Dermatology · Medicine
Nail disorders
Also known as Nail disorders · Onychodystrophy · Onychomycosis · Nail psoriasis · Nail lichen planus
Comprehensive nail disorders reference for MBBS/board exam: Onychomycosis (tinea unguium — confirm with KOH/PCR before oral antifungal; terbinafine 250 mg daily 6wk finger/12wk toe first-line; alternatives itraconazole pulse 200 mg BID 1-week-on/3-weeks-off ×3, fluconazole 150 mg weekly); Nail psoriasis (pitting, oil-drop, onycholysis with erythematous border); Nail lichen planus (dorsal pterygium is irreversible scarring — urgent corticosteroid); Beau's lines, Onycholysis, Koilonychia (iron deficiency), Melanonychia (single band + Hutchinson's sign → subungual melanoma biopsy). Special types: trachyonychia / twenty-nail dystrophy (rough nails ± alopecia areata; biotin 5-10 mg daily for brittle nails, biotin deficiency dose 5 mg), median nail dystrophy (central canaliform split), onychogryphosis (ram's horn toenail), onychauxis (thickened nail without deformity), parakeratosis pustulosa (children; thumb), pterygium inversum unguis (ventral pterygium; gel polish), onychoatrophy / anonychia (nail loss). Procedures: partial nail avulsion (ingrown toenail), chemical matrixectomy with phenol 88% (recurrence <5%), surgical matrixectomy, CO2 laser ablation. Systemic signs: clubbing (lung cancer/IBD), Lindsay/Terry/Mees/Muehrcke. Red flag: single band melanonychia + Hutchinson's sign in a Caucasian adult = subungual melanoma until proven otherwise.
On this page & tools
Your progress
Saved locally on this device.
Exam tags
Red flags
Common Nail Disorders
Onychomycosis (tinea unguium)
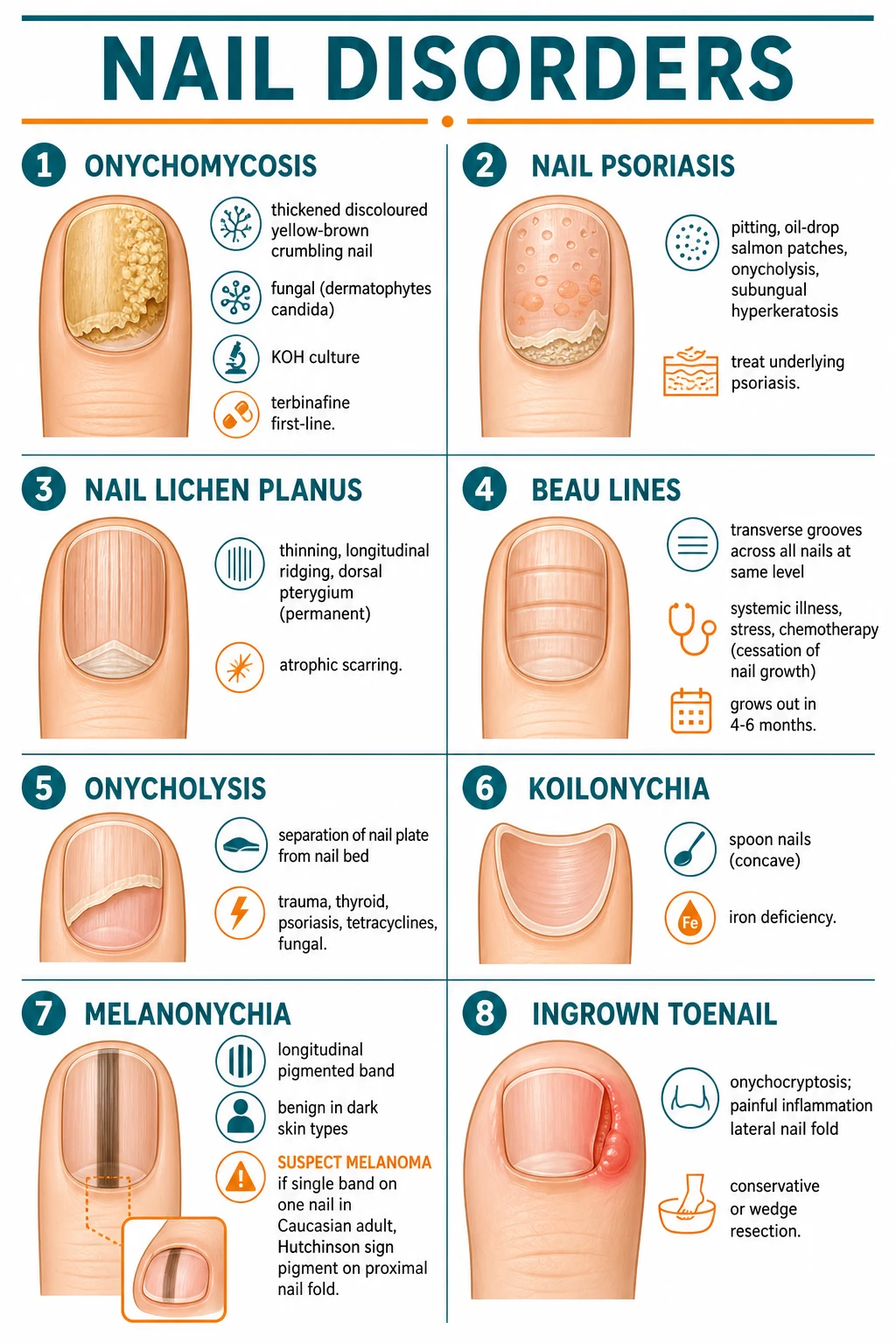
- Fungal infection of the nail plate and/or nail bed; commonest nail disorder.[2][4]
- Clinical: thickened, discoloured (yellow-brown-white), crumbling nail plate; subungual hyperkeratosis; onycholysis.[4]
- Usually toenails (often asymmetric); may spread from tinea pedis.
- Organisms: dermatophytes (Trichophyton rubrum ~90%), Candida, non-dermatophyte moulds (Scopulariopsis, Aspergillus).[4]
- Diagnosis: CONFIRM with fungal culture/PCR BEFORE starting oral antifungals (clinical appearance alone is unreliable — ~50% of abnormal nails are NOT fungal). Send nail clippings for: (1) KOH microscopy (immediate; lower sensitivity); (2) fungal culture (Sabouraud agar; takes 4-6 weeks; identifies organism); (3) PCR (faster; 1-3 days; growing use).[2][4]
- Treatment:[2]
- Oral terbinafine 250 mg daily — first-line for dermatophyte onychomycosis; 6 weeks (fingernails), 12 weeks (toenails); monitor LFTs (baseline + at 6 weeks).[2]
- Oral itraconazole 200 mg daily or pulse therapy (1 week on, 3 weeks off × 3-4 pulses); alternative; CHF warning (negative inotrope); CYP3A4 inhibitor; monitor LFTs.[2]
- Topical (amorolfine 5% lacquer weekly, ciclopirox 8% lacquer daily) — for mild/localised disease or as adjunct; low cure rate for moderate-severe disease.[2]
- Prevent recurrence: treat concurrent tinea pedis; avoid barefoot in communal showers; keep feet dry; breathable socks/shoes.[2]
- Nail grows slowly: fingernails 3 mm/month; toenails 1 mm/month → visible improvement takes months; complete cure at 12-18 months for toenails.[2]
Nail psoriasis
- Pitting (ice-pick depressions on the nail plate surface), oil-drop/salmon patches (yellow-brown discoloration under the nail), onycholysis (separation of nail plate from bed; usually with an erythematous border), subungual hyperkeratosis (thickening under the nail).[1]
- Usually affects multiple nails symmetrically; skin psoriasis usually present elsewhere.[1]
- Management: treat underlying psoriasis; topical calcipotriol (vitamin D analogue) under the nail; intralesional triamcinolone into nail matrix; systemic/biologic for severe disease.[1]
Nail lichen planus
- Thinning, longitudinal ridging, fissuring of the nail plate; dorsal pterygium (the nail fold fuses with the nail bed → permanent scarring and nail loss).[3]
- May affect one or several nails; permanent nail loss if untreated.
- Management: urgent treatment to prevent permanent scarring (pterygium is irreversible); potent topical or intralesional corticosteroids; systemic corticosteroids for severe/progressive disease.[3]
Other common nail disorders
ABCDEF of nail signs
Iron deficiency: koilonychia (spoon nails), brittleness, onychorrhexis
Beau's lines: single transverse groove; severe illness, chemotherapy, high fever
Clubbing: bronchogenic carcinoma, ILD, cyanotic heart disease, IBD, SBE
Drugs: minocycline (blue-grey), antimalarials (blue-black), chemotherapy (Beau's, melanonychia)
Splinter haemorrhages: SBE (proximal), trauma (distal); Janeway lesions, Osler nodes
Onychomycosis 50% of all nail disease; T. rubrum 90%; confirm with KOH
| Condition | Description | Cause |
|---|---|---|
| Beau's lines | Transverse grooves across ALL nails at the same level | Systemic illness, chemotherapy, high fever (temporary cessation of nail growth) |
| Onycholysis | Separation of nail plate from nail bed | Trauma, thyroid, psoriasis, tetracyclines, fungal |
| Koilonychia | Spoon nails (concave) | Iron deficiency |
| Melanonychia | Longitudinal pigmented band | Benign (racial in dark skin); subungual melanoma if single band + Hutchinson's sign |
| Ingrown toenail (onychocryptosis) | Painful inflammation of lateral nail fold | Tight shoes, incorrect nail cutting; treat conservatively or wedge resection |
Quick numbers for the examiner
Special Nail Disorders & Morphology[1]
[1]Special nail morphology quick numbers
Rarer Nail Signs & Syndromes — High-Yield for Fellowship Viva
This section covers the less common but classically tested nail signs that examiners love. Each has a specific systemic association — knowing the morphology is half the answer; knowing the underlying cause is the other half.[1]
Koilonychia (spoon nails)
Concave, spoon-shaped depression of the nail plate that can hold a drop of water. Typically affects multiple fingernails in a symmetric pattern; toenails spared. Iron deficiency anaemia is the classic association (ferritin below 30 µg/L); it is also seen in Plummer-Vinson syndrome, haemochromatosis, Raynaud's disease, occupational exposure to mineral oils, and congenital forms. In children under 4 years, koilonychia can be a physiological variant. The nails become flat first, then concave, then the eponychium may elevate. Workup: CBC, ferritin, iron studies, and consider upper GI endoscopy if iron deficiency is unexplained. Treat the cause — the nails regrow with replacement of iron.[1]
Anonychia and onychatrophy
Anonychia = complete absence of the nail plate from birth (congenital) or following destruction of the matrix. Congenital anonychia is rare and may be isolated (autosomal dominant or recessive) or part of syndromes such as nail–patella syndrome (Fong disease) with absent/hypoplastic patellae, iliac horns, elbow dysplasia, and Lunula triangularis (triangular lunulae — pathognomonic). Acquired anonychia follows scarring lichen planus, severe trauma, burns, or Stevens-Johnson syndrome. Onychatrophy describes a shrunken, atrophic, rudimentary nail that fails to grow — also seen in lichen planus, peripheral vascular disease, and epidermolysis bullosa.[1]
Pterygium (dorsal and ventral)
Dorsal pterygium (nail lichen planus): the proximal nail fold fuses with the nail bed, splitting the nail into two portions that gradually shrink; the central split resembles a pterygium (wing). Irreversible scarring — every attempt at treatment is to halt progression, not regrow nail. Urgent potent/intralesional corticosteroid is the cornerstone. Ventral pterygium is rarer and may occur in Raynaud's disease, scleroderma, and graft-versus-host disease. Pseudo-pterygium is post-traumatic adhesion without active disease.[1]
Digital clubbing
Bulbous enlargement of the distal phalanx with loss of the Lovibond angle (normal less than 180°; clubbing greater than 180°). Schamroth's window test — placing the dorsal surfaces of two opposite distal phalanges together normally produces a diamond-shaped gap; in clubbing the gap obliterates. Phalangeal depth ratio (distal phalangeal depth / interphalangeal joint depth greater than 1) is the bedside screening rule. Causes: bronchogenic carcinoma (especially non-small-cell, apical; look for Horner's), suppurative lung disease (bronchiectasis, empyema, lung abscess, cystic fibrosis), cyanotic congenital heart disease, infective endocarditis, IBD (especially Crohn's), cirrhosis, thyroid acropachy, and idiopathic / familial. Unilateral clubbing suggests subclavian artery aneurysm, Pancoast tumour, or brachial plexus lesion. Rapid-onset clubbing + joint pain = hypertrophic pulmonary osteoarthropathy (synovitis, periostitis, finger clubbing) — think lung cancer.[1]
Lindsay's nails (half-and-half nails)
First described by Lindsay in 1967 in chronic renal failure. The nail plate shows a distinct sharp demarcation: the proximal 40-80% is white / dull (ground-glass appearance) and the distal 20-60% is red, pink, or brown. The border does NOT move with nail growth (unlike Mees lines) — suggesting nail bed rather than nail plate pathology. Found in up to 40% of patients on chronic haemodialysis and correlates with azotaemia; rare in earlier CKD stages. The proposed mechanism is increased melanin deposition in the distal nail bed. Not pathognomonic — also reported in Crohn's disease, Kawasaki disease, Behçet disease, cirrhosis, and zinc deficiency.[1]
Splinter haemorrhages
Tiny linear, reddish-brown, longitudinally oriented streaks under the nail plate, resembling wood splinters under the nail. They represent microemboli or microthrombi in the longitudinally oriented capillaries of the nail bed. The classic association is infective endocarditis — but trauma is the commonest cause (most distal splinters; usually 1-2 nails). Proximal splinters or multiple splinters across many nails raise concern for SBE, antiphospholipid syndrome, vasculitis (polyarteritis nodosa, microscopic polyangiitis, rheumatoid vasculitis), cryoglobulinaemia, scurvy, and psoriasis. On exam: count the splinters, check the distribution (distal vs proximal, single vs multiple), look for other stigmata (Janeway lesions, Osler nodes, Roth spots, murmur), and order blood cultures × 3, echo, ANA, ANCA, antiphospholipid antibodies, and viral hepatitis serology as clinically indicated.[1]
Muehrcke's lines
Paired, transverse, white bands that run parallel to the lunula across multiple nails — first described by Robert Muehrcke in 1956. Unlike Mees or Beau lines, Muehrcke's lines do NOT move with nail growth (they are in the nail bed, not the nail plate) and disappear transiently when the nail is compressed (because they are due to vascular changes in the nail bed). Classically associated with hypoalbuminaemia (serum albumin below 2.2 g/dL — the threshold for clinical detection); seen in nephrotic syndrome, liver cirrhosis, severe malnutrition, and after chemotherapy. They resolve as albumin normalises. Differentiate from Mees lines (transverse white lines that MOVE with nail growth; arsenic/thallium/heavy-metal poisoning, chemotherapy).[1]
Terry's nails
Originally described by Dr. Richard Terry in 1954 in patients with hepatic cirrhosis. The nail is white / opaque over the proximal 80% with a narrow pink-brown distal band 1-2 mm wide (the Terry's band). The lunula is obliterated. Like Muehrcke's, it does not move with growth — it is a nail bed sign. Causes: cirrhosis (classic; ~80% of cirrhotics may have it), chronic congestive heart failure, diabetes mellitus (type 2), hyperthyroidism, malnutrition, and advanced age. Often coexists with clubbing in chronic liver disease. The pathophysiology involves decreased vascularity of the nail bed with increased connective tissue. Distinguish from Lindsay (half-and-half) — Terry has a narrower distal pink band (1-2 mm) with the proximal 80% white; Lindsay has roughly equal white/pink halves.[1]
Half-and-half nails (Lindsay) vs Terry's vs Muehrcke's vs Mees
All four are paired transverse white bands of the nail and commonly confused. The key discriminators:[1]
- Lindsay / half-and-half — proximal white (40-80%) + distal pink/brown (20-60%) with sharp border; does NOT move with growth; CKD / haemodialysis; vascular bed sign.
- Terry's — proximal white (80%) + narrow distal pink-brown band (1-2 mm); does NOT move; cirrhosis, CHF, diabetes; vascular bed sign.
- Muehrcke's — paired transverse white lines that do NOT move with growth; blanch on compression; hypoalbuminaemia (nephrotic, cirrhosis, malnutrition).
- Mees — single transverse white line(s) that DO move with growth; no blanching; arsenic / thallium poisoning, chemotherapy, heavy metals — nail plate sign.[1]
Yellow nail syndrome (YNS)
A rare triad first described by Samman and White in 1964: (1) slow-growing, thickened, yellow-green, hard nails with onycholysis, cross-ridging, and loss of lunula and cuticle; (2) lymphoedema (usually peripheral, often lower limbs); (3) respiratory manifestations (chronic cough, bronchiectasis, pleural effusion, recurrent sinusitis). Nails grow less than 0.25 mm/week (normal 0.5 to 1.2 mm/week) and may shed spontaneously. Pathogenesis is impaired lymphatic drainage (functional lymphangiectasia) — nails, lymphatics, and lungs share lymphatic endothelial dysfunction. Associations: cancers, immunodeficiency, connective tissue disease, exposure to titanium, D-penicillamine, and BUCCOLAM. Differential includes onychomycosis, psoriasis, and drug-induced yellowing (tetracyclines, beta-carotene). Treatment is difficult — vitamin E (tocopherol) 1000 IU daily, itraconazole pulses (sometimes helpful), oral zinc, and aggressive management of the underlying lymphatic and respiratory disease. Spontaneous remission occurs in up to 30% of cases. Prognosis is dominated by the underlying disease — 5-year mortality ~25-50%, mostly from respiratory failure, malignancy, or infection.[1]
Rarer nail signs quick numbers
Procedures & Surgical Management
[2]Nail matrix biopsy — operative technique and indications
When a pigmented or unexplained nail lesion must be sampled, the site of biopsy determines what pathology you can diagnose, and the technique differs from cutaneous punch biopsy. For a longitudinal melanonychia (single pigmented band, especially with Hutchinson's sign), the standard is a 3 mm punch biopsy of the proximal nail fold and matrix centred over the pigment origin, or a longitudinal lateral biopsy of the entire matrix if the band is wide or atypical — the latter gives full-thickness histology and is the preferred approach in most centres for suspected subungual melanoma because it allows accurate Breslow depth measurement, which shave biopsy cannot.[1]
Steps: (1) digital nerve block with 1-2% plain lidocaine (no adrenaline); (2) exsanguinate and apply a digital tourniquet (Penrose drain or commercial finger tourniquet — record time, maximum 30 min); (3) avulse the overlying nail plate by splitting longitudinally with a Beaver blade and lifting it off the matrix; (4) for matrix biopsy, take a 3 mm punch through the matrix to bone (matrix lies just above bone, full-thickness is required for staging); (5) for bed biopsy, take a 2-3 mm wide × 4-5 mm long ellipse from the bed after avulsion; (6) suture the matrix defect with absorbable 6-0 if needed; (7) dress and remove tourniquet. Onychocryptosis (matrixectomy with phenol 88%) is technically a destruction not a biopsy — the avulsed lateral spicule is sent only if clinically suspicious, but the procedure is therapeutic, not diagnostic. Send all true biopsies in formalin for histopathology; do NOT put phenol-treated tissue in formalin for histology as it is destroyed.[1]
Specific drug doses — onychomycosis oral regimens
Three oral regimens are the workhorses; choose on organism, comorbidity and drug interactions. Baseline LFTs are mandatory for all three; recheck at 4-6 weeks if abnormal or on long courses.[2][4]
- Terbinafine 250 mg once daily — first-line for dermatophyte onychomycosis (Trichophyton rubrum, T. mentagrophytes); 6 weeks for fingernails, 12 weeks for toenails; take with food; fungicidal; minimal drug interactions; check baseline LFTs; rare taste/smell disturbance, rare severe cutaneous reactions (SJS).[2]
- Itraconazole 200 mg pulse — 200 mg twice daily for 1 week, then 3 weeks off, repeat × 3 pulses for fingernails or × 4 pulses for toenails; alternative for dermatophytes, also covers Candida and some non-dermatophyte moulds; avoid in CHF (negative inotrope); potent CYP3A4 inhibitor (statins, warfarin, colchicine, DOACs); take with acid drink (cola) for absorption.[2]
- Fluconazole 150 mg once weekly — third-line; useful when terbinafine and itraconazole are contraindicated; mild-mod disease; 6-9 months for fingernails, 9-12 months for toenails; fewest drug interactions of the three; safe in renal impairment at weekly dosing.[2]
Topical adjuncts (mild disease, superficial white onychomycosis, or adjuvant to oral): amorolfine 5% lacquer once weekly, ciclopirox 8% lacquer daily × 6-12 months. Systemic nail treatment is slow because the nail grows only 3 mm/month (finger) or 1 mm/month (toe) — clinical cure requires full regrowth which takes 12-18 months for a great toenail.[2]
Nail procedure & oral antifungal quick numbers
Onychomycosis vs Nail Psoriasis vs Nail Lichen Planus
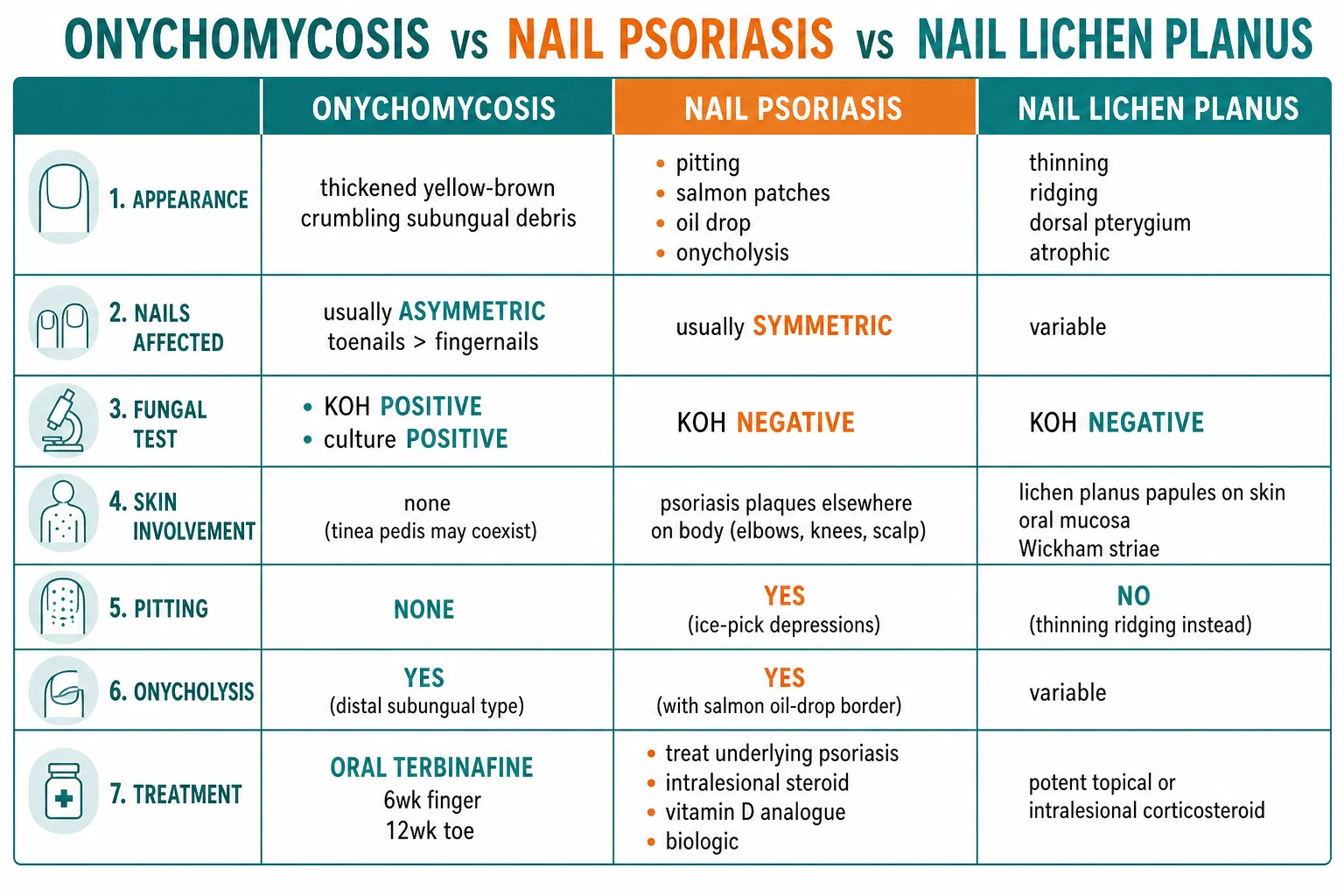
| Feature | Onychomycosis | Nail psoriasis | Nail lichen planus |
|---|---|---|---|
| Appearance | Thickened, yellow-brown, crumbling, subungual debris | Pitting, oil-drop, onycholysis with erythematous border | Thinning, ridging, dorsal pterygium |
| Fungal test | KOH + culture + | KOH − | KOH − |
| Pitting | No | Yes | No |
| Distribution | Often asymmetric, toenails > fingernails | Symmetric | Variable; may be single nail |
| Skin signs | Tinea pedis may coexist | Psoriasis plaques elsewhere | LP papules on skin/mucosa |
| Treatment | Terbinafine (6wk finger/12wk toe) | Treat psoriasis; intralesional steroid | Urgent corticosteroid (prevent pterygium) |
High-yield nail signs of systemic disease
Nail Signs of Systemic Disease
Quick numbers for the examiner
INGROWN NAIL — ingrown toenail management
Cellulitis/tissue infection: oral flucloxacillin; soak in warm saline/iodine
Partial or total nail avulsion under local anaesthetic; phenol ablation of matrix for definitive cure
Lift the lateral edge of the nail with a cotton wick; offloads the inflamed fold
Wide-toe box, low heel; avoid narrow/tight footwear
Flucloxacillin or erythromycin; treat surrounding cellulitis if present
Definitive surgery: wedge resection of the lateral nail fold and underlying matrix
Cut nails straight across; do NOT cut down the lateral edges; this is the commonest cause
Sensible footwear; cotton socks; allow toes to spread
Povidone-iodine or chlorhexidine soak; prevention of infection
Lift lateral edge with cotton wick inserted under the ingrown edge to offload
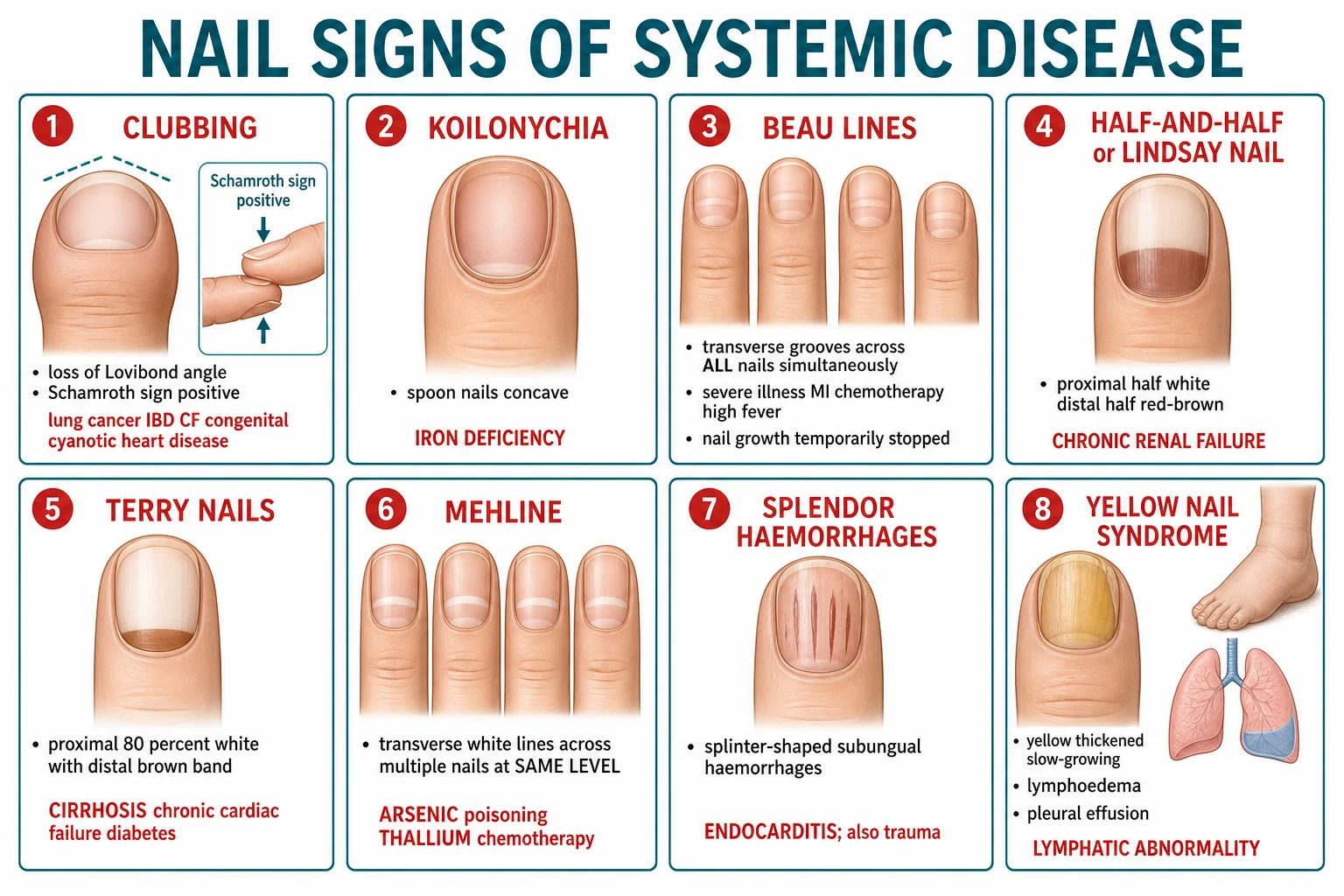
| Sign | Appearance | Systemic association |
|---|---|---|
| Clubbing | Loss of Lovibond angle; Schamroth sign positive | Lung cancer, IBD, CF, cyanotic heart disease |
| Koilonychia | Spoon nails (concave) | Iron deficiency |
| Beau's lines | Transverse grooves across ALL nails simultaneously | Severe illness, MI, chemotherapy, high fever |
| Half-and-half (Lindsay nail) | Proximal half white, distal half red-brown | Chronic renal failure |
| Terry nails | Proximal 80% white with distal brown band | Cirrhosis, chronic heart failure, diabetes |
| Mees lines | Transverse white lines across multiple nails at same level | Arsenic/thallium poisoning, chemotherapy |
| Splinter haemorrhages | Splinter-shaped subungual haemorrhages | Endocarditis (also trauma) |
| Yellow nail syndrome | Yellow thickened slow-growing nails + lymphoedema + pleural effusion | Lymphatic abnormality |
Onychomycosis Diagnosis and Management
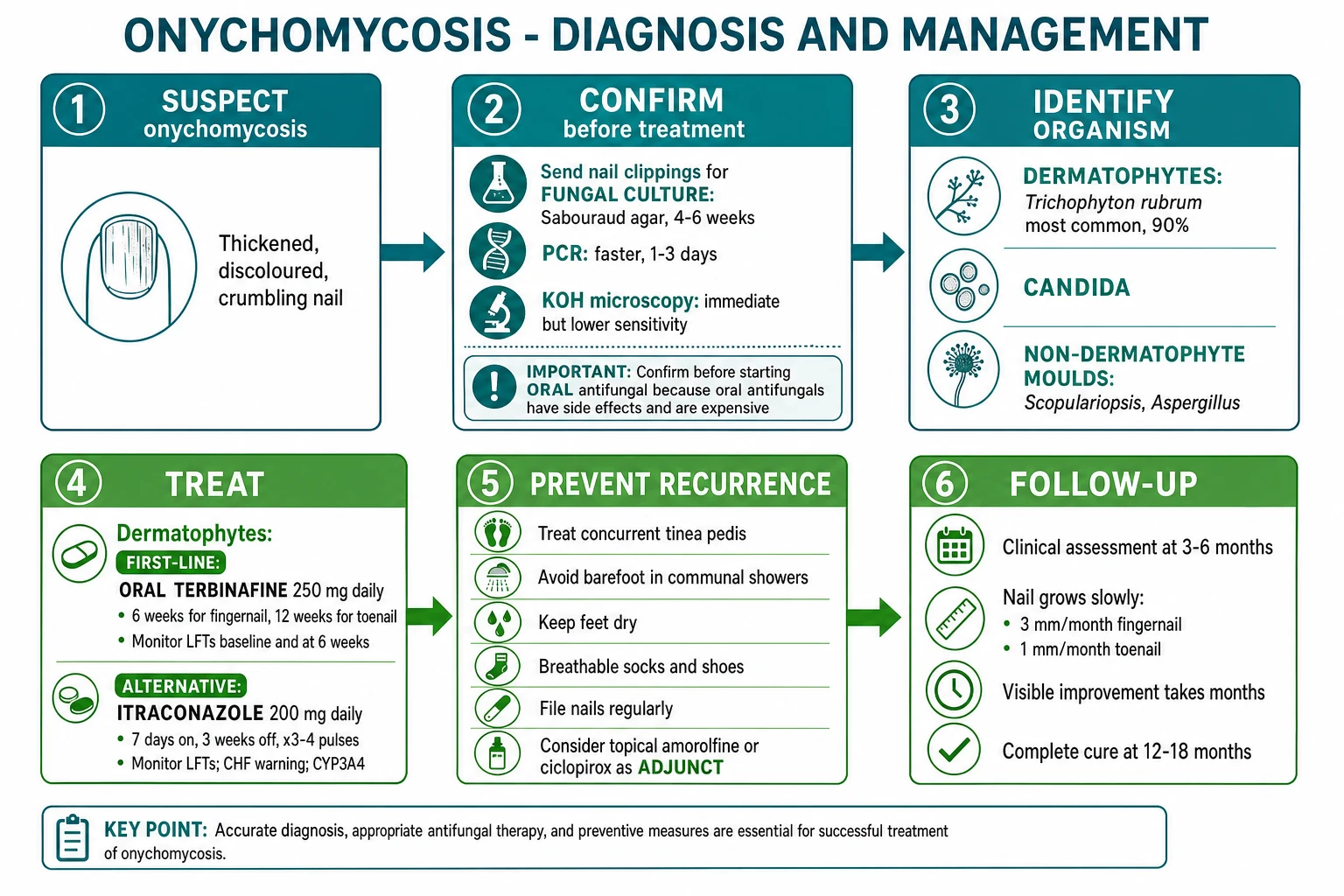
- ALWAYS confirm with fungal culture/PCR before starting oral antifungal — clinical appearance alone is unreliable (~50% of abnormal nails are NOT fungal); oral antifungals have side effects (hepatotoxicity) and cost.[2][4]
- Terbinafine = first-line for dermatophytes (T. rubrum — 90% of cases); fungicidal.[2]
- Itraconazole = alternative; broader spectrum (also covers Candida and some moulds); pulse therapy; CHF warning; CYP3A4 inhibitor.[2]
- Nail growth is slow → visible improvement takes months; toenails may take 12-18 months to completely replace.[2]
Exam Pearls
Red Flags
Exam application bank (NEET-PG / INICET)
One-line answer
Comprehensive nail disorders reference for MBBS/board exam: Onychomycosis (tinea unguium — confirm with KOH/PCR before oral antifungal; terbinafine 250 mg daily 6wk finger/12wk toe first-line; alternatives itraconazole pulse 200 mg BID 1-week-on/3-weeks-off ×3, fluconazole 150 mg weekly); Nail psoriasis (pitting, oil-drop, onycholysis with erythematous border); Nail lichen planus (dorsal pterygium is irreversible scarring — urgent corticosteroid); Beau's lines, Onycholysis, Koilonychia (iron deficiency), Melanonychia (single band + Hutchinson's sign → subungual melanoma biopsy). Special types: trachyonychia / twenty-nail dystrophy (rough nails ± alopecia areata; biotin 5-10 mg daily for brittle nails, biotin deficiency dose 5 mg), median nail dystrophy (central canaliform split), onychogryphosis (ram's horn toenail), onychauxis (thickened nail without deformity), parakeratosis pustulosa[1]
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard.[5]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes.[1]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change.[1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each.[1]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory.[1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Nail disorders.
[1]References
- [1]Hwang JK, Grover C, Iorizzo M, et al. Nail psoriasis and nail lichen planus: Updates on diagnosis and management. Journal of the American Academy of Dermatology, 2024.PMID 38007038
- [2]Lipner SR, Scher RK. Onychomycosis: Treatment and prevention of recurrence. Journal of the American Academy of Dermatology, 2019.PMID 29959962
- [3]Gupta MK, Lipner SR. Review of Nail Lichen Planus: Epidemiology, Pathogenesis, Diagnosis, and Treatment. Dermatologic Clinics, 2021.PMID 33745635
- [4]Gupta AK, Stec N, Summerbell RC, et al. Onychomycosis: a review. Journal of the European Academy of Dermatology and Venereology : JEADV, 2020.PMID 32239567
- [5]Leung AKC, Lam JM, Leong KF, et al. Onychomycosis: An Updated Review. Recent patents on inflammation & allergy drug discovery, 2020.PMID 31738146