Dermatology · Medicine
Mohs micrographic surgery
Also known as Mohs micrographic surgery (MMS) · Mohs surgery · Mohs micrographically controlled surgery · CCPDMA (complete circumferential peripheral and deep margin assessment)
Mohs micrographic surgery (MMS) is the microscopically controlled, tissue-sparing surgical excision of skin cancer in which the operating surgeon examines 100% of the surgical margin on horizontal (en face) frozen sections and re-excises only the tumour-positive areas until the entire margin is clear. It is the gold-standard treatment for non-melanoma skin cancer (NMSC) at high-risk sites. Cure rates are the highest of any skin-cancer treatment: 98 to 99% for primary basal cell carcinoma (BCC), 94 to 96% for recurrent BCC, and 96 to 97% for primary cutaneous squamous cell carcinoma (SCC). Indications cluster around the H-zone of the face, recurrent tumours, aggressive histological subtypes, poorly defined clinical margins, immunosuppression, and infiltrative tumours such as dermatofibrosarcoma protuberans (DFSP). The defining advantage over standard wide local excision is that bread-loaf vertical sectioning samples under 1% of the margin, whereas Mohs samples 100% in a single day, with the surgeon acting as their own pathologist.
On this page & tools
Your progress
Saved locally on this device.
Exam tags
Red flags
Overview & Definition
Mohs micrographic surgery is best understood as a single-day surgical method that fuses complete histological margin control with maximal tissue conservation. The operating dermatological surgeon removes the clinically apparent tumour with a narrow rim of surrounding skin, then systematically maps, colour-codes, freezes, sections, stains, and reads the entire peripheral and deep margin under the microscope while the patient waits. Wherever tumour touches the edge, the surgeon returns to that precise location, removes another thin layer, and repeats the cycle until every margin is histologically clear — and only then reconstructs the defect.[1][3]
The name is precise and matters at viva. Micrographic refers to the detailed map (the Greek graphos, drawn) that links every piece of removed tissue back to its anatomical origin on the patient. Microscopically controlled means the resection is governed by what is seen under the microscope, not by a predetermined distance of normal skin. An older, equivalent and increasingly used term is CCPDMA — complete circumferential peripheral and deep margin assessment — which emphasises that the entire true margin, not a sampling of it, is examined.[1]
Historical Development
The technique is the work of Frederic E. Mohs, a general surgeon at the University of Wisconsin, who developed it in the 1930s as a research tool to study cancer in rats. His original chemosurgery technique applied 20% zinc chloride paste in situ to fix (kill and harden) the tissue in the living patient; the fixed tissue was then excised the next day and sectioned horizontally. The zinc chloride provided both chemical fixation and a degree of tissue anaesthesia, and crucially allowed the fixed specimen to be sectioned en face so that the entire margin could be inspected.[3]
The fixed-tissue method was reliable but painful, slow (each layer took a day), and produced a stiff eschar that delayed healing. In 1953, while operating on the eyelid (where zinc chloride was too destructive), Mohs began excising fresh, unfenestrated tissue and processing it with frozen sections — the fresh-tissue technique. It proved superior, and over the next two decades fresh tissue replaced chemosurgery for nearly all sites. In the 1970s, Tromovitch and Stegman popularised the fresh-tissue technique and proposed the modern name Mohs (micrographic) surgery to honour the inventor while distinguishing it from the obsolete fixed-tissue method.[3]
Evolution of Mohs surgery
Frederic Mohs at the University of Wisconsin develops zinc chloride in-situ fixation to study rat cancers; the fixed tissue can be sectioned horizontally for complete margin review.[3]
Mohs reports chemosurgical treatment of human skin cancer, with complete margin control.
Working on periocular tumours where zinc chloride is too destructive, Mohs excises fresh unfixed tissue and uses frozen sections — the technique used today.
Mohs founds the college to train surgeons; it later becomes the American College of Mohs Surgery (ACMS).
Tromovitch and Stegman popularise the fresh-tissue method and propose the modern name, distancing it from zinc chloride chemosurgery.[3]
The ACMS fellowship (1 to 2 years) formalises training; the technique becomes the US standard for facial NMSC and spreads to Europe, Australasia and Asia.
Epidemiology & the Patient at Risk
Mohs exists because of the tumours it treats, and the tumour it treats most is basal cell carcinoma, the commonest cancer in humans. BCC accounts for roughly 70 to 80% of all non-melanoma skin cancer, with cutaneous SCC making up most of the remainder. The lifetime risk of developing a BCC is highest in fair-skinned (Fitzpatrick I to II) populations with chronic ultraviolet exposure, and is steepest in Australasia, where roughly one in two people will develop an NMSC by age 70.[1][4]
The Mohs indications map directly onto the epidemiology of high-risk NMSC. The factors that make a tumour biologically dangerous are the same factors that make standard excision unreliable, and they cluster in recognisable patient phenotypes:[1]
UV and phenotype
- **Cumulative and intermittent UV exposure** — outdoor workers, military, golfers, sunburn history
- **Fair skin, red/blonde hair, blue eyes, freckling** (Fitzpatrick I to II)
- **Older age** — decades of latency between UV damage and tumour emergence
Immunity
- **Solid-organ transplant recipients** — 65-fold or higher increase in SCC risk; tumours more aggressive, more multiple, higher metastasis
- **Chronic haematological disease and CLL** (on or off treatment) — SCC outnumbers BCC and behaves aggressively
- **HIV** with low CD4 counts; **iatrogenic immunosuppression** (azathioprine, cyclosporin, TNF inhibitors)
Genetic syndromes
- **Gorlin (basal cell naevus) syndrome** — PTCH1 mutation, hundreds of BCCs; Mohs for facial lesions (radiotherapy is contraindicated)
- **Xeroderma pigmentosum** — defective nucleotide excision repair, early and multiple skin cancers
- **Albinism** — cumulative UV damage on unprotected skin
Prior treatment and field change
- **Prior skin cancer** (BCC or SCC) — field cancerisation predicts new and recurrent tumours
- **Previously irradiated** skin — tissue compromised, recurrence high after standard excision
- **Chronic scars and sinuses** (osteomyelitis, burn scars) — Marjolin ulcer pattern, SCC in chronic wound
For these patients, Mohs is not an occasional referral but the default surgical pathway for any new facial NMSC, because the alternative — standard excision with its under 1% margin sampling — fails precisely where these patients need it most: on a face where subclinical extension is invisible and where each recurrence removes more of an already scarce cosmetic subunit.[1][4]
Principle: Why Mohs Works
The central principle is complete circumferential and deep margin assessment. Two technical choices make this possible, and both are examinable.[3]
First, the specimen is processed horizontally (en face). After the saucerised disc of tissue is removed, its outer rim is flattened down onto the cryostat chuck so that a single microtome cut samples the entire peripheral edge and the deep dermal/subcutaneous margin in one plane. Every cell at the true margin is therefore represented on the slide.[1][3]
Second, the surgeon who operated reads their own slides. Mohs surgeons are trained as both surgeon and dermatopathologist. The surgeon knows exactly where each piece of tissue came from (because they drew the colour-coded map), so when tumour is found at the edge they can return to that exact clock-position on the patient and remove only the additional involved tissue. This closed-loop feedback between resection and histology is what makes the technique both curative and tissue-sparing.[3]
Mohs vs standard excision at a glance
By contrast, standard wide local excision fixes the specimen in formalin and cuts it into a series of vertical cross-sections ("bread-loaves"). Only the cut face of each slice is examined — a tiny fraction (under 1%) of the entire margin. Tumour extending in the unsampled gaps between slices is invisible, so a "clear" report from standard pathology does not actually prove the margin is clear; it proves the sampled slices are clear. This is the single most important concept to articulate at viva: standard excision offers high sensitivity for bulk disease but low sensitivity for subclinical skip extension, which is exactly what aggressive facial tumours exhibit.[1][3]
The reason this matters is subclinical extension — tumour that extends microscopically beyond what the eye can see. The magnitude is subtype-dependent and is itself examinable: a nodular BCC on the trunk is cleared by a 4 mm clinical margin in over 95% of cases, whereas a morpheaform or infiltrative BCC has subclinical extension of more than 1 cm in roughly one-third of cases, and of more than 2 cm in a smaller but clinically important minority. On the face this is compounded by embryonic fusion planes (the so-called H-zone, where ectoderm fused in utero), along which BCC preferentially tracks — the same planes that make recurrence after standard excision highest on the nose, perinasal, periauricular and perioral skin. SCC behaves similarly once it becomes poorly differentiated or gains perineural invasion, following named nerves (the infraorbital, mental, facial and trigeminal branches) for many centimetres beyond the visible tumour.[4] Standard excision, by sampling only the cut face of each bread-loaf slab, is structurally blind to this extension; Mohs, by reading the entire true margin, makes it visible and resectable layer by layer.
Clinical Assessment & Pre-operative Workup
Because Mohs is planned around the biology of the tumour and the anatomy it occupies, the pre-operative assessment determines both whether Mohs is appropriate and how the defect will be reconstructed. A focused assessment has four layers: confirm the histology, define the clinical and subclinical extent, map the danger anatomy, and plan the repair.[1][3]
Histological confirmation. A pre-operative biopsy is mandatory — usually a shave (for nodular BCC) or a punch (for sclerosing, recurrent, or deeply infiltrative lesions) — read by a dermatopathologist. The biopsy establishes the diagnosis, the histological subtype (which dictates subclinical extension risk: morpheaform/infiltrative greater than micronodular greater than nodular greater than superficial), the grade (well versus poorly differentiated SCC), and the presence of perineural or lymphovascular invasion, any of which can upgrade a "low-risk" lesion into a Mohs indication. A biopsy that shows only superficial BCC may still mandate Mohs if the clinical appearance suggests deeper disease.[4]
Defining clinical and subclinical extent. Dermoscopy and, increasingly, reflectance confocal microscopy and optical coherence tomography help delineate the true border of poorly defined or pigmented tumours. The lesion and a margin are marked under good lighting with the patient seated upright (so gravitational distortion of facial subunits is accounted for). Photographs are taken at rest and with animation, both to document the lesion and to plan reconstruction that preserves facial movement.[2]
Mapping the danger anatomy. Before any cut, the surgeon marks the relevant facial nerve danger zones (the temporal branch crossing a line from 0.5 cm below the tragus to 1.5 cm above the lateral brow; the marginal mandibular branch along the jawline), identifies the free margins of the eyelids, lips and nasal ala where contraction causes ectropion/eclabium/alar notching, and notes any previous surgical scars or flaps that limit local tissue movement.[2]
[2]Investigations for the high-risk tumour. Routine blood tests are not required for Mohs. However, for clinically enlarged nodes (palpable cervical, parotid or axillary lymphadenopathy) on SCC, Merkel cell carcinoma or aggressive BCC, ultrasound or CT of the regional nodes is performed before surgery, and a sentinel node biopsy may be discussed for Merkel cell carcinoma within the multidisciplinary team. For large (over 2 cm), fixed, or deeply infiltrative tumours, or when perineural invasion is reported on biopsy, MRI (for skull-base, cavernous sinus, or large-nerve involvement) or CT (for bone invasion of the maxilla or mandible) guides whether Mohs alone is sufficient or whether additional parotidectomy, neck dissection, or adjuvant radiotherapy will be needed. These imaging decisions are made by the skin cancer multidisciplinary team, not unilaterally by the Mohs surgeon.[7]
Consent. The patient is counselled that the procedure takes several hours in total (mostly waiting between stages), that a same-day reconstruction may use a flap or graft, that a small proportion of cases (under 5%) need a second day, and that bleeding, infection, nerve injury and recurrence are the recognised risks. Expectation-setting on the cosmetic result — including that the scar matures over 12 to 18 months — is part of consent, not an afterthought.[2]
Technique: The Mohs Procedure Step by Step
Mohs is performed as an outpatient, single-day procedure under local anaesthesia (typically 1% lidocaine with adrenaline, maximum 7 mg/kg; plain lidocaine near end-appendages). The stages below are iterative — a "layer" or "stage" is one complete excise-map-freeze-read cycle.[3]
One Mohs stage
Mark, debulk, anaesthetise
Outline the clinical tumour with a surgical pen; curette away friable tumour to better define true border; infiltrate local anaesthetic in a ring around the lesion.
Excise the saucerised layer
Remove the tumour with a 1 to 3 mm rim of normal skin at a 45 degree bevel, leaving a saucer-shaped disc whose deep surface is bevelled outward — this bevel lets the specimen flatten on the cryostat.
Map and colour-code
Cut reference notches at known clock positions; paint specimen edges with coloured dyes (blue, red, green, black). Draw an anatomical map recording which dye is at which edge.
Orient and freeze
Place the disc deep-side up (en face) on the cryostat; invert and freeze so the peripheral and deep margins lie in one horizontal plane; cut 5 to 7 micrometre sections.
Stain and read
Stain with H and E or toluidine blue; the Mohs surgeon reads the slides (15 to 30 min) and marks any tumour on the map.
Re-excise positive areas only
If tumour touches the margin, use the map to return to that exact clock position on the patient and remove a further thin layer — never the whole wound again.
Repeat until clear
Re-map, re-freeze, re-read each new layer until every margin is negative (most tumours clear in 1 to 3 stages).
Reconstruct same day
Once clear, repair the defect (primary closure, flap, graft, or second intention) — the surgeon knows the exact size and that margins are negative before closing.
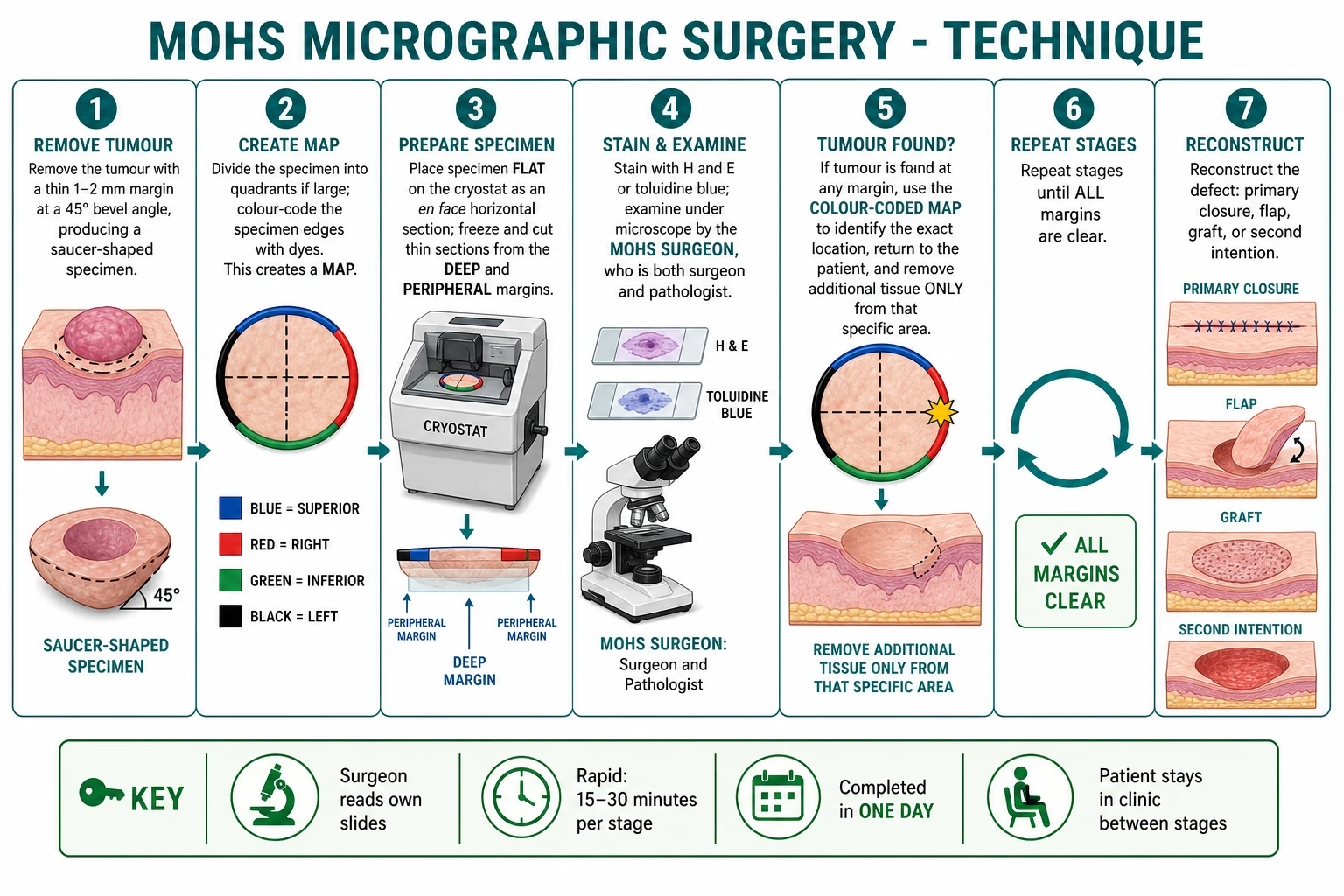
Three technical points deserve emphasis. The bevel (45 degrees) and the saucerised deep surface are not cosmetic — they are what allow the specimen to be inverted and flattened so that the peripheral edge and the deep margin come to lie in the same horizontal sectioning plane; without the bevel, the rim would buckle and the margin could not be read as a single continuous line. The reference notches (small cuts at known clock positions) and dye colour-coding are the geometric link between the slide and the patient: a red-dye tumour at the 3 o'clock position on the map sends the surgeon back to the 3 o'clock position on the wound. Reading speed (15 to 30 minutes per stage, versus days for permanent paraffin) is what makes same-day completion possible.[3]
A common viva trap: Mohs frozen sections are not the same as the generic "frozen section" used intra-operatively by general or ENT surgeons. A generic frozen section is a single representative vertical cut sent to a separate pathologist, sampling only a fraction of the margin; Mohs sections are horizontal en face preparations of the entire true margin, read by the operating surgeon using a mapped specimen. The distinction between "complete circumferential margin assessment" (Mohs) and "representative margin sampling" (frozen section) is exactly what examiners probe.[3]
Indications
The Appropriate Use Criteria for Mohs, developed jointly by the American Academy of Dermatology, the American College of Mohs Surgery and related societies, and reflected in international guidelines, sort indications into absolute (first-line), relative, and not indicated.[1][3]
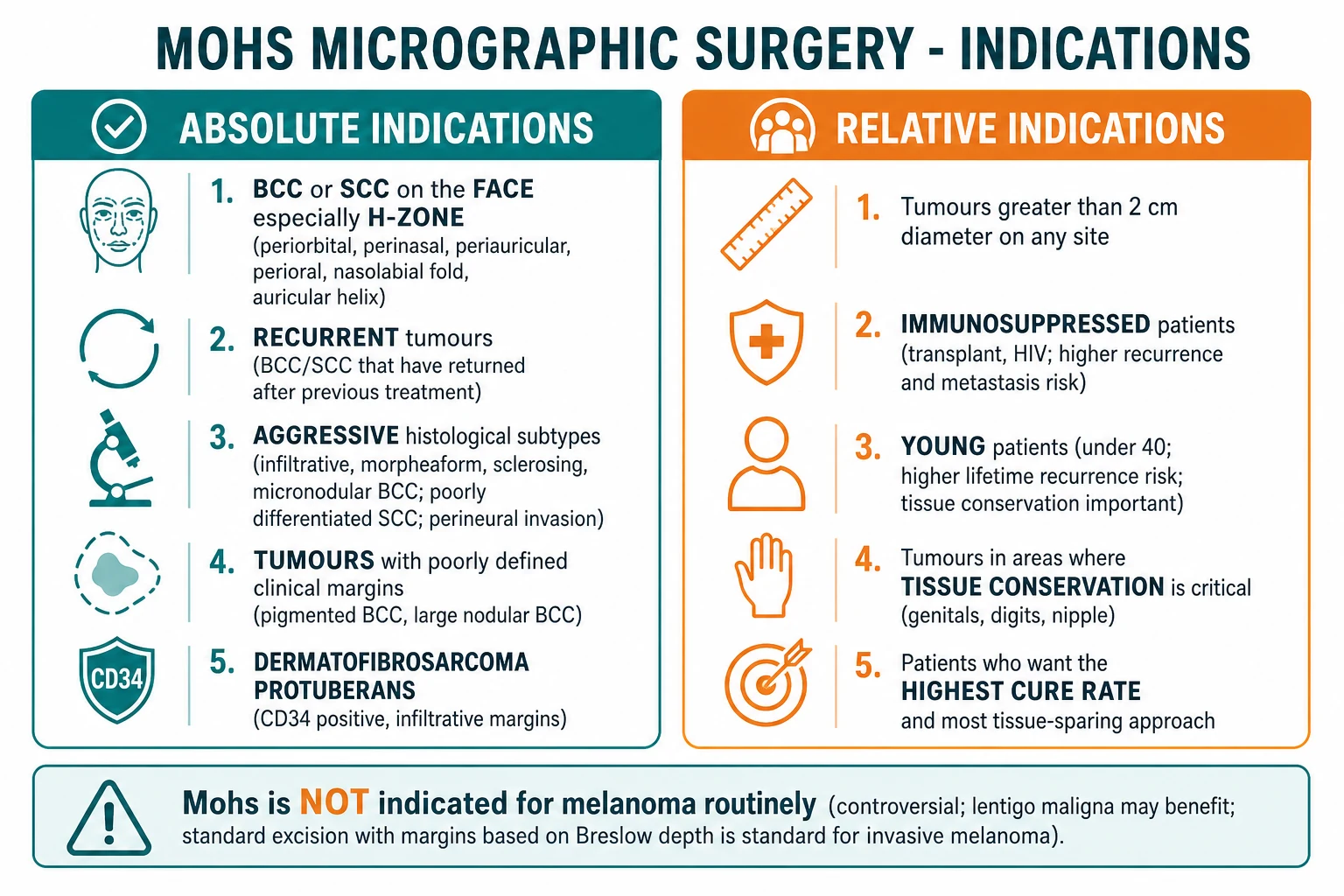
Absolute indications (Mohs first-line)
Anatomical site
- BCC or SCC in the **H-zone of the face**: periorbital, perinasal, periauricular, perioral, nasal ala and tip, nasolabial fold, auricular helix/concha
- Tumours of the **genitalia, perianal skin, hands/feet, nail units, and digits** — tissue conservation is critical and margins unreliable
- Sites with **high recurrence** after standard excision: nasolabial fold, perinasal, periauricular, scalp
Tumour behaviour
- **Recurrent** BCC/SCC (recurrence after any prior treatment — surgery, RT, topical)
- **Aggressive histological subtypes**: infiltrative, morpheaform/sclerosing, and micronodular BCC; poorly differentiated SCC; **perineural invasion**
- **Poorly defined clinical margins** — pigmented, large nodular, or fibrosing tumours where the eye cannot see the true border
Specific tumours
- **Dermatofibrosarcoma protuberans (DFSP)** — infiltrative honeycomb margins; Mohs gives the lowest local recurrence of any treatment
- **Atypical fibroxanthoma (AFX)** and malignant fibrous histiocytoma
- **Merkel cell carcinoma** where available, for local control
- **Extramammary Paget disease**, **leiomyosarcoma** of skin, **microcystic adnexal carcinoma**
Patient factors
- **Immunosuppressed** patients (solid-organ transplant, chronic haematological disease, HIV) — higher recurrence and metastasis, mandate Mohs for any NMSC
- **Previously irradiated** field — tissue compromised, recurrence high
- **Positive margins** on a recent standard excision — Mohs to map residual disease
Relative indications
Relative indications are those in which Mohs is preferred but standard excision with adequate margins is acceptable if Mohs is unavailable:[1]
- Tumours over 2 cm in diameter on any site.
- Young patients (under 40) — high lifetime recurrence risk and greatest cosmetic benefit from tissue conservation.
- Tumours where maximum tissue conservation is desired (cosmetic units, large trunk lesions, the elderly with comorbidity).
- Any BCC/SCC in a patient who has already had multiple skin cancers.[1]
Not routinely indicated
Mohs is over-treatment and not indicated for:[3]
- Low-risk BCC/SCC on the trunk or extremities — well-defined, under 2 cm, nodular or superficial histology. Standard excision with 4 mm margin (BCC) or 4 to 6 mm margin (SCC) gives equivalent cure at lower cost.
- Invasive melanoma — standard excision with margins dictated by Breslow thickness (1 cm for in situ/under 1 mm, 1 to 2 cm for 1.01 to 2 mm, 2 cm for over 2 mm) remains the standard. Mohs for invasive melanoma is controversial because frozen-section diagnosis of melanoma is difficult, and melanoma in transit/satellite disease is not a margin problem.
- The exception is lentigo maligna (melanoma in situ on chronically sun-damaged skin), where subclinical extension is notorious and standard margins (5 mm) are frequently inadequate; Mohs (often with MART-1 immunostaining) or modified slow-Mohs with paraffin sections is increasingly used.[8]
US (AAD/ACMS Appropriate Use Criteria): Mohs is the default for facial NMSC and is well reimbursed; the majority of US facial BCC/SCC are treated by Mohs. UK (BAD/NHS): Mohs is commissioned through regional skin cancer specialist centres (the British Society for Dermatological Surgery maintains a register of units); access is more limited than the US, reserved for high-risk facial/recurrent/DFSP tumours. Australia (ACD): Mohs availability is expanding rapidly given the world's highest NMSC incidence; funded through a mix of Medicare and private practice. India/global: Mohs is concentrated in a few academic centres; cost and access limit routine use, but DFSP and facial tumours are increasingly referred.
Specific Tumours Where Mohs Is First-Line
BCC and SCC dominate Mohs practice by volume, but several rarer tumours are first-line Mohs indications in their own right, either because their subclinical extension defeats standard margins or because tissue conservation on the face is at a premium. Each warrants a one-paragraph defence at viva.[6]
Dermatofibrosarcoma protuberans (DFSP) is the paradigm. This low-grade dermal sarcoma infiltrates subcutaneous fat in a honeycomb/lace pattern of slender CD34-positive spindle cells that extend far beyond the visible plaque. Standard wide local excision with 2 to 3 cm margins still leaves local recurrence rates historically of 20 to 50%, because the residual tentacles are missed. Mohs (often slow-Mohs with permanent paraffin sections and CD34 immunostain) reduces local recurrence to under 2 to 5% while sparing normal tissue — the modern standard of care for DFSP at any site where it is available.[6]
Atypical fibroxanthoma (AFX) and its deeper variant pleomorphic dermal sarcoma occur on the sun-damaged head and neck of the elderly. AFX is locally aggressive but rarely metastasises; Mohs offers complete margin control and high cure. The deeper pleomorphic variant behaves more like a sarcoma and is managed jointly with the MDT, sometimes with adjuvant radiotherapy.[6]
Merkel cell carcinoma is a neuroendocrine skin cancer with a propensity for lymphatic spread and recurrence, so Mohs alone addresses only the primary site; sentinel lymph node biopsy, imaging, and consideration of adjuvant radiotherapy are decided by the multidisciplinary team. Slow-Mohs or modified Mohs with CK20 immunostaining helps confirm margin clearance of the subtle dermal infiltrate.[7]
Extramammary Paget disease (vulval, scrotal, perianal) has multifocal, skip-lesion epidermal spread that clinical margins cannot capture. Slow-Mohs with cytokeratin-7 immunostaining maps the true extent and dramatically lowers the recurrence rate compared with wide excision.[6]
Microcystic adnexal carcinoma (sclerosing sweat duct carcinoma) infiltrates deeply along nerves and into muscle with perineural invasion, so standard excision is frequently margin-positive; Mohs is the surgical treatment of choice.[6]
Lentigo maligna (melanoma in situ on chronically sun-damaged skin) is the one melanocytic tumour for which Mohs is increasingly accepted. Subclinical extension is notorious — 5 mm margins clear only roughly 60 to 70% — so Mohs with MART-1 (Melan-A) immunostaining or slow-Mohs with paraffin sections is used to achieve histological clearance while sparing normal facial skin, with reported recurrence under 2%.[8]
SCC in situ (Bowen disease) on the face or digit, and verrucous carcinoma, are relative indications: Mohs is chosen when standard excision would sacrifice a critical structure (eyelid margin, nail unit, digit tip) or when the lesion is large and poorly defined.[6]
For invasive melanoma, as noted below, standard excision with Breslow-based margins remains the rule; Mohs is the exception, reserved for the in-situ lentigo maligna pattern.[3]
Variants of Mohs
Two processing variants exist, and the distinction is frequently tested.[6]
| Feature | Standard Mohs (frozen) | Modified / slow Mohs (paraffin) |
|---|---|---|
| Section type | Frozen (cryostat) horizontal en face | Permanent paraffin horizontal en face |
| Turnaround | 15 to 30 min per stage | 24 hours per stage |
| Sessions | Single day | Multiple days; defect dressed between stages |
| Best for | BCC, SCC, AFX, routine NMSC | DFSP, Merkel cell, lentigo maligna, extramammary Paget, melanoma in situ |
| Why | Fast, adequate for most tumours | Superior morphology + immuno (MART-1, CD34) for subtle tumours where frozen sections miss single cells |
| Example immunostain | Toluidine blue / H and E | MART-1 for lentigo maligna; CD34 for DFSP; CK20 for Merkel |
Slow Mohs (modified Mohs with permanent sections) is preferred for tumours in which a single malignant cell at the margin matters and frozen-section morphology is unreliable — DFSP (CD34-positive slender cells infiltrating fat), lentigo maligna (atypical melanocytes along the basal layer, easily missed on H and E frozen), Merkel cell carcinoma, and extramammary Paget disease.[6][8] The trade-off is that reconstruction is deferred for 24 to 48 hours while the defect is dressed.
A related variant is the square procedure (Mohs with peripheral in-continuity margin), used for lentigo maligna, in which a peripheral rim of skin is removed and processed as a continuous strip to examine the entire perimeter in one block.[8]
Outcomes
Mohs delivers the highest published cure rates of any skin-cancer treatment, a fact that should be reproduced verbatim.[1][3]
Cure rates after Mohs micrographic surgery
For comparison, standard excision achieves roughly 90 to 95% cure for primary BCC and 80 to 85% for recurrent BCC — the gap is widest precisely where Mohs is indicated (face, recurrent, aggressive).[4] Cosmetic outcomes are excellent because Mohs is tissue-sparing (only tumour-positive tissue is removed) and reconstruction is performed by the same surgeon, on the same day, with exact knowledge of the defect dimensions.[2]
Mohs vs Standard Excision and Other Treatments
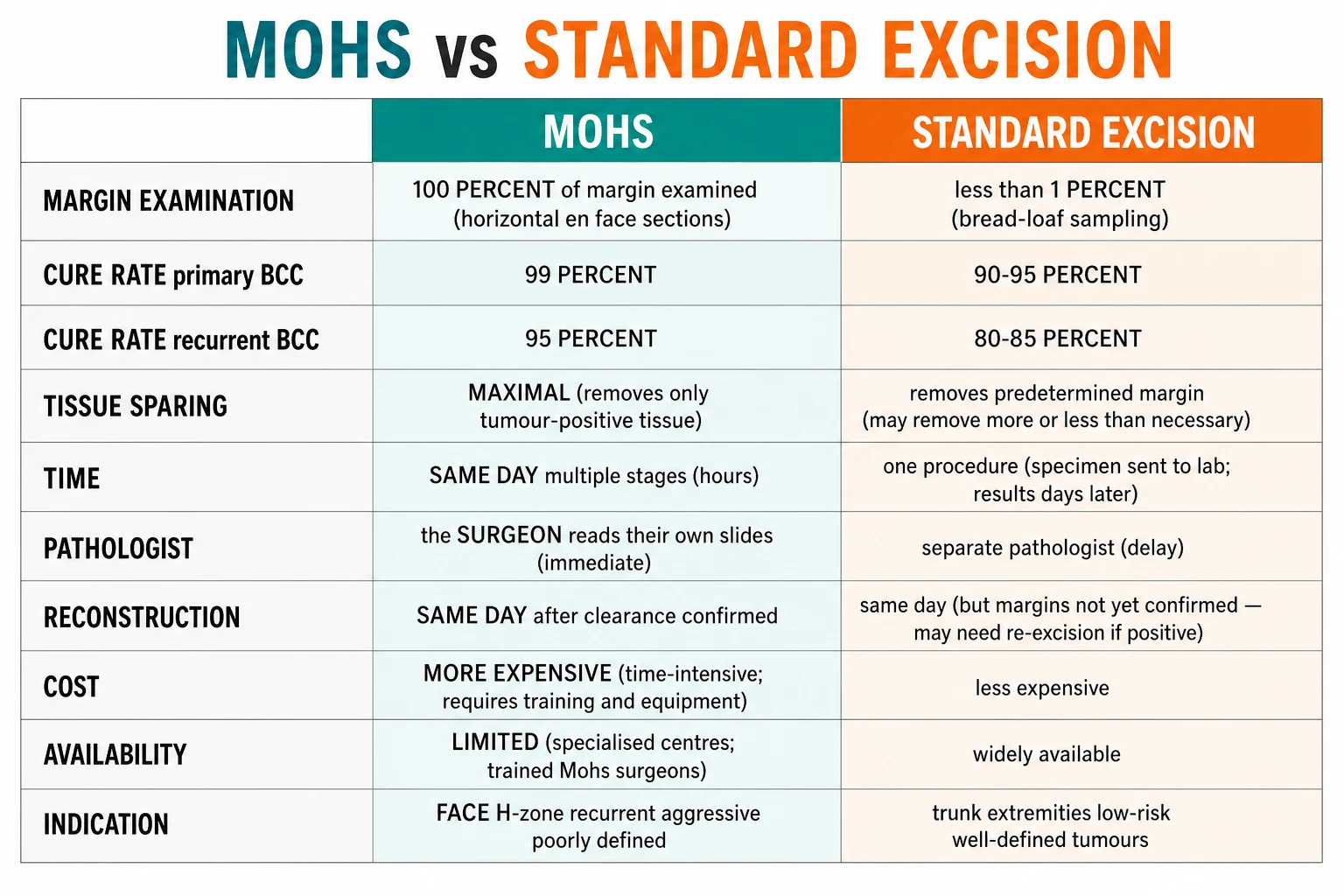
| Feature | Mohs micrographic surgery | Standard wide local excision |
|---|---|---|
| Margin examined | 100% (entire true margin, horizontal en face) | under 1% (vertical bread-loaf sampling) |
| Typical margins | 1 to 3 mm rim, then map-guided re-excision | 4 mm for primary low-risk BCC; 4 to 6 mm for primary low-risk SCC |
| Cure, primary BCC | 98 to 99% | 90 to 95% |
| Cure, recurrent BCC | 94 to 96% | 80 to 85% |
| Tissue sparing | Maximal — only positive tissue re-excised | Predetermined; may remove excess normal skin |
| Pathology | Surgeon reads own slides, in-house | Separate pathologist, days later |
| Reconstruction | Same day, after clearance confirmed | Same day, margins not yet known |
| Cost | Higher per procedure | Lower per procedure |
| Availability | Specialised Mohs centres only | Widely available |
For low-risk trunk/extremity tumours, the other NMSC treatments also have a place and are compared against Mohs: curettage and electrodesiccation (high cure for small low-risk nodular BCC but no histological margin control and a white atrophic scar); cryotherapy (good for actinic keratoses and selected superficial BCC); radiotherapy (for patients unfit for surgery or where surgery would be mutilating; contraindicated in Gorlin syndrome and previously irradiated fields); topical 5-fluorouracil and imiquimod (superficial BCC, actinic keratoses, Bowen disease; no margin control). None examines the margin, so none can match Mohs for high-risk tumours.[4]
Reconstruction of the Mohs Defect
Once margins are clear, the surgeon repairs the defect using the reconstructive ladder, choosing the method that best restores form and function for that anatomical subunit.[2]
- Second-intention healing (allow granulation and contraction) — best for concave sites (concave temple, medial canthus, conchal bowl, postauricular sulcus), where contraction pulls the wound into a natural contour; convex sites heal with a depressed scar.
- Primary closure (side-to-side) — for small defects with lax surrounding skin; convert to an ellipse along resting skin tension lines, excise dog-ears.
- Local flaps (advancement, rotation, transposition such as rhomboid and bilobed) — for nasal, cheek, perioral and periauricular defects; redistribute adjacent tissue of matching colour and texture. Subunits (nasal tip, ala, helical rim) are reconstructed as units.
- Skin grafts (split- or full-thickness) — for large defects or those exposing cartilage/bone without a vascular bed for a flap; full-thickness for face (better colour match), split-thickness for large trunk/scalp; secured with a tie-over bolster.[6]
Because the surgeon knows the exact final defect size and that all margins are negative before closure, reconstruction after Mohs is more reliable than after standard excision, where a positive margin may necessitate re-operation through a newly closed wound.[2]
Complications & Pitfalls
Common surgical complications
- **Bleeding** — intra-operative and post-operative haematoma (lower than expected even on anticoagulants, but still the commonest issue)
- **Infection** — rare (under 2%); prophylactic antibiotics only for high-risk sites (nose, ear, contaminated wounds, prosthetic valves)
- **Dehiscence** of closure — from tension, premature activity, or infection
- **Flap/graft failure** — partial or total necrosis from poor vascularity, haematoma under the graft, or smoking
Site-specific nerve injury
- **Temporal branch of facial nerve** — forehead/temple (results in brow ptosis, inability to raise forehead)
- **Marginal mandibular branch** — jawline and chin (lower-lip weakness)
- **Infraorbital and supraorbital nerves** — periorbital and cheek (sensory loss)
- **Great auricular nerve** — postauricular and lateral neck (earlobe numbness)
- Knowledge of danger zones is mandatory; most deficits are neuropraxia and recover
Cosmetic and functional
- **Ectropion or eclabium** from contraction near eyelids/lips — prevented by lid-tightening and proper flap design
- **Alar notching** from primary closure under tension at the nasal rim
- **Hypertrophic scar / keloid** — risk in patients with prior keloids, chest/shoulder sites
Recurrence (Mohs failure)
- True recurrence after Mohs is under 2% for primary BCC — when it occurs it reflects aggressive biology, skip areas, or perineural spread
- Re-excision or radiotherapy for recurrence
- Positive final margin (tumour tracking beyond reach) — rare; managed by re-Mohs, RT, or paraffin permanent sections
A pitfall specific to the technique: frozen-section artefact can obscure single atypical cells, which is why slow-Mohs with permanent paraffin and immunostains is preferred for DFSP, lentigo maligna and Merkel cell carcinoma. A second pitfall is inadequate mapping — if the colour-code/notation is wrong, the surgeon returns to the wrong site, and the tumour is missed. This is why Mohs is performed only by formally trained, fellowship-educated surgeons.[3]
Special Populations
- Immunosuppressed patients (solid-organ transplant recipients, chronic lymphocytic leukaemia, HIV with low CD4) develop more aggressive, more recurrent and more metastatic NMSC. Mohs is indicated for essentially all NMSC in this group, with lifelong surveillance because new and recurrent tumours are common.[1]
- Anticoagulated patients (warfarin, DOACs, aspirin, clopidogrel): contemporary practice is to continue anticoagulation for Mohs because the risk of a thromboembolic event on interruption exceeds the bleeding risk from a superficial skin procedure under careful local haemostasis. Bridging is rarely required; the decision is individualised. Surgeons must have electrocoagulation and absorbable haemostatic agents available.
- Pacemakers and implantable defibrillators: bipolar electrosurgery (or battery-operated heat cautery) is used instead of monopolar to avoid current passing through the device. Grounding plates are avoided.
- Paediatric patients: Mohs is occasionally used for congenital or paediatric skin tumours (DFSP, giant congenital melanocytic naevus with atypia, basal cell naevus syndrome); the technique is identical but sedation and cooperation must be managed, and second-intention healing is favoured where possible.
- Pregnancy: Mohs can be performed safely in any trimester with local anaesthesia; large reconstruction may be deferred post-partum. Lidocaine with adrenaline is safe; avoid NSAIDs in the third trimester for post-operative analgesia.
Evidence, Guidelines & Controversies
The evidence base for Mohs rests on decades of large prospective cohort series (not randomised trials, which are ethically difficult when one arm forgoes margin control). The seminal long-term outcome data come from Mohs's own Wisconsin series and from the systematic reviews by Rowe and colleagues, repeatedly showing 5-year cure of 99% for primary BCC and 95% for recurrent BCC, against 90 to 95% and 80 to 85% respectively for standard excision. The Appropriate Use Criteria for Mohs Micrographic Surgery (2012, updated), jointly authored by the AAD, ACMS, ASDS and AAD, formalise the indications used worldwide.[1]
[1]Two genuine controversies remain. Mohs for invasive melanoma is not standard because (a) frozen-section diagnosis of melanoma is hard — cytology at the margin is unreliable and inflammation mimics tumour; (b) melanoma spreads lympho-haematogenously, so local margin is not the only determinant of outcome; and (c) Breslow-based excision margins are well-validated by randomised trials. The exception is lentigo maligna (in-situ melanoma on sun-damaged skin), where subclinical extension defeats standard 5 mm margins; here Mohs with MART-1 immunostaining or slow-Mohs achieves higher clearance and lower recurrence, and is increasingly accepted.[8] The cost-effectiveness debate (below) is the second: Mohs costs more per procedure but saves system cost for high-risk tumours.
Emerging adjuncts include 3D whole-specimen imaging and digital pathology to accelerate slide reading, artificial intelligence for margin interpretation, and 3D bioprinting for defect reconstruction — all still adjuncts to, not replacements for, the mapped en-face principle.[5]
Training & Credentialing
Mohs is performed only by physicians who have completed a dedicated Mohs micrographic surgery fellowship — most commonly the 1 to 2 year fellowship of the American College of Mohs Surgery (ACMS), undertaken after dermatology residency. The fellowship trains the surgeon across the three intersecting disciplines: dermatological surgery (excision and complex reconstruction), dermatopathology (reading one's own frozen sections), and clinic-based pathology laboratory management (running a cryostat and histology lab).[3]
Outside the US, the British Society for Dermatological Surgery (BSDS) and the Australasian College of Dermatologists (ACD) run Mohs training pathways within dermatology, and the European and Asian colleges are developing equivalents. The unifying principle is that the surgeon who reads the slides is the surgeon who operated; delegation of slide reading to a remote pathologist is not Mohs.[9]
Cost-Effectiveness
Mohs is more expensive per procedure than standard excision (extra surgeon, histotechnician, on-site laboratory and patient time), but cost-effective overall for high-risk tumours because it avoids the downstream costs of recurrence surveillance, re-operation, and management of advanced recurrent disease. Systematic reviews report that, for tumours meeting the Appropriate Use Criteria, Mohs is cost-neutral or cost-saving versus standard excision plus the cost of recurrence, and its cost per quality-adjusted life-year (QALY) is highly favourable.[9]
The economic logic is clearest at the two extremes: for a low-risk nodular BCC on the trunk, standard excision is cheaper and equivalent in cure; for a recurrent infiltrative BCC on the nose, Mohs is both more curative and, over a lifetime, less costly than serial re-excision. The AUC exist precisely to direct the technique to where its margin benefit is worth its price.[9]
Definition
Microscopically controlled, tissue-sparing excision of skin cancer with 100% margin examination on horizontal en face frozen sections read by the operating surgeon.
Mechanism
Saucerised layer excised with 45 degree bevelSpecimen mapped and colour-coded (dyes + reference notches)Frozen, sectioned horizontally (en face) — entire margin on one slideSurgeon reads own slides (15 to 30 min)Positive margin mapped back to exact site; only that area re-excisedRepeat until clear; reconstruct same day
Management
Local anaesthesia, outpatient, single day1 to 3 stages typicalReconstruction: second intention, primary closure, flap, or graft
Prognosis
Highest cure of any skin-cancer treatment; recurrence under 2% for primary BCC; excellent cosmesis due to tissue conservation and immediate, defect-matched repair.
Exam Pearls
MOHSWhy Mohs wins
Hook:Mapped + Own slides + Horizontal en face + Same day = the four features that make Mohs the gold standard.
Exam application bank (NEET-PG / INICET)
One-line answer
Mohs micrographic surgery (MMS) is the microscopically controlled, tissue-sparing surgical excision of skin cancer in which the operating surgeon examines 100% of the surgical margin on horizontal (en face) frozen sections and re-excises only the tumour-positive areas until the entire margin is clear. It is the gold-standard treatment for non-melanoma skin cancer (NMSC) at high-risk sites. Cure rates are the highest of any skin-cancer treatment: 98 to 99% for primary basal cell carcinoma (BCC), 94 to 96% for recurrent BCC, and 96 to 97% for primary cutaneous squamous cell carcinoma (SCC). Indications cluster around the H-zone of the face, recurrent tumours, aggressive histological subtypes, poorly defined clinical margins, immunosuppression, and infiltrative tumours such as dermatofibrosarcoma protuberans (DFSP). The defining advantage over standard wide local excision is that bread-loaf
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard.[9]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes.[1]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change.[6]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each.[6]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory.[6]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Mohs micrographic surgery.
Quick self-test: name the five absolute indications for Mohs
H-zone of the face; recurrent tumours; aggressive histological subtypes (infiltrative/morpheaform BCC, poorly differentiated SCC, perineural invasion); poorly defined clinical margins; and specific infiltrative tumours (DFSP, AFX, Merkel cell, extramammary Paget, microcystic adnexal carcinoma). Immunocompromised status and prior radiation make any of these more urgent.
Quick self-test: what cure rate would you quote for a recurrent BCC on the nose treated by Mohs?
94 to 96% five-year cure after Mohs, versus approximately 80 to 85% after standard excision — the gap is widest precisely for recurrent facial tumours, which is why the H-zone plus recurrence is the canonical indication.
References
- [1]Bittner GC, Cerci FB, Kubo EM, et al. Mohs micrographic surgery: a review of indications, technique, outcomes, and considerations. Anais Brasileiros de Dermatologia, 2021.PMID 33849752
- [2]Owens WR, Quirarte DM, Gillipelli SR, et al. Lip Reconstruction. Seminars in plastic surgery, 2024.PMID 39697401
- [3]Golda N, Hruza G. Mohs Micrographic Surgery. Dermatologic Clinics, 2023.PMID 36410982
- [4]Marzuka AG, Book SE. Basal cell carcinoma: pathogenesis, epidemiology, clinical features, diagnosis, histopathology, and management. The Yale journal of biology and medicine, 2015.PMID 26029015
- [5]Pulumati A, Algarin YA, Kim S, et al. 3D bioprinting: a review and potential applications for Mohs micrographic surgery. Archives of dermatological research, 2024.PMID 38698273
- [6]Mullen JT, Feng L, Xing Y, et al. Dermatofibrosarcoma Protuberans: Wide Local Excision Versus Mohs Micrographic Surgery. Surgical oncology clinics of North America, 2016.PMID 27591501
- [7]Lewis DJ, Sobanko JF, Etzkorn JR, et al. Merkel Cell Carcinoma. Dermatologic clinics, 2023.PMID 36410971
- [8]Cline E, Papac N, McBride J, Collins L. Oral Mucosal Lentigo Maligna Treated With Mohs Micrographic Surgery. Dermatologic surgery, 2023.PMID 36946694
- [9]Tierney EP, Hanke CW. Cost effectiveness of Mohs micrographic surgery: review of the literature. Journal of drugs in dermatology, 2009.PMID 19852120