swab, drug history, pregnancy test, CBC with ESR and CRP. If the chest X-ray shows bilateral hilar lymphadenopathy with ankle arthritis, stop: this is Lofgren syndrome; no biopsy is required. If the ASO is raised or the throat swab positive, treat streptococcus. If GI symptoms or a raised stool calprotectin are present, refer for colonoscopy. If all are negative, the diagnosis is idiopathic EN after a complete workup. Reserve skin biopsy for the atypical or refractory case — and then send deep, fat-inclusive tissue with a request for special stains and tissue culture for acid-fast bacilli and fungi so that the mimics (erythema induratum, infectious panniculitis, subcutaneous lymphoma) are not missed.[1][3]
Management — Acute Symptomatic Care
EN itself is self-limiting and benign; the immediate goal is symptom relief (pain, fever, arthralgia) while the cause is being identified. There is no role for antibiotics directed at the skin lesions, and no role for empirical corticosteroids until infection — particularly tuberculosis — has been excluded.[1]
Acute first-line symptomatic bundle
Identify and treat the underlying cause FIRST — this alone resolves most EN (e.g. penicillin for strep, stop the causative drug, treat IBD, manage sarcoidosis).
Bed rest and leg elevation — reduces dependent oedema, pain and the mechanical stress on inflamed septa; the single most effective non-drug measure.
Cool compresses to tender nodules.
Compression stockings (grade 2, 18-24 mmHg) if tolerated and no arterial insufficiency.
NSAIDs for pain and inflammation — ibuprofen 400 mg three times daily (or naproxen 500 mg twice daily) with food, for the duration of symptoms (typically 1-2 weeks); avoid in late pregnancy, renal impairment, active peptic ulcer.
Reassure the patient: self-limiting over 2-6 weeks, no ulceration, no scarring.
Management — Definitive and Stepwise
Once symptomatic care is underway, definitive management proceeds in three layers: (1) treat or remove the trigger; (2) symptomatic anti-inflammatory therapy; (3) second-line agents for refractory, recurrent or severe disease.[1]

Layer 1 — Treat or remove the trigger
This is the most effective single intervention. Penicillin V 500 mg orally four times daily for 10 days (or benzathine penicillin 1.2 million units intramuscularly once) for confirmed streptococcal pharyngitis. Discontinue the oral contraceptive pill or offending drug and substitute an alternative. Treat active tuberculosis with standard quadruple therapy before any immunosuppression. Optimise IBD therapy (the EN usually parallels gut disease activity and settles as the bowel is controlled).[2][5] Sarcoid Lofgren syndrome generally needs no specific sarcoid therapy — observation is correct, with NSAIDs for arthralgia.
Layer 2 — Symptomatic anti-inflammatory therapy
As above: bed rest, leg elevation, cool compresses, compression stockings, and an NSAID such as ibuprofen 400 mg three times daily for one to two weeks. This is sufficient for the majority of patients. [1]
Ibuprofen (first-line NSAID)
Dose
400 mg three times daily
Layer 3 — Second-line agents for refractory, recurrent, or severe disease
When lesions persist beyond six weeks, recur repeatedly, or are unusually severe, escalate to one of the following, chosen according to comorbidity and the suspected cause:[1]
Potassium iodide (SSKI)
Dose
300 to 900 mg daily (start at the lower end and titrate)
Colchicine
Dose
0.5 mg twice daily
Hydroxychloroquine
Dose
200 to 400 mg daily
Dapsone
Dose
50 to 150 mg daily
Prednisolone (short course)
Dose
0.5 to 1 mg/kg/day (max 60 mg) for 1-2 weeks, then taper over 2-4 weeks
A practical note on potassium iodide: it is the most-studied second-line agent for refractory EN, with a long track record and a clear although incompletely understood mechanism (inhibition of neutrophil chemotaxis and suppression of the delayed hypersensitivity reaction). It is contraindicated in pregnancy and should be used cautiously in patients with thyroid disease, with baseline and follow-up TSH monitoring.[7]
Specific Subtypes and Scenarios
Lofgren syndrome (sarcoidosis)
EN plus bilateral hilar lymphadenopathy plus ankle arthritis. The triad is diagnostic; no biopsy required when complete. Management is observation plus NSAIDs for arthralgia; the syndrome resolves within two years in most patients. HLA-DRB1*03 predicts a favourable outcome. Reserve corticosteroids for disabling arthritis or symptomatic pulmonary disease, and only after excluding TB.[4][8]
Erythema nodosum in inflammatory bowel disease
EN is the commonest cutaneous manifestation of IBD and, of the two, Crohn disease is more often associated than ulcerative colitis. A useful and well-tested feature is that EN activity parallels intestinal disease activity — EN often flares before or during a bowel relapse and settles as the gut is controlled. Investigate with stool calprotectin and colonoscopy; treat the underlying IBD. Paradoxically, EN may also appear as a reaction to anti-TNF agents used for IBD; a careful drug history resolves this.[2][5]
Erythema nodosum of pregnancy
May occur in any trimester or the puerperium and is benign and self-limiting. Manage with bed rest, leg elevation and cool compresses; avoid NSAIDs after 20 weeks' gestation (oligohydramnios, premature ductus arteriosus closure) and throughout lactation if preferred; avoid potassium iodide (fetal goitre) and colchicine (teratogenic). Reassure the mother; the prognosis is excellent and there is no long-term harm to mother or baby.[1]
Childhood erythema nodosum
Almost always streptococcal; confirm with ASO titre and throat swab and treat with penicillin V (weight-based: 250 mg three times daily for under 27 kg; 500 mg three times daily for over 27 kg, for 10 days). Consider Yersinia (with diarrhoea) and Bartonella henselae (cat-scratch disease, with lymphadenopathy). The prognosis is excellent; biopsy is rarely required in children.[1]
Behcet disease
The nodules of Behcet disease are clinically and histologically EN-like (a septal panniculitis, sometimes with a vasculitic component). They are distinguished by the company they keep: recurrent oral aphthae (obligatory), genital ulceration, uveitis, skin pathergy, and (in some) arterial or venous thrombosis. Colchicine is first-line for the mucocutaneous disease; TNF inhibitors (especially infliximab) for severe disease.[6]
Chronic, recurrent, or migratory EN
Persistent or recurrent EN demands a repeat or deepened workup — the commonest reason for "recurrence" is that the trigger was missed (occult IBD, chronic infection, ongoing drug exposure). Migratory subacute nodular panniculitis responds particularly well to potassium iodide.[1][7]
Complications and Pitfalls
True complications of EN are few — it does not ulcerate, scar, or leave atrophy. The morbidity is the pain and immobility of the acute phase, the arthralgia, and the cosmetic anxiety of the bruise-like discolouration, all of which resolve. The serious consequences belong to the underlying cause (untreated strep with rheumatic fever or glomerulonephritis; untreated IBD with stricturing and fistulae; untreated tuberculosis).[1]
The classic pitfalls an examiner tests: [1]
- Mislabelling erythema induratum as EN. If the nodules ulcerate, sit on the calves, or show vasculitis on biopsy, it is not EN — reclassify as erythema induratum and investigate tuberculosis.[3]
- Stopping the workup at "idiopathic" before completing the core panel (chest X-ray, ASO, drug history, pregnancy test, and — if symptomatic — stool studies and IBD screen). "Idiopathic" is a conclusion, not a starting point.
- Giving corticosteroids before excluding tuberculosis. In TB-endemic regions this can activate or disseminate latent TB. Always perform an IGRA or Mantoux and a chest X-ray, and scrutinise for constitutional symptoms, before any systemic steroid.[1]
- Biopsy that misses the fat. A superficial punch that does not include subcutaneous fat is non-diagnostic; always specify the need for fat and prefer an incisional or wedge biopsy of a deep nodule.
- Missing IBD. EN with any GI symptom merits stool calprotectin and, if raised, colonoscopy — EN can predate a bowel diagnosis by months.[2][5]
- Forgetting the Lofgren shortcut. The complete triad is a clinical diagnosis that does not need a biopsy; over-investigation is itself a pitfall.[4]
- Prescribing potassium iodide in pregnancy (fetal goitre) or without thyroid monitoring.[7]
Prognosis and Disposition
The prognosis is excellent. Individual lesions resolve over two to six weeks without ulceration or scarring, although new crops may continue to appear for several weeks if the trigger persists. Most patients are managed entirely in the outpatient setting; admission is almost never required for the skin disease itself. The long-term outcome is governed by the underlying cause: streptococcal EN resolves completely after antibiotic treatment; IBD-associated EN follows the course of the bowel disease; and Lofgren syndrome resolves within two years in the great majority, with HLA-DRB1*03 portending the best outcome.[1][4][8]
Recurrence is the main reason patients re-present. It is most likely when the trigger persists or recurs — continued oral contraceptive use, repeated streptococcal infections, uncontrolled IBD, or ongoing drug exposure — and should prompt a careful re-review of the original workup rather than simply re-treating the skin.[2] The total duration of an episode (from the first crop to complete resolution of the last) is usually three to six weeks, with crops appearing in succession over the first one to two weeks before the eruption winds down. A minority of patients have a more prolonged course extending to two to three months, particularly when the trigger is unrecognised or ongoing; persistence beyond this should always prompt re-evaluation rather than reflexive escalation of immunosuppression. Chronic or recurrent EN (loosely defined as recurrence beyond six months or multiple discrete episodes) accounts for a small but important minority, is most often tied to an identifiable and treatable trigger such as ongoing OCP exposure or uncontrolled IBD, and is the setting in which second-line agents such as potassium iodide, colchicine and hydroxychloroquine earn their place.[1][7]
Follow-up and safety-net: review in two to four weeks to confirm resolution and review cause-directed results. Give the patient a clear safety-net to return urgently if nodules ulcerate, spread beyond the shins, persist beyond six weeks, or if new systemic symptoms (fever, weight loss, cough, diarrhoea) appear.[1]
Special Populations
- Children — predominantly streptococcal; weight-based penicillin V; consider Yersinia and Bartonella. Prognosis excellent; biopsy rarely needed.
- Pregnant and lactating women — avoid NSAIDs after 20 weeks and potassium iodide and colchicine throughout; favour rest, elevation, cool compresses; paracetamol for pain. EN itself does not harm the pregnancy.[1]
- The elderly — EN is uncommon; when it occurs, weigh malignancy (lymphoma) and drug causes more heavily, and screen accordingly.
- Immunocompromised / HIV — broaden the infectious differential (mycobacteria including MAC, endemic and opportunistic fungi, Bartonella); biopsy and tissue culture early if any atypical feature.
- TB-endemic regions (South Asia, sub-Saharan Africa) — tuberculosis and BCG vaccine are leading precipitants; IGRA and chest X-ray are part of the core panel, not an add-on, and must precede any corticosteroid.
Evidence, Guidelines and Regional Differences
There are no large randomised trials in EN; management rests on pathophysiological rationale, retrospective series and expert consensus. The consensus is remarkably uniform across regions on the principles — treat the cause, rest and elevate, NSAIDs first-line, potassium iodide/colchicine for refractory disease — but the cause profile and pre-steroid workup differ by geography.[1]
[1] [1]A short evidence appraisal: the Perez-Garza 2021 practical approach and diagnostic algorithm remains the most useful single contemporary reference and underpins most of the workup above.[1] Wick 2017 summarises the panniculitides and the septal-lobular classification.[3] The Rogler 2021 and Antonelli 2021 papers ground the IBD-EN relationship and the principle that EN parallels gut activity.[2][5] Abdelghaffar 2024 and the Kolek 2023 HLA study define Lofgren syndrome, its clinical diagnosis, and the favourable HLA-DRB1*03-linked prognosis.[4][8] Ramam 2025 is the current reference for potassium iodide pharmacology and adverse effects in dermatology.[7] Espinosa 2025 covers the EN-like nodules of Behcet disease.[6]
Exam Pearls
[1]NO ULCER
Exam application bank (NEET-PG / INICET)
One-line answer
Erythema nodosum (EN) is an acute septal panniculitis — the commonest panniculitis. Clinical: bilateral, symmetric, tender, erythematous subcutaneous nodules on the anterior shins; NO ulceration, NO scarring (resolves like a bruise: red then purple then brown). Self-limiting over two to six weeks. Causes (screen for ALL): streptococcal infection (most common in children), sarcoidosis (Lofgren syndrome: EN plus bilateral hilar lymphadenopathy plus ankle arthritis; excellent prognosis), inflammatory bowel disease (Crohn's more often than UC), drugs (oral contraceptive pill, sulphonamides, penicillins, bromides), pregnancy, and other infections (TB, histoplasmosis, coccidioidomycosis, Yersinia, Chlamydia). About 30 to 50 percent remain idiopathic. Histology: septal panniculitis (thickened inflamed septa; lobules spared; Miescher radial granulomas; no vasculitis). Management: treat the under
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard. [1]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes. [1]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change. [1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each. [1]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory. [1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Erythema nodosum.
[1] [1]References
- [1]Perez-Garza DM, Chavez-Alvarez S, Ocampo-Candiani J, et al. Erythema Nodosum: A Practical Approach and Diagnostic Algorithm Am J Clin Dermatol, 2021.PMID 33683567
- [2]Rogler G, Singh A, Kavanaugh A, et al. Extraintestinal Manifestations of Inflammatory Bowel Disease: Current Concepts, Treatment, and Implications for Disease Management Gastroenterology, 2021.PMID 34358489
- [3]Wick MR. Panniculitis: A summary Semin Diagn Pathol, 2017.PMID 28129926
- [4]Abdelghaffar M, Hwang E, Damsky W. Cutaneous Sarcoidosis Clin Chest Med, 2024.PMID 38245372
- [5]Antonelli E, Bassotti G, Tramontana M, et al. Dermatological Manifestations in Inflammatory Bowel Diseases J Clin Med, 2021.PMID 33477990
- [6]Espinosa G. Behçet syndrome Med Clin (Barc), 2025.PMID 40378634
- [7]Ramam M, Prasad NK, Poojary S, et al. Potassium Iodide in Dermatology- Recent Advances in Mechanism of Action, Preparation, Uses and Adverse Effects Indian J Dermatol, 2025.PMID 40487487
- [8]Kolek V, Losertova P, Zatloukalova L, et al. Association between sarcoidosis and HLA polymorphisms in a Czech population from Central Europe: focus on a relationship with clinical outcome and treatment Front Med (Lausanne), 2023.PMID 37153085