Dermatology · Medicine
Skin cancer staging and management algorithms
Also known as AJCC skin cancer staging · Melanoma staging · Cutaneous SCC staging · BWH staging · Skin cancer management algorithm
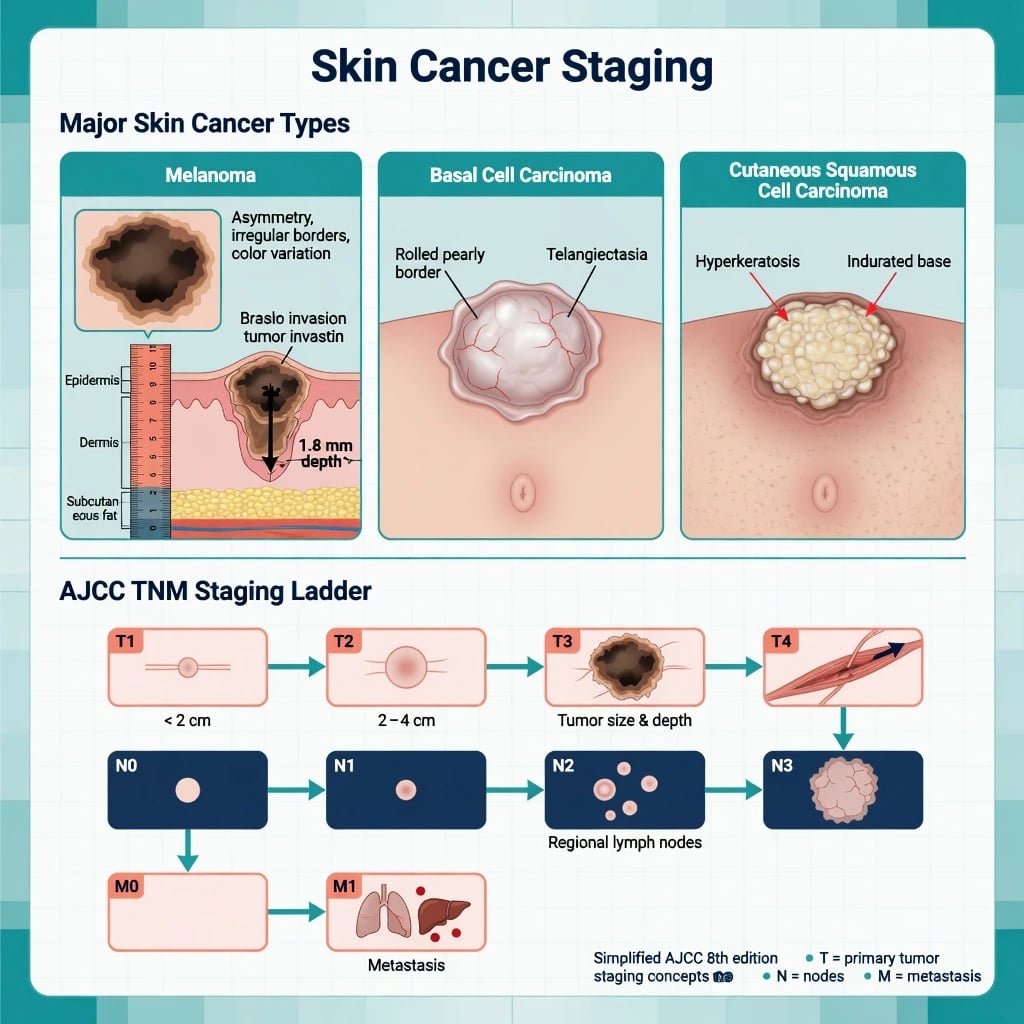
Board-level synthesis of how cutaneous melanoma, cutaneous squamous cell carcinoma (cSCC) and basal cell carcinoma (BCC) are staged or risk-stratified and then managed. Melanoma uses AJCC 8th edition TNM driven by Breslow thickness and ulceration; cSCC uses AJCC 8th T categories plus Brigham and Women's Hospital (BWH) high-risk factor counting; BCC is risk-stratified (NCCN/AAD) rather than routinely TNM-staged when localised. Algorithms cover biopsy technique, wide local excision margins, Mohs micrographic surgery, sentinel lymph node biopsy, adjuvant and systemic options (PD-1, BRAF/MEK, cemiplimab, Hedgehog inhibitors).
On this page & tools
Your progress
Saved locally on this device.
Exam tags
Red flags
Definition & Scope
Staging assigns anatomic extent so that prognosis, imaging, surgery and systemic therapy can be standardised. For cutaneous disease the three high-volume pathways are:[1][5][9]
| Tumour | Staging / risk system | Dominant drivers |
|---|---|---|
| Melanoma | AJCC 8th TNM | Breslow thickness, ulceration, SLN/regional nodes, distant sites, LDH |
| cSCC | AJCC 8th T (+ N/M); BWH alternative T | Diameter, depth, differentiation, PNI, bone, host immunosuppression, site |
| BCC | Risk strata (NCCN/AAD/EuroGuiDerm), not routine TNM if localised | H-zone, size, aggressive histology, recurrence, ill-defined borders, immunosuppression |
Rare entities (Merkel cell carcinoma, cutaneous lymphomas) use separate systems and are not covered in depth here. [1]
Why Algorithms Matter in Exams and Clinics
Examiners test whether you (1) choose the correct biopsy, (2) read the pathology elements that change stage, (3) apply margins / Mohs / SLNB thresholds, and (4) know when systemic therapy enters the pathway. Mixing melanoma rules into NMSC (or vice versa) is a classic fail point.[2][6]
Melanoma — AJCC 8th Edition

T category (primary tumour)
Breslow thickness is measured from the granular layer (or base of ulcer) to the deepest invasive melanoma cell.[1][2]
| T | Definition (core teaching thresholds) |
|---|---|
| Tis | Melanoma in situ |
| T1a | less than 0.8 mm, no ulceration |
| T1b | 0.8–1.0 mm or ulcerated less than 1.0 mm |
| T2 | 1.01–2.0 mm (a/b by ulceration) |
| T3 | 2.01–4.0 mm (a/b) |
| T4 | greater than 4.0 mm (a/b) |
Ulceration (full-thickness epidermal loss over tumour, not pure traumatic artefact) defines the b subcategory and worsens prognosis at a given thickness.[1]
N and M categories (high-yield)
- N: clinically occult (SLN) vs clinically detected nodes; number of nodes; in-transit / satellite / microsatellite disease modifies N.[1]
- M: distant skin/soft tissue/nodes vs lung vs other visceral; LDH elevates M subcategory and prognosis discussions.[1][3]
Melanoma management algorithm (stage-linked)
- Biopsy — full-thickness excisional biopsy with narrow clinical margins (about 1–3 mm) preferred so Breslow is measurable; avoid incomplete superficial shaves when melanoma is likely.[2][3]
- Wide local excision (WLE) — guideline-level clinical margins commonly taught as: in situ ~5 mm; ≤1.0 mm → 1 cm; 1.01–2 mm → 1–2 cm; 2.01–4 mm → 1–2 cm; greater than 4 mm → 2 cm (exact institutional protocols may refine intermediate categories).[3]
- SLNB — discuss for ≥T1b (and selected thinner lesions with adverse features) for staging and adjuvant eligibility.[1][3]
- Positive SLN — MSLT-II: completion lymph-node dissection vs nodal observation with ultrasound surveillance — observation is acceptable for many; CLND is not mandatory solely because SLN is positive.[4]
- Adjuvant / systemic — anti-PD-1 (and BRAF+MEK if BRAF V600) for appropriate resected high-risk stage II–III and for unresectable/metastatic disease in specialist care.[3]
Cutaneous SCC — AJCC 8th and BWH

High-risk clinicopathologic features
European and AAD guidance emphasise depth, diameter, poor differentiation, perineural invasion, high-risk sites (ear, lip, temple), recurrence, and immunosuppression as drivers of poor outcome.[5][6]
BWH alternative staging (exam favourite)
BWH counts high-risk factors (commonly taught set): diameter greater than 2 cm, poor differentiation, PNI ≥0.1 mm, invasion beyond subcutaneous fat; categories rise from T1 (0 factors) through T2a (1), T2b (2–3), to T3 (≥4 or bone invasion).[7][8] T2b/T3 tumours carry substantially higher nodal metastatic risk and should trigger nodal examination ± imaging and MDT discussion, with SLNB considered in selected high-risk cases rather than routine for all cSCC.[12]
Local therapy
- Low-risk primary cSCC: standard excision with adequate clinical margins (commonly taught ~4–6 mm depending on risk) or destructive modalities in carefully selected low-risk lesions.[6]
- High-risk / H-zone / recurrent / poorly defined: Mohs or other complete margin-control techniques when available; adjuvant radiotherapy for selected high-risk features after multidisciplinary review.[6][5]
Advanced cSCC
Unresectable or metastatic cSCC may respond to PD-1 blockade (cemiplimab) — a landmark systemic option changing the algorithm beyond pure surgery/radiotherapy.[11]
Basal Cell Carcinoma — Risk Stratification
Localised BCC almost never needs full TNM staging; decisions hinge on low-risk vs high-risk features:[9][10]
| Low-risk (typical) | High-risk (typical) |
|---|---|
| Primary nodular/superficial | Morpheaform, infiltrative, micronodular, basosquamous |
| Trunk/limb, smaller size | H-zone face, large size thresholds |
| Well-defined borders | Ill-defined, recurrent, prior RT field |
| Immunocompetent | Immunosuppression |
High-risk → Mohs / specialist excision; selected low-risk superficial → excision, imiquimod, 5-FU, or PDT per guidelines; locally advanced / metastatic BCC → Hedgehog pathway inhibitors (vismodegib, sonidegib) ± multidisciplinary care.[9][10]
Melanoma pathway
- Excisional biopsy first
- AJCC 8 Breslow + ulceration
- WLE margins by thickness
- SLNB ≥T1b discussion
- MSLT-II observation option if SLN+
- PD-1 / BRAF+MEK by stage & mutation
NMSC pathway (cSCC/BCC)
- Diagnostic punch/shave often OK
- cSCC: AJCC + BWH risk factors
- BCC: risk strata not routine TNM
- Mohs for high-risk H-zone
- Nodal work-up for high-risk cSCC
- Cemiplimab (advanced cSCC); SMO inhibitors (advanced BCC)
Unified Management Algorithm

Practical sequence
- Suspect — morphology + dermoscopy; full skin and nodal exam.
- Biopsy correctly — excisional for melanoma; adequate sample for NMSC subtype and high-risk features.
- Read the report — Breslow/ulceration (melanoma); differentiation, depth, PNI, margins (cSCC/BCC).
- Assign stage/risk — AJCC ± BWH ± BCC risk table.
- Local control — WLE margins or Mohs; document clear margins.
- Regional — SLNB / imaging / MDT when thresholds met.
- Adjuvant/systemic — oncology pathways for advanced or high-risk resected disease.
- Surveillance — stage-based skin and nodal follow-up; counsel on UV protection and second primaries.
Investigations Beyond the Skin
| Scenario | Consider |
|---|---|
| Melanoma ≥ stage III or symptomatic | Cross-sectional imaging / PET-CT per protocol; MRI brain if neurological symptoms |
| High-risk cSCC (BWH T2b/T3, clinical nodes) | Regional node US/CT; discuss SLNB in selected cases |
| Locally advanced BCC | CT/MRI for bone/orbit/perineural pathways |
| Planned immunotherapy / targeted therapy | Baseline organ function, infection screen, BRAF (melanoma) |
Pitfalls That Change Stage or Outcome
- Wrong biopsy understages melanoma Breslow.[2]
- Ignoring H-zone + aggressive BCC histology → high recurrence after narrow excision.[9]
- Treating all cSCC as low risk — missed PNI/depth/immunosuppression.[7]
- Automatic CLND for every positive SLN without applying MSLT-II era observation principles.[4]
- Delayed systemic referral for unresectable cSCC or metastatic melanoma.[11][3]
Special Populations
- Transplant / chronic immunosuppression — accelerated cSCC biology; shorter surveillance intervals; lower threshold for imaging and aggressive local control.[5]
- Elderly frail — balance Mohs/radical surgery against comorbidity; still do not undertreat high-risk facial disease that threatens function.
- Skin of colour — later presentation of melanoma (acral/mucosal patterns) and under-recognition of pigmented BCC — staging still AJCC once diagnosed.[3]
Regional Guideline Notes
- AAD BCC and cSCC guidelines underpin US risk stratification and surgical choices.[6][9]
- European interdisciplinary cSCC and EuroGuiDerm BCC documents align risk features and multidisciplinary care.[5][10]
- AJCC 8th remains the global melanoma language for trials and boards.[1]
- Resource-limited settings: prioritise correct biopsy, adequate excision margins, and clinical nodal exam; refer high-risk H-zone and node-positive disease to centres with Mohs/oncology.
Prognosis Snapshot (Teaching Ranges)
Melanoma survival falls steeply from thin non-ulcerated primaries to thick, ulcerated, node-positive and distant disease — Breslow remains the dominant primary-tumour prognostic factor.[1][3] Most BCC is cured by adequate local therapy; morbidity is local invasion. High-risk cSCC drives nearly all NMSC nodal/metastatic events.[5][7]
Exam Pearls
STAGE-SKIN
STAGESKIN
Melanoma vs cSCC vs BCC — different rules
Breslow (melanoma); diameter/depth/PNI (cSCC)
Melanoma T modifier
Excisional for melanoma
H-zone high-risk → Mohs
Melanoma staging; MSLT-II if positive
High nodal risk cSCC → MDT
PD-1, BRAF/MEK, cemiplimab, SMO inhibitors
Document basins at presentation
- Breslow + ulceration = melanoma T.[1]
- BWH factors refine cSCC risk beyond size alone.[7]
- BCC = risk table, not default TNM.[9]
- Cemiplimab for advanced cSCC; Hedgehog inhibitors for advanced BCC; checkpoint ± targeted therapy for advanced melanoma.[11][3][10]
Exam application bank (NEET-PG / INICET)
One-line answer
Board-level synthesis of how cutaneous melanoma, cutaneous squamous cell carcinoma (cSCC) and basal cell carcinoma (BCC) are staged or risk-stratified and then managed. Melanoma uses AJCC 8th edition TNM driven by Breslow thickness and ulceration; cSCC uses AJCC 8th T categories plus Brigham and Women's Hospital (BWH) high-risk factor counting; BCC is risk-stratified (NCCN/AAD) rather than routinely TNM-staged when localised. Algorithms cover biopsy technique, wide local excision margins, Mohs micrographic surgery, sentinel lymph node biopsy, adjuvant and systemic options (PD-1, BRAF/MEK, cemiplimab, Hedgehog inhibitors).
Worked stems (answer without another resource)
Stem 1 — Classic presentation. Map symptoms to mechanism; name the first investigation and first treatment step with dose/route if drug therapy is standard. [1]
Stem 2 — Unstable / complicated. List red flags that force immediate resuscitation, theatre, ICU, antidote, or reperfusion — and what you do in the first 15 minutes. [1]
Stem 3 — Atypical group. Elderly, pregnancy, child, or immunocompromised: how presentation and thresholds change. [1]
Stem 4 — Differential trap. Name the three closest mimics and one discriminator for each. [1]
Stem 5 — Disposition. Who goes home with safety-netting, who is admitted, who needs HDU/ICU/theatre, and what follow-up is mandatory. [1]
Rapid viva checklist
- Definition + classification
- Pathophysiology chain
- Bedside signs / criteria
- Score with exact components (if any)
- Emergency bundle
- Definitive therapy with doses
- Complications of disease and of treatment
- Special populations
- Guideline/trial name if classic
- Three exam traps
Coverage self-check
If you cannot answer any stem above from this page alone, re-read the matching section — the page is intended to be self-sufficient for final-prof and NEET-PG/INICET questions on Skin cancer staging and management algorithms.
Expanded exam teaching (depth pass)
Clinical reasoning
For Skin cancer staging and management algorithms, examiners test whether you can prioritise life threats, choose the right first test, and give specific therapy (agent, dose, route, timing). Generic phrases without numbers score poorly.
Mechanism → feature map
Build a short chain: cause → pathophysiologic intermediate → clinical feature → complication. Every major symptom in the classic vignette should sit on that chain.
Investigation strategy
- Bedside/first-line tests that change immediate management
- Confirmatory or staging tests
- What a normal result does not exclude
- When not to delay treatment for imaging (unstable patient)
Management ladder
- Resuscitation / ABC / sepsis or haemorrhage bundle as relevant
- Specific antidote / procedure / antimicrobial / reperfusion / surgery
- Supportive care and monitoring targets
- Definitive long-term therapy and secondary prevention
- Disposition and safety-net advice
Special populations
Always prepare one line each for children, pregnancy, elderly, renal/hepatic impairment, and immunocompromised patients when the topic allows.
Pitfalls that fail candidates
- Treating the number not the patient
- Missing pregnancy status when relevant
- Imaging before stabilisation
- Wrong empiric cover or wrong antidote timing
- Incomplete counselling on recurrence, adherence, or red-flag return
Board-level synthesis of how cutaneous melanoma, cutaneous squamous cell carcinoma (cSCC) and basal cell carcinoma (BCC) are staged or risk-stratified and then managed. Melanoma uses AJCC 8th edition TNM driven by Breslow thickness and ulceration; cSCC uses AJCC 8th T categories plus Brigham and Women's Hospital (BWH) high-risk factor counting; BCC is risk-stratified (NCCN/AAD) rather than routinely TNM-staged when localised. Algorithms cover biopsy technique, wide local excision margins, Mohs m [1]
Structured revision sheet
Must-know numbers and names
List every score, size threshold, dose, and time window from this topic on a blank page from memory, then check against the sections above.
Three classic MCQ angles
- Most likely diagnosis given a vignette
- Next best step in management
- Most appropriate investigation
Three classic SAQ angles
- Pathophysiology in five steps
- Management algorithm with doses
- Complications and prevention
Clinical station flow
Greet → focused history → targeted exam → investigations → explain diagnosis → emergency care → definitive plan → safety-net / follow-up → answer examiner questions on mechanism and pitfalls.
References
- [1]Gershenwald JE, Scolyer RA. Melanoma Staging: American Joint Committee on Cancer (AJCC) 8th Edition and Beyond Ann Surg Oncol, 2018.PMID 29850954
- [2]Scolyer RA, Rawson RV, Gershenwald JE, et al. Melanoma pathology reporting and staging Mod Pathol, 2020.PMID 31758078
- [3]Tasdogan A, Sullivan RJ, Katalinic A, et al. Cutaneous melanoma Nat Rev Dis Primers, 2025.PMID 40180935
- [4]Faries MB, Thompson JF, Cochran AJ, et al. Completion Dissection or Observation for Sentinel-Node Metastasis in Melanoma N Engl J Med, 2017.PMID 28591523
- [5]Stratigos AJ, Garbe C, Dessinioti C, et al. European interdisciplinary guideline on invasive squamous cell carcinoma of the skin: Part 1. epidemiology, diagnostics and prevention Eur J Cancer, 2020.PMID 32113941
- [6]Work Group, Invited Reviewers, Kim JYS, et al. Guidelines of care for the management of cutaneous squamous cell carcinoma J Am Acad Dermatol, 2018.PMID 29331386
- [7]Cañueto J, Burguillo J, Moyano-Bueno D, et al. Comparing the eighth and the seventh editions of the American Joint Committee on Cancer staging system and the Brigham and Women's Hospital alternative staging system for cutaneous squamous cell carcinoma: Implications for clinical practice J Am Acad Dermatol, 2019.PMID 30003984
- [8]Karia PS, Morgan FC, Califano JA, et al. Comparison of Tumor Classifications for Cutaneous Squamous Cell Carcinoma of the Head and Neck in the 7th vs 8th Edition of the AJCC Cancer Staging Manual JAMA Dermatol, 2018.PMID 29261835
- [9]Work Group, Invited Reviewers, Kim JYS, et al. Guidelines of care for the management of basal cell carcinoma J Am Acad Dermatol, 2018.PMID 29331385
- [10]Peris K, Fargnoli MC, Kaufmann R, et al. European consensus-based interdisciplinary guideline for diagnosis and treatment of basal cell carcinoma-update 2023 Eur J Cancer, 2023.PMID 37604067
- [11]Migden MR, Rischin D, Schmults CD, et al. PD-1 Blockade with Cemiplimab in Advanced Cutaneous Squamous-Cell Carcinoma N Engl J Med, 2018.PMID 29863979
- [12]Fox M, Brown M, Golda N, et al. Nodal staging of high-risk cutaneous squamous cell carcinoma J Am Acad Dermatol, 2019.PMID 30227190