Dermatology · Medicine
Halo naevus (Sutton's naevus)
Also known as Halo naevus · Sutton's naevus · Halo mole · Leucoderma acquisitum centrifugum · Perinaevic vitiligo
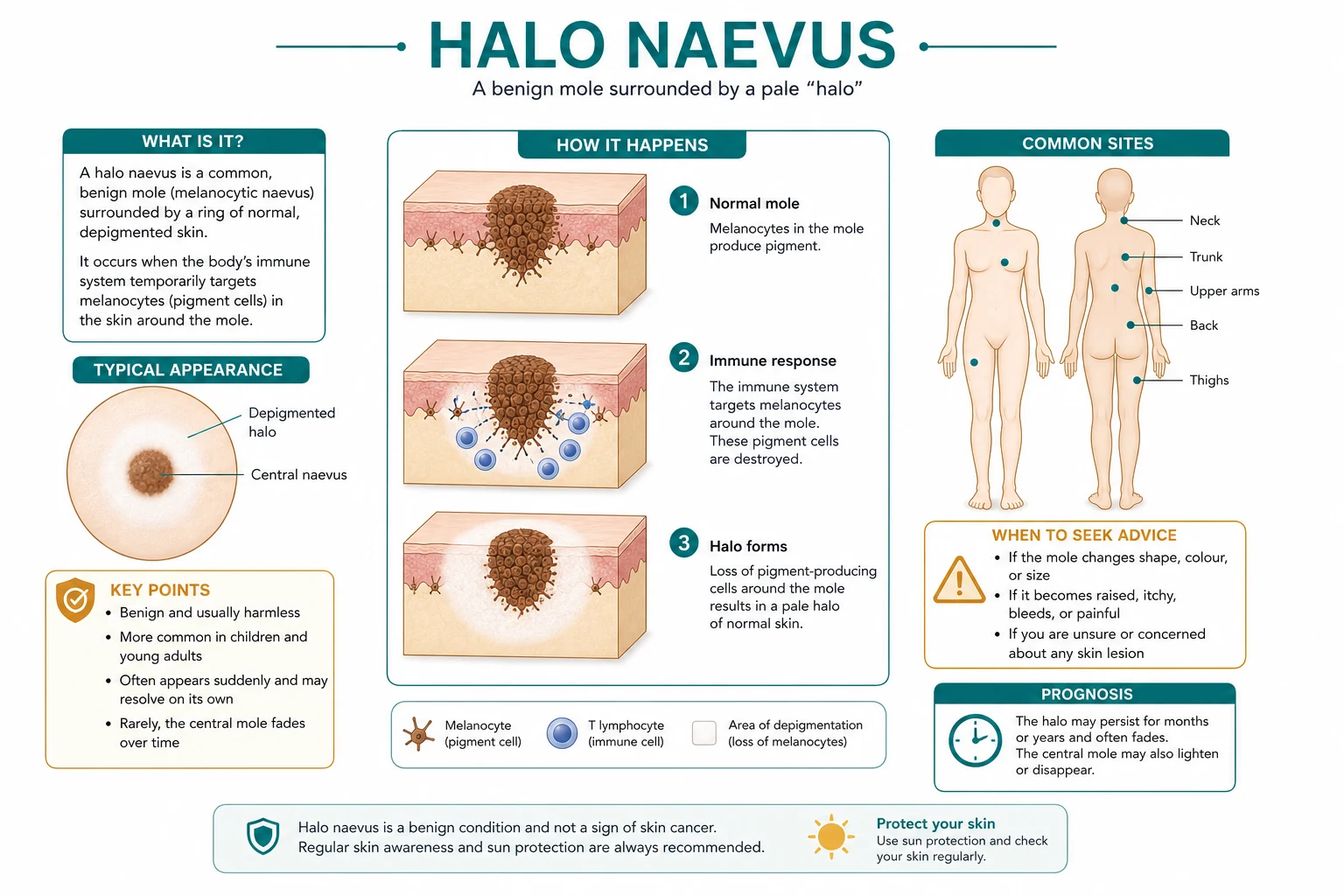
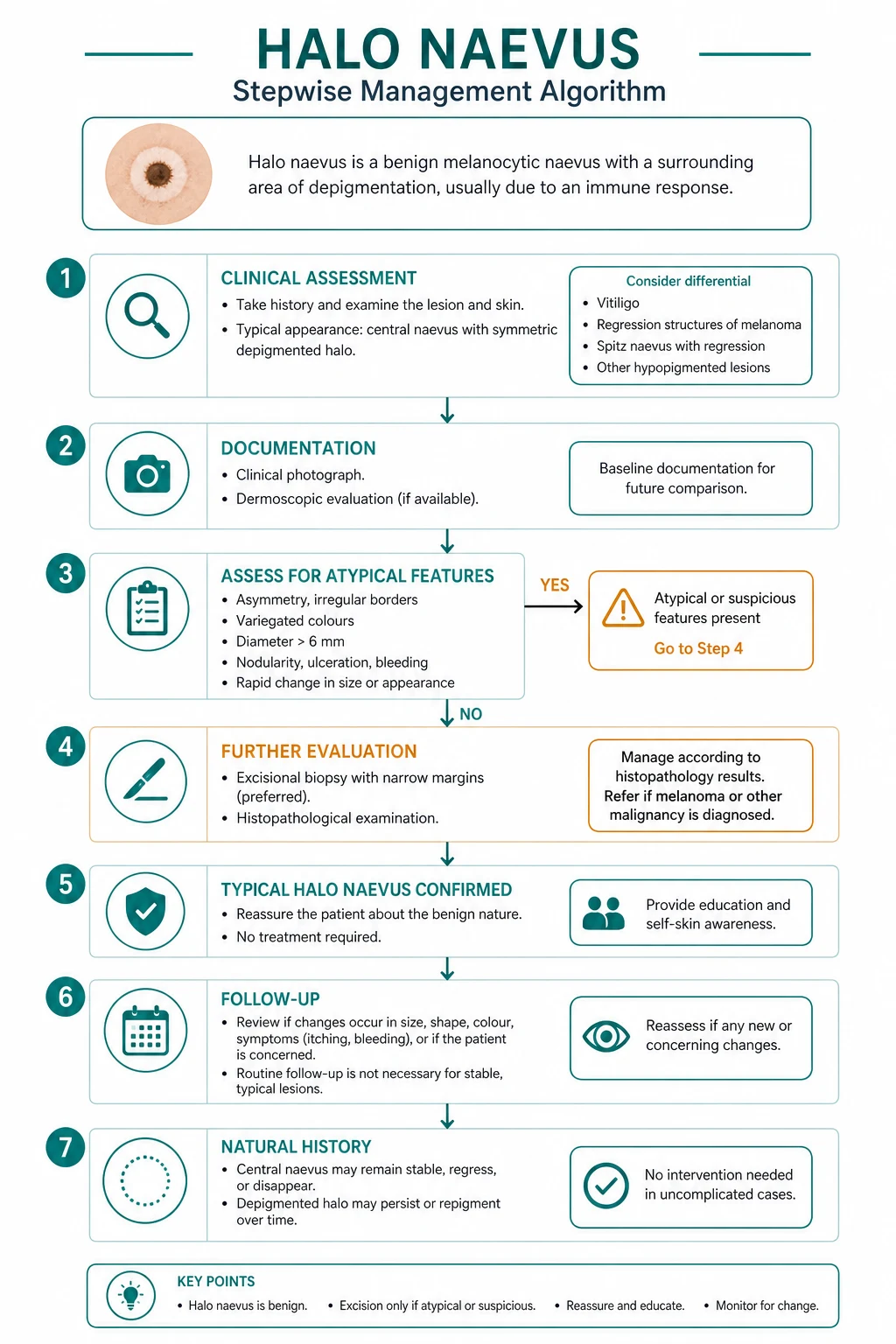
Halo naevus (Sutton's naevus, leucoderma acquisitum centrifugum) is a benign acquired melanocytic naevus surrounded by a symmetric, well-demarcated depigmented (white) halo, caused by autoimmune CD8+ cytotoxic T-cell-mediated destruction of both naevus melanocytes and the surrounding normal epidermal melanocytes (target antigens Melan-A/MART-1, gp100, tyrosinase). Prevalence is around 1 per cent, predominantly in children and adolescents (average age 15), on the trunk, and usually multiple. Associated with vitiligo (up to a quarter of cases) and autoimmune thyroid disease (Hashimoto's, anti-TPO). Natural history is benign and self-limiting in four stages: naevus with developing halo, fading naevus, disappearance of naevus leaving a depigmented macule, and gradual repigmentation of the halo over months to years. Management is reassurance, observation and sun protection; no treatment is needed unless cosmetic concern or atypical features. Biopsy is mandatory for any asymmetric halo, a solitary halo without a central naevus in an adult, or any changing lesion, to exclude melanoma with regression.
On this page & tools
Your progress
Saved locally on this device.
Exam tags
Red flags
Overview & Definition
A halo naevus — also called Sutton's naevus, halo mole, and historically leucoderma acquisitum centrifugum — is a benign acquired melanocytic naevus surrounded by a symmetric, well-demarcated ring (halo) of depigmented (white) skin.[1][4] The depigmentation is the visible signature of a T-cell-mediated autoimmune attack on melanocytes that destroys both the naevus cells themselves and the surrounding normal epidermal melanocytes. The name leucoderma acquisitum centrifugum — "acquired white skin spreading outward" — captures the phenomenon precisely: the white halo expands centrifugally from the central pigmented mole.[5]
Although the lesion looks alarming to patients and parents, it is benign and self-limiting. The defining clinical behaviour is a predictable four-stage evolution: the halo forms around a pigmented naevus, the central naevus progressively fades and disappears, and the residual depigmented macule eventually repigments over months to years.[1] The same autoimmune mechanism links halo naevus to vitiligo — both conditions are driven by T-cell recognition of melanocyte differentiation antigens — which is why the two conditions coexist and why a search for vitiligo and autoimmune thyroid disease is part of the assessment.[6]
The clinical importance of halo naevus lies in three examiner-tested problems: distinguishing a typical halo naevus from melanoma with regression, recognising the systemic autoimmune associations when multiple halo naevi appear, and knowing that the default management is reassurance, not excision — while never missing the rare adult or atypical lesion that is in fact a regressed melanoma.[3][7]
Classification & Evolution (the Four Stages)
Halo naevus is a single clinicopathological entity, but its natural history unfolds in four reproducible stages, first described in the classic clinicopathological literature and still the framework examiners expect.[1][5] Knowing the stages is essential because a lesion can present at any point in the sequence, and the patient's anxiety is often driven by the change itself.
Four stages of halo naevus evolution
A brown-black melanocytic naevus is surrounded by a developing symmetric ring of white depigmentation. The halo is uniform in width around the entire circumference. This is the classic textbook picture most patients present with.
The central naevus begins to lighten — from dark brown to lighter brown, then pink, then erythematous — as the cytotoxic T-cell response destroys the naevus melanocytes. The halo is now fully developed.
The central naevus is completely destroyed, leaving behind a round depigmented macule — only the halo remains, with no pigmented centre. Patients may interpret this as a mole that "vanished".
The depigmented area gradually repigments over months to years, as melanocyte precursors migrate in from the surrounding normal skin and the autoimmune response subsides. Skin returns to normal colour, sometimes incompletely.
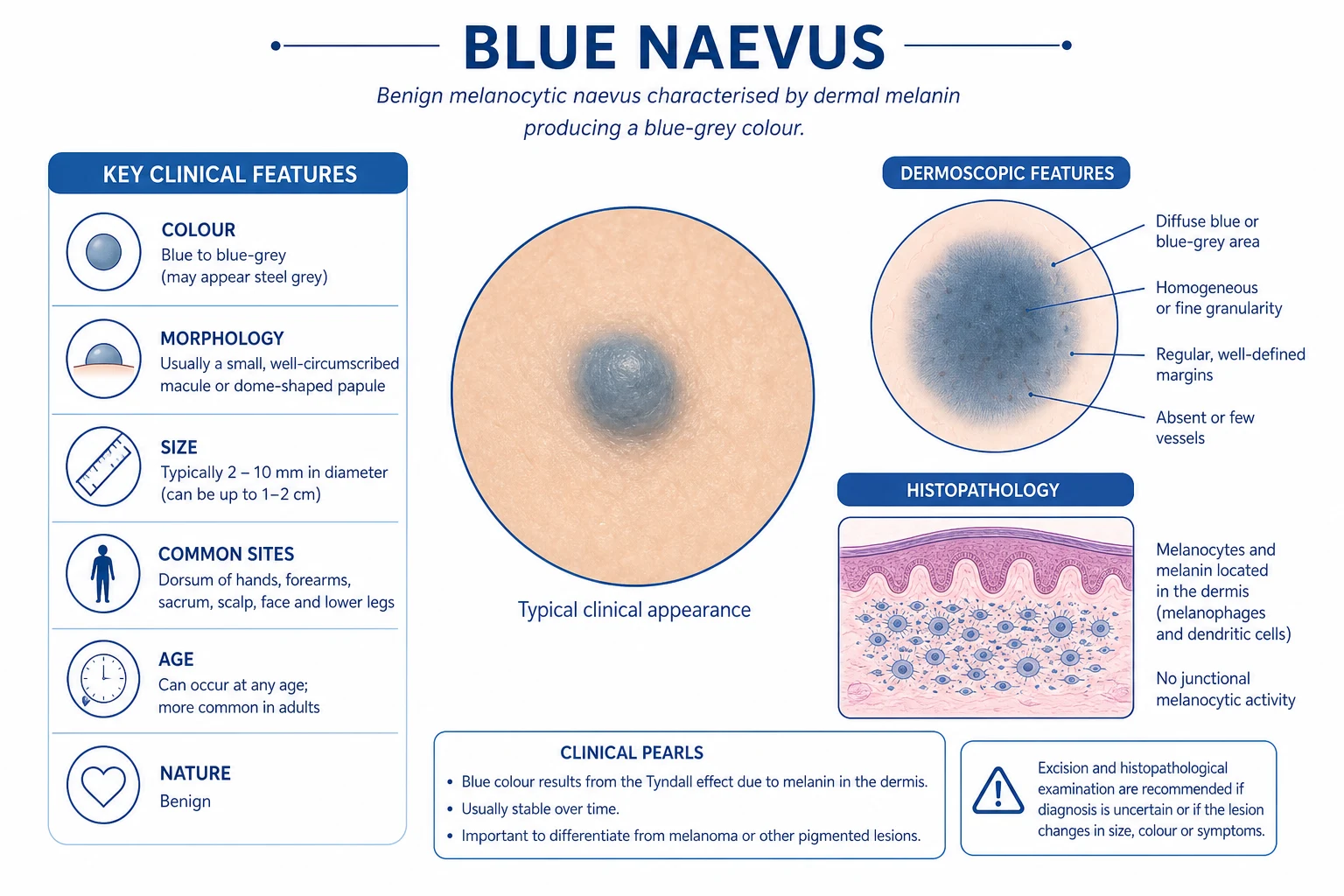
The halo phenomenon itself is not restricted to common acquired naevi. The same immune event can encircle congenital naevi, Spitz naevi, blue naevi, dysplastic (atypical) naevi, melanoma, and even non-melanocytic lesions (such as angiokeratoma, dermatofibroma, seborrhoeic keratosis, or a tattoo) — the umbrella term "halo phenomenon" covers all of these, while "halo naevus" is reserved for the benign acquired melanocytic naevus with halo.[5][8] This terminological distinction is a common viva trap.
Classic halo naevus
Sutton's naevus
- Common acquired naevus + symmetric halo
- Children/adolescents; trunk; multiple
- Benign, self-limiting four-stage course
- Default: reassure
Halo phenomenon
Same depigmentation, other lesion
- Halo around a non-classic lesion
- Congenital, Spitz, blue, dysplastic naevus
- Melanoma can trigger a halo phenomenon
- Biopsy if the central lesion is atypical
Pseudo-halo naevus
Depigmentation without immunity
- Naevus surrounded by pale skin from non-immune cause
- e.g. tattoo, steroid atrophy, prior inflammation
- No T-cell infiltrate on histology
- Distinguish by history and biopsy
Epidemiology & Risk Factors
Halo naevus is common but under-reported, because most lesions are never shown to a clinician. The estimated prevalence is around 1 per cent of the general population, with the peak incidence in the second decade of life.[1][4]
Epidemiology at a glance
Established risk factors and associations are age (children and adolescents dominate), personal or family history of vitiligo or autoimmune thyroid disease, and a familial tendency — multiple family members with halo naevi are described, suggesting a heritable autoimmune predisposition.[1][4] There is no clear sex predilection and no strong racial or phototype bias, although the depigmented halo is more visually obvious in darker phototypes. The role of sun exposure is debated; some series report seasonal onset or Koebner-type triggering at sun-exposed sites, but UV is not the driver of the autoimmune response.
The most important "risk" is not of the lesion itself but of its associations and mimics: a new halo naevus in a child warrants a screen for vitiligo and thyroid autoimmunity, while a new solitary halo in an adult warrants a search for occult melanoma that has triggered the halo phenomenon.[3][7]
Pathophysiology
The autoimmune attack on melanocytes
The depigmented halo is the visible end-result of a CD8+ cytotoxic T-cell-mediated immune response directed against melanocyte differentiation antigens — the same family of antigens (Melan-A/MART-1, gp100/Pmel-17, tyrosinase, tyrosinase-related proteins TRP-1 and TRP-2) that drives vitiligo and that melanoma immunotherapy exploits.[1][6] When the immune system mounts this response, it does not discriminate between the naevus melanocytes (which express these antigens abundantly) and the surrounding normal epidermal melanocytes (which express the same antigens) — both are destroyed, producing the symmetric, centrifugal depigmentation that defines the halo.[5]
The mechanism is a coordinated cellular and humoral attack: [1]
- CD8+ cytotoxic T-cells infiltrate the naevus and the epidermis immediately around it, recognising melanocyte antigens presented on MHC class I and releasing perforin and granzyme to induce melanocyte apoptosis.
- Granulysin, a cytotoxic protein released by these T-cells, has recently been shown to be markedly upregulated in both halo naevus and vitiligo skin, supporting a shared effector mechanism.[6]
- Autoantibodies against tyrosinase, Melan-A, and gp100 are detectable in the serum of many patients, but they are thought to be a secondary marker of melanocyte damage rather than the primary effector — the tissue destruction is T-cell driven.
- Melanophages accumulate in the papillary dermis as pigment is released from destroyed naevus cells, producing the faint tan/pink hue sometimes seen in the regressing naevus.
Why the halo is symmetric, and why it repigments
The symmetry of the halo is its most distinctive clinical feature and a key discriminator from melanoma with regression. It reflects the fact that the antigen load is highest at the naevus and falls off concentrically into the surrounding epidermis, so the cytotoxic T-cell response eliminates melanocytes in a uniform radial band around the mole. As the naevus cells are themselves destroyed, the antigenic stimulus fades, the T-cell response subsides, and melanocyte stem cells from the outer hair follicle bulge and adjacent interfollicular epidermis migrate centrally to repigment the halo — the same mechanism by which vitiligo repigments around hair follicles (perifollicular repigmentation).[1][6]
Why vitiligo and halo naevus are linked
The shared antigenic target — melanocyte differentiation antigens — explains the strong clinical overlap between halo naevus and vitiligo.[6] In vitiligo, the autoimmune response is systemic and progressive, targeting melanocytes throughout the skin; in halo naevus, it is localised to one naevus (and its immediate surround) and is self-limited. Why the same immune process is localised and benign in one patient and generalised and chronic in another is not fully understood, but the same susceptibility genes (autoimmune diathesis, HLA associations, non-HLA immune regulators) and the same effector T-cells are involved. This shared biology is the reason a halo naevus can be the first presentation of vitiligo, and why patients with widespread vitiligo frequently have one or more halo naevi.[1]
The melanoma paradox
A crucial and counter-intuitive point: the halo phenomenon is occasionally triggered by melanoma itself. In this scenario the immune system mounts a successful response against the melanoma (which expresses the same melanocyte antigens, abundantly), destroying the tumour cells and the surrounding normal melanocytes in the process — the result is a depigmented halo at the site of a regressed melanoma, which can closely mimic a benign halo naevus.[3][7] This is the biological basis for the cardinal rule: a solitary halo without a central naevus in an adult must be biopsied to exclude a fully regressed melanoma. The immune response, in this sense, can be both a marker of good prognosis (it has destroyed the tumour) and a trap (it has hidden the diagnosis).[3]
Clinical Presentation
Morphology and distribution
The classic halo naevus at presentation (Stage 1) is a brown, dark-brown or pink-brown melanocytic naevus at the centre, surrounded by a symmetric, uniform-width ring of pure white (depigmented) skin — the halo.[1][4] The halo is sharply demarcated from the surrounding normally pigmented skin and is complete (it encircles the entire naevus, with no gaps). The central naevus is usually 3–6 mm, round or oval, and otherwise typical — it has the regular architecture of a benign acquired naevus, with no asymmetry, border irregularity, colour variegation, or diameter over 6 mm in its own right.

The distribution favours the trunk — the back (especially the upper back and scapular area) more than the chest and abdomen — followed by the extremities (proximal limbs) and, less often, the head and neck.[1][4] Lesions on the palms, soles, genitalia, and mucosa are rare but described. The predilection for the trunk mirrors the distribution of common acquired naevi generally, since halo naevus is essentially a common naevus plus an immune event.
Number and pattern
Halo naevi are multiple in over half of cases, with two to ten lesions occurring either simultaneously or sequentially over months to years.[1] New halo naevi can continue to appear throughout adolescence — each running its own four-stage course independently — which is a source of parental anxiety but is itself a typical and benign pattern. Agminated halo naevi (multiple halos clustered within a single anatomical area) and generalised halo naevi (dozens of lesions) are rarer patterns that have been reported as novel presentations.[8]
Symptoms
A classic halo naevus is asymptomatic. There is no pain, itching, burning, bleeding, or ulceration — the only change the patient notices is the cosmetic appearance of the white halo and, later, the fading or disappearance of the central mole. The presence of any symptom (pain, pruritus, bleeding, crusting, ulceration, rapid growth, or surrounding erythema) is a red flag that the lesion may NOT be a halo naevus, and mandates biopsy to exclude melanoma with regression or an irritated alternative diagnosis.[7]
Atypical presentations
Examiners deliberately probe the atypical presentations: [1]
- Adult onset. A first halo naevus appearing in an adult over 40 is unusual; the priority is to exclude melanoma with regression rather than to reassure.[3][7]
- Solitary lesion. While multiple halo naevi in a child are typical, a single halo naevus — especially without a long history — should be examined carefully for atypia of the central lesion.
- Halo without a central naevus. When the patient presents with a round depigmented macule and no central pigmented lesion (Stage 3 in evolution, or a fully regressed lesion), the question is whether this is a halo naevus in its late stage (likely, in a child with other halo naevi) or a regressed melanoma (a real possibility in an adult).[7]
- Asymmetric or irregular halo. A halo that is thicker on one side, notched, or geometrically irregular is atypical; melanoma must be excluded.[3]
- Halo around an atypical naevus or congenital naevus. The halo phenomenon can encircle a dysplastic naevus, a congenital melanocytic naevus, a Spitz naevus, or a blue naevus — these are variants of the halo phenomenon, not classic Sutton's naevus.[5][8]
- Darker phototypes. The halo is more visually striking and may cause greater cosmetic distress; repigmentation can be incomplete and postinflammatory hyperpigmentation can complicate the picture.
Differential Diagnosis
The differential of "a pigmented lesion with surrounding white skin" is one of the highest-yield areas of this topic, because the single most dangerous error is mistaking a regressed melanoma for a benign halo naevus.[3][7]
Melanoma with regression
The must-not-miss
- SOLITARY halo; adult onset
- Central lesion may be asymmetric, irregular, variably pigmented
- ABCDE positive; history of change/bleeding
- Dermoscopy: atypical network, regression structures, blue-white veil
- Biopsy essential — never reassure
Vitiligo overlying a naevus
Generalised vitiligo
- Vitiligo elsewhere on body (face, hands, flexures)
- Depigmentation is part of a generalised pattern, not a single symmetric halo
- Naevus is incidental — sits within an area of vitiligo
- Family history of autoimmunity
Post-inflammatory hypopigmentation
Following inflammation
- History of preceding eczema, psoriasis, infection, or trauma at the site
- Hypopigmented (not pure white); ill-defined
- No central naevus
- Resolves over weeks-months as inflammation settles
Naevus depigmentosus
Congenital stable lesion
- Congenital or early-childhood onset
- Single stable hypopigmented patch
- No central naevus; no evolution
- Wood's lamp: off-white (not pure white)
Meyerson's naevus
Eczematous halo
- Eczematous (red, scaly, pruritic) halo around a naevus
- NOT depigmented
- Histology: spongiotic eczema
- Responds to topical corticosteroid
Piebaldism / chemical leukoderma
Other causes of white patches
- Piebaldism: congenital, forelock, autosomal dominant
- Chemical leukoderma: exposure to phenols/catechols (adhesives, rubber, hair dye)
- Distribution pattern and exposure history distinguish
- No central naevus
Two clinical rules govern the differential. First, a typical halo naevus in a child or adolescent — symmetric halo, benign central naevus, multiple lesions, asymptomatic — is a clinical diagnosis that requires no investigation. Second, any atypical feature (solitary, adult onset, asymmetric halo, changing lesion, symptomatic, or a central lesion with any ABCDE feature) mandates dermoscopy and biopsy to exclude melanoma.[3][7]
Distinguishing each mimic — what the examiner wants
Melanoma with regression is the lesion that must never be missed. The clinical clue is asymmetry of the central lesion, irregular border, colour variegation, diameter over 6 mm, and evolution (the ABCDE criteria), together with any history of change, bleeding, or itching.[3] The halo in regressed melanoma is often irregular, asymmetric, or geographic rather than the uniform ring of a halo naevus, and the patient is more likely to be an adult rather than a child. Dermoscopy of a regressed melanoma may show regression structures (scar-like depigmentation, peppering/blue-grey granules) alongside any residual atypical melanoma features (atypical network, streaks, blue-white veil, atypical vessels). The decision rule is absolute: if there is any doubt, biopsy.[7]
Vitiligo is the closest biological cousin of halo naevus. The distinction is one of distribution and pattern: vitiligo produces multiple, often symmetric, depigmented macules on the face, hands, flexures, and extensor surfaces, while a halo naevus is one naevus with its own surrounding halo. When a patient has both — a halo naevus and depigmentation elsewhere — the diagnosis is straightforward. When a naevus sits within an area of vitiligo, the depigmentation is part of the vitiligo pattern rather than a halo phenomenon. [1]
Post-inflammatory hypopigmentation follows an identifiable inflammatory event (eczema, psoriasis, tinea, a burn, a resolved infection) at the same site. The hypopigmentation is usually off-white rather than pure white, ill-defined rather than sharply demarcated, and there is no central naevus. It resolves as the skin repigments over weeks to months. [1]
Naevus depigmentosus is a congenital or early-childhood stable hypopigmented patch that does not change, has no central naevus, and shows an off-white colour under Wood's lamp (in contrast to the pure white, accentuated depigmentation of vitiligo or a halo naevus). It is a developmental pigmentary mosaicism, not an immune event. [1]
Meyerson's naevus is the other important "halo" naevus that examiners name. It is a melanocytic naevus surrounded by an eczematous (red, scaly, pruritic) halo — the halo is inflammatory, not depigmented. Histology shows spongiotic eczema overlying the naevus, and the lesion resolves with a topical corticosteroid. Confusing Meyerson's naevus with Sutton's naevus is a classic viva trap: the former is eczematous and red, the latter is depigmented and white. [1]
Piebaldism is a congenital, autosomal dominant leukoderma with a characteristic forelock and stable depigmented patches; it is present from birth, distinguishing it from the acquired halo naevus. Chemical leukoderma follows exposure to depigmenting chemicals (phenols, catechols in adhesives, rubber gloves, hair dyes, and some cleaning agents) and produces a pattern of depigmentation matching the exposure; there is no central naevus, and the history identifies the cause. [1]
Clinical & Bedside Assessment
The assessment of a suspected halo naevus is built around two questions: Is this really a halo naevus? and, if yes, does this patient have vitiligo or thyroid autoimmunity? [1]
Begin with inspection under good lighting, examining the lesion and the surrounding skin. Confirm the four clinical pillars of a halo naevus: a benign-appearing central naevus, a symmetric uniform-width halo, asymptomatic course, and the right demographic (child or adolescent). Look specifically for the features that would demand biopsy — asymmetry, irregular border, colour variegation, diameter over 6 mm, evolution (ABCDE), and any symptom (pain, itching, bleeding) — and examine the central naevus with a dermatoscope.[1]
Because halo naevi are multiple and coexist with vitiligo, always examine the whole skin, not just the presenting lesion. Inspect the face, peri-orificial skin, hands, wrists, axillae, groin, knees, and elbows for depigmented macules of vitiligo, and check the neck for goitre and the hands for signs of thyroid disease (bradycardia, slow-relaxing reflexes, dry skin for hypothyroidism). Take a focused autoimmune history — vitiligo, thyroid disease, type 1 diabetes, Addison's disease, pernicious anaemia, alopecia areata — in the patient and first-degree relatives.[1]
Wood's lamp (long-wave ultraviolet light) examination is a useful bedside adjunct: the depigmented halo fluoresces bright pure white under Wood's lamp, confirming complete loss of melanin (as in vitiligo) and distinguishing it from the off-white hypopigmentation of post-inflammatory change or naevus depigmentosus, which does not fluoresce.[4]
Investigations
The diagnosis is clinical
For a typical halo naevus in a child or adolescent — symmetric halo, benign central naevus, multiple lesions, asymptomatic — the diagnosis is clinical and no investigation is required.[1][4] The history, morphology, and demographic are diagnostic; performing biopsies or bloods on a typical lesion adds cost, scarring, and anxiety without changing management.
Dermoscopy — confirming the benign pattern
Dermoscopy is the key bedside tool for the typical lesion and, more importantly, for the atypical lesion where melanoma must be excluded.[2]
The classic dermoscopic features of a halo naevus are:[1][2]
- Central naevus: a regular globular (brown dots/globules of nested naevus cells at the dermoepidermal junction) or homogeneous brown pattern, with a symmetric, regular architecture. In children the globular pattern predominates; in adolescents a homogeneous or combined pattern may be seen.
- Surrounding halo: a structureless, pure white area encircling the naevus, uniform in width, with no pigment network (because there are no melanocytes producing melanin).
- As the naevus regresses (Stages 2–3): the central globules become fewer, smaller and lighter, may show regression structures (blue-grey granules, peppering from melanophages), and finally disappear, leaving only the white structureless area. [1]
Equally important are the features that are absent in a halo naevus: there is no atypical pigment network, no streaks/pseudopods, no blue-white veil, and no atypical (dotted/linear/polymorphous) vessels in the central lesion. The presence of any of these should prompt biopsy, because a regressed or regressing melanoma can display a depigmented halo indistinguishable from that of a halo naevus.[3][7]
Dermoscopy of halo naevus — the four features
GSWA
Regular brown globules/homogeneous pattern — benign
Uniform-width pure white ring; no network
Halo is depigmented — no pigment network
No atypical network, streaks, blue-white veil, or atypical vessels
When to biopsy — the atypical lesion
Biopsy is indicated whenever the clinical or dermoscopic picture is not that of a typical halo naevus.[3][7] Specifically, biopsy is mandatory for:
- A solitary halo without a central naevus in an adult (possible fully regressed melanoma).
- An asymmetric, irregular, or geometric halo around a pigmented lesion.
- A central naevus with any ABCDE feature (asymmetry, border irregularity, colour variegation, diameter over 6 mm, evolution).
- Any symptomatic lesion (pain, itching, bleeding, ulceration, rapid growth).
- A changing lesion, or any lesion that does not behave as expected over follow-up. [1]
When biopsy is performed, a full-thickness excisional biopsy (complete excision with a 2 mm margin) is preferred for any lesion where melanoma is genuinely suspected, to allow complete histological assessment. A punch or shave biopsy may be acceptable for a lesion where the diagnosis is uncertain but melanoma is not the leading concern, but excision is safer if there is any real doubt.[7]
Histopathology
When a halo naevus is biopsied, the histology confirms the diagnosis and excludes melanoma. The cardinal features are:[1][5]
- A dense, band-like lymphocytic inflammatory infiltrate at the dermoepidermal junction and superficial dermis, embracing the naevus cells in a "brace-like" or "moth-eaten" pattern — naevus cell nests are infiltrated and disrupted by lymphocytes (predominantly CD8+ cytotoxic T-cells).
- Naevus cells may show regression changes — apoptosis, diminished pigment, and reduced nest size; in late-stage lesions the naevus cells are absent.
- Melanophages in the papillary dermis (from released melanin).
- Loss of epidermal melanocytes in the halo region (confirmed on Melan-A/MART-1 or SOX10 immunostain — the depigmented halo has no melanocytes).
- Crucially, absence of cytological atypia (no severe atypia, no mitoses, no pagetoid scatter) distinguishes a halo naevus from melanoma. [1]
Screening for autoimmune associations
When a patient has multiple halo naevi, or any halo naevus with features suggesting autoimmunity, screening is appropriate:[1][4]
- Full skin examination for vitiligo (depigmented macules on the face, hands, flexures).
- Thyroid function tests (TSH, free T4) and anti-thyroid peroxidase antibodies (anti-TPO) — to detect autoimmune thyroid disease (Hashimoto's thyroiditis most commonly; Graves' disease less often).
- In selected cases, screening for other autoimmune diseases (type 1 diabetes, Addison's disease, pernicious anaemia, alopecia areata) if clinical features suggest them. [1]
No imaging is required for a typical halo naevus. [1]
Management — Resuscitation (the Diagnostic Safety Step)
Halo naevus is not an emergency; a confirmed typical lesion needs no urgent treatment. The "resuscitation" step for this topic is really a diagnostic safety step: when a patient presents with a "new white ring around a mole", the immediate priority is to exclude melanoma by careful clinical examination and dermoscopy, and to biopsy if there is any atypical feature — never to reassure on the basis of a presumed "halo naevus" without confirming the diagnosis.[3][7] Equally, when multiple new halo naevi appear in an adult, the priority is to perform a full skin examination for occult melanoma (since melanoma can trigger a generalised halo phenomenon) rather than to dismiss the eruption as benign.
Management — Definitive & Stepwise
The management of a confirmed halo naevus is built on a simple principle: reassure and observe; intervene only for cosmetic concern or diagnostic uncertainty.[1][4]
Step 1 — Reassure, observe, and sun-protect
For a typical halo naevus in a child or adolescent, the correct management is reassurance: explain that the lesion is benign, that it is not a cancer, that the central naevus will gradually regress and disappear, and that the white halo will eventually repigment over months to years.[1][4] This is both the safest and the most cost-effective option and should be the default.
Photograph the lesion at baseline and re-examine in 6 to 12 months to document the expected regression; serial photographs are reassuring for the family and provide objective evidence of the benign course. Sun protection of the depigmented area is essential — without melanin, the halo skin burns easily — using clothing, shade, and a broad-spectrum SPF 30+ sunscreen reapplied regularly.[4]
Step 2 — Screen for autoimmune associations (if multiple)
When a patient has multiple halo naevi, screen for vitiligo and autoimmune thyroid disease: a full skin examination for depigmentation, and TSH with anti-TPO.[1] If thyroid disease is detected, manage it on its own merits (levothyroxine for hypothyroidism, endocrine referral as needed). If vitiligo is present, manage it according to vitiligo guidelines (topical corticosteroid or calcineurin inhibitor, NB-UVB, or topical ruxolitinib in selected cases).
Step 3 — Cosmetic treatment of persistent depigmentation
In a minority of cases the depigmented halo persists for years (or permanently) and is a significant cosmetic concern, especially on visible sites or in darker phototypes. When repigmentation is desired, the same treatments used for localised vitiligo are appropriate, because the underlying mechanism is the same:[1][6]
Topical calcineurin inhibitor
First-line topical
- Tacrolimus 0.1% ointment or pimecrolimus 1% cream
- Twice daily to the depigmented area for 3–6 months
- Steroid-sparing; safe on face and folds
- Local burning/itching; no skin atrophy
Topical corticosteroid
Alternative topical
- e.g. methylprednisolone aceponate or mometasone 0.1%
- Once daily; limit to 2–3 months on body, avoid face
- Monitor for atrophy, telangiectasia
- Use calcineurin inhibitor if face/fold involved
Excimer laser (308 nm)
Targeted phototherapy
- Targeted UVB to the depigmented macule
- Two to three sessions per week for several months
- Best for small, localised lesions
- Erythema, blistering at higher fluence
Narrowband UVB phototherapy
Widespread depigmentation
- Whole-body NB-UVB; 2–3×/week
- Used when multiple halo naevi + coexistent vitiligo
- Slow response (months); perifollicular repigmentation
- Cumulative UV dose — limit total sessions
Cosmetic camouflage
Immediate concealment
- Makeup matched to skin tone
- Immediate cosmetic result; no active treatment
- Useful for visible sites (face, hands)
- Combine with sun protection
Repigmentation, when it occurs, typically appears first as perifollicular brown macules — melanocyte precursors repopulating from the hair follicle bulge — and gradually expands to fill the halo. The response is slow (months) and often incomplete, and patients should be counselled that perfect repigmentation is not guaranteed. [1]
Step 4 — Biopsy or excise if atypical
The one situation in which the benign "reassure and observe" pathway does NOT apply is the atypical lesion. Biopsy — preferably excisional — is mandatory for:[3][7]
- A solitary halo without a central naevus in an adult (possible regressed melanoma).
- An asymmetric, irregular, or changing halo around a pigmented lesion.
- Any central naevus with ABCDE features or any symptom (pain, itching, bleeding).
- A lesion that fails to behave as expected over follow-up (a halo naevus that does not regress, or that enlarges, darkens, or becomes symptomatic). [1]
Technique notes
Topical calcineurin inhibitors (tacrolimus 0.1% ointment, pimecrolimus 1% cream) are applied twice daily to the depigmented area for 3 to 6 months; they are steroid-sparing and the preferred choice on the face, neck and intertriginous skin where topical corticosteroids cause atrophy. Local burning and itching are common in the first week and usually settle.[6]
The 308 nm excimer laser delivers targeted UVB to the depigmented macule in sessions two to three times weekly for several months; it is best suited to small, localised lesions and is the treatment of choice when a single persistent halo on a visible site is the cosmetic concern. Erythema and occasional blistering are the main side effects. [1]
Narrowband UVB (NB-UVB) phototherapy (311 nm) is reserved for widespread depigmentation, typically in a patient who has multiple halo naevi and coexistent vitiligo; treatment is two to three times weekly, with repigmentation appearing slowly over months as perifollicular macules. The cumulative lifetime UV dose should be tracked. [1]
Post-treatment and follow-up
For a typical lesion under observation, follow-up is pragmatic rather than scheduled: a baseline photograph and a review at 6 to 12 months to confirm the expected regression, then return-as-needed advice. For a lesion that has been excised for atypia and confirmed benign, no further follow-up is required. New halo naevi may continue to appear through adolescence; the patient and family should be reassured that each runs the same benign course. [1]
Specific Subtypes & Scenarios
The halo phenomenon on non-classic lesions
The same autoimmune event can encircle lesions other than a common acquired naevus. These are variants of the halo phenomenon, not classic Sutton's naevus, but they are examined and worth knowing:[5]
- Halo congenital naevus — a congenital melanocytic naevus that develops a symmetric halo; benign, but the central lesion is followed for the usual congenital-naevus considerations.
- Halo Spitz naevus — a Spitz naevus (a benign but histologically alarming pink papule in children) with a halo; histology is essential because Spitzoid melanoma is in the differential.
- Halo blue naevus — a dermal blue naevus with a halo; the blue colour persists because dermal melanocytes are spared.
- Halo dysplastic (atypical) naevus — an atypical naevus with a halo; the central lesion is biopsied to grade the atypia.
- Halo around non-melanocytic lesions — seborrhoeic keratosis, dermatofibroma, angiokeratoma, basal cell carcinoma, and even tattoos have been reported with a halo phenomenon.[5]
Agminated and segmental halo naevi
Agminated halo naevi — multiple halos clustered within a single anatomical area, sometimes in a segmental/dermatomal distribution — are a rare recognised pattern reported as a novel presentation.[8] They follow the same benign course as classic halo naevi but suggest a more localised triggering event.
Halo naevus as the first sign of vitiligo
A patient (often a child) presenting with multiple new halo naevi may develop generalised vitiligo months to years later — the halo naevi are the first manifestation of the underlying autoimmune diathesis.[1][6] These patients should be examined periodically for new depigmentation, counselled about the possibility, and screened for thyroid autoimmunity.
Halo naevus and melanoma (the regressed melanoma trap)
The most important subtype to recognise is the halo phenomenon triggered by melanoma — the immune system has destroyed the tumour, leaving a depigmented halo with no (or minimal) residual pigmented lesion.[3][7] This is rare but is the reason for the cardinal rule: a solitary halo without a central naevus in an adult must be biopsied. Equally, a patient with multiple new halo naevi and a personal or family history of melanoma should have a full skin examination for occult melanoma, since the generalised halo phenomenon can be a paraneoplastic immune response to a melanoma elsewhere.[3]
Complications & Pitfalls
Disease-related complications
In their natural state, halo naevi cause few problems. The complications that matter are largely cosmetic and psychological:[1][4]
- Sunburn of the depigmented halo — without melanin, the halo skin burns easily; sun protection is essential.
- Cosmetic distress — especially for facial, hand, or widespread lesions, or in darker phototypes where the contrast is greatest; repigmentation may be incomplete.
- Psychological distress in children and adolescents — anxiety about a "changing mole" and fear of cancer; reassurance is itself a treatment.
- Incomplete repigmentation — the halo may persist permanently as a depigmented macule in some patients. [1]
Treatment-related complications
Topical corticosteroids can cause skin atrophy, telangiectasia, and striae if used for too long, especially on the face and folds — a calcineurin inhibitor is preferred at these sites. Excimer laser and NB-UVB can cause erythema, blistering, and (in darker skin) postinflammatory hyperpigmentation, and the cumulative UV dose must be tracked. Biopsy and excision carry the usual risks of scarring, infection, and dyspigmentation, but these are acceptable when melanoma is in the differential. [1]
The defining pitfalls
Prognosis & Disposition
The prognosis of halo naevus is uniformly benign: the central naevus regresses and disappears (typically over 6 to 12 months from onset of the halo), and the halo gradually repigments over months to years (often 1 to 5 years), sometimes incompletely or not at all.[1][4] No halo naevus itself undergoes malignant transformation; the only malignant concern is the melanoma that mimics a halo naevus, not the halo naevus itself. New halo naevi may continue to appear through adolescence; each runs the same benign independent course.
Typical lesions are managed in primary care or in general dermatology outpatient clinics. Specialist referral is appropriate for atypical lesions where melanoma cannot be confidently excluded, for widespread depigmentation with significant cosmetic impact, and for the patient with multiple halo naevi and an autoimmune diathesis who needs screening and counselling. The safety-net for every patient is clear advice to return if the lesion changes colour, shape or size, becomes symptomatic, or if new halo naevi appear in adulthood. [1]
Special Populations
Children and adolescents
Children and adolescents are the typical population for halo naevus. The priorities are to reassure the patient and parents, to confirm the diagnosis clinically (avoiding unnecessary biopsy), to provide baseline photography, and to screen for vitiligo and thyroid autoimmunity when lesions are multiple. Sun protection of the depigmented area is essential. Counselling should address the natural history (the mole will fade and disappear, the halo will eventually repigment) and the benign prognosis.[4]
Adults
A first halo naevus in an adult, especially over 40, is unusual; the priority is to exclude melanoma with regression by dermoscopy and biopsy if there is any atypical feature or if the lesion is solitary without a central naevus.[3][7] The generalised halo phenomenon in an adult also warrants a full skin examination for occult melanoma.[3]
Darker phototypes
In darker phototypes (Fitzpatrick IV–VI), the depigmented halo is more visually striking and may cause greater cosmetic distress; repigmentation can be incomplete and postinflammatory hyperpigmentation can complicate any inflammatory treatment. Sun protection is essential. Topical calcineurin inhibitors are preferred over topical corticosteroids on the face and folds, and excimer laser can be effective for localised lesions.[6]
Patients with autoimmune disease
Patients with known vitiligo, autoimmune thyroid disease, type 1 diabetes, Addison's disease, or alopecia areata are more likely to develop halo naevi. These patients should be examined for new halo naevi (which are usually benign and need no treatment) and counselled about the shared autoimmune mechanism. Coexistent thyroid disease should be managed on its own merits.[1]
Immunocompromised patients and pregnancy
Halo naevi are not specifically increased in the immunocompromised, but any new atypical pigmented lesion should be examined carefully. Pregnancy does not specifically affect halo naevi, but any pigmented lesion arising or changing in pregnancy still requires dermoscopy to exclude melanoma. [1]
Evidence, Guidelines & Regional Differences
Key evidence
The classic clinicopathological framework was established by the 1995 case series of 142 halo naevi (Mooney, Barr, Buxton), which defined the morphology, the symmetric halo, the natural four-stage history, and the broad range of lesions that can carry the halo phenomenon — distinguishing "halo naevus" (classic Sutton's naevus) from the wider "halo phenomenon".[5] The 2015 review (Weyant, Chung, Helm) consolidates the clinicopathological criteria, the histology (dense CD8+ lymphocytic infiltrate embracing naevus cells, regression, melanophages), the differential from melanoma, and the management ladder — and remains the best single modern reference.[1] The 2024 Scientific Reports study (Hlača et al.) demonstrates marked upregulation of granulysin in both halo naevus and vitiligo skin, providing modern molecular evidence for the shared T-cell effector mechanism.[6] The 2022 review of nevus-associated melanoma (Dessinioti, Geller, Stratigos) frames the rare but critical scenario of a melanoma triggering a halo phenomenon, underpinning the rule to biopsy atypical or solitary adult halos.[3] A 2018 case report (Langford, Al-Ghazal) and a 2023 report of agminated halo naevus (Hassab-El-Naby, Rageh) document the diagnostic difficulty of distinguishing a benign halo naevus from a regressed melanoma and the rare agminated pattern.[7][8]
Regional differences
[1] [1]Across Europe (EADV) and in Australia (ACD), the approach is consistent with the UK/US: reassure typical lesions, biopsy atypical ones. In India and South Asia (IADVL), where the burden of vitiligo is high and the social consequences of depigmentation are significant, there is greater emphasis on screening for vitiligo and thyroid autoimmunity when multiple halo naevi appear, and on cosmetic camouflage and NB-UVB for the persistent halo. In all regions the cardinal rule is the same: a solitary halo without a central naevus in an adult must be biopsied.[4]
Controversies
The main controversies are minor. First, whether any treatment is warranted for the persistent halo in a child — most authorities recommend reassurance and camouflage over active treatment, reserving topical calcineurin inhibitors or excimer laser for cases of significant cosmetic distress. Second, the threshold for biopsy of an atypical lesion in a child: some clinicians biopsy aggressively to exclude a Spitzoid lesion or melanoma, while others rely on dermoscopy and short-interval follow-up, accepting a small residual uncertainty to avoid scarring. Third, the optimal screening strategy for autoimmune associations (how extensive the workup should be) varies; most guidelines recommend TSH and anti-TPO and a full skin examination, with further testing only if clinically indicated.[1]
Exam Pearls
Exam application bank (NEET-PG / INICET)
One-line answer
Halo naevus (Sutton's naevus, leucoderma acquisitum centrifugum) is a benign acquired melanocytic naevus surrounded by a symmetric, well-demarcated depigmented (white) halo, caused by autoimmune CD8+ cytotoxic T-cell-mediated destruction of both naevus melanocytes and the surrounding normal epidermal melanocytes (target antigens Melan-A/MART-1, gp100, tyrosinase). Prevalence is around 1 per cent, predominantly in children and adolescents (average age 15), on the trunk, and usually multiple. Associated with vitiligo (up to a quarter of cases) and autoimmune thyroid disease (Hashimoto's, anti-TPO). Natural history is benign and self-limiting in four stages: naevus with developing halo, fading naevus, disappearance of naevus leaving a depigmented macule, and gradual repigmentation of the halo over months to years. Management is reassurance, observation and sun protection; no treatment is ne
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard. [1]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes. [1]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change. [1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each. [1]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory. [1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Halo naevus (Sutton's naevus).
Self-test: A 45-year-old woman presents with a single round depigmented macule on her back, 8 mm across, with no central pigmented lesion. It appeared over three months. What is your concern and what must you do?
The concern is melanoma with regression — a fully regressed melanoma can leave a depigmented halo with no visible residual tumour, closely mimicking a halo naevus. Unlike a halo naevus, this is a solitary lesion in an adult with no central naevus, which are the three red flags. The correct action is to perform a full skin examination for a primary melanoma elsewhere (the halo may be a paraneoplastic immune response), and to biopsy the depigmented lesion — preferably an excisional biopsy — for histology. Even if no melanoma cells remain, the histology may show melanophages and a lymphocytic infiltrate consistent with a regressed melanoma, which still requires staging and surveillance. Never reassure a solitary adult halo without histology.[3][7]
References
- [1]Weyant GW, Chung CG, Helm KF. Halo nevus: review of the literature and clinicopathologic findings Int J Dermatol, 2015.PMID 26146814
- [2]Ko E, Panchal N. Pigmented Lesions Dermatol Clin, 2020.PMID 32892857
- [3]Dessinioti C, Geller AC, Stratigos AJ. A review of nevus-associated melanoma: What is the evidence? J Eur Acad Dermatol Venereol, 2022.PMID 35857388
- [4]Bandyopadhyay D. Halo nevus Indian Pediatr, 2014.PMID 25362030
- [5]Mooney MA, Barr RJ, Buxton MG. Halo nevus or halo phenomenon? A study of 142 cases J Cutan Pathol, 1995.PMID 7499574
- [6]Hlača N, Vičić M, Kaštelan M, et al. Analysis of granulysin expression in vitiligo and halo-nevus Sci Rep, 2024.PMID 39020008
- [7]Langford MA, Al-Ghazal SK. Halo naevus or malignant melanoma: A case report JPRAS Open, 2018.PMID 32158818
- [8]Hassab-El-Naby HMM, Rageh MA. Agminated Halo Nevus: A Novel Presentation Am J Dermatopathol, 2023.PMID 36939134