Dermatology · Medicine
Melanocytic pathology (naevus vs melanoma)
Also known as Naevus versus melanoma histology · Melanocytic lesion pathology · MPATH-Dx · Spitz pathology · Dysplastic naevus histology
Board-level dermatopathology leaf on distinguishing benign melanocytic naevi from melanoma and intermediate lesions. Covers biopsy strategy that preserves Breslow staging, architectural and cytologic criteria, special-site traps, Spitz spectrum, dysplastic naevi, MPATH-Dx reporting hierarchy, essential AJCC pathology elements, and ancillary immunohistochemistry including PRAME with known pitfalls.
On this page & tools
Your progress
Saved locally on this device.
Exam tags
Red flags
Definition & Scope
Melanocytic pathology is the histologic and molecular interpretation of lesions composed of melanocytes — from banal acquired naevi through intermediate/uncertain lesions to melanoma in situ (MIS) and invasive melanoma.[3][4] This leaf is the pattern and reporting companion to clinical topics on naevi, melanoma, and staging: it answers how the pathologist and clinician together avoid understaging and overtreatment.
| Category (teaching) | Prototype | Core message |
|---|---|---|
| Benign naevus | Common acquired, congenital, blue, Spitz (classic) | Maturation, symmetry, limited atypia |
| Intermediate / atypical | Dysplastic naevus, atypical Spitz tumour | Incomplete excision + expert review often needed |
| Malignant | MIS, invasive melanoma (including Spitz melanoma) | Full AJCC elements; oncology pathway |
Why Biopsy Technique Is Pathology
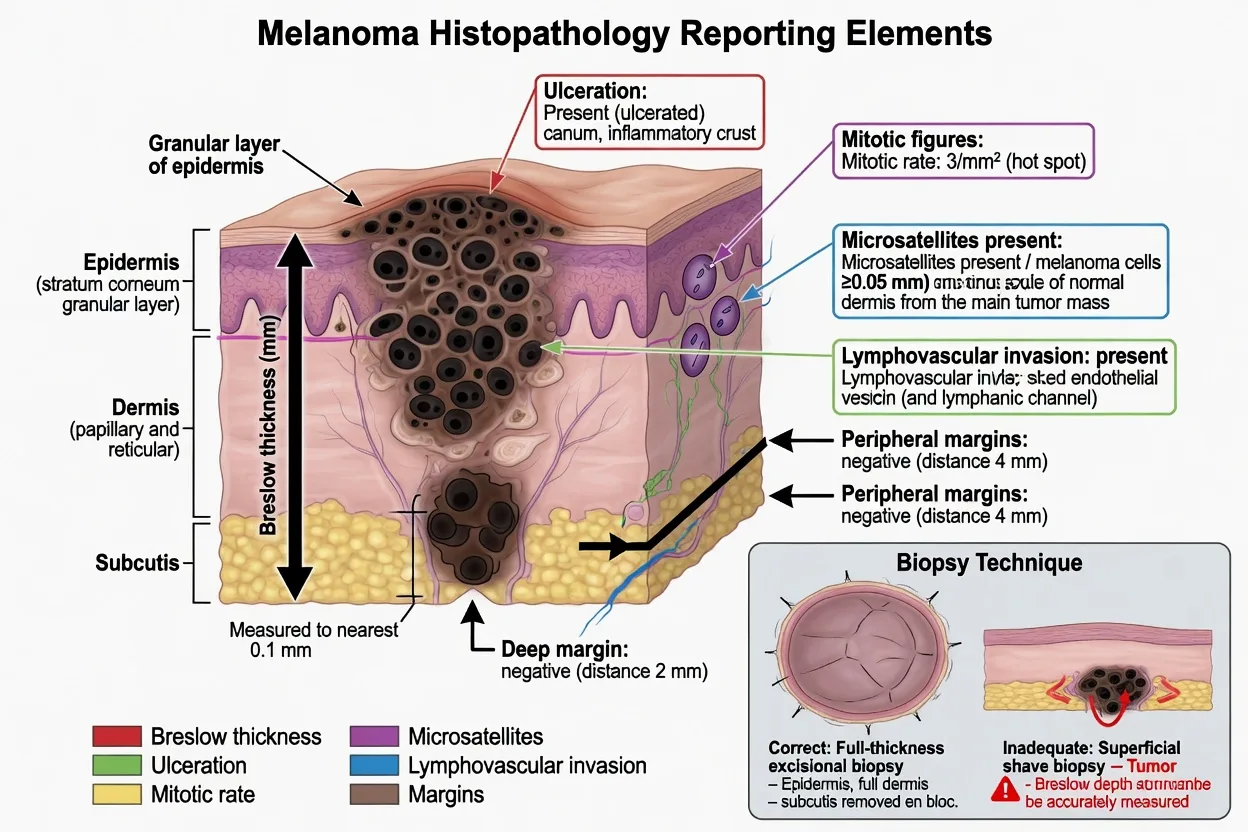
AJCC T category depends on Breslow thickness and ulceration measured on a full-thickness sample. Partial or superficial biopsies can understage invasive melanoma and distort subtype.[1][2][3]
Preferred for suspected melanoma: full-thickness excisional biopsy with narrow clinical margins (about 1–3 mm), oriented if helpful, submitted entirely.[2][3]
Acceptable with caution: deep saucerisation or punch when site/size preclude ellipse — report must state if the base is transected.[2]
Avoid as sole sample when melanoma is likely: incomplete superficial shave through the epidermis only. [1]
Exam application bank (NEET-PG / INICET)
One-line answer
Board-level dermatopathology leaf on distinguishing benign melanocytic naevi from melanoma and intermediate lesions. Covers biopsy strategy that preserves Breslow staging, architectural and cytologic criteria, special-site traps, Spitz spectrum, dysplastic naevi, MPATH-Dx reporting hierarchy, essential AJCC pathology elements, and ancillary immunohistochemistry including PRAME with known pitfalls.
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard. [1]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes. [1]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change. [1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each. [1]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory. [1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Melanocytic pathology (naevus vs melanoma).
Expanded exam teaching (depth pass)
Clinical reasoning
For Melanocytic pathology (naevus vs melanoma), examiners test whether you can prioritise life threats, choose the right first test, and give specific therapy (agent, dose, route, timing). Generic phrases without numbers score poorly.
Mechanism → feature map
Build a short chain: cause → pathophysiologic intermediate → clinical feature → complication. Every major symptom in the classic vignette should sit on that chain.
Investigation strategy
- Bedside/first-line tests that change immediate management
- Confirmatory or staging tests
- What a normal result does not exclude
- When not to delay treatment for imaging (unstable patient)
Management ladder
- Resuscitation / ABC / sepsis or haemorrhage bundle as relevant
- Specific antidote / procedure / antimicrobial / reperfusion / surgery
- Supportive care and monitoring targets
- Definitive long-term therapy and secondary prevention
- Disposition and safety-net advice
Special populations
Always prepare one line each for children, pregnancy, elderly, renal/hepatic impairment, and immunocompromised patients when the topic allows.
Pitfalls that fail candidates
- Treating the number not the patient
- Missing pregnancy status when relevant
- Imaging before stabilisation
- Wrong empiric cover or wrong antidote timing
- Incomplete counselling on recurrence, adherence, or red-flag return
Board-level dermatopathology leaf on distinguishing benign melanocytic naevi from melanoma and intermediate lesions. Covers biopsy strategy that preserves Breslow staging, architectural and cytologic criteria, special-site traps, Spitz spectrum, dysplastic naevi, MPATH-Dx reporting hierarchy, essential AJCC pathology elements, and ancillary immunohistochemistry including PRAME with known pitfalls. [1]
Structured revision sheet
Must-know numbers and names
List every score, size threshold, dose, and time window from this topic on a blank page from memory, then check against the sections above.
Three classic MCQ angles
- Most likely diagnosis given a vignette
- Next best step in management
- Most appropriate investigation
Three classic SAQ angles
- Pathophysiology in five steps
- Management algorithm with doses
- Complications and prevention
Clinical station flow
Greet → focused history → targeted exam → investigations → explain diagnosis → emergency care → definitive plan → safety-net / follow-up → answer examiner questions on mechanism and pitfalls.
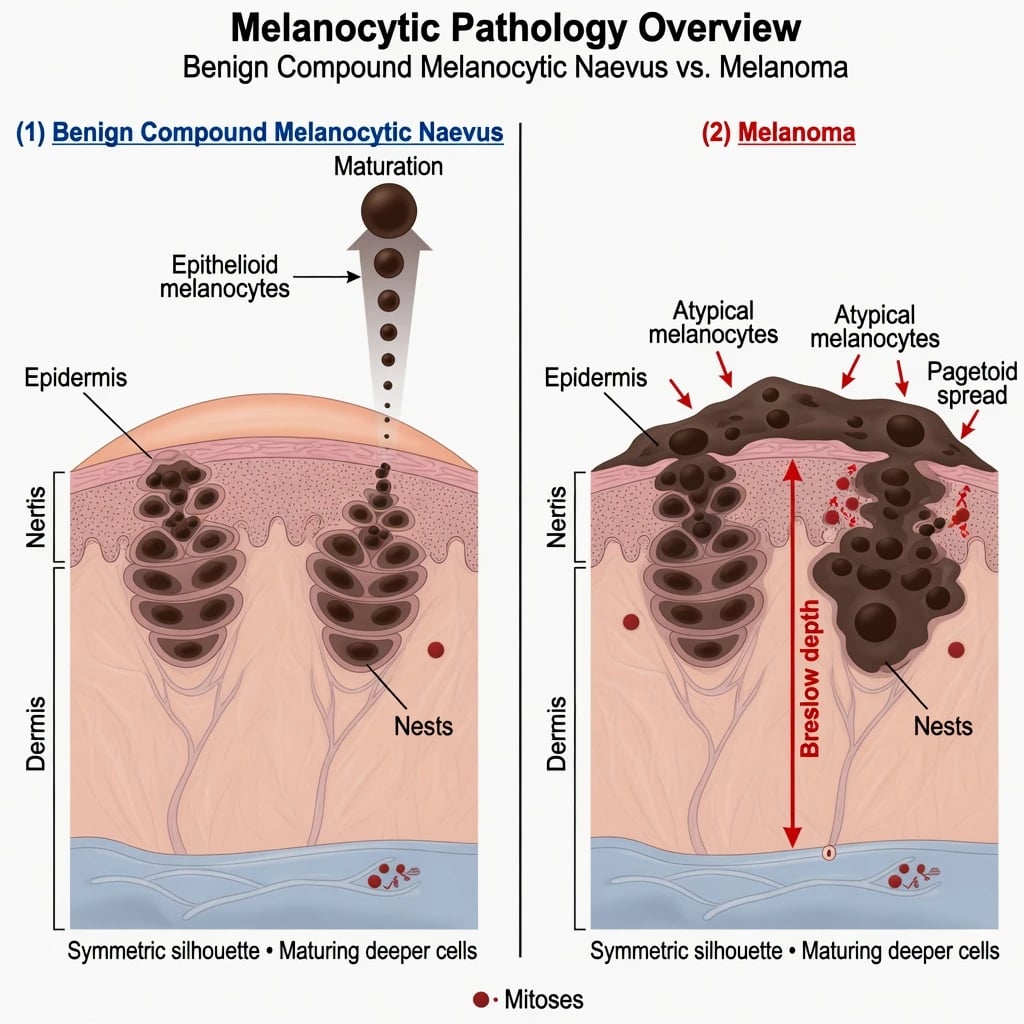
[1]Architecture-First Criteria (Naevus vs Melanoma)
Features that favour a benign naevus
- Overall symmetry and sharp lateral circumscription
- Nested growth that becomes smaller and more disperse with depth (maturation)
- Limited pagetoid scatter (if any), usually central and in appropriate clinical context (e.g. traumatised or special-site naevus)
- Low dermal mitotic rate, especially deep [1]
Features that raise concern for melanoma
- Asymmetry, poor circumscription, consumption of epidermis
- Sheet-like dermal growth without maturation
- Pagetoid melanocytes at edges or throughout
- Cytologic atypia with dermal mitoses (especially deep)
- Ulceration, regression with residual atypical cells, satellites [1]
No single feature is absolute; constellation + clinical data decide.[2][3][12]
Favours naevus
- Symmetric silhouette
- Maturation with depth
- Sharp borders
- Nested orderly growth
- Few/no deep mitoses
Favours melanoma
- Asymmetry / poor borders
- No maturation
- Pagetoid scatter at edges
- Sheet-like dermal growth
- Deep mitoses, ulceration
Essential Melanoma Report Elements
Pathology reports that feed AJCC staging should capture at least:[1][2]
| Element | Why it matters |
|---|---|
| Diagnosis + subtype | SS, nodular, lentigo maligna, acral, desmoplastic, etc. |
| Breslow thickness | Primary T driver — granular layer (or ulcer base) to deepest invasive cell |
| Ulceration | Defines a/b T subcategory |
| Dermal mitoses | Prognostic context (reporting practice varies by era/system) |
| Margins | Peripheral and deep clearance |
| Microsatellites / LVI / PNI | Upstages N or local risk |
| Regression, TIL, precursor naevus | Interpretation and residual risk context |
Dysplastic (Atypical) Naevi
Dysplastic naevi show architectural disorder and cytologic atypia short of melanoma; history, classification debates, and epidemiology are reviewed in contemporary JAAD series.[6] Exam stance:
- Mild dysplasia completely excised → often observation per local protocol
- Moderate–severe dysplasia or positive margins → re-excision commonly advised
- Severe dysplasia vs MIS can be subjective — clear clinical photos, dermoscopy, and expert review reduce harm [1]
Never use “dysplastic naevus” as a dustbin label for incompletely sampled melanoma. [1]
Spitz Spectrum
Spitz tumours range from classic Spitz naevus through atypical Spitz tumour to Spitz melanoma, with distinctive molecular drivers (including kinase fusions / HRAS in subsets) that differ from conventional BRAF-driven naevi.[7][8] Age matters: childhood Spitz naevi are common; adult Spitzoid lesions deserve higher suspicion and complete excision.[7][12]
Criteria re-evaluations continue to stress combined clinical, histologic, and molecular integration rather than any single mitotic cutoff.[12][8]
Special-Site and Morphologic Traps
| Trap | Why it mimics melanoma | Mitigation |
|---|---|---|
| Acral naevus | Manchu-line scatter, elongated rete | Know site norms; full clinical context |
| Genital / milk-line naevus | Atypia and irregular nests | Site-aware thresholds |
| Recurrent / persistent naevus | Traumatic scatter in scar | History of prior shave/excision |
| Naevoid melanoma | Subtle dermal atypia | Look for deep mitoses, sheet growth |
| Desmoplastic melanoma | Scar-like spindle cells | SOX10/S100; low Melan-A often |
| Partially sampled lesion | False “naevus” | Re-excise if clinical concern |
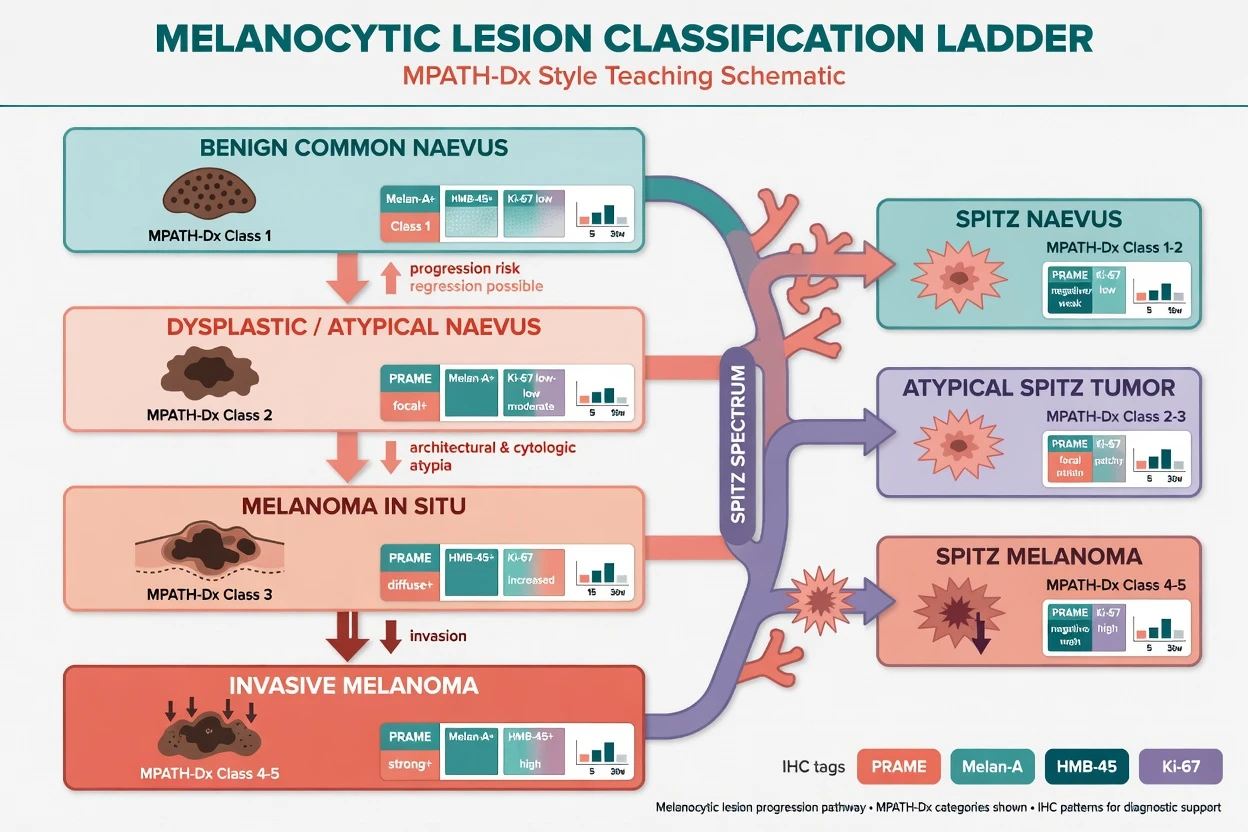
Immunohistochemistry & Ancillary Tests
- Melan-A/MART-1, SOX10, S100 — highlight melanocytes / map pagetoid spread
- HMB-45 — gradient with maturation in many naevi; diffuse deep labelling concerning in context
- Ki-67 — proliferation hotspots (interpret with care)
- PRAME — often diffuse in melanoma and limited in many naevi; ancillary only, with documented pitfalls and non-melanocytic positivity risks in broader practice[9][10][11]
Molecular tests (FISH, SNP array, NGS panels) are for selected ambiguous cases in specialist centres — they do not replace complete excision of concerning lesions.[7][3]
MPATH-Dx: Standardising the Grey Zone
The Melanocytic Pathology Assessment Tool and Hierarchy for Diagnosis (MPATH-Dx) maps diverse free-text diagnoses into classes linked to suggested management intensity, improving communication between pathologists and clinicians.[4][5] Version revisions refine class definitions for real-world reporting consistency.[4][5]
Teaching map (conceptual — follow institutional implementation): [1]
| Class concept | Examples | Typical action theme |
|---|---|---|
| Benign | Common naevus | Observation / no further Rx |
| Low-risk atypical | Mild dysplasia | Often observe if clear margins |
| Higher-risk atypical | Severe dysplasia, AST | Re-excise; specialist input |
| Melanoma in situ | MIS / LM | Complete excision with MIS margins |
| Invasive melanoma | pT1–T4 | WLE ± SLNB pathway |
Management Algorithm (Pathology-Linked)
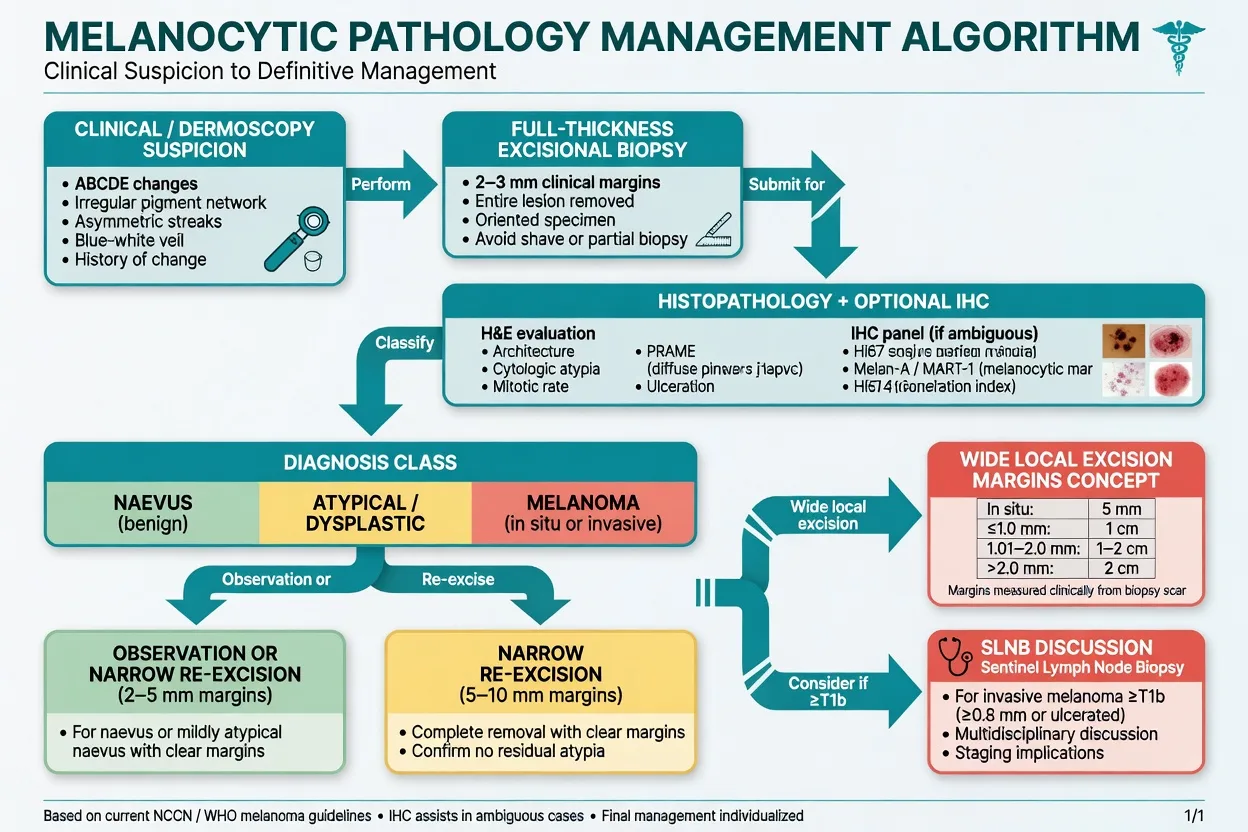
Practical sequence
- Suspect — ABCDE + dermoscopy; photograph; full skin and nodal exam.
- Biopsy correctly — full-thickness excision preferred when melanoma is in the differential.
- Report completely — Breslow, ulceration, margins, subtype for melanoma; clear atypia grade for naevi.
- Ancillary tests — IHC/PRAME/molecular only if they change management class.
- Act on class — observation vs re-excision vs WLE; discuss SLNB from ≥T1b context per staging leaf.
- Second opinion — adult Spitzoid, ambiguous severe atypia, or high-stakes sites before radical surgery.
- Surveillance — residual scar checks; educate on new/changing lesions.
Special Populations
- Children: Spitz-rich differential; avoid overcalling melanoma; still fully excise atypical Spitz tumours when advised.[7]
- Skin of colour / acral sites: sample full thickness; do not dismiss amelanotic or hyperkeratotic acral lesions.[3]
- Pregnancy: biopsy timing is clinical; histologic criteria are not relaxed.
- Immunosuppression: melanoma biology may be aggressive — first-pass histology must still be adequate for staging.[3]
Pitfalls That Change Outcome
- Superficial shave of obvious melanoma → wrong Breslow.[2]
- Accepting “compound naevus” on a transected base when clinically irregular.
- Treating PRAME as standalone melanoma proof.[11]
- Ignoring special-site norms → overdiagnosis of acral naevi as MIS.
- No clinical history on the request → wrong threshold for atypia.
- Skipping expert review for Spitz melanoma candidates.[8]
Regional & Systems Notes
AJCC 8th pathology elements are the global language for trials and boards.[1][2] MPATH-Dx offers a US-origin framework increasingly discussed for standardising ambiguous reports.[4][5] Resource-limited settings: prioritise complete excision biopsy, measured Breslow, ulceration, and margin status even when PRAME/FISH are unavailable.
Exam Pearls
NAEVUS-MEL
NAEVUSMEL
Full thickness when melanoma possible
Symmetry, borders, maturation
Breslow + ulceration + margins
Site, age, dermoscopy photos
Action-oriented language
Higher concern; complete excision
PRAME helps, does not rule alone
Ambiguous high-stakes cases
Invasive melanoma staging leaf
- Maturation deep = friend; deep mitoses + sheets = foe.[2][12]
- MPATH-Dx reduces chaotic synonyms into management classes.[4][5]
- PRAME diffuse → supports melanoma in context; negative does not exclude it.[9][10]
- Link next steps to the skin-cancer-staging algorithm once invasive melanoma is confirmed.[1][3]
References
- [1]Gershenwald JE, Scolyer RA. Melanoma Staging: American Joint Committee on Cancer (AJCC) 8th Edition and Beyond Ann Surg Oncol, 2018.PMID 29850954
- [2]Scolyer RA, Rawson RV, Gershenwald JE, et al. Melanoma pathology reporting and staging Mod Pathol, 2020.PMID 31758078
- [3]Tasdogan A, Sullivan RJ, Katalinic A, et al. Cutaneous melanoma Nat Rev Dis Primers, 2025.PMID 40180935
- [4]Barnhill RL, Elder DE, Piepkorn MW, et al. Revision of the Melanocytic Pathology Assessment Tool and Hierarchy for Diagnosis Classification Schema for Melanocytic Lesions: A Consensus Statement JAMA Netw Open, 2023.PMID 36630138
- [5]Barnhill RL, Piepkorn MW, Duncan LM, et al. MPATH-Dx version 2.0 schema for melanocytic lesions: A robust tool for standardized diagnostic reporting Clin Dermatol, 2025.PMID 39260462
- [6]Drozdowski R, Spaccarelli N, Peters MS, et al. Dysplastic nevus part I: Historical perspective, classification, and epidemiology J Am Acad Dermatol, 2023.PMID 36038073
- [7]Yeh I, Busam KJ. Spitz melanocytic tumours - a review Histopathology, 2022.PMID 34958498
- [8]LeBoit PE. Spitz melanoma Clin Dermatol, 2025.PMID 39265841
- [9]Lezcano C, Jungbluth AA, Nehal KS, et al. PRAME Expression in Melanocytic Tumors Am J Surg Pathol, 2018.PMID 30045064
- [10]Lezcano C, Jungbluth AA, Busam KJ. PRAME Immunohistochemistry as an Ancillary Test for the Assessment of Melanocytic Lesions Surg Pathol Clin, 2021.PMID 34023098
- [11]Lezcano C, Jungbluth AA, Busam KJ. Immunohistochemistry for PRAME in Dermatopathology Am J Dermatopathol, 2023.PMID 37856737
- [12]Ritter A, Tronnier M, Vaske B, et al. Reevaluation of established and new criteria in differential diagnosis of Spitz nevus and melanoma Arch Dermatol Res, 2018.PMID 29417221