Dermatology · Medicine
Leprosy (Hansen disease)
Also known as Hansen disease · Tuberculoid leprosy · Lepromatous leprosy · Borderline leprosy · Type 1 (reversal) and type 2 (erythema nodosum leprosum) reactions
Leprosy (Hansen disease) is a chronic mycobacterial infection by Mycobacterium leprae (and M. lepromatosis) with tropism for skin and peripheral nerves, classified across an immunological spectrum from tuberculoid (paucibacillary, strong cell-mediated immunity) to lepromatous (multibacillary, anergy). Fellowship-level assessment demands mastery of the Ridley-Jopling classification and ILC (Indian classification), hypopigmented anaesthetic skin lesions with thickened nerves, slit-skin-smear and histopathological diagnosis, WHO multidrug therapy (rifampicin, dapsone, clofazimine) by paucibacillary/multibacillary regimen, the immunological type 1 (reversal) and type 2 (erythema nodosum leprosum) reactions and their distinct management (corticosteroids vs thalidomide), nerve damage and disability prevention, and public-health elimination strategies.
On this page & tools
Your progress
Saved locally on this device.
Exam tags
Red flags
Overview
Leprosy (Hansen disease) is a chronic mycobacterial infection by Mycobacterium leprae (and the related M. lepromatosis) with a characteristic tropism for skin and peripheral nerves. Its clinical expression spans an immunological spectrum from tuberculoid (paucibacillary, strong cell-mediated immunity) to lepromatous (multibacillary, anergy), with borderline forms in between. Fellowship-level competence requires mastery of the classification, the hypopigmented anaesthetic lesions with thickened nerves, slit-skin-smear/histology/PCR diagnosis, WHO multidrug therapy (MDT), the distinct type 1 and type 2 reactions and their management, nerve damage and disability prevention, and public-health elimination.[1][2][3]

Quick numbers for the examiner
TREAT EARLY — prevention of leprosy disability
Ulnar at elbow, common peroneal at fibular head, greater auricular at neck, posterior tibial at medial malleolus
Type 1: reversal; inflamed existing lesions + neuritis. Type 2: ENL; new tender nodules + systemic features
Lagophthalmos, corneal anaesthesia, iritis, cataract; eye checks every 6 months
Loss of sensation leads to trauma, burns, ulcers; footwear inspection, MCR shoes
Foot ulcers get infected quickly; antibiotics; rest; debridement; avoid amputation
Patient education: daily foot inspection, emollient for dry skin, comfortable shoes, self-care
Eyes, hands, feet; grade 0 = none, 1 = anaesthesia, 2 = visible deformity/visible damage
Corticosteroids for type 1; thalidomide/corticosteroids for type 2; clofazimine adjunctive
Daily inspection; treat cracks early; orthotics; MCR shoes
Voluntary muscle testing (VMT); monofilament test; record deterioration
Pathophysiology and microbiology [1]

Mycobacterium leprae is an obligate intracellular, acid-fast bacillus with tropism for Schwann cells of peripheral nerves and skin macrophages (cooler tissues). Its long doubling time (~14 days) explains the chronic, indolent course. Transmission is thought to occur via prolonged close contact and respiratory droplets (lepromatous disease is highly bacilliferous); most people are naturally resistant. The clinical spectrum reflects the host's cell-mediated immunity: a strong Th1 response produces tuberculoid (paucibacillary) disease with granulomas and few bacilli, while anergy produces lepromatous (multibacillary) disease with abundant bacilli, foamy macrophages, and poor granuloma formation.[3][6][7]
Classification (Ridley-Jopling spectrum)
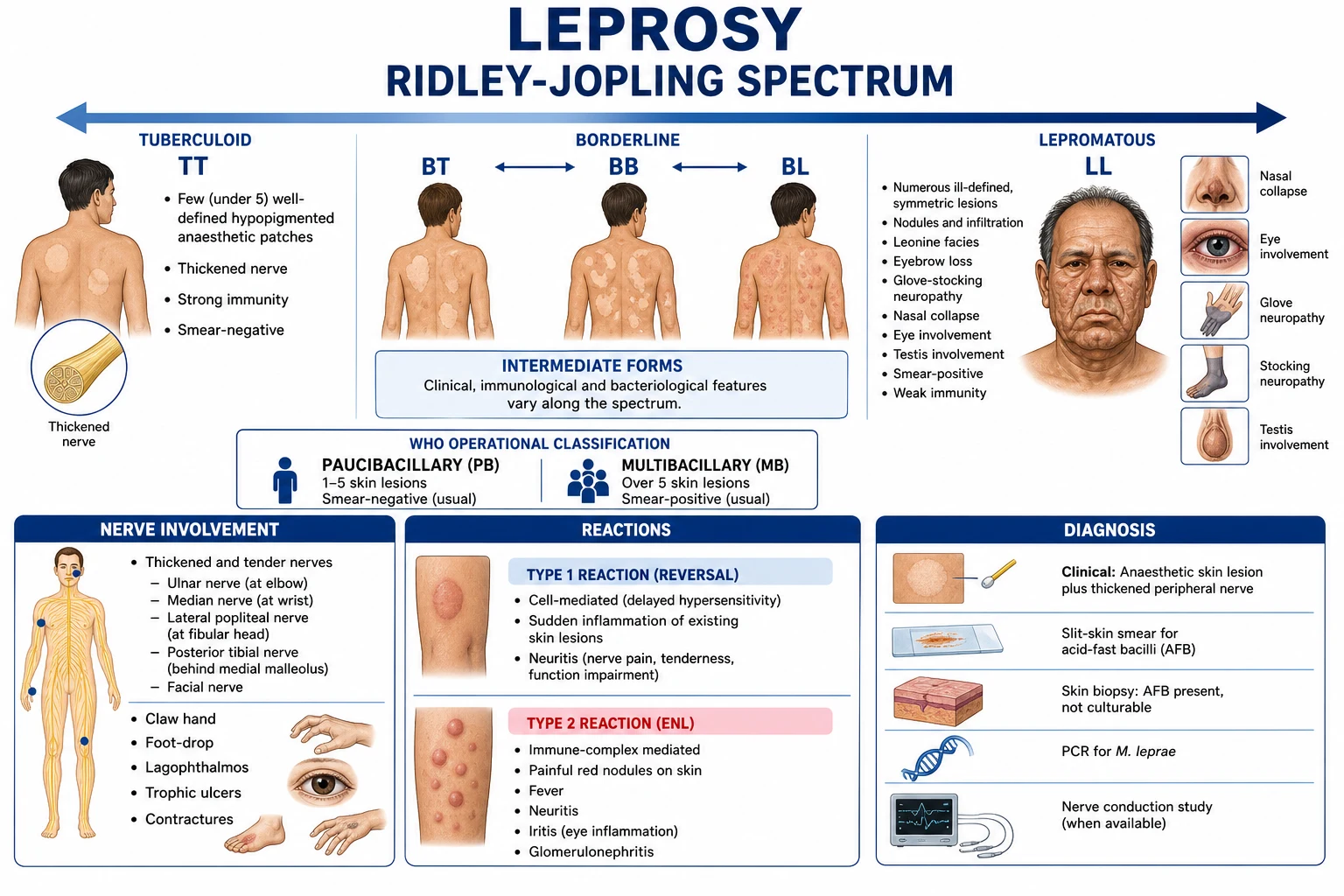
The Ridley-Jopling spectrum is the immunological classification that places patients along a continuum determined by their cell-mediated immune response to M. leprae antigens. It is the classification the examiner expects, and it must be distinguished from the operational WHO paucibacillary/multibacillary grouping that drives MDT duration. The full spectrum has six Ridley-Jopling poles plus one unstable early form:[1][9][12]
- Tuberculoid (TT, polar tuberculoid) — single (occasionally up to 3) large, well-demarcated, hypopigmented or erythematous anaesthetic plaque with raised erythematous borders and central hypopigmentation; a single thickened peripheral nerve in the vicinity of the lesion. Strong Th1 cell-mediated immunity; granulomas with epithelioid cells, Langhans giant cells, and erosion of the epidermis; bacterial index (BI) 0 (no bacilli on slit-skin smear); lepromin (Mitsuda) test strongly positive (≥5 mm); classification paucibacillary. Stable; rarely downgrades; type 1 reversal reactions are uncommon.
- Borderline tuberculoid (BT) — several asymmetric, well-defined hypopigmented/erythematous plaques, all with definite sensory loss; satellite lesions around a larger lesion are characteristic; multiple thickened peripheral nerves (ulnar, common peroneal, greater auricular). Granulomas with epithelioid cells, but less organised than TT; BI 0-1+; lepromin weakly positive. Classified multibacillary by WHO (>5 lesions) but functionally closer to TT; unstable and the most prone to type 1 reversal reactions, especially during the first 6-12 months of MDT.
- Mid-borderline (BB) — numerous annular "punched-out" or "target" lesions with a well-defined erythematous outer ring, a relatively normal midzone, and a hypopigmented anaesthetic centre (the classic "Swiss cheese" appearance); asymmetry preserved. Granulomas with epithelioid cells but no giant cells; lymphocytes are present but do not organise into a compact granuloma; BI 2-3+; lepromin negative. The most immunologically unstable pole; can upgrade to BT or downgrade to BL/LL; type 1 reactions common.
- Borderline lepromatous (BL) — many symmetric, ill-defined, shiny, hypopigmented or erythematous macules, papules, plaques, and nodules; sensory loss is patchy and less obvious than in BT. Numerous bacilli in macrophages; poorly formed granulomas with a few epithelioid cells and many lymphocytes that do not invade the epidermis; BI 3-4+; lepromin negative. Classified multibacillary; at high risk of both type 1 (downgrade) and type 2 ENL reactions.
- Lepromatous (LL, polar lepromatous) — diffuse, symmetric infiltration of the skin with macules, papules, plaques, and nodules; leonine facies (thickened, corrugated facial skin with deep nasolabial folds); madarosis (lateral eyebrow loss, progressing to complete loss); saddle-nose deformity from septal cartilage destruction; testicular atrophy, gynaecomastia, infertility; ichthyosis-like dry skin on the legs; widespread bacilli with foamy (Virchow/lepra) cells containing globi (clumps of bacilli); BI 4-6+; lepromin negative. Anergy; Th2-dominated antibody response that fails to control the bacillus; multibacillary. Lucio phenomenon is a particular necrotising cutaneous reaction seen predominantly in diffuse LL (see below).
- Indeterminate (I) leprosy — an early, unstable form with a single, faint, hypopigmented macule, often on the face or exposed limb; sensory loss may be equivocal, nerve thickening usually absent, slit-skin smear usually negative. About 70-80% of indeterminate cases resolve spontaneously (often misdiagnosed as pityriasis alba), 20-30% evolve along the spectrum toward TT or LL. PCR for M. leprae DNA and a positive lepromin favour evolution toward TT; anergy favours evolution toward LL.[9][12]
- Pure neuritic leprosy (a WHO category, not in the original Ridley-Jopling spectrum) — peripheral nerve involvement without cutaneous lesions; thickened tender nerves with sensory and motor loss; biopsy of the affected nerve or a pure sensory nerve shows granulomatous neuritis with AFB; classified PB or MB by nerve biopsy bacterial index.
Operationally, the WHO classifies disease as paucibacillary (PB: up to 5 lesions, slit-skin-smear negative at all sites) or multibacillary (MB: 6 or more lesions, OR slit-skin-smear positive at any site) to guide MDT duration. The two systems must not be confused: a BT patient with 7 lesions is operationally MB and receives 12-month MDT, even though immunologically they sit at the tuberculoid pole.[1][4][9]
Clinical features
Type 1 reversal reaction mnemonic
- Skin — hypopigmented or erythematous plaques/macules with loss of sensation (the cardinal sign); distribution and number reflect the classification. Leonine facies and nodules in lepromatous disease.[2][12]
- Nerves — thickened, tender peripheral nerves (ulnar, median, common peroneal, posterior auricular, radial cutaneous) with anaesthesia and motor weakness leading to claw hand, foot drop, and plantar ulceration (disability).
- Mucosa/systemic — nasal mucosal involvement (epistaxis, saddle-nose), eye involvement (lagophthalmos, keratitis, blindness), testicular atrophy, and (in LL) amyloidosis.
Diagnosis
- Cardinal signs: (1) hypopigmented/erythematous skin lesions with definite loss of sensation, (2) thickened peripheral nerves, (3) acid-fast bacilli on slit-skin smear.
- Slit-skin smear (ear lobule, lesion) with Ziehl-Neelsen/Fite stain — bacillary load (bacterial index); positive in multibacillary disease.
- Skin biopsy histology — granulomatous dermatitis with perineural involvement and acid-fast bacilli (Fite-Faraco); confirms and classifies.[2]
- PCR for M. leprae DNA (research/confirmation).
- Lepromin test (Mitsuda) — assesses host immunity (not diagnostic; positive in tuberculoid).
Differential diagnosis
HANSEN'S HINTS — clinical features of leprosy
Cardinal sign; loss of sensation confirms leprosy vs other hypopigmented disorders
Temperature and light touch lost first; protective sensation absent; trauma and burns unnoticed
Ulnar at elbow; common peroneal at fibular head; greater auricular at neck
Hypopigmented or erythematous patch with definite sensory loss
Diffuse infiltration of earlobes in lepromatous disease
Firm nodules on face (leonine facies) and ears; characteristic of multibacillary disease
(mnemonic separator)
Bacterial index; AFB on Ziehl-Neelsen/Fite stain from earlobe or lesion
Pityriasis versicolor, pityriasis alba, vitiligo, post-inflammatory hypopigmentation, tinea corporis, cutaneous tuberculosis, sarcoidosis, granuloma annulare, leishmaniasis, and (for nodules) neurofibromatosis. The anaesthesia and thickened nerves are the cardinal distinguishing features.[2][13]
Management
Multidrug therapy (MDT) — WHO regimen (doses for adults, monthly blister packs)
The current WHO regimen (provided free as monthly calendar blister packs through national leprosy programmes) is the same as first introduced in 1981. All doses are taken under direct observation on the named day; unsupervised daily doses are self-administered. The duration is fixed regardless of clinical improvement. [1]
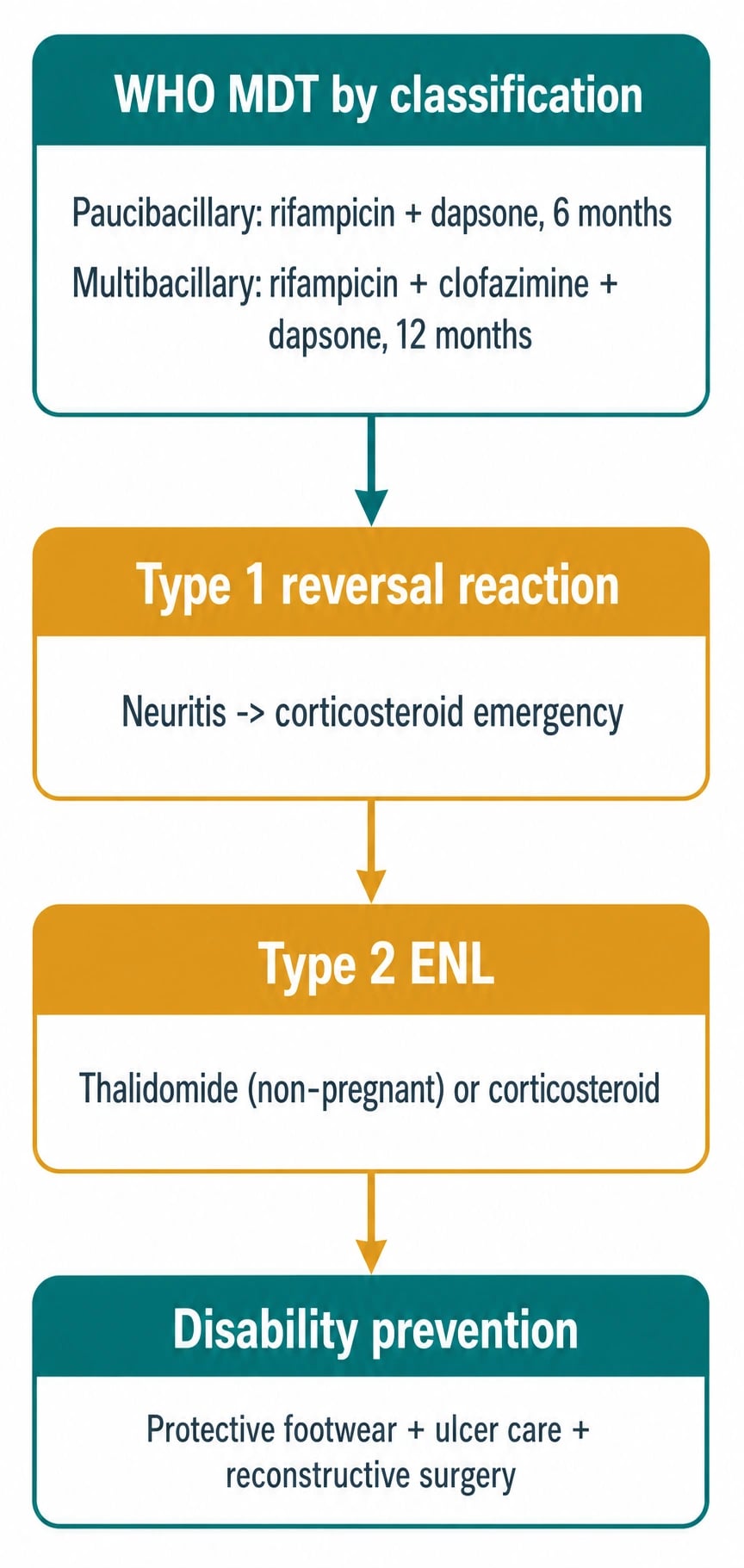
- Paucibacillary (PB) — adult PB blister pack, 28 days × 6 cycles (6 months total):
- Rifampicin 600 mg orally once monthly, supervised (450 mg if adult weight < 35 kg).
- Dapsone 100 mg orally daily, unsupervised (50 mg daily if adult weight < 35 kg).
- Single-dose rifampicin-ofloxacin-minocycline (ROM) is an alternative single-dose regimen for single-lesion PB leprosy in selected WHO programmes: rifampicin 600 mg + ofloxacin 400 mg + minocycline 100 mg, all single oral dose under observation.
- Multibacillary (MB) — adult MB blister pack, 28 days × 12 cycles (12 months total):
- Rifampicin 600 mg orally once monthly, supervised (450 mg if weight < 35 kg).
- Clofazimine 300 mg orally once monthly, supervised (150 mg if weight < 35 kg).
- Dapsone 100 mg orally daily, unsupervised (50 mg daily if weight < 35 kg).
- Clofazimine 50 mg orally daily, unsupervised (taken between supervised monthly doses; this additional daily clofazimine is what produces the characteristic reddish-brown skin pigmentation in MB patients on therapy).
- Child dose adjustment (10-14 years): rifampicin 450 mg monthly, dapsone 50 mg daily, clofazimine 150 mg monthly and 50 mg alternate-day. Paediatric blister packs are pre-prepared.
- MDT renders the patient non-infectious within days of the first supervised dose (single-dose ROM is non-infectious by 24 h); MDT is provided free by WHO and supplied through national programmes.
- Monitoring: monthly clinical review for nerve function and reaction; slit-skin smear at 6 and 12 months for MB; liver function tests if signs of dapsone or rifampicin toxicity (haemolysis, hepatitis, drug rash).[1][4][5][10]
Leprosy reactions (immunological, not treatment failure)
- Type 1 (reversal) reaction — a delayed-hypersensitivity flare in borderline disease, with red, swollen, tender existing lesions and acute neuritis (nerve tenderness, new weakness); an emergency managed with oral corticosteroids (prednisolone 40-60 mg, tapering over months) to prevent irreversible nerve damage; continue MDT.[8]
- Type 2 reaction (erythema nodosum leprosum, ENL) — an immune-complex phenomenon of borderline-lepromatous/lepromatous disease, with crops of tender erythematous nodules, fever, neuritis, iritis, orchitis, dactylitis; managed with thalidomide (non-pregnant, with contraception/pregnancy-prevention), corticosteroids, or clofazimine.[8]
- Type 1 (reversal) reaction — detailed management:
- Mechanism: type IV delayed hypersensitivity (Th1 / CD4+ T-cell) directed at M. leprae antigens in borderline (BT/BB/BL) disease, occurring in 25-30% of borderline cases, usually within the first 6-12 months of MDT ("upgrading" reaction) or rarely as a "downgrading" reaction before MDT.
- Clinical features: sudden redness, swelling, induration, and tenderness of pre-existing skin lesions; new lesions may appear; new or worsening nerve tenderness (palpate ulnar at the elbow, common peroneal at the fibular head, median at the wrist, posterior tibial at the medial malleolus); new sensory loss; new motor weakness (small muscles of the hand, foot dorsiflexion, eyelid closure); oedema of hands, feet, or face. A reaction with neuritis is a steroid emergency: within hours of onset, urgent prednisolone can prevent permanent paralysis.
- Treatment: prednisolone 0.5-1 mg/kg/day (typically 40-60 mg adult, 1 mg/kg child) orally, continued for 3-6 months (typical course 12-24 weeks), then slow taper (no faster than 5 mg every 2 weeks). MDT must continue. Adjuncts: limb splinting in functional position, analgesia (paracetamol, amitriptyline for neuropathic pain), physiotherapy.
- Severe/refractory neuritis: consider IV methylprednisolone pulses, azathioprine 50-150 mg/day or cyclosporine 3-5 mg/kg/day as steroid-sparing agents; decompressive surgery for nerve abscesses (rare).
- Type 2 reaction (erythema nodosum leprosum, ENL) — detailed management:
- Mechanism: type III immune-complex hypersensitivity (antigen-antibody-complement) in BL/LL disease, occurring in 20-50% of LL patients; can be acute (single episode, less than 6 months), recurrent (≥2 episodes), or chronic (continuing more than 6 months despite therapy).
- Clinical features: crops of tender, erythematous, evanescent subcutaneous nodules on the trunk, face, and extensor surfaces of limbs (unlike type 1, nodules are NEW lesions, not inflamed pre-existing plaques); fever, malaise, arthralgia; neuritis (in 10-20%); iritis/uveitis (slit-lamp examination mandatory); orchitis (testicular pain and swelling); dactylitis; lymphadenitis; proteinuria (renal immune-complex deposition).
- First-line (non-pregnant men and post-menopausal women, no reliable contraception in women of childbearing potential): thalidomide 100-400 mg/day orally (start 100 mg nocte, titrate up by 100 mg every 2-4 days to control symptoms, typical maintenance 50-200 mg/day). Thalidomide is the only FDA-approved drug for ENL. Mandatory Pregnancy Prevention Programme: two forms of contraception, monthly pregnancy tests, and prescriber registration in iPLEDGE/equivalent; absolutely contraindicated in pregnancy (phocomelia).
- Pregnancy and women of childbearing potential: prednisolone 0.5-1 mg/kg/day (typically 30-60 mg/day), taper over weeks to months. Thalidomide is teratogenic; alternative clofazimine high-dose (300 mg daily reducing to 50 mg daily) is slower but safe in pregnancy.
- Adjunctive clofazimine: clofazimine 100-300 mg/day as adjunctive therapy, especially in recurrent or chronic ENL; takes 4-6 weeks to be effective; not useful for acute control.
- Refractory or chronic ENL: pentoxifylline 400 mg three times daily (TNF-α inhibition); colchicine 0.6-1.2 mg/day; azathioprine 50-150 mg/day or methotrexate 7.5-15 mg/week as steroid-sparing agents; anti-TNF agents (infliximab, etanercept) for life-threatening refractory ENL; ciclosporin 3-5 mg/kg/day. Continue MDT throughout; do not stop.[1][8][12]
WHO disability grading (EHF score)
The WHO disability grading is a standardised three-tier classification applied independently to each of the six sites (each eye, each hand, each foot). The maximum total score is 12 (0 = no disability anywhere; 12 = grade 2 at all six sites). It must be documented at diagnosis, at completion of MDT, and at every reaction assessment, and is the principal audit indicator for leprosy control programmes worldwide. The grader's hands should be warm and a 10 g Semmes-Weinstein monofilament should be used for sensory testing.[8][11]
- Eyes (each scored 0, 1, or 2):
- Grade 0: no eye problem due to leprosy; vision 6/60 or better (can count fingers at 6 metres).
- Grade 1: eye problem due to leprosy present but vision not severely affected; includes lagophthalmos, corneal anaesthesia, chronic iritis, but vision 6/60 or better (can count fingers at 6 m).
- Grade 2: severe visual impairment (vision worse than 6/60, cannot count fingers at 6 m), including blindness, lagophthalmos with exposure keratitis, dense corneal opacity, mature cataract from chronic iritis.
- Hands (each scored 0, 1, or 2):
- Grade 0: no anaesthesia, no visible deformity or damage.
- Grade 1: anaesthesia present (loss of protective sensation on palm with 10 g monofilament or cotton wisp) but no visible deformity or damage. The single most common disability grade on diagnosis.
- Grade 2: visible deformity or damage present — claw hand (ulnar ± median nerve palsy), contractures, wounds/ulcers, amputation of digits, absorption of phalanges, wrist drop (radial nerve), contracture from burn or trauma unnoticed in the anaesthetic hand.
- Feet (each scored 0, 1, or 2):
- Grade 0: no anaesthesia, no visible deformity or damage.
- Grade 1: anaesthesia present (10 g monofilament test on sole fails at one or more of the 10 standard sites) but no visible deformity or damage.
- Grade 2: visible deformity or damage present — foot drop (common peroneal nerve palsy, high-stepping gait), plantar ulceration (mal perforans, often under the 1st metatarsal head or heel), claw toes, contractures, absorption/shortening of toes, Charcot joint, amputation.
- Maximum score = 12 (grade 2 at all six sites). The score is recorded as a single number (sum of all six sites) on the WHO patient record card; an increase of ≥1 point during MDT is a sentinel event triggering urgent nerve-function review. [1]
E-H-F 0-1-2 — the WHO disability grading
Grade 0: no leprosy eye problem, vision 6/60 or better; Grade 1: lagophthalmos, corneal anaesthesia, iritis, vision still 6/60 or better; Grade 2: vision worse than 6/60 — blindness, dense corneal opacity, mature cataract
Grade 0: normal; Grade 1: ANAESTHESIA only (10 g monofilament); Grade 2: CLAW HAND, contractures, ulcers, wounds, amputation, absorption
Grade 0: normal; Grade 1: ANAESTHESIA only (10 g monofilament sole test); Grade 2: FOOT DROP, plantar ulcer (mal perforans), claw toes, Charcot joint, amputation
No anaesthesia, no deformity, vision intact
Loss of protective sensation only; often reversible with treatment and self-care
Claw hand, foot drop, ulcer, contracture, amputation, blindness — usually irreversible
Complications of nerve damage and disease
The cumulative lifetime complication rate in untreated or inadequately-treated leprosy is 30-50%, and these complications are what make leprosy the leading infectious cause of disability worldwide before tuberculosis. They are classified into primary nerve palsies, secondary consequences of anaesthesia, ocular complications, systemic complications, and chronic sequelae of reactions.[2][8][12]
- Primary peripheral nerve palsies (the immediate consequences of M. leprae invasion of Schwann cells and granulomatous neuritis):
- Ulnar nerve palsy at the elbow — most common nerve lesion; produces claw hand (hyperextension at the MCP joints, flexion at the IP joints of the 4th and 5th digits from unopposed long flexors), wasting of the first dorsal interosseous, sensory loss on the ulnar border of the hand and the little finger. "Ulnar claw + ulnar border sensory loss" is the registrar-level buzzword.
- Median nerve palsy at the wrist — adds thenar wasting (loss of thumb opposition), sensory loss on the radial palm and the index/middle fingers; combined ulnar + median produces a total claw hand with loss of all intrinsic hand function.
- Common peroneal (lateral popliteal) nerve palsy at the fibular head — produces foot drop (loss of ankle dorsiflexion and eversion, high-stepping gait, "foot slap"), sensory loss on the dorsum of the foot and the lateral shin. Most common lower-limb nerve lesion.
- Posterior tibial nerve palsy behind the medial malleolus — loss of intrinsic foot muscle function, sensory loss on the sole; combined with the foot drop above this produces a flail, anaesthetic, ulcer-prone foot.
- Facial (VII) nerve palsy — zygomatic and temporal branches — lagophthalmos (inability to close the eye, "rabbit eye"), loss of corneal reflex (corneal anaesthesia from trigeminal involvement), exposure keratitis, corneal ulceration, and ultimately blindness.
- Greater auricular nerve thickening over the sternocleidomastoid — a useful diagnostic sign.
- Radial cutaneous nerve of the forearm — sensory loss on the radial dorsum of the hand; rarely motor.
- Posterior auricular nerve — Earlobe sensory loss.
- Secondary consequences of anaesthesia (the disabling cascade that follows loss of protective sensation):
- Plantar ulceration (mal perforans pedis) — repetitive, unnoticed trauma on the anaesthetic sole leads to callus formation, sub-callus haemorrhage, ulceration, deep infection, osteomyelitis, and ultimately amputation. The classic site is under the 1st metatarsal head or the heel. Prevention is the cornerstone of disability prevention.
- Hand injuries — burns from cooking pots, cuts from tools, recurrent infections, contractures, and digital absorption ("licking" of digits).
- Charcot (neuropathic) joint in the foot and, less commonly, the hand — painless destruction with deformity, subluxation, and ultimately a "bag of bones" foot.
- Wrist drop, foot drop, claw hand, claw toes — motor sequelae of chronic nerve damage.
- Ocular complications (the second commonest cause of disability):
- Lagophthalmos (5th and 7th nerve involvement).
- Exposure keratitis and corneal ulceration from lagophthalmos.
- Corneal anaesthesia from trigeminal involvement, allowing unnoticed trauma.
- Chronic iritis/uveitis from ENL or chronic smouldering disease; eventual synechiae, glaucoma, and cataract.
- Madarosis (loss of eyebrows and lashes) — cosmetic but also impairs protection against dust.
- Cataract — accelerated by chronic iritis; the leading cause of blindness in long-term leprosy.
- Ultimately blindness (the most feared complication in endemic communities).
- Systemic complications (predominantly LL):
- Nasal septal perforation, saddle-nose deformity from chronic mucosal infiltration.
- Testicular atrophy, gynaecomastia, infertility from direct M. leprae invasion of the testes and consequent hypogonadism (LL); elevated LH and FSH; impotence.
- Renal amyloidosis (AA type) — a late, life-threatening complication of long-standing LL/ENL, secondary to chronic inflammation; presents with nephrotic syndrome, renal failure; historically a leading cause of death in LL patients.
- Chronic or recurrent ENL — the most common reason for prolonged corticosteroid dependence; can persist for years after MDT completion.
- Latex-fruit syndrome and other immunological complications (less common): type I hypersensitivity to M. leprae antigens cross-reacting with environmental allergens. [1]
Clinical pearl
[1]Red flags
Exam application bank (NEET-PG / INICET)
One-line answer
Leprosy (Hansen disease) is a chronic mycobacterial infection by Mycobacterium leprae (and M. lepromatosis) with tropism for skin and peripheral nerves, classified across an immunological spectrum from tuberculoid (paucibacillary, strong cell-mediated immunity) to lepromatous (multibacillary, anergy). Fellowship-level assessment demands mastery of the Ridley-Jopling classification and ILC (Indian classification), hypopigmented anaesthetic skin lesions with thickened nerves, slit-skin-smear and histopathological diagnosis, WHO multidrug therapy (rifampicin, dapsone, clofazimine) by paucibacillary/multibacillary regimen, the immunological type 1 (reversal) and type 2 (erythema nodosum leprosum) reactions and their distinct management (corticosteroids vs thalidomide), nerve damage and disability prevention, and public-health elimination strategies.
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard. [1]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes. [1]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change. [1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each. [1]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory. [1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Leprosy (Hansen disease).
[1]References
- [1]Grijsen ML, Nguyen TH, Pinheiro RO, et al. Leprosy Nat Rev Dis Primers, 2024.PMID 39609422
- [2]Maymone MBC, Laughter M, Venkatesh S, et al. Leprosy: Clinical aspects and diagnostic techniques J Am Acad Dermatol, 2020.PMID 32229279
- [3]Britton WJ, Lockwood DN. Leprosy Lancet, 2004.PMID 15081655
- [4]Chen KH, Lin CY, Su SB, et al. Leprosy: A Review of Epidemiology, Clinical Diagnosis, and Management J Trop Med, 2022.PMID 35832335
- [5]Li X, Ma Y, Li G, et al. Leprosy: treatment, prevention, immune response and gene function Front Immunol, 2024.PMID 38440733
- [6]Mungroo MR, Khan NA, Siddiqui R. Mycobacterium leprae: Pathogenesis, diagnosis, and treatment options Microb Pathog, 2020.PMID 32931893
- [7]Sugawara-Mikami M, Tanigawa K, Kawashima A, et al. Pathogenicity and virulence of Mycobacterium leprae Virulence, 2022.PMID 36326715
- [8]Ebenezer GJ, Scollard DM. Treatment and Evaluation Advances in Leprosy Neuropathy Neurotherapeutics, 2021.PMID 34799845
- [9]Alrehaili J. Leprosy Classification, Clinical Features, Epidemiology, and Host Immunological Responses: Failure of Eradication in 2023 Cureus, 2023.PMID 37809252
- [10]Gupte M. Global leprosy scenario: Eradication, elimination or control? Indian J Med Res, 2023.PMID 37040220
- [11]Makhakhe L. Leprosy review S Afr Fam Pract (2004), 2021.PMID 34797098
- [12]Froes LAR Junior, Sotto MN, Trindade MAB. Leprosy: clinical and immunopathological characteristics An Bras Dermatol, 2022.PMID 35379512
- [13]Franco-Paredes C, Marcos LA, Henao-Martínez AF, et al. Cutaneous Mycobacterial Infections Clin Microbiol Rev, 2018.PMID 30429139