Dermatology · Medicine
Pityriasis rosea
Also known as Pityriasis rosea Gibert
Pityriasis rosea is an acute, self-limiting papulosquamous eruption of probable herpesviral aetiology (HHV-6/7 reactivation), characterised by a herald patch and a secondary eruption in a Christmas-tree distribution. Fellowship-level assessment requires recognition of classic and atypical morphology, validated diagnostic criteria, histopathological and dermoscopic clues, targeted differential diagnosis, evidence-based symptomatic and antiviral therapy, and the pregnancy-adverse-outcome signal.
On this page & tools
Your progress
Saved locally on this device.
Exam tags
Red flags
Definition & Classification
Pityriasis rosea (PR) is an acute, self-limiting inflammatory dermatosis of the papulosquamous group. It is clinically characterised by: [1]
- A single, larger herald patch in most cases.
- A subsequent generalised eruption of oval, salmon-pink or erythematous plaques with a peripheral collarette of scale.
- A characteristic distribution along skin cleavage lines, producing the "Christmas-tree" pattern on the trunk. [1]
A comprehensive classification divides PR into classic and atypical forms, with further subdivision by morphology, distribution, and disease course.[1]
| Form | Features | Exam relevance |
|---|---|---|
| Classic PR | Herald patch → generalised oval plaques, truncal/proximal limb distribution, collarette scale, Christmas-tree orientation | Board-favourite morphology |
| Atypical PR | Inverse, vesicular, urticarial, purpuric, unilateral, localized, persistent, or mucosal variants | Diagnostic pitfall; may need biopsy |
| Pityriasis rosea-like drug eruption | Often more extensive, eosinophils on biopsy, temporal association with medication (e.g., captopril, isotretinoin, TNF inhibitors) | Stop suspected drug |
| Pityriasis rosea-like exanthem | COVID-19 infection or vaccination have been reported triggers | Take exposure history |

Epidemiology & Risk Factors
Pityriasis rosea affects all ages but peaks in adolescents and young adults (10–35 years). It accounts for approximately 0.5–2% of dermatology outpatient diagnoses and is slightly more common in females in some series.[2][9]
Key epidemiological points [1]
- Seasonal clustering in spring and autumn has been reported in temperate climates, supporting an infectious trigger.
- A mild prodrome of malaise, low-grade fever, headache, or lymphadenopathy occurs in a minority of patients.
- Recurrence is uncommon (~2%).
- There is no consistent racial or geographical predilection, although darker skin phototypes may show more violaceous or post-inflammatory pigmentary change. [1]
Pathophysiology
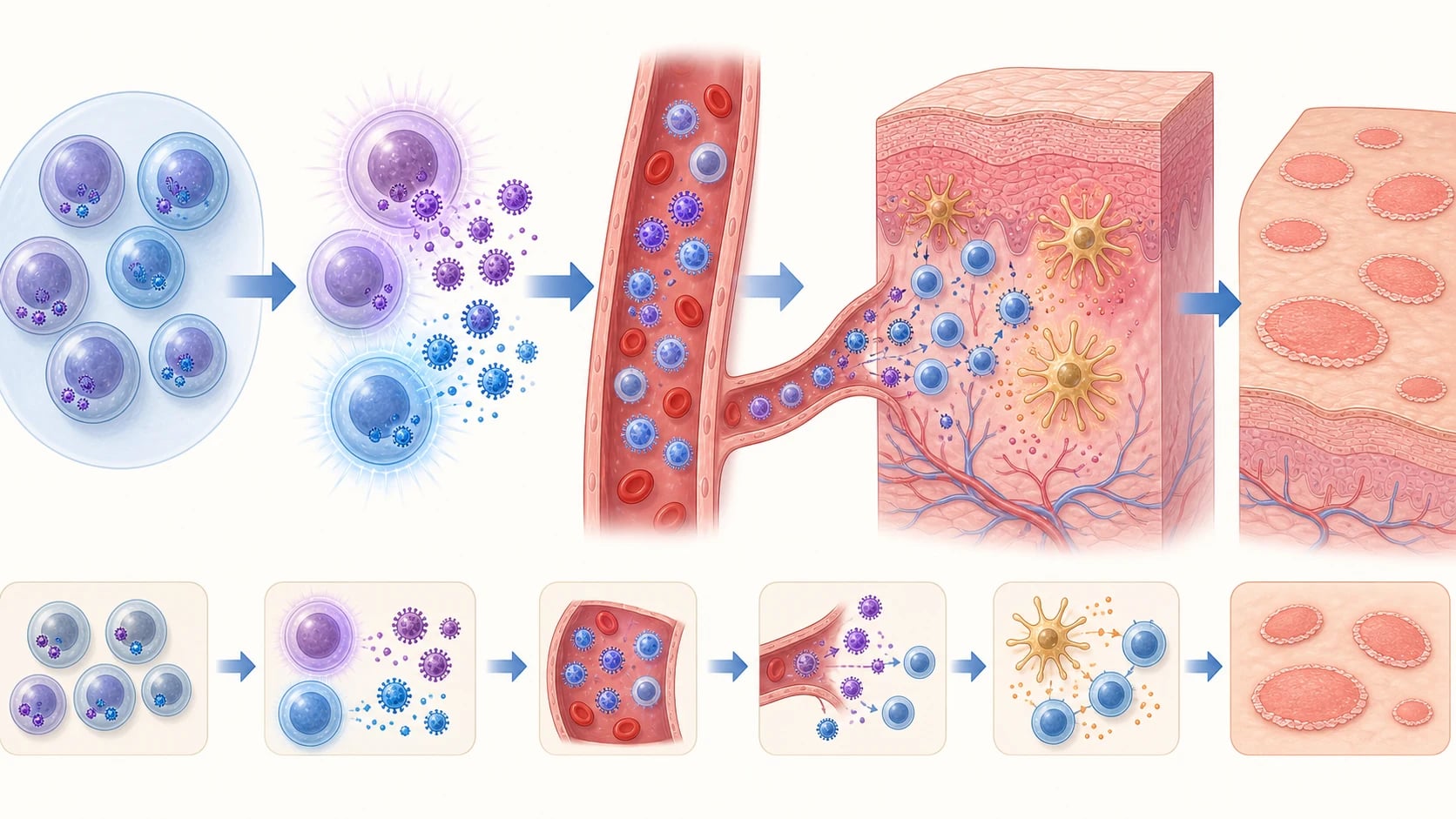
The exact cause remains unproven, but the leading hypothesis is endogenous reactivation of human herpesvirus-6 (HHV-6) and/or HHV-7, with a subsequent cell-mediated immune response in the skin. [1]
Evidence for HHV-6/7
- Viral DNA has been detected in plasma, peripheral blood mononuclear cells, saliva, and lesional skin of PR patients using PCR.
- Calibrated quantitative real-time PCR with concurrent plasma and skin sampling improves detection and supports active replication rather than incidental latency.
- Some studies have reported conflicting results, likely reflecting differences in PCR technique, tissue sampled, and timing relative to rash onset. [1]
Viral reactivation model — latency, viraemia, and skin seeding
Both HHV-6 (variants A and B) and HHV-7 are beta-herpesviruses that establish lifelong latency after primary infection in early childhood — HHV-6 typically by age two (roseola infantum, exanthem subitum), HHV-7 slightly later. Latency is maintained principally in CD34+ haematopoietic progenitor cells, CD4+ and CD8+ T lymphocytes, monocytes, macrophages, and salivary-gland epithelium; chromosomal integration of HHV-6 DNA into the host germline (ciHHV-6) occurs in roughly 0.5–1% of the population and complicates PCR interpretation, because a positive whole-blood result in such individuals reflects chromosomally integrated viral DNA rather than active replication. [1]
The proposed sequence in classic pityriasis rosea is therefore: [1]
- Trigger — intercurrent physiological stress (fatigue, sleep deprivation, recent viral upper-respiratory infection), immunosuppression, drug exposure, or seasonal change permits endogenous reactivation of latent HHV-6 (most often variant B) and/or HHV-7.
- Viraemia — cell-free viral DNA spills into plasma; quantitative real-time PCR on paired plasma and lesional skin substantially raises detection sensitivity over skin biopsy alone (Aydin Kurc et al., Diagnostics 2024).
- Cutaneous seeding — viral particles traffic to the skin via infected lymphocytes or via cell-free spread; the herald patch is thought to represent the initial cutaneous focus of viral replication.
- Host immune response — antiviral CD4+ and CD8+ T-cell responses, Langerhans-cell activation, and a Th1-skewed cytokine milieu (interferon-gamma, IL-2, TNF-alpha) generate the secondary eruption; resolution coincides with effective cell-mediated control of viral replication.
- Latency re-established — virus returns to latency in the lymphoid reservoir; recurrent PR is uncommon but documented, particularly in immunocompromised hosts. [1]
HHV-6 reactivation
variant B (roseola strain)
- Most consistently recovered from PR lesional skin and plasma
- Strongest correlate with the herald-patch phenotype and the post-viral-prodrome symptom cluster
- Plasma viral load is quantitatively higher in pregnancies ending in poor outcome (Drago et al., JAAD 2008)
- Integrates into the host telomere in ~1% of individuals (ciHHV-6) — interpret positive whole-blood PCR cautiously
HHV-7 reactivation
co-factor or alternative driver
- Frequently co-detected with HHV-6 in PR lesions and saliva
- Some series suggest HHV-7 is the dominant or sole detectable virus, particularly in children and adolescents
- Salivary shedding is near-universal in adulthood, so swab PCR alone is unreliable as proof of causality
- Proposed as a trans-acting reactivator of latent HHV-6 — supports a two-hit viral model
Cell-mediated immunity
the cutaneous effector
- Dermal CD4+ T-cell predominant infiltrate with Langerhans-cell recruitment
- Th1-skewed cytokine profile (IFN-gamma, IL-2, TNF-alpha) explains the spongiotic, parakeratotic histology
- Onset 1–2 weeks after the viraemic peak mirrors the time required for clonal T-cell expansion
- Immunosuppression (HIV, biologics, chemotherapy) can prolong, recur, or atypically present PR
Immunology
PR lesions show a T-cell infiltrate (predominantly CD4+ in the dermis) and Langerhans cells, consistent with a host immune response to viral antigen. The herald patch may represent the initial site of viral reactivation, with the secondary eruption reflecting systemic spread.[2]
Clinical Presentation
The herald patch
- Occurs in 50–90% of cases, usually 1–2 weeks before the generalised eruption.
- A single, oval, salmon-pink or erythematous plaque, 2–5 cm in diameter.
- Has a collarette of scale (peripheral scale with central clearing) and may be mistaken for tinea corporis.
- Common sites: trunk, neck, proximal limbs. [1]
The secondary eruption
- Appears in crops over 7–14 days.
- Multiple smaller oval papules and plaques, typically 0.5–2 cm.
- Distributed over the trunk and proximal extremities, sparing the face and distal limbs in classic cases.
- Long axes of the oval lesions align along skin cleavage lines (Langer lines), producing the "Christmas-tree" pattern on the back.
- Lesions may be mildly pruritic; intense itching is uncommon and should prompt consideration of atypical variants or differential diagnoses. [1]
Systemic symptoms
A minority report low-grade fever, malaise, headache, or arthralgia preceding the rash. [1]
[1] [4] [9]Atypical variants
| Variant | Description | Pitfall |
|---|---|---|
| Inverse PR | Lesions predominantly in axillae, groin, or skin folds | Mimics tinea, inverse psoriasis, intertrigo |
| Vesicular PR | Small vesicles within or at the edge of plaques | Mimics varicella, dermatitis herpetiformis |
| Urticarial PR | Oedematous, pruritic plaques | Mimics urticaria |
| Purpuric/petechial PR | Haemorrhagic lesions | Mimics vasculitis, thrombocytopenia |
| Unilateral/localised PR | Limited to one body area | Mimics nummular eczema, tinea |
| Persistent PR | Rash lasts >3 months | May need biopsy to exclude mycosis fungoides |
| Mucosal involvement | Oral erosions, ulcers, or plaques | Mimics lichen planus, secondary syphilis |
Atypical variants — detailed morphology, pitfalls, and mimics
Up to 20% of pityriasis rosea cases deviate from classic morphology, and these are the cases most likely to present to a tertiary pigmented-skin clinic, an emergency department, or an obstetrics clinic. Recognising the morphology by subtype is the single highest-yield fellowship-level skill in this topic. [1]
Inverse (axillary, inguinal, and flexural) PR. The eruption localises to the axillae, groin, submammary folds, and neck, often sparing the classic truncal Christmas-tree distribution. Lesions are typically more pruritic and oedematous in flexural skin because of maceration, and the peripheral collarette scale is the discriminator from tinea cruris, inverse psoriasis, erythrasma (coral-red Wood's lamp fluorescence), and intertriginous candidiasis. Inverse PR is over-represented in children, in skin of colour, and in patients using topical steroids — in whom steroid-modified "tinea incognito"-like presentations are common. [1]
Vesicular PR. Crops of clear, tense vesicles 1–3 mm in diameter develop within or adjacent to the herald patch and secondary plaques, occasionally with central umbilication. When the vesicles predominate, the eruption mimics varicella, herpes zoster (when dermatomal), dermatitis herpetiformis, or bullous insect hypersensitivity. Mucosal vesicles or erosions (oral, genital) occur in a minority but should prompt consideration of pemphigoid, linear IgA disease, and secondary syphilis. Vesicular PR is more common in children and young adults and may follow a more prolonged course (8–12 weeks). [1]
Purpuric PR. Petechiae or palpable purpura develop within otherwise typical plaques, producing the "pityriasis rosea with haemorrhagic lesions" phenotype. The mechanism is thought to be perivascular lymphocytic vasculitis with erythrocyte extravasation, not a true leukocytoclastic vasculitis — direct immunofluorescence is typically negative. The key differential is purpuric drug eruption, IgA vasculitis (Henoch-Schönlein), and hypergammaglobulinaemic purpura; platelet count, coagulation screen, and urinalysis should be checked. Purpuric PR is self-limiting and resolves with the parent eruption, but cosmetically more conspicuous and slower to fade. [1]
PR-like drug eruption (persistent pityriasis rosea-like eruption). A clinically indistinguishable eruption can be triggered by a growing list of medications — most consistently reported with captopril and other ACE inhibitors, isotretinoin, allopurinol, gold, penicillins, metronidazole, terbinafine, TNF-alpha inhibitors, baricitinib, adalimumab, and COVID-19 mRNA vaccination. The eruption typically lasts more than 3 months (hence "persistent pityriasis rosea-like eruption"), histology shows eosinophil-rich interface or perivascular dermatitis, and withdrawal of the suspect drug produces gradual resolution over weeks to months. Differentiating features from classic PR are therefore: drug temporal relationship, eosinophil-rich biopsy, persistent course beyond 12 weeks, and resistance to standard symptomatic therapy. [1]
Inverse PR
flexural accentuation
- Axillae, groin, neck, submammary folds; truncal Christmas-tree pattern may be absent
- More pruritic and oedematous than classic PR because of maceration
- Differential: tinea cruris (KOH+), inverse psoriasis (silvery scale), erythrasma (Wood lamp coral-red), candidal intertrigo (satellite pustules)
- Clue: collarette scale at the lesion edge is preserved, even in flexures
- Course: same self-limiting 6–12 week trajectory; treat with mid-potency topical steroid and emollient
Vesicular PR
clear fluid-filled lesions
- 1–3 mm tense clear vesicles within or adjacent to PR plaques; rare central umbilication
- Mimics: varicella (centripetal, all stages), herpes zoster (dermatomal), dermatitis herpetiformis (grouped on extensors, pruritic), bullous insect hypersensitivity
- Mucosal vesicles/erosions broaden the differential — exclude pemphigoid, linear IgA disease, secondary syphilis
- More common in children and young adults; course often 8–12 weeks
- Treatment is supportive; consider oral acyclovir if symptomatic and HHV-driven
Purpuric PR
haemorrhagic lesions
- Petechiae or palpable purpura within typical PR plaques
- Mechanism: perivascular lymphocytic vasculitis with erythrocyte extravasation (DIF negative)
- Differential: purpuric drug eruption, IgA vasculitis (check urinalysis and platelet count), hypergammaglobulinaemic purpura
- Self-limiting; resolves with the parent eruption; cosmetically slower to fade
- No specific therapy beyond reassurance and treatment of the underlying PR
PR-like drug eruption
persistent, eosinophil-rich
- Offenders: ACE inhibitors, isotretinoin, allopurinol, gold, penicillins, metronidazole, terbinafine, TNF inhibitors, COVID-19 vaccination
- Course >3 months — "persistent pityriasis rosea-like eruption"
- Histology: eosinophil-rich interface or perivascular dermatitis (vs classic PR — usually eosinophil-poor)
- Treatment: identify and withdraw the culprit drug; topical corticosteroid; course settles over weeks to months
- Differentiation from true PR hinges on drug temporal link, eosinophil-rich biopsy, and persistence
Atypical variants — quick-reference clinical signals
HERALD — the atypical-pitfall sieve
HERALD
The single collarette-scale plaque is regularly misdiagnosed as tinea corporis — KOH the leading edge if the scale is atypical; dermoscopy shows peripheral collarette scale plus dotted vessels, not the advancing hyphal border of tinea.
Guttate psoriasis (post-streptococcal, silvery scale, Auspitz sign), secondary syphilis (palms/soles, lymphadenopathy, RPR positive), lichen planus (Wickham striae, flexor wrists), pityriasis lichenoides chronica (red-brown papules with fine scale, chronic course).
Axillae, groin, and skin folds — mimics tinea cruris, inverse psoriasis, and intertrigo; collarette scale at the edge is the discriminator.
Vesicular PR can mimic varicella or dermatitis herpetiformis; mucosal lesions broaden the differential to lichen planus or secondary syphilis.
Persistent PR should trigger biopsy to exclude mycosis fungoides or PR-like drug eruption (eosinophils on histology, temporal link to captopril, isotretinoin, TNF inhibitors, or COVID-19 vaccination).
PR-like drug eruption and COVID-19-related exanthem share morphology; the temporal relation to medication or recent viral illness, plus eosinophils on biopsy, point to the cause.

Differential Diagnosis
[1]Pityriasis rosea
classic morphology
- Herald patch precedes the secondary eruption by 1–2 weeks
- Oval salmon-pink plaques with peripheral collarette scale along skin cleavage lines
- Truncal and proximal limb — Christmas-tree pattern on the back
- Palms/soles spared; mucosa spared
- Self-limiting over 6–12 weeks; serology negative; KOH negative
Secondary syphilis
the critical mimic
- Copper-red papulosquamous eruption including palms/soles and mucous membranes
- Generalised lymphadenopathy, low-grade fever, condylomata lata
- History of primary chancre weeks earlier; risk-factor screen positive
- RPR/VDRL reactive; treponemal test positive
- Treatment: intramuscular benzathine penicillin G 2.4 million units
Guttate psoriasis
drop-like mimic
- Abrupt eruption of 2–10 mm salmon-pink drop-like papules with silvery scale
- Strongly linked to recent streptococcal pharyngitis or perianal streptococci
- Auspitz sign positive; nail pitting may be present
- Trunk and proximal limbs; spares palms/soles
- Treatment: phototherapy, tonsillectomy if recurrent, topical or systemic therapy for chronic disease
Tinea corporis
annular mimic
- Annular plaque with active scaly advancing border and central clearing
- Single or few lesions; KOH from the border shows branching septate hyphae
- Scaling more pronounced at the periphery; pruritus common
- May complicate by tinea incognito after topical steroid misuse
- Treatment: topical terbinafine 1% OD–BD 1–2 weeks; oral antifungal if extensive
Clinical & Bedside Assessment
Chuh diagnostic criteria (2003)
Validated clinical criteria that allow diagnosis without laboratory testing: [1]
Essential features (all required)
- Discrete circular or oval lesions.
- Scaling on most lesions.
- Peripheral collarette scaling with central clearance on at least two lesions. [1]
Optional features (at least one required)
- Truncal and proximal limb distribution (less than 10% of lesions distal to mid-upper-arm and mid-thigh).
- Orientation of most lesions along skin cleavage lines (Christmas-tree pattern).
- Herald patch appearing at least 2 days before secondary eruption. [1]
Exclusion criteria (none may be present)
- Multiple small vesicles at the centre of two or more lesions.
- Two or more lesions on palmar or plantar skin surfaces. [1]
Dermoscopy
Dermoscopy is useful when the diagnosis is uncertain or the herald patch is atypical. [1]
Characteristic findings [1]
| Feature | Description | Frequency |
|---|---|---|
| Peripheral collarette scale | Fine scale attached to the periphery, pointing inwards | Most consistent |
| Peripheral dotted vessels | Patchy distribution at the edge | 35–65% |
| Central yellow with peripheral reddish background | Background colour pattern | ~40% |
| Central scale / brown globules / blood spots | Supporting features | Variable |
In darker skin phototypes the background may appear more violaceous with white scales. [1]
[10] [11]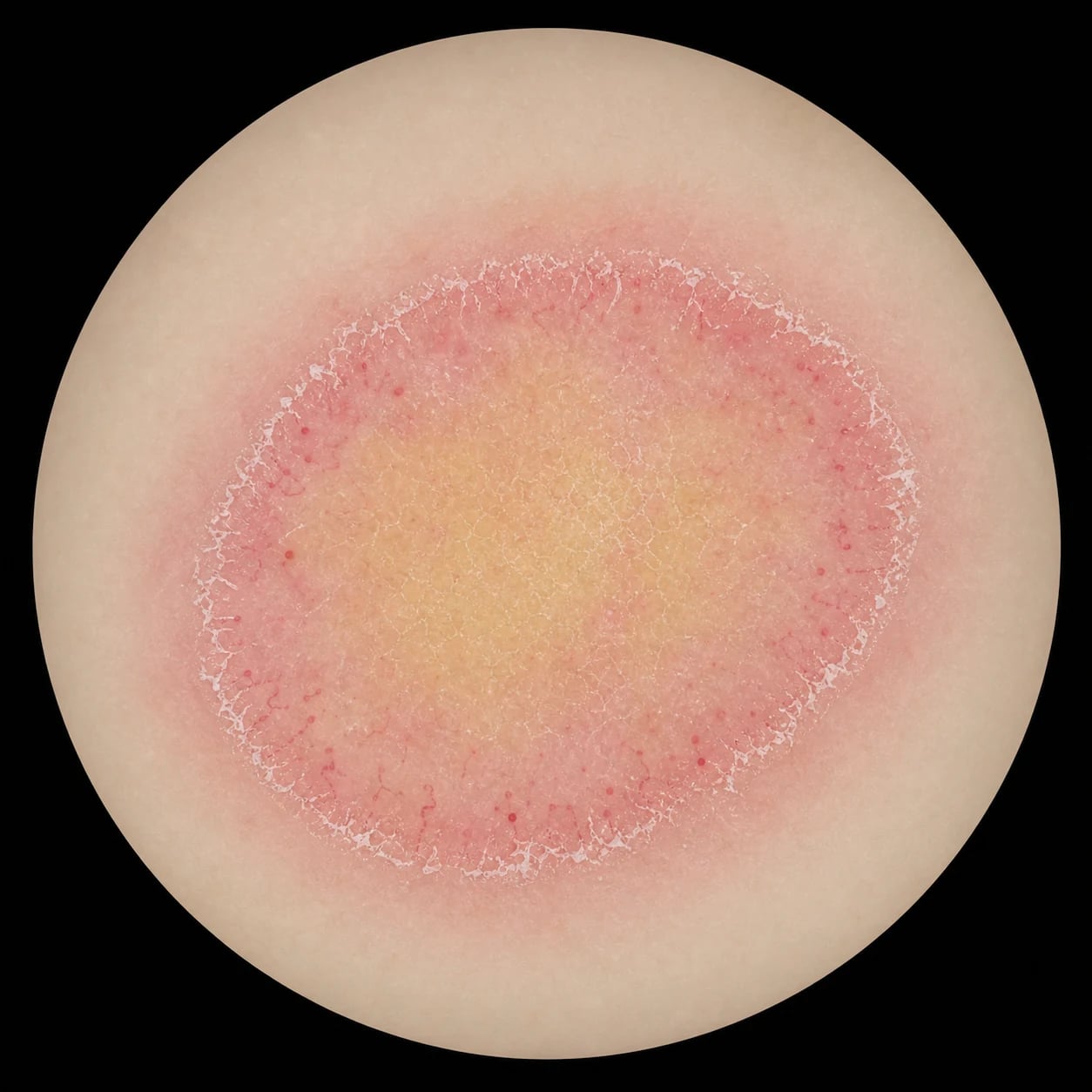
Investigations
Pityriasis rosea is primarily a clinical diagnosis. Investigations are reserved for atypical cases or when the differential includes conditions requiring laboratory confirmation. [1]
When to investigate
- Atypical morphology (palmar/plantar, vesicular, purpuric, mucosal, persistent).
- Systemic symptoms or lymphadenopathy suggesting secondary syphilis.
- Pregnancy.
- Lesions persisting beyond 3 months or failing to respond to conservative therapy.
- Diagnostic uncertainty requiring histopathology. [1]
Useful tests
| Test | Rationale |
|---|---|
| RPR/VDRL + treponemal test | Exclude secondary syphilis in atypical or high-risk patients |
| KOH preparation / fungal culture | Exclude tinea corporis when herald patch is atypical |
| Skin biopsy | Atypical cases; nonspecific spongiotic dermatitis pattern with clues |
| HHV-6/7 PCR | Research or selected refractory cases; not routine |
Histopathology
PR histology is nonspecific and resembles subacute spongiotic dermatitis. Helpful features include: [1]
- Focal parakeratosis with mounds of scale.
- Spongiosis with small spongiotic vesicles.
- Diminished or absent granular layer.
- Erythrocyte extravasation in the papillary dermis and sometimes epidermis.
- Superficial perivascular lymphohistiocytic infiltrate.
- Eosinophils may be present, particularly in drug-induced cases. [1]
These findings exclude psoriasis, lichen planus, and mycosis fungoides but cannot alone diagnose PR. [1]
[8]
Management
The cornerstone of management is reassurance: PR is self-limiting and benign in the vast majority of patients. [1]
General measures
- Explain the natural history: most lesions resolve within 6–8 weeks, sometimes up to 12 weeks; rarely persistent.
- Emollients and mild cleansers to reduce irritation.
- Avoid hot baths, vigorous rubbing, and irritating topical agents. [1]
Symptomatic therapy
- Pruritus: non-sedating antihistamines; sedating antihistamines at night if sleep disturbance.
- Topical corticosteroids: mild-to-moderate potency for 1–2 weeks to reduce pruritus and erythema.
- Calamine lotion or menthol-containing preparations for symptomatic relief. [1]
Active pharmacological therapy
Reserved for extensive, persistent, or highly symptomatic disease. [1]
| Agent | Evidence | Notes |
|---|---|---|
| Oral acyclovir / valaciclovir | Cochrane review: oral acyclovir may improve rash clearance compared with placebo/no treatment; evidence for itch is inconclusive | Most likely to help if started early; typical adult acyclovir 400 mg five times daily or valaciclovir 1000 mg three times daily for 1–2 weeks |
| Erythromycin | Low-to-moderate quality evidence that erythromycin may reduce pruritus compared with placebo | Adult dose 250–500 mg four times daily for 2 weeks (paediatric 25–50 mg/kg/day in divided doses); less commonly used; GI side effects; avoid in pregnancy unless clearly indicated |
| Emollients / zinc oxide cream | Symptomatic relief; no disease-modifying effect | Liberal application 2–3 times daily, especially after bathing; cheap and well tolerated |
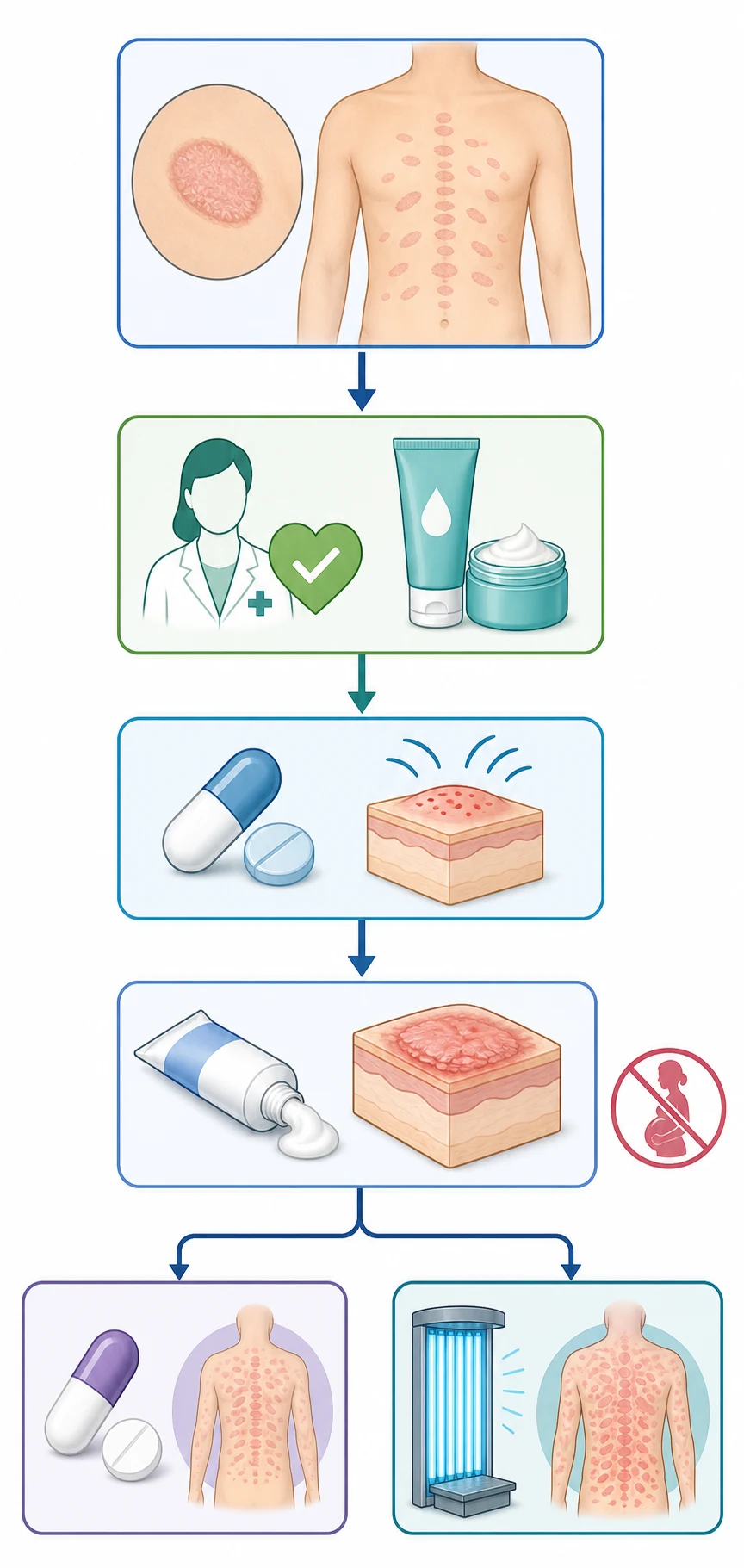
Treatment algorithm
- Mild/classic PR → reassurance + emollients ± antihistamine.
- Moderate pruritus / limited extent → add mild-to-moderate potency topical corticosteroid.
- Extensive, early, or highly symptomatic → consider oral acyclovir/valaciclovir.
- Persistent or refractory → narrowband UVB phototherapy; biopsy if atypical. [1]
Complications, Emergencies & Pitfalls
Pregnancy
Pityriasis rosea in pregnancy is the most important red flag. A landmark series reported: [1]
- Overall preterm delivery rate ~24%.
- Spontaneous abortion rate ~13%.
- Among women with onset before 15 weeks gestation, the spontaneous abortion rate was markedly higher (62 per cent in the landmark Drago series versus 4 per cent with later-onset disease). [1]
Pityriasis rosea in pregnancy — landmark adverse-outcome signals (Drago et al., JAAD 2008)
Subsequent studies have reported lower complication rates, but early gestational onset, widespread rash, constitutional symptoms, and high HHV-6 viral load are considered risk factors for adverse outcomes. Management should include obstetric co-management and targeted fetal surveillance.[7]
Classic pitfalls
- Misdiagnosing the herald patch as tinea corporis — check KOH if scale is atypical; dermoscopy helps.
- Missing secondary syphilis — always consider in atypical cases, palmar/plantar involvement, or high-risk patients.
- Unnecessary extensive work-up in classic PR — the diagnosis is clinical.
- Over-treating self-limiting disease — avoid systemic steroids; they do not alter natural history and may cause rebound.
- Ignoring persistence >3 months — consider biopsy to exclude mycosis fungoides or PR-like drug eruption. [1]
Prognosis & Follow-Up
Pityriasis rosea is self-limiting: [1]
- Most cases resolve within 6–12 weeks without scarring.
- Post-inflammatory hyperpigmentation or hypopigmentation, especially in darker skin types, may persist for weeks to months.
- Recurrence is uncommon. [1]
Follow-up is required when:
- Pregnancy is diagnosed or suspected.
- Rash persists beyond 3 months.
- Atypical morphology or systemic symptoms develop.
- Treatment response is inadequate. [1]
Special Populations
Children
- PR is less common in children under 10 years and rare under 2 years.
- Atypical presentations are more frequent; face and scalp involvement may occur.
- Management is primarily supportive; avoid oral acyclovir unless clearly indicated and weight-based dosing used. [1]
Pregnancy
- Reassurance alone is insufficient; co-manage with obstetrics.
- Emollients and mild topical corticosteroids are generally safe.
- Systemic acyclovir/valaciclovir may be considered after risk–benefit discussion; erythromycin is generally avoided near term.
- Document gestational age at onset and counsel about early-pregnancy risk signal. [1]
Evidence, Guidelines & Regional Differences
Key guideline
- European Academy of Dermatology and Venereology position statement (Chuh et al., 2016) — emphasises reassurance, symptomatic care, and judicious use of acyclovir/erythromycin/phototherapy for selected patients. [1]
Landmark systematic review
- Cochrane review (2019) — evaluated oral acyclovir, erythromycin, and other interventions; concluded acyclovir may improve rash clearance, evidence for itch inconclusive, erythromycin may reduce pruritus. [1]
Regional notes
- In tropical and darker-skinned populations, lesions may appear more violaceous and post-inflammatory pigmentary change may be more prominent.
- Where syphilis prevalence is high, a lower threshold for RPR/VDRL testing is appropriate. [1]
Exam Pearls
[1]Red Flags
Exam application bank (NEET-PG / INICET)
One-line answer
Pityriasis rosea is an acute, self-limiting papulosquamous eruption of probable herpesviral aetiology (HHV-6/7 reactivation), characterised by a herald patch and a secondary eruption in a Christmas-tree distribution. Fellowship-level assessment requires recognition of classic and atypical morphology, validated diagnostic criteria, histopathological and dermoscopic clues, targeted differential diagnosis, evidence-based symptomatic and antiviral therapy, and the pregnancy-adverse-outcome signal.
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard. [1]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes. [1]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change. [1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each. [1]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory. [1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Pityriasis rosea.
Expanded exam teaching (depth pass)
Clinical reasoning
For Pityriasis rosea, examiners test whether you can prioritise life threats, choose the right first test, and give specific therapy (agent, dose, route, timing). Generic phrases without numbers score poorly.
Mechanism → feature map
Build a short chain: cause → pathophysiologic intermediate → clinical feature → complication. Every major symptom in the classic vignette should sit on that chain.
Investigation strategy
- Bedside/first-line tests that change immediate management
- Confirmatory or staging tests
- What a normal result does not exclude
- When not to delay treatment for imaging (unstable patient)
Management ladder
- Resuscitation / ABC / sepsis or haemorrhage bundle as relevant
- Specific antidote / procedure / antimicrobial / reperfusion / surgery
- Supportive care and monitoring targets
- Definitive long-term therapy and secondary prevention
- Disposition and safety-net advice
Special populations
Always prepare one line each for children, pregnancy, elderly, renal/hepatic impairment, and immunocompromised patients when the topic allows.
Pitfalls that fail candidates
- Treating the number not the patient
- Missing pregnancy status when relevant
- Imaging before stabilisation
- Wrong empiric cover or wrong antidote timing
- Incomplete counselling on recurrence, adherence, or red-flag return
Pityriasis rosea is an acute, self-limiting papulosquamous eruption of probable herpesviral aetiology (HHV-6/7 reactivation), characterised by a herald patch and a secondary eruption in a Christmas-tree distribution. Fellowship-level assessment requires recognition of classic and atypical morphology, validated diagnostic criteria, histopathological and dermoscopic clues, targeted differential diagnosis, evidence-based symptomatic and antiviral therapy, and the pregnancy-adverse-outcome signal. [1]
[1]References
- [1]Drago F, Broccolo F, Rebora A, et al. Pityriasis Rosea: A Comprehensive Classification Dermatology, 2016.PMID 27096928
- [2]Drago F, Broccolo F, Rebora A. Pityriasis rosea: an update with a critical appraisal of its possible herpesviral etiology J Am Acad Dermatol, 2009.PMID 19615540
- [3]Aydin Kurc M, Cihan FG. Association between Pityriasis Rosea (PR) and HHV-6/HHV-7 Infection: Importance of Sample Selection and Diagnostic Techniques Diagnostics (Basel), 2024.PMID 38667488
- [4]Chuh AA. Diagnostic criteria for pityriasis rosea: a prospective case control study for assessment of validity J Eur Acad Dermatol Venereol, 2003.PMID 12602987
- [5]Chuh A, Chan H, Zawar V. A position statement on the management of patients with pityriasis rosea J Eur Acad Dermatol Venereol, 2016.PMID 27406919
- [6]Contreras-Ruiz J, Mas-Vidal A, Chi-Veng JC, et al. Interventions for pityriasis rosea Cochrane Database Syst Rev, 2019.PMID 31684696
- [7]Drago F, Broccolo F, Javor S, et al. Pregnancy outcome in patients with pityriasis rosea J Am Acad Dermatol, 2008.PMID 18489054
- [8]Prasad D, Pandhi R, Negi KS. Pityriasis rosea: A histopathologic study Indian J Dermatol Venereol Leprol, 2000.PMID 20877089
- [9]Shende AA, Koley S, Nagpal N. A Cross-Sectional Study of Epidemiological and Clinical Aspects of Pityriasis Rosea along with Dermoscopic Analysis and Histopathology Correlation Indian J Dermatol, 2024.PMID 38841213
- [10]Vasisht S, Kansal NK. Dermoscopic features of pityriasis rosea BMJ Case Rep, 2023.PMID 37816577
- [11]Nwako-Mohamadi MK, Blasum C, Baybay H, et al. Dermoscopic Features of Psoriasis, Lichen Planus, and Pityriasis Rosea in Patients With Skin Type IV and Darker Attending the Regional Dermatology Training Centre in Northern Tanzania Dermatol Pract Concept, 2019.PMID 30775148
- [12]Jairath V, Singal A, Gupta S. Narrowband UVB phototherapy in pityriasis rosea Indian Dermatol Online J, 2015.PMID 26500862
- [13]Litchman G, Le JK. Pityriasis Rosea 2026.PMID 28846360