Dermatology · Medicine
Pityriasis versicolor
Also known as Tinea versicolor · Pityriasis versicolor
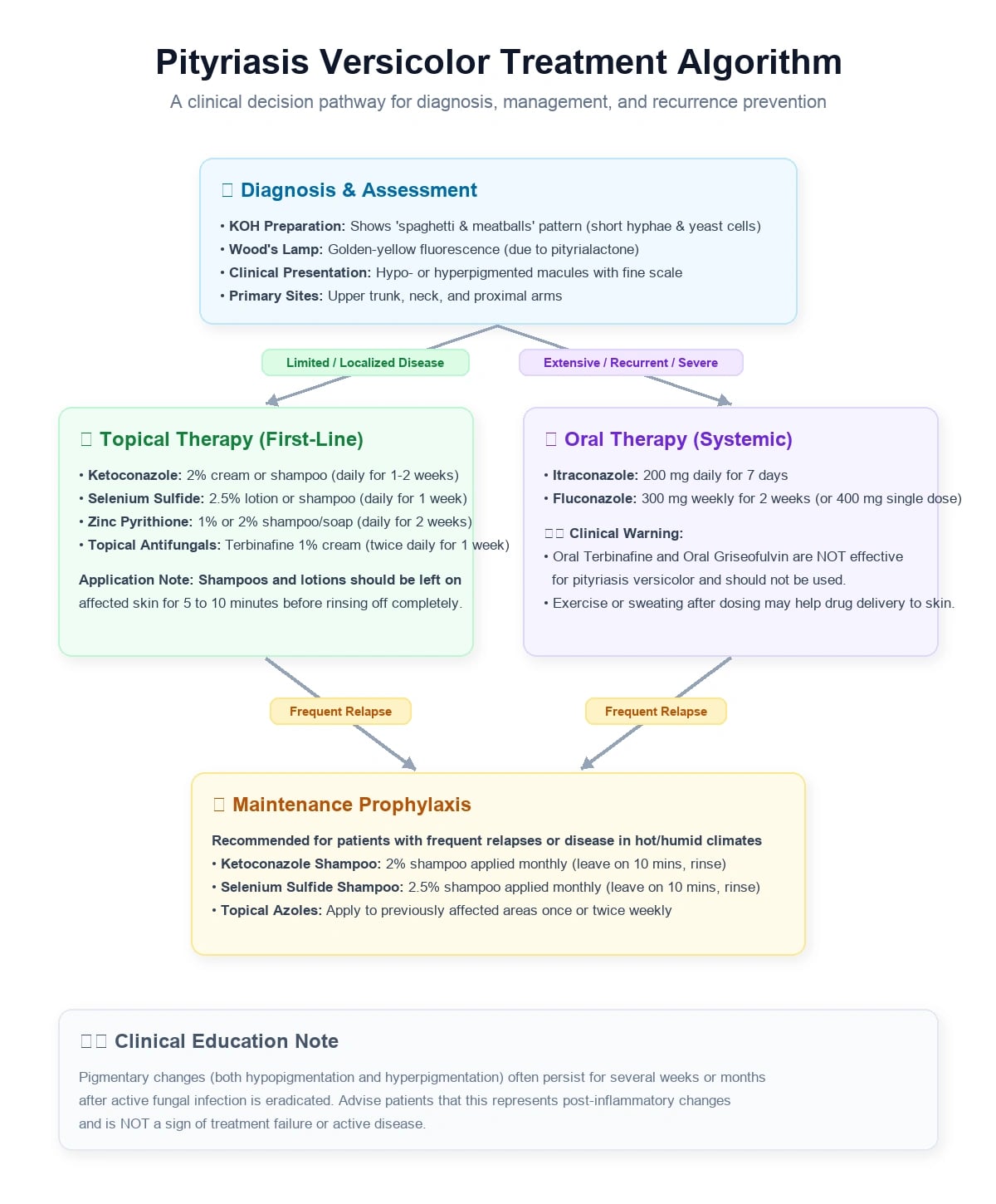
Pityriasis versicolor is a common superficial fungal infection caused by Malassezia yeasts, presenting with scaly hypopigmented or hyperpigmented macules on the trunk and proximal limbs. Fellowship-level assessment requires understanding of the transition from commensal to pathogen, diagnostic techniques (KOH microscopy, Wood's lamp, dermoscopy), first-line topical therapies (ketoconazole, selenium sulfide, zinc pyrithione), systemic options for extensive or recalcitrant disease (itraconazole, fluconazole), and strategies to prevent the high recurrence rate.
On this page & tools
Your progress
Saved locally on this device.
Exam tags
Red flags
Definition & Classification
Pityriasis versicolor (PV), also called tinea versicolor, is a chronic, superficial fungal infection limited to the stratum corneum. It is caused by lipophilic yeasts of the genus Malassezia that are part of the normal human skin flora. Disease represents a switch from the commensal yeast phase to the pathogenic mycelial (hyphal) phase in susceptible hosts.[1][3]
Key nomenclature[1]
- Pityriasis versicolor — preferred dermatology term; "versicolor" refers to variable pigmentation.
- Tinea versicolor — historical term; the organism is a yeast, not a dermatophyte, so "tinea" is a misnomer but remains in common use.
Epidemiology & Risk Factors
PV is one of the most common superficial mycoses worldwide. A 2022 United States commercial insurance analysis of 32,679 cases reported an incidence of 2.8 per 1,000 person-years, with the highest rate in 18–24-year-olds (5.0 per 1,000) and males (3.2 per 1,000).[2]
Prevalence is strongly climate-dependent:[1]
- Tropical and humid regions: up to 40–50% in some populations.
- Temperate regions: approximately 0.5–4%.
Risk factors and triggers[1]
| Factor | Mechanism |
|---|---|
| High temperature and humidity | Promotes yeast overgrowth on sebum-rich skin |
| Hyperhidrosis / occlusive clothing | Creates a favourable microenvironment |
| Oily skin / adolescence | Malassezia requires exogenous lipids |
| Immunosuppression | Impaired control of commensal yeast |
| Cushing syndrome / corticosteroid use | Steroid-induced seborrhoea and immunomodulation |
| Malnutrition and prolonged sweating | Altered cutaneous environment |
Pathophysiology
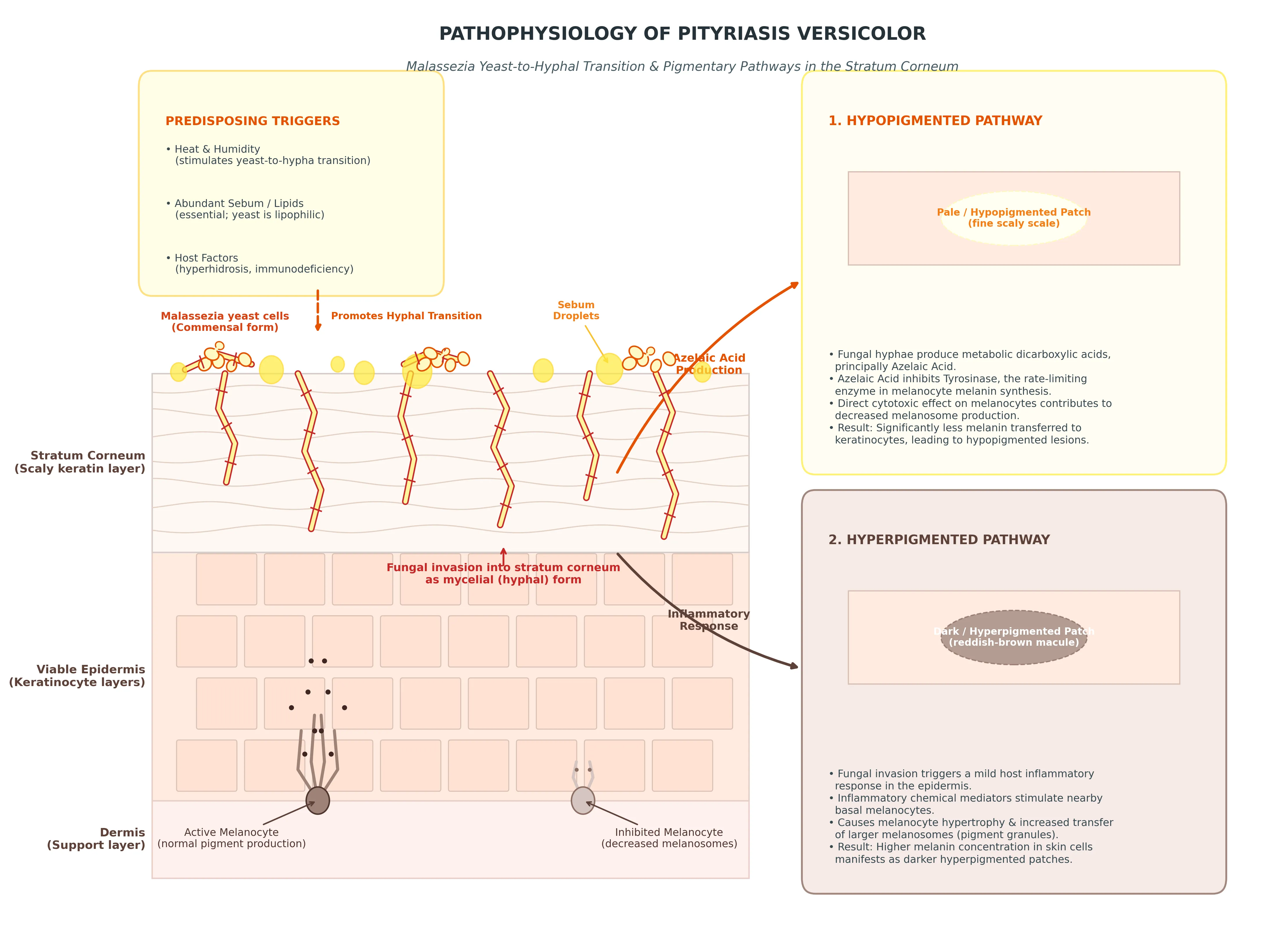
Malassezia species are lipophilic yeasts that colonise human skin shortly after birth. They are obligate lipids and cannot synthesise fatty acids de novo; they rely on sebaceous triglycerides and produce lipases and phospholipases to liberate lipids for growth.[1][3]
From commensal to pathogen
The central event in PV is the conversion of the yeast form to a mycelial form:[3]
- Triggering factors (heat, humidity, seborrhoea, immunosuppression) alter the cutaneous microenvironment.
- Malassezia proliferates and switches to hyphal growth.
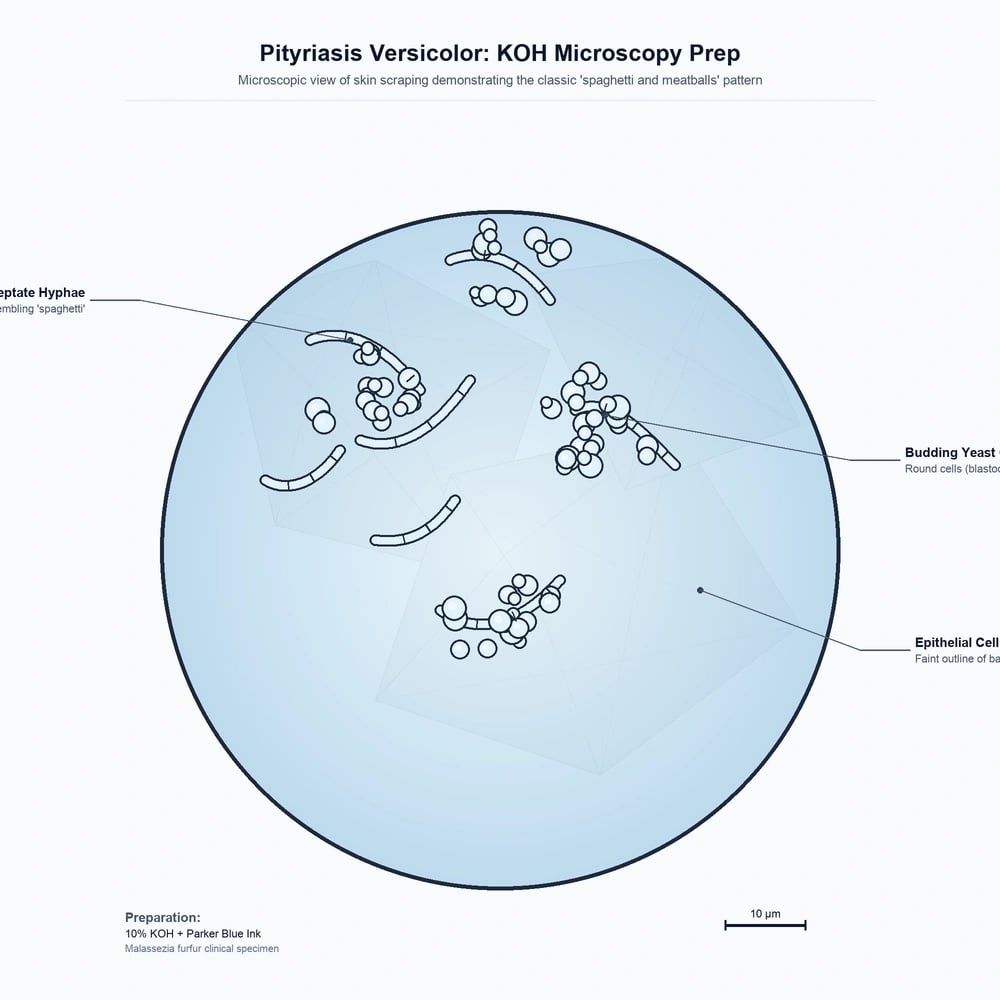
- The mycelial form invades the stratum corneum, producing the clinical lesions and the characteristic "spaghetti and meatballs" appearance on microscopy.
Key species
Molecular studies show geographic variation, but M. globosa is the predominant species isolated from PV lesions in most temperate regions:[4]
| Region | Predominant species | Findings |
|---|---|---|
| Iran (Tehran) | M. globosa | 53.3% of lesions; mycelial form dominant in lesions vs yeast form on healthy skin[4] |
| Greece | M. globosa | 77% alone in PV; pigmented PV correlated with female sex[5] |
| Turkey | M. globosa | 65.1%, followed by M. obtusa 17.4%[6] |
| Northern Iran | M. globosa | 47.6% by PCR-RFLP[7] |
Other implicated species include M. furfur, M. sympodialis, M. obtusa, M. slooffiae, and M. restricta.
[3] [4]Pigmentary change
Both hypopigmentation and hyperpigmentation occur:[1]
- Hypopigmentation is thought to result from yeast metabolites that block melanogenesis and transfer of melanosomes to keratinocytes.
- Hyperpigmentation may reflect inflammation, mild spongiosis, and increased melanosome transfer.
Clinical Presentation
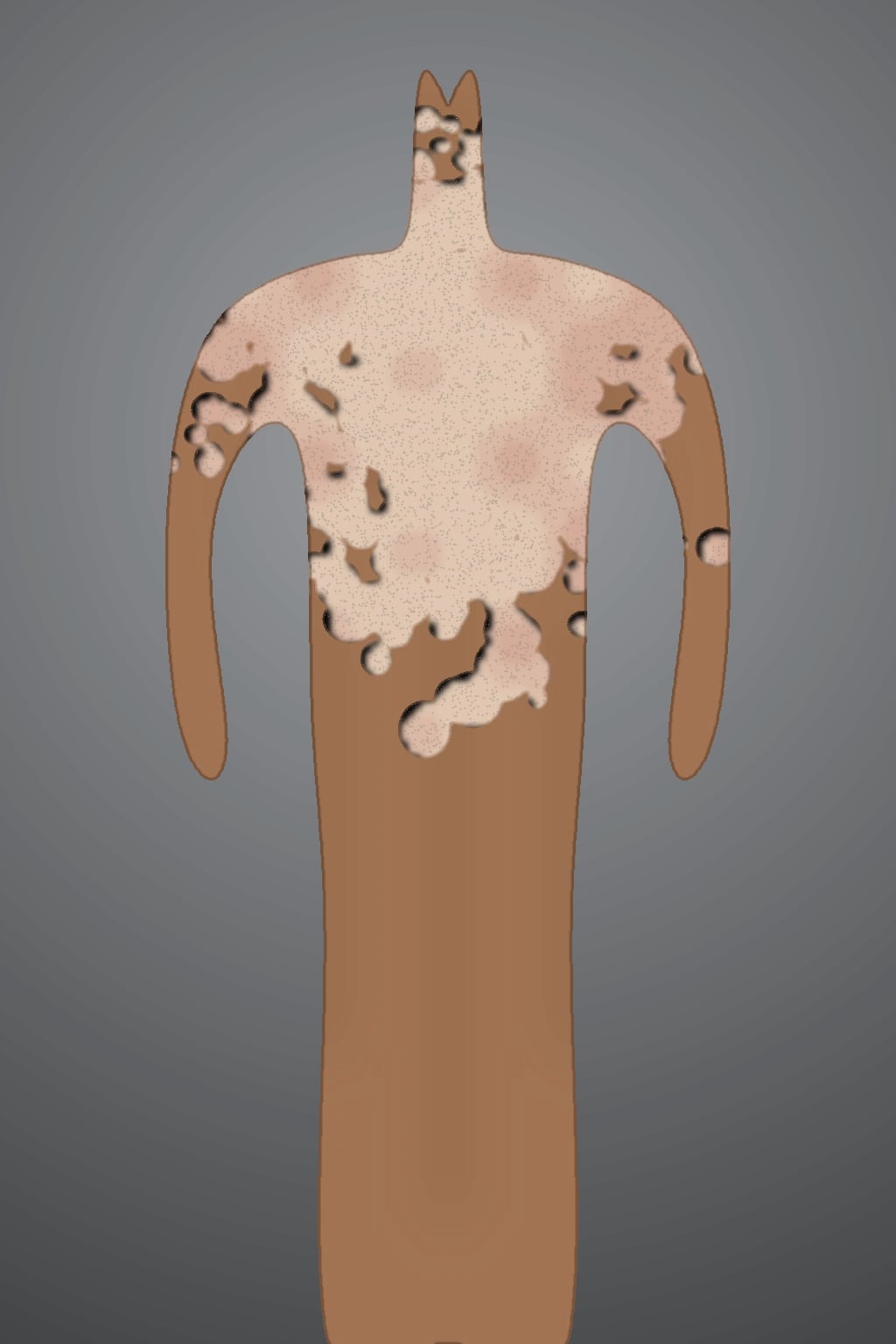
PV classically presents with well-demarcated, finely scaly macules or patches that may be hypopigmented, hyperpigmented, or erythematous. Lesions begin on the upper trunk, neck, shoulders, and proximal arms — the sebum-rich areas — and may coalesce into larger patches with central clearing. Scale is often subtle and best appreciated by gentle scraping (the evoked scale sign).[1]
Clinical variants[1]
| Variant | Features |
|---|---|
| Hypopigmented | Most common, especially in darker skin and children; appears as off-white or light-pink macules |
| Hyperpigmented | Tan, brown, or copper-coloured macules; more common in lighter skin |
| Erythematous / inflammatory | Pink patches with more noticeable scale |
| Atrophic | Rare; associated with dermal elastolysis |
| Follicular | Perifollicular papules or pustules |
| Inverse | Axillary, groin, or inframammary involvement |
Atypical presentations examiners test
- Infants and young children: facial involvement is more common than in adults. A 2025 Chinese observational study of 415 children found that 35.4% were under 6 months old and the face was the most frequently involved site (65.3%); hypopigmented PV accounted for 96.9% of cases.[14]
- Neonatal PV: rare; may relate to close maternal contact or active maternal infection.
- Immunocompromised host: more extensive, recurrent, or treatment-resistant disease.
Differential Diagnosis
[1] [9]Clinical & Bedside Assessment
Key diagnostic signs
| Sign | Finding |
|---|---|
| Evoked scale sign | Fine scale becomes visible when the skin is stretched or gently scraped |
| Spaghetti and meatballs (KOH) | Short hyphae and clusters of yeast cells on microscopy |
| Yellow-green fluorescence (Wood's lamp) | Due to pityrialactone, a tryptophan metabolite of Malassezia |
Wood's lamp examination
Active lesions often show yellow, yellow-green, or coppery-orange fluorescence, attributed to pityrialactone. However, fluorescence is not universal; it may be absent after bathing (water-soluble chromophores wash off) or after recent topical antifungal shampoo use.[8][1]
Dermoscopy
Dermoscopy is increasingly used as a bedside adjunct. Characteristic findings include:[9]
- Fine white scales in skin furrows creating a "wire-fence" or "fish-net" pattern.
- Double-edged scale when the skin is stretched.
- Non-uniform pigmentation in both hypopigmented and hyperpigmented lesions.
- Perifollicular scaling or hypopigmentation.
Investigations
Potassium hydroxide (KOH) microscopy
A 10% KOH mount of skin scrapings is the standard confirmatory test. It reveals the pathognomonic "spaghetti and meatballs" pattern:[1]
- Spaghetti — short, curved hyphae.
- Meatballs — clusters of round or oval yeast cells.[3]
Chicago Sky Blue 6B or other contrast stains can improve visualization. KOH is cheap, rapid, and highly specific when performed correctly.[1]
Culture and molecular testing
Malassezia requires lipid-supplemented media such as modified Dixon's agar and grows slowly. Culture is rarely needed for routine diagnosis but is useful for epidemiological or research purposes. PCR-RFLP of the internal transcribed spacer (ITS) region can accurately speciate isolates.[5][7]
When to investigate further
- Atypical or widespread disease in infants — consider immunodeficiency work-up if recurrent or refractory.
- Treatment failure after two appropriate courses — repeat KOH and consider culture/speciation.
- Suspicion of secondary syphilis, vitiligo, or other mimics — directed serology or biopsy.
Management — Topical Therapy
Topical agents are first-line for limited or moderate disease. A 2024 meta-analysis found no significant difference in clinical cure between topical azole antifungals and keratolytic agents such as selenium sulfide, although the evidence quality was low.[13]
First-line topical options
| Agent | Formulation | Typical regimen | Notes |
|---|---|---|---|
| Ketoconazole | 2% shampoo or cream | Shampoo: apply to affected areas, leave 5–10 min, rinse; daily or twice weekly for 2–4 weeks | Considered a topical gold standard; well tolerated[10] |
| Selenium sulfide | 2.5% shampoo/lotion | Apply to trunk and proximal limbs, leave 10 min, rinse; daily for 1 week then weekly | Can irritate or discolour hair; avoid broken skin[10] |
| Zinc pyrithione | Shampoo or soap | Wash affected areas, leave several minutes, rinse; several times weekly | Useful for mild disease or maintenance[10] |
| Clotrimazole / miconazole | 1–2% cream | Twice daily for 2–4 weeks | Imidazole alternatives |
| Terbinafine | 1% cream/gel | Once or twice daily for 1–2 weeks | Topical allylamine; oral terbinafine is ineffective |
| Ciclopirox olamine | 1% cream/shampoo | Twice daily or as shampoo | Broad antifungal and anti-inflammatory activity |
A small comparative study of 40 patients found 95% clinical cure with 2% ketoconazole shampoo versus 85% with 2.5% selenium sulfide shampoo after three weekly applications, with no statistically significant difference.[16]
Practical application tips
- Apply shampoo or lotion widely from the jawline down, not only to visible lesions, because subclinical colonisation is common.
- Leave the product in contact with the skin for several minutes before rinsing.
- Warn patients that repigmentation may take weeks to months even after mycological cure; persistent colour change is not treatment failure.
Management — Systemic Therapy
Oral azoles are reserved for extensive, recalcitrant, or recurrent disease and for patients unable to apply topical agents reliably. A 2014 systematic review of 57 trials supported evidence-based dosing regimens.[12]
Oral options
Important cautions
- Oral ketoconazole is no longer recommended because of hepatotoxicity risk.
- Oral terbinafine is ineffective for PV.
- Check liver function, drug interactions, and pregnancy status before systemic azoles.
- Avoid systemic therapy in pregnancy; topical agents are preferred.
Management by Special Site or Scenario
Extensive truncal disease
Use a topical shampoo (ketoconazole 2% or selenium sulfide 2.5%) applied to the entire trunk and proximal limbs, left in place for 5–10 minutes, then rinsed. If response is inadequate after 2–4 weeks, add oral itraconazole 200 mg/day for 5–7 days.[1][12]
Facial or infantile PV
- Prefer topical imidazole creams (clotrimazole, ketoconazole cream) because shampoos can irritate facial skin.
- Infantile hypopigmented PV has responded to 1% clotrimazole lotion twice daily for four weeks in reported cases.[15]
Pregnancy and breastfeeding
- Topical azoles and selenium sulfide are generally considered safe.
- Avoid systemic azoles in pregnancy; if essential, specialist advice is required.
Recurrent disease — maintenance prophylaxis
Because Malassezia is a commensal, recurrence is common. Maintenance options include:[3]
- Ketoconazole 2% shampoo or selenium sulfide 2.5% shampoo applied to trunk and proximal limbs for 10 minutes, once or twice monthly.
- Some clinicians use oral itraconazole 200 mg twice daily for one day per month when topical prophylaxis fails.[16]
Evidence for the optimal frequency and duration is limited, but prophylaxis is widely accepted in clinical practice.[1][10]
Malassezia Species, Topical & Systemic Dosing Protocols
This section consolidates the species-level microbiology and the practical dosing schedules examiners are likely to ask about — selenium sulfide 2.5% shampoo, ketoconazole 200 mg daily, and itraconazole pulse therapy.[7]
Malassezia species revisited
Eleven Malassezia species are recognised, of which nine have been isolated from human skin. M. globosa remains the dominant cause of pityriasis versicolor in temperate regions (53–77% of culture-positive lesions across European, Middle-Eastern and Turkish cohorts), while M. furfur is more often recovered in tropical settings and M. sympodialis is the most frequent commensal on healthy adult skin. M. restricta is highly sebaceous and is implicated in seborrhoeic dermatitis and dandruff rather than PV.[3][4][5]
Each species shares a strict dependence on exogenous C12–C24 fatty acids, but they differ in colony morphology, lipid requirement, and melanocyte-interacting metabolites. M. globosa and M. furfur generate azelaic acid and pityrialactone from tryptophan metabolism; azelaic acid competitively inhibits tyrosinase and accounts for much of the hypopigmentation, while pityrialactone is the fluorochrome responsible for the yellow–green Wood's lamp fluorescence.[8][1]
Pityriasis versicolor at a glance — the high-yield numbers
Topical antifungal dosing — specific regimens
For fellowship and board exams the numerator-and-denominator of topical doses must be memorised. The following protocols are drawn from the systematic review of 93 trials (Hu & Bigby 2010) and the 2024 meta-analysis of synthetic antifungals versus keratolytics.[11][13]
- Dose: 2.5% lotion or shampoo, apply to **entire trunk, neck and proximal limbs** (not only visible lesions)
- Contact time: **5–10 minutes** before rinsing; insufficient contact time is the commonest cause of treatment failure
- Frequency: **daily for 7 days**, then **weekly** for maintenance, OR **twice weekly for 2–4 weeks**
- Adverse effects: xerosis, irritant dermatitis, transient hair discolouration (especially in bleached or light hair); avoid within 48 h of facial peel/wax
- Evidence: ~85% clinical cure vs 95% with ketoconazole 2% in the only direct comparison trial (Aggarwal 2003)
- Dose: 2% shampoo — same wide-area application from the jawline down; 5–10 minutes contact time
- Frequency: **once daily for 5 days**, or **twice weekly for 2–4 weeks**; a single application has lower mycological cure
- Alternative: 2% cream twice daily for **2–4 weeks** for focal or facial lesions
- Paediatric face: 1% clotrimazole lotion BD for 4 weeks is the cited regimen for infantile hypopigmented PV
- Evidence: topical gold standard; included in the Cochrane-aligned review of 93 trials as one of the highest-cure agents
- Dose: 1% shampoo or bar soap, lather widely, contact **3–5 minutes**
- Frequency: **daily for 2 weeks** then 1–2 times weekly; ideal for very mild disease or maintenance
- Adverse effects: well tolerated; rare contact dermatitis; no staining unlike selenium sulfide
- Evidence: comparable mycological cure to azole shampoos in small trials; favoured by patients who dislike selenium sulfide odour
- **Ciclopirox 1%** cream or shampoo — broad antifungal and anti-inflammatory; apply BD for 2–4 weeks
- **Terbinafine 1%** cream/gel — once or twice daily for 1–2 weeks; topical only — oral is INACTIVE against Malassezia
- **Clotrimazole 1% / miconazole 2%** cream — BD for 2–4 weeks for focal/facial disease
- **Sulfur–salicylic acid** combinations — historical keratolytic option; useful when imidazoles are not tolerated
Systemic dosing — itraconazole and fluconazole
Oral azoles are reserved for extensive (more than 20% body surface), recalcitrant, or frequently relapsing disease. The 2014 systematic review of 57 trials established evidence-based dosing regimens.[12]
Itraconazole pulse therapy — preferred oral regimen. The "200 mg daily × 7 days" or "400 mg/day × 2 days once monthly" regimen exploits the drug's keratinophilic concentration and lipophilic reservoir in the stratum corneum. In documented trials the 7-day 200 mg/day regimen achieves ~75–85% mycological cure at week 12; the 2-day pulse (400 mg/day on days 1 and 2 of each month, repeated once or twice) achieves comparable cure with lower cumulative dose and is often used as long-term suppressive prophylaxis. Take with an acidic beverage (cola, not water) to maximise absorption, and avoid in patients with congestive heart failure.[10][12]
Oral ketoconazole is no longer recommended for PV — the FDA-EMA hepatotoxicity warning (2013–2014) and adrenal-insufficiency signal precipitated its withdrawal from first-line use. Oral terbinafine does not work for Malassezia because the fungus does not synthesise ergosterol by the squalene-epoxidase-dependent pathway in sufficient quantity to be drug-sensitive.[10][12]
Fluconazole 300 mg once weekly for 2 weeks is the alternative oral azole; achievable cure rates 70–80%. Randomised data suggest itraconazole pulse is marginally more effective than weekly fluconazole, but fluconazole has fewer drug interactions and a more favourable cardiac safety profile.[12]
- **Pulse-1: 200 mg BD on day 1 (or 200 mg/day × 7 days)** — for active disease
- **Pulse-2: 400 mg/day × 2 consecutive days each month** — prophylactic suppression
- Take with cola / acid; high-fat meal; check LFTs and drug interactions (CYP3A4)
- Avoid in HFrEF, pregnancy, and with statins, dofetilide or quinidine
- Mycological cure 75–85% at week 12 in trials
- **300 mg PO once weekly for 2 weeks** (range 200–400 mg)
- Long half-life; tissue-persistent; mild GI side effects; rare hepatotoxicity
- Fewer CYP3A4 interactions than itraconazole; safer with statins
- Cure rate 70–80% in randomised trials; useful when itraconazole contraindicated
- Continue maintenance prophylaxis (same dose monthly) in frequent relapsers
- Ketoconazole 2% OR selenium sulfide 2.5% OR zinc pyrithione 1% shampoo
- Apply widely; leave on 5–10 min; rinse; daily × 5–7 days then weekly
- Reserve systemic therapy for **>20% BSA**, recalcitrant, or recurrent disease
Malassezia species — extended taxonomy and clinical correlations
A working knowledge of Malassezia species is high-yield for fellowship exams because the species differ in lipid requirement, colony morphology, pathogenicity, and response to antifungals. The genus was revised by Gueho and colleagues in 1996 (seven species) and has since expanded; current taxonomy recognises eleven species, of which nine have been isolated from human skin — M. furfur, M. globosa, M. sympodialis, M. restricta, M. slooffiae, M. obtusa, M. japonica, M. dermatis, and M. yamatoensis. Two non-human-associated species, M. nana and M. equina, complete the genus but are not relevant to PV.[3][4]
Lipid dependence. All human-pathogenic Malassezia are obligate lipophiles — they cannot synthesise C12–C24 fatty acids de novo and require an exogenous source. This is why they colonise sebum-rich sites (face, scalp, upper trunk) only after puberty, when sebaceous glands become active, and why neonatal PV is uncommon but can occur via maternal contact. M. furfur and M. sympodialis are the most lipid-tolerant and grow on routine mycological media if supplemented with olive oil; M. restricta and M. globosa are fastidious and grow only on lipid-enriched media such as modified Dixon's agar, Leeming-Notman agar, or Dixon's broth at 32–35 °C for 5–14 days.[1][3]
Species-level pathogenesis. Although all Malassezia species can produce pityriasis versicolor under the right host conditions, M. globosa is the predominant isolate in temperate-zone PV (53–77% of culture-positive lesions in Iranian, Greek, Turkish and Northern Iranian cohorts), and its mycelial form is found almost exclusively in lesional skin while the yeast form dominates on healthy skin of the same patient — confirming the pathogenic switch from yeast to hyphal morphology.[4][5][6][7] M. furfur is more often recovered in tropical settings and from patients with hyperpigmented PV. M. sympodialis is the commonest commensal on healthy adult skin but is implicated less often in PV. M. restricta is highly sebaceous and is implicated more in seborrhoeic dermatitis and dandruff than in PV.[5][3]
Mechanism of pigmentary change. M. globosa and M. furfur elaborate azelaic acid (a C9 dicarboxylic acid) through peroxisomal beta-oxidation of sebum-derived oleic acid. Azelaic acid is a competitive inhibitor of tyrosinase and impairs melanosome transfer to keratinocytes, producing the characteristic hypopigmentation. The same tryptophan pathway generates pityrialactone, the indole fluorochrome responsible for the yellow–green Wood's lamp fluorescence that is so useful at the bedside. Hyperpigmented variants reflect inflammation and increased melanin transfer rather than a different metabolic pathway.[8][1]
Practical implications. Because species distribution varies geographically and recurrence is driven by the commensal reservoir, culture and speciation are not routine — but they should be considered in recalcitrant, recurrent, or extensively hyperpigmented disease where resistance or species-specific drug tolerance is suspected. PCR-RFLP of the internal transcribed spacer (ITS) region or ITS-1 / ITS-2 sequencing is the gold standard for species identification; matrix-assisted laser desorption/ionisation time-of-flight (MALDI-TOF) mass spectrometry is increasingly used in reference mycology labs.[5][7]
Reference dosing protocols — exact numbers examiners ask for
The following are the precise, exam-tested doses and protocols that should be memorised verbatim. They are drawn from the 2010 Cochrane-aligned review (Hu & Bigby), the 2014 systematic review of systemic therapy (Gupta, Lane & Paquet), and the 2024 meta-analysis of synthetic antifungals vs keratolytics (Genuino et al.).[11][12][13]
Selenium sulfide 2.5% shampoo. Apply the 2.5% lotion or shampoo to the entire trunk, neck, shoulders, and proximal limbs (not only visible lesions — subclinical carriage is the rule, not the exception). Lather and leave in contact with the skin for 5–10 minutes before rinsing; this contact time is the single most common reason for treatment failure. Standard regimens are daily application for 7 consecutive days for induction, followed by weekly application for maintenance prophylaxis; an alternative induction regimen is twice weekly for 2–4 weeks. Adverse effects include xerosis, irritant contact dermatitis, and transient orange-brown staining of hair (more conspicuous in bleached or naturally light hair) and of jewellery; the shampoo should not be applied within 48 hours of a facial peel or wax. Selenium sulfide is fungistatic via disruption of fungal cell-wall thiol groups and is keratolytic, which adds mechanical scale removal.[10][11][16]
Ketoconazole 200 mg daily (oral). Although topical ketoconazole is the topical gold standard, oral ketoconazole is no longer recommended for any superficial mycosis including pityriasis versicolor — the FDA-EMA hepatotoxicity warnings of 2013–2014 and the adrenal-insufficiency signal led to its withdrawal from first-line systemic use worldwide. The historical adult dose was 200 mg orally once daily, typically for 5–7 days, sometimes extended to 14 days for recalcitrant disease; the drug inhibits CYP-mediated 14-α-demethylation of lanosterol, blocking ergosterol synthesis. Modern practice substitutes itraconazole or fluconazole whenever systemic therapy is needed, and topical ketoconazole 2% (shampoo or cream) remains the preferred topical agent.[10][12]
Itraconazole pulse therapy — 200 mg BD for one week, monthly. This is the preferred systemic regimen for extensive or recalcitrant PV. The most widely used induction schedule is itraconazole 200 mg orally twice daily (BD) for 7 days, taken with an acidic beverage (cola, not water) and a high-fat meal to maximise absorption. For frequent relapsers, the same 200 mg BD × 7 days course is repeated once per month as suppressive prophylaxis, exploiting the drug's keratinophilic concentration and lipophilic reservoir in the stratum corneum — Malassezia remains exposed for weeks after plasma levels fall. Mycological cure rates of 75–85% at week 12 are documented across the systematic-review base. Pre-treatment checks: liver function tests (LFTs), drug interactions (CYP3A4 — avoid with statins, dofetilide, quinidine), pregnancy test, and a cardiac history (avoid in HFrEF because of negative inotropic effect).[10][12]
Fluconazole 300 mg weekly. A practical alternative when itraconazole is contraindicated, when drug interactions are a concern, or when monthly monitoring is difficult. The standard regimen is fluconazole 300 mg orally once weekly for 2 weeks (range 200–400 mg per dose); the long plasma half-life (~30 hours) and tissue-persistent distribution maintain antifungal concentrations in the stratum corneum between doses. Cure rates of 70–80% are documented; for frequent relapsers the same dose may be repeated monthly as suppressive prophylaxis. Fluconazole has fewer CYP3A4 interactions than itraconazole, a more favourable cardiac safety profile, and is generally better tolerated, but hepatotoxicity and rare Stevens-Johnson syndrome are reported. Pregnancy is a contraindication.[12]
Ciclopirox 1% shampoo. An underused but evidence-supported alternative when azoles or selenium sulfide are not tolerated. Ciclopirox 1% is a broad-spectrum hydroxypyridone with both antifungal and anti-inflammatory activity; the shampoo formulation is applied to affected areas, lathered, left in contact for 3–5 minutes, then rinsed — typically twice weekly for 2–4 weeks, with optional weekly maintenance. It inhibits fungal metal-dependent enzymes (cytochrome P450, catalase, peroxidase) and has activity against both yeast and mycelial phases of Malassezia. It is safe in pregnancy and well tolerated in children, making it a useful second-line topical option. Ciclopirox 1% cream or lotion applied twice daily for 2–4 weeks is the corresponding leave-on formulation.[10][11]
High-yield dosing numbers for board exams
Quick-reference dosing summary table
| Drug | Strength | Dose | Duration | Notes |
|---|---|---|---|---|
| Selenium sulfide shampoo / lotion | 2.5% | Apply widely, 5–10 min contact | Daily × 7 days, then weekly; OR twice weekly × 2–4 weeks | Avoid within 48 h of facial peel/wax |
| Ketoconazole shampoo | 2% | Apply widely, 5–10 min contact | Daily × 5 days; OR twice weekly × 2–4 weeks | Topical gold standard |
| Ketoconazole cream | 2% | Twice daily, focal lesions | 2–4 weeks | Useful for facial / focal disease |
| Ciclopirox shampoo | 1% | Apply widely, 3–5 min contact | Twice weekly × 2–4 weeks, then weekly | Safe in pregnancy; anti-inflammatory |
| Ciclopirox cream / lotion | 1% | Twice daily | 2–4 weeks | Second-line topical option |
| Itraconazole (systemic) | 200 mg cap | 200 mg BD × 7 days, repeat monthly if needed | 7-day course; monthly prophylaxis | With cola, high-fat meal; check LFTs, CYP3A4 |
| Fluconazole (systemic) | 150 mg cap | 300 mg (two 150 mg caps) once weekly | 2 weeks; optional monthly | Fewer interactions than itraconazole |
Complications, Emergencies & Pitfalls
Classic pitfalls
- Misdiagnosing PV as vitiligo — PV lesions are scaly and show incomplete, not complete, depigmentation; KOH is diagnostic.
- Stopping therapy because colour has not normalised — repigmentation lags behind mycological cure by weeks to months.
- Using oral terbinafine — it is ineffective for Malassezia.
- Prescribing oral ketoconazole — avoid because of hepatotoxicity.
- Treating only visible lesions — subclinical carriage leads to early relapse; treat a wide area.
When to escalate
- Diagnostic uncertainty or atypical morphology — biopsy or refer to dermatology.
- Recurrent episodes despite appropriate therapy — consider maintenance prophylaxis, culture/speciation, or immunodeficiency screening.
- Severe contact dermatitis to topical agents — switch drug class or formulation.
Prognosis & Follow-Up
PV is benign but frequently recurrent. With appropriate therapy, mycological cure is achieved in the majority of patients, but relapse is common in warm, humid climates or in those with ongoing risk factors. Follow-up should confirm:[12]
- Mycological clearance — repeat KOH if lesions persist after 4 weeks.
- Pigmentary recovery — reassure patients that colour may take 1–3 months (sometimes longer) to return.
- Prevention strategy — offer maintenance shampoo to patients with two or more episodes per year.
Special Populations
Children and infants
- PV is increasingly recognised in infants; in a recent cohort, the under-6-month age group was the largest and facial involvement predominated.
- Use gentle topical imidazoles; systemic therapy is rarely needed.
Immunocompromised patients
- HIV, transplant recipients, and patients on systemic corticosteroids or biologics may have more extensive or refractory disease.
- Treat more aggressively and consider oral azoles, with specialist input.
Pregnancy
- Limit treatment to topical agents.
- Avoid oral azoles unless absolutely necessary.
Evidence, Guidelines & Regional Differences
Major reviews
- Gupta & Foley (2015) — systematic review concluding topical antifungals are first-line and oral terbinafine and ketoconazole should be avoided.[10]
- Hu & Bigby (2010) — Cochrane-aligned systematic review and meta-analysis of 93 trials; most topical and systemic agents are effective versus placebo, but trial quality is generally low.[11]
- Gupta, Lane & Paquet (2014) — evidence-based systemic dosing: itraconazole 200 mg/day for 5–7 days, fluconazole 300 mg weekly for 2 weeks.[12]
- Genuino et al. (2024) — meta-analysis showing no significant difference between topical azoles and keratolytic agents for clinical cure.[13]
Regional notes
- M. globosa predominates in European, Middle Eastern, and Turkish cohorts, but species distribution varies; local microbiology may influence treatment response in refractory cases.
- Tropical regions see higher prevalence and more frequent recurrence, influencing the greater use of maintenance prophylaxis.
Exam Pearls
[16]Red Flags
Exam application bank (NEET-PG / INICET)
One-line answer
Pityriasis versicolor is a common superficial fungal infection caused by Malassezia yeasts, presenting with scaly hypopigmented or hyperpigmented macules on the trunk and proximal limbs. Fellowship-level assessment requires understanding of the transition from commensal to pathogen, diagnostic techniques (KOH microscopy, Wood's lamp, dermoscopy), first-line topical therapies (ketoconazole, selenium sulfide, zinc pyrithione), systemic options for extensive or recalcitrant disease (itraconazole, fluconazole), and strategies to prevent the high recurrence rate.
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard.[12]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes.[1]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change.[14]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each.[1]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory.[1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Pityriasis versicolor.
[13]References
- [1]Łabędź N, Navarrete-Dechent C, Kubisiak-Rzepczyk H, Bowszyc-Dmochowska M, Pogorzelska-Antkowiak A, Pietkiewicz P. Pityriasis Versicolor-A Narrative Review on the Diagnosis and Management. Life (Basel), 2023.PMID 37895478
- [2]Gold JAW, Benedict K, Lipner SR. Pityriasis versicolor epidemiology, disease predictors, and health care utilization: Analysis of 32,679 cases in a large commercial insurance database. Journal of the American Academy of Dermatology, 2025.PMID 39389424
- [3]Crespo-Erchiga V, Delgado Florencio V. Malassezia yeasts and pityriasis versicolor. Current Opinion in Infectious Diseases, 2006.PMID 16514338
- [4]Tarazooie B, Kordbacheh P, Zaini F, Zomorodian K, Saadat F, Zeraati H, Hallaji Z, Rezaie S. Study of the distribution of Malassezia species in patients with pityriasis versicolor and healthy individuals in Tehran, Iran. BMC Dermatology, 2004.PMID 15119958
- [5]Gaitanis G, Velegraki A, Alexopoulos EC, Chasapi V, Tsigonia A, Katsambas A. Distribution of Malassezia species in pityriasis versicolor and seborrhoeic dermatitis in Greece. Typing of the major pityriasis versicolor isolate M. globosa. The British Journal of Dermatology, 2006.PMID 16634886
- [6]Rodoplu G, Saracli MA, Gümral R, Taner Yildiran S. Distribution of Malassezia species in patients with pityriasis versicolor in Turkey. Journal de Mycologie Médicale, 2014.PMID 24746716
- [7]Shokohi T, Afshar P, Barzgar A. Distribution of Malassezia species in patients with pityriasis versicolor in Northern Iran. Indian Journal of Medical Microbiology, 2009.PMID 19736400
- [8]Mayser P, Stapelkamp H, Krämer HJ, Podobinska M, Wallbott W, Irlinger B, Steglich W. Pityrialactone- a new fluorochrome from the tryptophan metabolism of Malassezia furfur. Antonie van Leeuwenhoek, 2003.PMID 14574113
- [9]Thomas N, Malakar S. Dermoscopy: An easy way to solve the diagnostic puzzle in pityriasis versicolor. Indian Journal of Dermatology, Venereology and Leprology, 2019.PMID 30117461
- [10]Gupta AK, Foley KA. Antifungal Treatment for Pityriasis Versicolor. Journal of Fungi (Basel), 2015.PMID 29376896
- [11]Hu SW, Bigby M. Pityriasis versicolor: a systematic review of interventions. Archives of Dermatology, 2010.PMID 20956647
- [12]Gupta AK, Lane D, Paquet M. Systematic review of systemic treatments for tinea versicolor and evidence-based dosing regimen recommendations. Journal of Cutaneous Medicine and Surgery, 2014.PMID 24636433
- [13]Genuino RNF, Dofitas BL, Batac MCFR, Pascual MBTG, Abrilla AA. Systematic Review and Meta-analysis on Synthetic Antifungal versus Keratolytic Agents for Topical Treatment of Pityriasis Versicolor. Acta Medica Philippina, 2024.PMID 38939846
- [14]Luo Z, Li X, Zhou Z, Shi J, Chen H, Wang Y, Xu L, Liang H. Pityriasis versicolor in the paediatric age group: a descriptive observational study of 415 children. Archives of Dermatological Research, 2025.PMID 40397164
- [15]Abdollahimajd F, Niknezhad N, Niknejad N, Nikvar M. Infantile hypopigmented pityriasis versicolor: two uncommon cases. Turkish Pediatrics Archive, 2019.PMID 31949421
- [16]Aggarwal K, Jain VK, Sangwan S. Comparative study of ketoconazole versus selenium sulphide shampoo in pityriasis versicolor. Indian Journal of Dermatology, Venereology and Leprology, 2003.PMID 17642841